Article Text

Abstract
Background Timely, high-quality obstetric services are vital to reduce maternal and perinatal mortality. We spatially modelled referral pathways between sending and receiving health facilities in Kigoma Region, Tanzania, identifying communication and transportation delays to timely care and inefficient links within the referral system.
Methods We linked sending and receiving facilities to form facility pairs, based on information from a 2016 Health Facility Assessment. We used an AccessMod cost-friction surface model, incorporating road classifications and speed limits, to estimate direct travel time between facilities in each pair. We adjusted for transportation and communications delays to create a total travel time, simulating the effects of documented barriers in this referral system.
Results More than half of the facility pairs (57.8%) did not refer patients to facilities with higher levels of emergency obstetric care. The median direct travel time was 25.9 min (range: 4.4–356.6), while the median total time was 106.7 min (22.9–371.6) at the moderate adjustment level. Total travel times for 30.7% of facility pairs exceeded 2 hours. All facility pairs required some adjustments for transportation and communication delays, with 94.0% of facility pairs’ total times increasing.
Conclusion Half of all referral pairs in Kigoma Region have travel time delays nearly exceeding 1 hour, and facility pairs referring to facilities providing higher levels of care also have large travel time delays. Combining cost-friction surface modelling estimates with documented transportation and communications barriers provides a more realistic assessment of the effects of inter-facility delays on referral networks, and can inform decision-making and potential solutions in referral systems within resource-constrained settings.
- AccessMod
- referral system
- transportation
- communication
- Kigoma
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
What is already known?
Strengthening obstetric inter-facility referral systems in developing countries, including reducing delays due to inadequate transportation and unreliable communication, increases access to timely, appropriate obstetric and neonatal care.
What are the new findings?
About 57.8% of facility pairs in Kigoma did not refer to facilities providing higher levels of care.
When accounting for communication and transportation delays, only 47.5% of the facility pairs have an estimated overall referral transit times below 2 hours.
What do the new findings imply?
Interventions for reducing referral transit times in Kigoma could include increasing the number of ambulances, developing an ambulance dispatch system and improving radio and ambulance communications.
Combining cost-friction surface modelling with fieldwork data provides stakeholders with a better understanding of their healthcare referral system.
Introduction
Almost 99% of all maternal deaths, and most perinatal deaths, occur in low- and middle-income countries.1–6 Strengthening the district-level referral system is a key government strategy to improve maternal health in Tanzania.7 8
An inter-facility first-line obstetric referral system allows patients delivering at primary care facilities to obtain emergency obstetric and neonatal care (EmONC) at higher-level facilities if life-threatening complications occur.9 Within the Three Delays Model of maternal mortality, the efficiency of a referral system affects the third delay (delay in receiving appropriate care on arrival to a health facility, including time to travel between facilities if the appropriate level of care is not available at the initial facility).10 Efforts to improve referral systems contribute to two of the United Nation’s Sustainability Development Goals: Goal 3 (ensuring healthy lives and promoting well-being) and Goal 9 (building resilient infrastructure).11 The timeliness of a referral process may be affected by the quality of the communication network among facilities, transportation resources, and road conditions.12 Understanding the current use and existing gaps of the emergency referral system is key to expanding coverage of high-quality intrapartum services.
Geographic information systems (GIS) and spatial analyses can play an important role in assessing estimated physical access, distance and travel time to both obstetric care and EmONC facilities.13–15 To our knowledge, only one study in sub-Saharan Africa has conducted spatial analyses on obstetric care referrals, taking into account existing transport and communication factors.16 Research related to developing and evaluating strategies for locally appropriate transport, communication and referral systems for obstetric emergencies has been identified as a high priority by the public health and medical community and policymakers.17
We describe observed inter-facility referral patterns found in Kigoma Region overall, and by facility type or EmONC level. We assess if these pairs transported patients to higher levels of care and consider the effect of travel delays due to transportation and communication barriers on the referral network. These observations will guide regional and programmatic efforts in improving the efficiency and effectiveness of the regional referral network.
Methods
Study site
Kigoma Region is a remote region in the western part of Tanzania bordering Lake Tanganyika and Burundi (figure 1). In 2012, the region had a total population of 2 127 930—of which 22% were women of reproductive age (aged 15–49 years)—and was predominantly rural (83% of the total population).18

Contextual map of Kigoma Region, Tanzania.
More than one-quarter of Kigoma Region (27%) is arable/grazing land, with the remainder either as forests or bodies of water. Paved primary roads exist between the main towns of Kigoma, Ujiji, Manyovu, Uvinza and Kasulu; remaining roads are packed dirt. Additionally, many communities along Lake Tanganyika are isolated from roads, relying on boat transportation.19
Compared with Tanzania as a whole, women in Kigoma have a higher total fertility rate (6.5 births per woman vs 5.4 per woman), lower contraceptive use (27% vs 34%) and a lower proportion of facility deliveries (60% vs 63%).20 21 The Tanzanian Ministry of Health, Community Development, Gender, Elderly and Children—or the MoH—has identified Kigoma as a high-priority region for health systems strengthening efforts to improve reproductive, maternal and newborn health outcomes.8
Most healthcare services in Tanzania are provided in public-sector health facilities: dispensaries, health centres and hospitals.22 Dispensaries provide primary outpatient care, including maternal and child health services, for their catchment areas. Health centres, usually the first level of referrals from dispensaries, provide outpatient and inpatient care, and may contain operating facilities. Hospitals, typically referral centres for dispensaries and health centres, provide outpatient and inpatient care in various wards (eg, obstetric/gynaecological, surgical). Obstetric healthcare services are provided by the government (92.5%) and by faith-based and voluntary organisations (7.5%).23 The health system is decentralised, and district health offices (DHOs) provided administrative and management support to facilities.
Data source: Health Facility Assessment
We based our analyses on the 2016 Health Facility Assessment (HFA) conducted in Kigoma Region by the Centers for Disease Control and Prevention, AMCA Interconsult, and the Tanzanian MoH.23 The HFA assessed 174 facilities providing delivery services, including all six hospitals, all 25 health centres (excluding a health centre located in a refugee camp), and 143 dispensaries (ie, 88% of all dispensaries providing routine obstetric care). The HFA collected information on each facility’s geographical location, self-reported inter-facility referral networks for obstetric cases, observable transportation resources (eg, presence of functional vehicles, drivers, fuel and vehicle maintenance) and communication capacity (eg, mobile phones, radios, landline telephones) for both facilities and ambulances.
We classified facilities based on their performance of life-saving interventions (signal functions) during the 3 months prior to the HFA. We defined a facility as basic EmONC (BEmONC) if it performed all of the seven basic signal functions: (1) administration of parenteral antibiotics, (2) administration of oxytocic drugs, (3) administration of anticonvulsants, (4) manual removal of the placenta, (5) removal of retained products of conception, (6) assisted vaginal delivery and (7) neonatal resuscitation. Comprehensive EmONC (CEmONC) facilities additionally performed (8) caesarean deliveries and (9) blood transfusions. We classified remaining facilities in the health system that did not meet either standard as providing non-EmONC, or routine, obstetric care (eg, skilled labour provision, partograph use, active management of third stage of labour).
During HFA fieldwork, we measured the geographical coordinates of each facility using Garmin eTrex 20 GPS devices (accuracy ±10 m).23 We cross-referenced these coordinates with a geocoded inventory of government facilities available from the health management information system maintained by the MoH.24
Referral pair case definitions
We built facility pairs based on receiving facilities’ staff reports collected in the HFA, where respondents named facilities which sent patients to their own facility. We defined an inter-facility referral pair as two facilities connected through the provision of care: a sending facility referring out patients experiencing delivery complications, and a receiving facility accepting patients providing an equivalent, or higher, standard of care. Health facilities may have more than one referral relationship, and some facilities, particularly hospitals, participate in multiple referral pairs. Additionally, 12 facilities acted as both sending and receiving facilities.
We paired facilities not mentioned as sending to any receiving facility (ie, ‘orphaned facilities’) with the nearest facility of equal or higher level, measured by straight-line distance between the two facilities. There were 77 orphaned facilities, which were dispensaries (97.4%) or health centres (2.6%).
Direct travel time estimation
We calculated the estimated travel time between sending and receiving facilities in each pair, called the direct travel time, using a cost-friction surface approach. We used AccessMod V.5.0, revisions 5.15 and earlier (WHO; Geneva, Switzerland), to estimate direct travel times between sending and receiving facilities, inclusive of miles and travel time from an external ambulance facility.25 26 AccessMod uses a cost-friction surface algorithm to generate a raster surface showing estimated direct travel time, based on geographical coordinates of health facilities, road network coverage, land cover raster data,27 digital elevation model raster data,28 water bodies and a travel scenario table (ie, travel speeds based on land cover classification and transportation mode), as described elsewhere.29
Road network data were obtained via OpenStreetMap, and were reclassified into primary, secondary and local roads.30 Local roads were then classified based on road width to reflect car-accessible and non-car-accessible roads; the latter included motorcycle-accessible, bicycle-accessible and walking-accessible roads.29 For our analysis, we considered all non-car-accessible roads as walking areas.
We assumed most transportation between facilities was motorised, and included Tobler’s function to allow for slope-dependent walking speeds.31 To define motorised speed values for each road category, we cross-referenced the authors’ direct observations in Kigoma Region with a cost-surface analysis conducted in Dar es Salaam, and the WHO’s Tanzania road safety brief.32 33 In line with the WHO recommendation of all women reaching EmONC services within 2 hours, we assessed a maximum of 2-hour travel time between sending and receiving facilities. However, as the direct travel time between distant pairs sometimes exceeded 2 hours, we modelled a maximum of 6-hour travel time for these pairs.
To obtain direct travel times to each receiving facility from each sending facility, we spatially joined the sending facilities’ geographical coordinates to each receiving facility’s modelled travel time surface using ArcGIS V.10.4. We divided direct travel times into five categories: 0 to <30 min (‘0–30’), 30 to <60 min (‘30–60’), 60 to <90 min (‘60–90’), 90 to <120 min (‘90–120’) and 120 min or more (‘120+’).
Total travel time estimation
To make the direct travel time estimates reflect actual travel conditions, we added standardised travel time adjustments to the direct travel times to create a set of total travel times (online supplementary appendix 1). We made a djustments based on ambulance availability and communication capacity, and used project partner feedback to influence our adjustments for the vehicle agreement and self-transport scenarios. As all referrals originated at the sending facility, we inferred adjustments using the characteristics of the sending facility. We performed a sensitivity analysis on the total travel times, by modifying the time adjustments to have low, moderate and high values. This allowed us to create uncertainty intervals, to observe the extent that transportation and communication adjustments had on the overall analysis when using the lowest possible and maximum possible parameters.
Supplemental material
We defined ambulance capacity at a sending facility as the presence of a functional motorised vehicle on-site explicitly designated to carry patients, with available driver and sufficient fuel. If a facility lacked any of these elements, the facility was considered to lack ambulance capacity.
Primary mode of transportation was based on a transportation allocation process that allocated transportation for a facility pair based on the highest form of primary transportation available at the sending facility (online supplementary appendix 2). While Tanzania lacks official guidelines on facility transportation and referrals, the MOH recommends that each hospital and health centre have ambulance capacity. Sending facilities without ambulance capacity could potentially use an ambulance from a nearby facility, or a vehicle from the DHO. We accounted for borrowing an off-site ambulance with an ambulance travel time from ambulance location to sending facility time adjustment. If no ambulance was available within a pair, we estimated time adjustments for identifying and mobilising privately hired motorised vehicles, whether through an agreement between facilities or in a self-transport situation.
We defined communication capacity at a sending facility as either a functioning cell phone, a functioning landline telephone or a radio transmitter available for external communications. If the sending facility had both a mobile phone and a functional landline/radio, the pair was classified as having high communication capacity. If a sending facility had either a mobile phone or a landline/radio, the pair had moderate communication capacity; if a sending facility had neither form of communication, the pair had low communication capacity.
Supplemental material
Mobilisation times include the time needed to call for transportation, and to prepare and depart, and is estimated based on ambulance and communication capacity (online supplementary appendix 1). We used the mobilisation time adjustments described in Appendix 1 to account for potential time delays according to documented ambulance and communication capabilities within the pair. We sum the direct travel time calculated with AccessMod with the corresponding mobilisation times to estimate the total travel time for the pair (total travel time = direct travel time + mobilisation time).
We used SAS V.9.3 to add transportation and communication adjustments to the estimated direct travel times. We created maps of the referral network using ArcGIS to show both direct travel time and total travel time between sending and receiving facilities.34 We calculated summary statistics for travel time—median, min, and max values—to better represent travel time distributions.
Patients and the public involvement
This research was performed without any patient or public involvement. The analysis was based on the HFA survey, collected through the Bloomberg Philanthropies-supported ‘Maternal and Reproductive Health in Tanzania Project’, and publically-available geospatial data.
Results
Health Facility Assessment
When assessing the primary means of transportation for the 174 facilities included in the HFA, 8.6% of facilities had functioning ambulances located on-site at the facility (table 1).
Facility-based quality of care, transportation and communication variables, 2016 Kigoma Health Facility Assessment
Over half of the facilities (54.6%) used an external ambulance, 2.3% used private vehicles and one-third (34.5%) required patients to self-transport. The majority of facilities reported multiple means of motorised transportation (ie, including self-transport means). Hospitals either had an ambulance on-site (66.7%) or required patients to self-transport (33.3%). Most health centres had an on-site or external ambulance (84.0%) or required patients to self-transport (16.0%). Dispensaries rarely had an on-site ambulance (0.7%) and depended on external ambulances (58.7%) or patients self-transporting (37.8%).
The majority of facilities relied on mobile phones for communication; nearly all facilities (97.1%) had mobile phones. However, less than one-eighth of facilities (12.1%) reported having a facility landline telephone/radio transmitter in working order.
Facility pair characteristics
We created 166 facility pairs, which used 169 distinct facilities of the 174 facilities included in the HFA. The number of pairs did not include dispensary/dispensary pairs, nor did referral pairs include facilities not in our HFA. Our facility pairs included 140 distinct sending facilities, 17 distinct receiving facilities and 12 distinct facilities that served as both sending and receiving facilities.
Distinct sending facilities were either hospitals (0.7% of sending facilities), health centres (1.4%) or dispensaries (97.9%) (table 2). Distinct receiving facilities were either health centres (76.5% of receiving facilities) or hospitals (23.5%). Distinct facilities with both sending and receiving functions were either hospitals (16.7% of simultaneous sending/receiving facilities) or health centres (83.3%).
Percent of facility pairs using transportation and communication characteristics, overall, by facility pair type and by EmONC pair type
Most referral pairs originated from a dispensary (83.3%). Overall, most referral pairs referred to a health centre (77.1%); few pairs referred directly to a hospital (22.9%). Few sending facilities (10.9%) referred patients to more than one receiving facility. Most receiving facilities (82.7%) received patients from four or more sending facilities. The receiving facility accepting the highest number of referrals, Kibondo Hospital, linked to 13 sending facilities.
Less than one-third of facility pairs (31.9%) referred from a BEmONC or non-EmONC facility to a CEmONC facility. Only 10.2% of facility pairs referred from a non-EmONC facility to a BEmONC facility (table 2). All other pairs were non-EmONC/non-EmONC or CEmONC/CEmONC pairs.
Transportation/communication policies in facility pairs
Transportation and communication policies differed prominently by facility pair type (table 2). Ambulances at health facilities were at all hospital/hospital pairs (100.0%) and few health centre/hospital pairs (10.0%). Around two-thirds of dispensary/health centre (60.7%) and health centre/health centre pairs (66.7%) used external ambulances. Self-transports were also reported at dispensary/health centre (36.9%) and dispensary/hospital pairs (52.2%). Private vehicles were used by dispensary/health centre (2.5%) or health centre/hospital pairs (10.0%). Communication capacity also differed across the pairs; 11.4% had high communication capacity, whereas 85.5% had moderate communication capacity (owning a mobile phone).
Transportation modes also varied by communication capacity (data not shown). Within the 19 pairs with high communication capacity, 52.6% used an external ambulance, whereas the remainder used an ambulance at the sending facility (21.1%) or required patients to self-transport (26.3%). In the 142 facility pairs with moderate communication capacity, most used an external ambulance (59.2%) or required patients to self-transport (37.3%), whereas others used an ambulance present at the facility (1.4%) or a private vehicle agreement (2.1%). The remaining 5 facility pairs with low communication capacity either used an external ambulance (40.0%), required patients to self-transport (40.0%), or used a private vehicle agreement (20.0%).
Direct travel times
The median direct travel time was 25.9 min (range: 4.4–356.6) (table 3).
Direct and total travel times, reported in minutes, overall, by health facility pair type, and by EmONC pair type (median (min-max))
More than half of facility pairs (61.5%) had direct travel times between 0–30 min. Nearly one-quarter of facility pairs (24.1%) had direct travel times between 30 and 60 min, 9.6% had direct travel times between 60 and 120 min and 4.8% of facility pairs had direct travel times above 2 hours.
Direct travel times varied by pair types (table 3). Dispensary/hospital pairs had the shortest direct travel times (19.8 min (range: 10.0–37.4)), followed by dispensary/health centre pairs (26.0 min (4.4–260.7)), health centre/hospital pairs (29.8 min (7.7–127.3)) and health centre/health centre pairs (38.4 min (12.1–69.3)). The longest direct travel time was for hospital/hospital pairs (156.4 min (7.8–356.6)). When considering EmONC status, BEmONC/CEmONC pairs had the shortest median direct travel times (15.2 min (15.1–43.5)), followed by non-EmONC/non-EmONC (24.9 min (4.4–260.7)), non-EmONC/CEmONC (26.1 min (7.7–127.3)) and non-EmONC/BEmONC pairs (30.9 min (10.8–198.7)). CEmONC/CEmONC pairs had the highest median direct travel time (156.4 min (7.9–356.6)).
Total travel times and shifts in travel time category
When communications and transportation adjustments were applied, the median travel time was 81.1 min (17.9–366.6) for low-adjusted times, 106.7 min (22.9–371.6) for moderate-adjusted times and 131.2 min (27.9–376.6) for high-adjusted times (table 3).
Most facility pairs (94.0%) shifted to a higher time category regardless of the adjustment type (online supplementary appendix 3). When comparing direct and moderate-adjusted total travel times, over one-quarter of facility pairs (27.2%) with under 2 hours of direct travel time had moderate-adjusted total travel times that exceeded 2 hours. Travel time pattern-shifting within the lower time categories were less drastic for the low-adjusted travel time scenarios compared with the moderate-adjusted and high-adjusted travel time scenarios.
Supplemental material
Some facility pairs, by facility type or EmONC, had large travel time shifts between direct travel times and moderate-adjusted total travel times (data not shown). Nearly one-third of dispensary/health centre (31.4%) and health centre/health centre pairs (33.3%) with a direct travel time under 2 hours shifted to a moderate-adjusted travel time over 2 hours. No significant travel time shifts occurred for dispensary/hospital, health centre/hospital, and hospital/hospital pairs. When considering EmONC status, 27.3% of non-EmONC/non-EmONC pairs, 43.8% of non-EmONC/BEmONC pairs and 24.0% of non-EmONC/CEmONC pairs with a direct travel time under 2 hours shifted to a total travel time over 2 hours (data not shown). No extensive travel time category shifts occurred for BEmONC/CEmONC or CEmONC/CEmONC pairs.
Geographical analyses
The referral network was concentrated in the main towns of the region—Kigoma, Kasulu, Kibondo and Kakonko—with higher-level facilities acting as both sending and receiving facilities (figures 1–2).
{kind=link}
{kind=link}
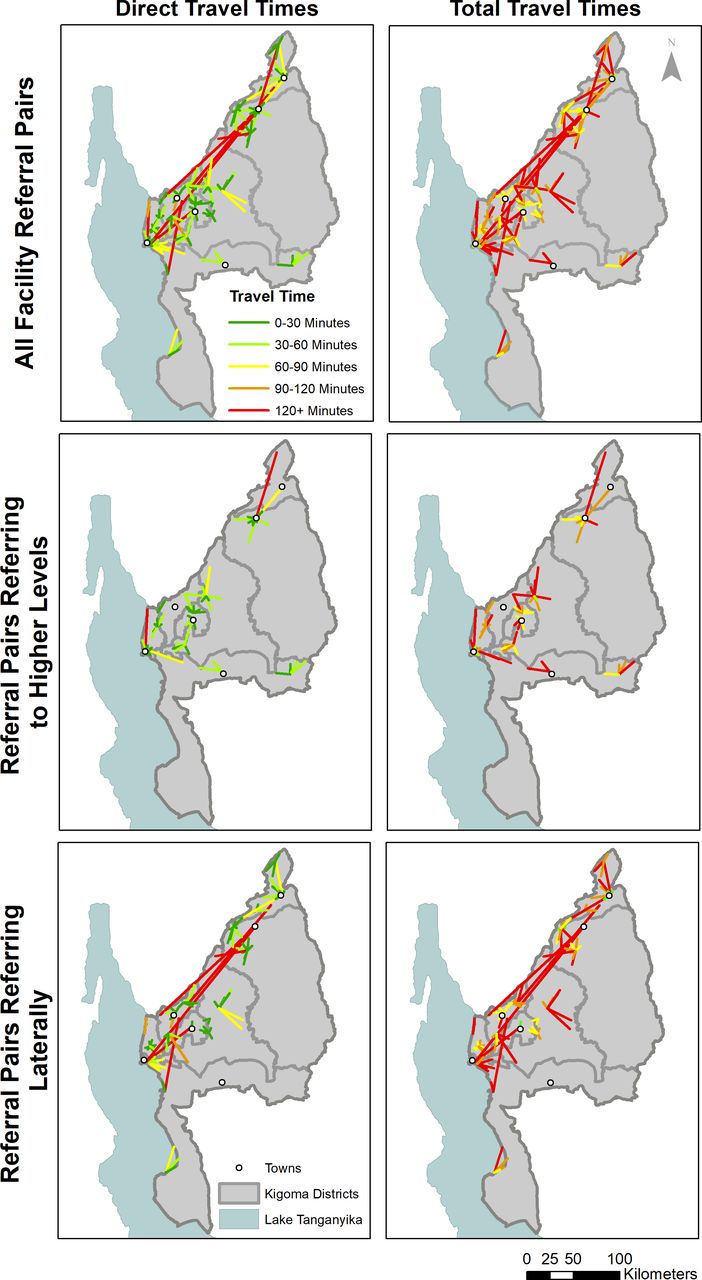
Visualisation of estimated travel times for all facility pairs.
Several referrals were sent to Kigoma Town from distant northern locations such as Kakonko District (1.2% of referral pairs) or Kibondo District (0.6%). However, some facilities located within the southernmost district of Uvinza—specifically Uvinza Health Centre in the centre, Nguruka Health Centre in the east, and Buhingu Health Centre in the south—reported not sending patients to any other facility. Facility pairs did not extend out from these facilities; these facilities were disconnected from the referral network.
We displayed direct and moderate-adjusted total travel times for the overall referral network and for referral pairs which refer to higher levels of care (figure 2). Facility pairs experiencing the shortest direct transportation times, shown in green, were located in Kasulu, Kibondo and Kigoma Town administrative councils. These were the more urbanised areas of the region, and facility pairs primarily referred patients to the hospitals in these regions (eg, Kibondo District Hospital, Maweni Hospital and Baptist Hospital). Most pairs sending patients within the same district had shorter direct travel times compared with pairs sending patients outside of the originating district, with a median direct travel time of 22.5 versus 37.4 min respectively.
Most facility pairs referring to higher EmONC levels were in western Kigoma region, stretching from Uvinza in the south to Kibondo in the north. Facility pairs referring up to a BEmONC facility were concentrated in the south, central and west of the region. Examples include Gungu Health Centre, in Kigoma Town near Lake Tanganyika, Uvinza Health Centre, in Uvinza District in the central south area of the region, and Rusesa Health Centre, in Kasulu Rural (figure 2). In contrast, facility pairs referring up to a CEmONC facility occurred along the main highway running parallel to the Burundian border, primarily in the central-south area of the region (Kigoma Town, Kigoma Rural, Buhigwe, Kasulu Town and Kasulu Rural districts). Such referrals also happened in the north (Kibondo) and the southeast (Uvinza) of the region. Most of these facility pairs stretched between districts encompassing this main road, although some were located exclusively in Kibondo District in the north, Kasulu Rural in the centre of the region, Uvinza District in the south and Kigoma Town next to Lake Tanganyika.
Discussion
Transportation and communication limitations are critical in understanding geographical access to EmONC and interventions that can improve access. Our findings highlighted characteristics associated with increased travel time between first-level and higher-level obstetric facilities, and demonstrated that transportation and communication policies between health facilities strongly differed by facility type and EmONC type. When accounting for referrals between all health facility types, Kigoma’s health system has a high proportion of lateral referrals between facilities with the same standard of care, which potentially delays receipt of higher levels of obstetric care. Within Kigoma Region, a lack of sufficient or external ambulances strongly influenced the transportation mode used in the referral system. Our HFA analysis showed that only 12 of 174 facilities had ambulances on-site; 2 additional ambulances were available at 2 district councils. Our findings also showed that a facility’s inability to use external ambulances affected dispensaries, the most common facility type to refer patients to higher-level facilities (87% of all facility pairs). A high percentage of referral pairs coming from dispensaries and health centres required patients to self-transport to a receiving facility, potentially increasing the travel time needed to reach adequate care, due to the extra time needed to identify and organise transportation.
A lack of communication methods between facilities was present in Kigoma Region, which could increase overall referral times; more than 97% of facilities had a mobile phone available, but only 12% of facilities had a working landline or radio transmitter. Even fewer facilities had an available ambulance-specific phone or radio. While our 2016 HFA could not adequately capture network coverage, field experience has shown that many facilities may be outside of adequate mobile network coverage, and mobile phones or landlines may not be specifically designated for referral purposes. Radios are more apt at breaching these barriers, particularly in areas that may lack mobile network coverage.35 Efforts to expand communications are being made within pilot referral projects as part of the broader project. For example, Thamini Uhai’s Kakonko/Kibondo hospital referral project guidelines included an emphasis on prioritisation of cell phones for emergency referrals using a toll-free closed user group connexion.36 Alternatively, sites can consider using short-wave two-way radios for referrals, with specific radio channels dedicated to referrals in areas with unreliable mobile network coverage.37 We suggest using standard operating procedures (SOPs) detailing usage of communication devices between facilities.
In Kigoma Region’s referral system, less than half of all facility pairs referred to higher levels of EmONC; only 10.2% of all facility pairs referred to EmONC facilities from non-EmONC facilities, and 34.9% referred to CEmONC facilities from non-CEmONC facilities. The WHO recommends that all women with serious direct obstetric complications should receive treatment in EmONC facilities.38 In Kigoma region, only 42% of deliveries occurred in facilities providing EmONC services in 2015, yet EmONC facilities provided care for 83% of all direct obstetric complications.39 The process of referring to lateral facilities unnecessarily lengthens the time needed to reach the appropriate level of care, and may require multiple referrals for the same case. We hypothesise that lateral referrals may occur because providers at sending facilities believe receiving facilities have a certain standard of care based on previous experiences or official designation. As we assessed the EmONC status based on the provision of signal functions within the last 3 months,38 the facilities we classified as EmONC may not consistently act as EmONC facilities. Facilities may lack infrastructure, equipment, supplies or staffing when services are actually needed. Lateral referrals may occur because of geographical proximity or convenience, without consideration for the level of care provided at the receiving facility.40 An updatable list of facilities’ current EmONC statuses, assessed quarterly, can be shared across the region, so providers can assess the most appropriate facilities for referral.
Our analysis demonstrated that total travel times were often longer than 2 hours, often considered the limit for acceptable travel time for patients experiencing severe obstetric complications, particularly obstetric haemorrhage.38 Across all facility pairs, the median total travel times neared 1.5 hours (81 min). Concernedly, the median total travel times for all pairs originating from a non-EmONC facility, regardless of where they were sending patients, was between 80 and 143 min (approximately 1.3–2.4 hours).
We observed two additional referral system characteristics that limit the system’s functionality, including lack of standardised national guidelines or SOPs available for referrals and poor coordination of ambulances for referrals. Although national health strategies—National Road Map Strategic Plan to Improve Reproductive, Maternal, Neonatal, Child and Adolescent Health in Tanzania (2016–2020), the Health Sector Strategic Plan July 2015–June 2020 (HSSP IV) and the Big Results Now project—prioritise referral improvements, they do not delineate specific actions to be taken and how to monitor referral strengthening efforts.7 8 41 In this context, the Bloomberg Philanthropies-supported project created detailed referral guidelines and SOPs to improve referrals between selected health facilities and their catchment areas.36
Regarding ambulance availability, an increase in the number of health facilities with on-site ambulances may be costly to maintain 24/7. A more cost-effective solution is to link transportation systems via a dispatch system to coordinate use of available vehicles. Kigoma District relies on a district-coordinated dispatch system with little regional oversight. While Kigoma Region has a dispatch centre, only one health facility explicitly reported relying on the dispatch centre when referring patients. A dispatch centre has been shown to improve access to EmONC services, decreasing travel time for facility-to-facility referrals.42 As decentralised service provision can be effective only if health facilities have the ability to communicate between facilities and receive transportation 24/7, sites may benefit from a regionally coordinated system with the ability to link district dispatch systems and increased awareness of transportation availability for facilities providing obstetric care. A dispatch system’s utility also depends on the density of patient demand.
Our analysis is unique as it measures travel time using geographical cost-friction modelling, communication and transportation availability, and documented facility-to-facility referral pattern. First, we identified opportunities for transportation and communication improvements in the referral system via direct observations collected in the survey. Second, we combined transportation and communication information with estimated cost-friction surfaces from AccessMod, V.5.25 43 44 While other authors used similar data sources and approaches to estimate travel times, they assumed a set adjustment across the entire referral network, rather than using field observations to determine transportation and communication types.16 Our methodology is designed to be accessible to those without extensive GIS knowledge, by simplifying the complicated process of creating cost-friction rasters used for travel time estimation with a graphical user interface. Our travel time measurement is grounded in an external estimation of travel and mobilisation times rather than using patient self-reports, making the direct travel more precise.45
It is important to reflect on the limitations of the study. Even when travel time is adequately measured using cost-friction surfaces, it is not an accurate reflection of the actual time spent within the referral process. Our transportation and communication adjustments are based on providers’ self-reports, and may vary between facilities. We used these reports to estimate communication and mobilisation delays, as direct measurements are not available for all pairs, particularly when patients must arrange self-transport. We did not assess other delays related to receipt of appropriate care of transferred patients, nor did we delineate the exact reasons for referral. Theoretically, the modelling itself is also affected by data quality, such as incomplete road networks or inaccurate coordinates.
While our analysis accounted for ambulance travel or patients arranging transportation themselves, we assumed only one transportation mode per facility pair. With poor availability and the potentially high cost of transport by automobile, referred patients may turn to other forms of transportation, such as bicycles or motorcycles.46–50 We may have underestimated travel time for self-transport using slower motorised, or non-motorised transport, and overestimated travel time for self-transport with automobiles. We assumed that ambulances were available if the facility reported in the HFA that they had a functional on-site ambulance, but recognise that additional delays may be encountered if a facility’s ambulance is in use for another emergency.
Travel times in this analysis were modelled on the land cover type, road network and travel speeds specified in dry season, and did not account for delays in the rainy season.16 44 51 This analysis could not account for degraded road conditions during the rainy season, though evidence suggests seeking transport for referral decreases as weather worsens, due to longer travel times and poorer road conditions.52
Adequate access to EmONC is essential to improve maternal and perinatal health, and our comprehensive analysis of travel time to EmONC takes into account availability, distances and patterns of inter-facility referrals.38 Additional research is needed to better understand how to optimise transport and referral pathways, including identifying barriers to direct referral to BEmONC and CEmONC facilities, rather than referring laterally. Understanding patients’ and providers’ current usage of the inter-facility referral systems in obstetric emergencies could improve resource allocation and optimise travel times. Future HFAs planned in the region can benefit from inclusion of factors influencing facility-to-facility referrals.
Emergencies during pregnancy, labour, delivery and postpartum often develop without warning, and not all facilities are able to provide appropriate and timely EmONC services. A functional referral system connects non-EmONC and EmONC care, and optimises the use of limited resources for women who access services.53 Systematic inter-facility referral protocols and SOPs—with an updatable and current list of facilities’ EmONC capacity—could improve referral practices. A functional referral system, emphasising the awareness and use of a dispatch system, can optimise use of limited ambulances without increasing costs. Improvements in timely communication, mobilisation, inter-facility agreements, and readiness to transport and receive obstetric emergencies are needed to improve maternal and neonatal survival in Kigoma Region. Our findings suggest that while referrals between similar levels of facilities are common, this practice of lateral referring may contribute to increased delays when life-saving services are unavailable at the initial receiving site, necessitating additional referrals. Referrals may be improved through implementation of national guidelines and SOPs, coupled with consideration for current EmONC capacity of referral facilities.
References
Footnotes
Handling editor Seye Abimbola
Contributors MMS, FS and YNC conceived and designed the study. MMS, GEA and YNC conducted the analysis and interpreted the data. MMS, FS and YNC coordinated the data collection and wrote the first draft of the manuscript. PC, AA, and MD were involved in revising the manuscript based on fieldwork-based experience. MMS, FS and YNC agreed to be accountable for all aspects of the work ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All authors read and approved the final manuscript submitted for publication.
Funding This study was funded by Bloomberg Philanthropies and the Fondation H&B Agerup.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This study was reviewed and approved by the CDC's Center for Global Health Human Subject Review Board and was determined not to comprise human subjects research.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data may be obtained from a third party and are not publicly available.