Article Text

Abstract
Introduction Guinea is a country with a critical deficit and maldistribution of healthcare workers along with a high risk of epidemics' occurrence. However, actors in the health sector have missed opportunities for more than a decade to attract political attention. This article aims to explain why this situation exists and what were the roles of actors in the agenda-setting process of the post-Ebola health system strengthening programme. It also assesses threats and opportunities for this programme's sustainability.
Methods We used Kingdon’s agenda-setting methodological framework to explain why actors promptly focused on the health sector reform after the Ebola outbreak. We conducted a qualitative explanatory study using a literature review and key informant interviews.
Results We found that, in the problem stream, the Ebola epidemic caused considerable fear among national as well as international actors, a social crisis and an economic system failure. This social crisis was entertained by communities’ suspicion of an 'Ebola-business'. In response to these problems, policy actors identified three sets of solutions: the temporary external funds generated by the Ebola response; the availability of experienced health workers in the Ebola control team; and the overproduction of health graduates in the labour market. We also found that the politics agenda was dominated by two major factors: the global health security agenda and the political and financial interests of national policy actors. Although the opening of the policy window has improved human resources, finance and logistics, and infrastructures pillars of the health system, it, however, disproportionally focuses on epidemic preparedness and response. and neglects patients’ financial affordability of essential health services.
Conclusion Domestic policy entrepreneurs must realise that agenda-setting of health issues in the Guinean context strongly depends on the construction of the problem definition and how this is influenced by international actors.
- agenda-setting
- Ebola outbreak
- health system strengthening
- health workforce
- global health security
- Guinea
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Healthcare workers’ deficit is an important area of concern for the achievement of global health security, universal health coverage and economic growth.
Guinea health indicators are among the worst in West Africa countries, resulting from decade-long underinvestment and non-prioritisation of the health system by policymakers.
After the Ebola outbreak, considerable attention has been given to stengthening the health system along with the agenda-setting of policies aiming at addressing healthcare workers’ deficit and maldistribution in Guinea, yet it is not clear how this sudden boost to the health system and national policy-agenda proceeded and how the global health security agenda will help to advance universal health coverage issues.
What are the new findings?
The fear of the Ebola outbreak spreading in high-income countries and the financial support from Western governments have become key enabling factors for the agenda-setting of the current health system strengthening programme.
However, challenges occurring in the current health system's design and implementation urgently need to be overcome to sustain opportunities generated by the global health security agenda.
What do the new findings imply?
Ensuring effective implementation of a Universal Health Coverage policy will require another policy momentum — different from the global health security agenda — including a strong and sustainable commitment of state actors.
Introduction
The critical deficit of healthcare workers (HCWs) in West African countries is a major concern for global health security (GHS) and the achievement of universal health coverage (UHC).1 2 This region hosts 3% of the global health workforce but is disproportionately confronted by 25% of the global disease burden.3
Despite substantial evidence of the positive impact of employment in the health sector on economic growth, governments in sub-Saharan Africa have been reluctant about investing in health systems.4 Currently, government expenditure allocated to the health sector remains far below the norm of 15% that all African countries pledged in the 2001 Abuja initiative.5
Given the crucial role of HCWs in care delivery, any healthcare policy should address their availability, affordability, acceptability and quality.6 In most of the countries with a critical deficit of HCWs, policies such as free obstetric care and maternal health fee-exemptions have received high attention mostly because preventing maternal mortality resonates with a vote-seeking political agenda.7–9 In addition, contextual factors such as epidemic emergencies are known to highly influence the health policies' agenda.8 10 For instance, the poliomyelitis outbreak of 2011 in Chad raised political attention on the health sector, especially maternal and child health (MCH), resulting in the agenda-setting of a pilot project to improve MCH.7
Guinea is a country with a high risk of epidemics. From 2000 to 2012, cholera and meningitis epidemics had led to approximately 29 000 cases and 1200 deaths, most of which occurred in rural settings.11 12 Measles, which causes less fear among the population and in reporting to health services, represents the most frequent and deadly epidemic in Guinea.13 In the 2014 measles outbreak, a total of 5248 cases and 11 deaths was reported.14 Moreover, poliomyelitis cases were detected in Guinea in 2009 and 2011, while yellow fever outbreaks led to 500 cases and 70 deaths between 2001 and 2013.14 15
However, these epidemics failed to attract domestic political attention to health system strengthening (HSS) needs until the emergence of the Ebola Virus Disease (EVD) outbreak in 2014.16 This epidemic, the largest in recent history, rapidly spread to Liberia and Sierra Leone, and infected more than 28 000 people including HCWs.17
This outbreak, by attracting considerable political attention to the health sector, has generated opportunities (policy window) for HSS.18 Therefore, this article aims at understanding the process of health policy agenda-setting that resulted during and from the Ebola epidemic as well as threats and opportunities for sustaining the policy window. Specifically, it explores the momentum of the Ebola outbreak and the role of actors in opening a policy window for HCW development in Guinea. Finally, it discusses whether the increasing GHS attention towards the health sector would generate opportunities for UHC reforms. This finding may contribute to advancing the evidence of health policy agenda-setting in the Western African region.
Contextual factors impeding health care workers’ policy in Guinea
Every year, at least 3000 HCWs graduate in Guinea.19 However, its formal public health sector only employs one HCW per 1000 population.20 This situation is worse in rural districts, where only 30% HCWs (2312 of 7706) are available to cover about 70% (~7.4 million) of the country’s population, implying 0.31 HCWs per 1000 population.20 Additionally, uneven distribution exists within districts as qualified HCWs — physicians, midwives and state nurses — mainly live in the urban parts of the districts.
The multi-sectorial complexity of the recruitment and management of HCWs is one of the major factors affecting their deficit and maldistribution in Guinea.19 21 The Ministry of Health (MoH) has little control over the training, recruitment and salary payment of this personnel.21 Despite multiple attempts in enabling the MoH, the Ministry of Public Services (MoPS) and the Ministry of Finances (MoF) have respectively kept control of the recruitment and salary payment of HCWs in Guinea.21 This power differential is seen to impede HCW's policy in two ways.19 First, the MoPS tends to almost exclusively recruit HCWs from the capital Conakry who may not be familiar with rural settings.19 Second, as salaries are directly wired by the MoF, civil servants do not feel they have an obligation vis-à-vis their supervisors and the communities they serve, for example, in terms of retention in rural areas.19
Moreover, operating expenses such as salary and services purchasing represent more than 80% of the national budget allocated to health.21 Additionally, the budget execution of the MoH is below 50%.21 All these facts give little room to the MoH to claim, from the MoF, any investment in the HCWs’ career development.21
Chronology of the health care workers’ problematic in Guinea
The deficit and maldistribution of HCWs in rural Guinea got explicit attention from the MoH in 2000 during a national health system assessment. Policy recommendations were formulated accordingly in the first triennial health development plan of 2003, including the recruitment of new staff, staff redeployment plan and reinforcement of management and governance boards such as the creation of a national division of human resources for health allocated with more resources for staff supervision.20
For more than a decade, the situation of HCWs in rural Guinea remained more or less the same despite several staff recruitments and deployments.20 Between 2007 and 2012, nearly 1800 HCWs were recruited and deployed in rural districts.21 However, the health sector budget as part of government expenditure stagnated at 3% and even decreased to 1.75% in 2012–13.22 Also, the proportion of HCWs employed in rural districts decreased from 30% in 2000 to 17% in 2012.21 22 Health indicators in rural areas consistently remained worse than those in urban areas (table 1).23
Comparison of five health indicators between rural and urban settings, Health Demographic Survey, 2012, Guinea23
To address the gap and reduce inequities in access to HCWs, international partners such as the World Bank (WB) and the United Nations Population Fund (UNFPA) temporarily recruited staff in some rural districts and proposed that state actors prioritise them in recruitment processes.21 However, because of poor governance and lack of regulation, outcomes from rural staffing projects could not be sustained and the contracted personnel would leave their positions as soon as their contracts were terminated.20 21 In 2012, 50% of the public HCWs lived in Conakry, to serve only 15% of the country’s population.20
Government actors turned a blind eye to HCWs' issues in rural settings until the Ebola outbreak emerged in Guinea in December 2013 in the Guéckédou health district and was declared a public health emergency in March 2014.16 The deficit of HCWs in rural areas and poor health information systems contributed to the spread of the outbreak in 24 (out of 33) other rural health districts and Conakry.24
As a consequence of the Ebola outbreak, Guinean and international high-level policymakers — The President of the Republic, and bilateral and multilateral diplomatic representatives — gave prominent attention to the health sector including the HCW deficit in rural Guinea. This article aims at assessing why this was the case in the wake of the Ebola outbreak and explores the role of policymakers and other actors in this process.
Methods
Study design and analytical framework
We conducted a qualitative explanatory study.25 This study design helps explain the reasons underlining the post-Ebola agenda-setting process, and the related political and financial patterns. It further seeks to identify and explain relationships between these phenomena25
Our analysis draws on the Kingdon model of agenda-setting.8 We have applied this framework because it allows understanding the role of policy entrepreneurs (actors) inside and outside government who take advantage of agenda-setting opportunities – known as policy windows – to move the health workforce issue onto the government’s formal agenda.8 Explicitly, this framework helps understand why overcoming HCWs’ deficit and maldistribution became a prominent issue in the eyes of policymakers during and after the Ebola outbreak.
The framework describes policy development as the result of three distinct ‘streams’: the problem, the policy and the politics.8 The problem stream refers to the characteristics of problems (HCWs' deficit and maldistribution) and their perception by decision-makers as public matters necessitating government action.8 The policy stream provides a set of problems' analysis and their solutions.8 Finally, the politics stream, or political will, consists of political events such as elections and international policy agendas.8 The meeting of these three streams creates a window of opportunity (policy window) that is enabled through active actors in society and the government (policy entrepreneurs).8 26
Data collection and study participants
We conducted a literature review of policy and media records and in-depth interviews with relevant stakeholders using an interview guide. National policies, strategic plans and audit reports were identified by the snowball method in conjunction with key informants’ interviews. We then used the findings to deconstruct the three streams of the Kingdon framework.8 These participants were purposively selected based on their potential participation in, first, the development or implementation of former HRH policies or, second, the agenda-setting of the post-Ebola HSS programme. In total, 20 key informants’ interviews (KIIs) were conducted out of 25 initially planned.
These respondents consisted of eight representatives of the MoH, seven international partners and donors, three staff members of the Ministries of Education and Public Services, and two representatives of civil society. Two private media organisations were contacted to obtain records of political speeches, events and conferences covering the period between March 2014 and December 2016, corresponding to the time between the start of the Ebola outbreak and the agenda-setting of the post-Ebola HSS programme in Guinea (table 2).
Details of data sources, June 2018, Guinea
Data analysis
The audio recordings and those from the KIIs were completely transcribed, encoded manually and grouped according to the elements of the Kingdon framework.8 We then analysed the transcripts using a thematic analysis approach according to a code grid.25 We compared the data from the different sources (media records, key informants, audits' reports) to triangulate the data and thus strengthen the internal validity (credibility) of the study.25 We addressed inter-coding bias by having three researchers coding the material and allowing for adjustment on team consultation.
Ethics approval and consent
Ethical approval for this study was granted by the National Ethics Committee for Health Research of Guinea (number: 076/CNERS/17). Informed consent was obtained from all respondents and respondents’ anonymity was protected using codes during the data analysis.
Patient and public involvement statement
This study did not require the involvement of patients. Thus, a patient informed consent was not necessary to conduct this study.
Results
The problem stream: mistrust and fear
According to the study participants, the Ebola outbreak was the crucial event that prompted the HCWs' issue to be on the top of the political agenda both nationally and internationally.
Some participants reported that the Ebola outbreak raised political attention to the health sector by rapidly spreading to and in Conakry, where important policymakers live (KII-20; KII-9). This political attention was driven by the realisation that everyone could be infected, with no regard of their social or economic class (KII-10). From a political viewpoint, the outbreak generated a social crisis and great distrust between the government and the communities as they (the government) were perceived to be disseminating the disease for economic interest (the so-called “Ebola business”) (KII-6; KII-11).
…The Ebola epidemic created a deeper mistrust between government officials and communities… at that moment, no official dared to travel to the countryside in administrative vehicles… (KII-6).
…The Womey (Womey is a small village located in Nzérékoré recognized as one of the reluctance areas to the Ebola outbreak awareness campaigns… A few moments after the reception of officials, their tribune was invaded by a group of women booing “leave, there is no Ebola home’ and asking men to respond to 'enemy' attacks who have “deliberately brought Ebola home’. This event took place in September 2014.) massacre is an illustration of the social crisis caused by Ebola… eight of the government officials and health (care) workers who went there for an awareness campaign against Ebola were murdered by an angry (and misinformed) community… (KII-11).
Other participants argued that the occurrence of EVD outside Guinea created tensions with its neighbouring countries which, in turn, impacted international trade and the national economic system (KII-3; KII-7). As the fear of EVD affected all countries in the world, some of these countries either forbade their citizens or airlines from travelling to West Africa or closed their land borders shared with the affected countries (KII-11; KII-14; KII-18).
…Women from Timbi Madina usually harvest potatoes and sell them in Senegal. Today, all these products rot in Guinea because the Senegalese have decided to close their border while it is us who feed them… (media records, Alpha Conde, President of Guinea, Guinea, November 2014).
Ebola has had a heavy burden on Guinea, Liberia and Sierra Leone. In addition to carrying thousands of lives, the virus has destroyed economies, health systems, social structures and families, destroying many years of development gains. (media records, Jim Yong Kim, President of the World Bank Group, Guinea, December 2014).
The policy stream: recruiting HCWs for a resilient health system
According to study participants, a key element enabling the agenda-setting of this policy is the changing practice of development cooperation partners regarding health financing, especially payment of staff salaries. Before the Ebola outbreak, partners would temporarily contract staff in their projects and propose to the government to recruit them afterwards without taking into account the state’s fiscal capacity. According to participants, partners such as EU and WB have allocated substantial budget support to the MoF to sustain post-Ebola reforms including HCWs' recruitments and salary payments (KII-2; KII-19). However, some participants reported that this financial support is conditional on the achievement of certain indicators, for example, ensuring a retention rate of new HCWs of more than 80% in rural health districts (KII-11; KII-19).
…The problem of human resources was known by everyone without investing in it… Partners rather provided other inputs of the system such as medications and vaccines but would exclusively leave salary payments to the government… (KII-2; KII-9; KII-20).
We (currently) receive European Union budgetary support conditional to the achievement of certain indicators… The human resources line is about 2 million Euros per year but to get this fund, we need to ensure the retention rate of the newly recruited (HCWs) in rural areas is 80%… (KII-2; KII-11; KII-19).
According to some participants, the availability of external funding for the Ebola control programme was among the proposed solutions to start recruiting additional HCWs (KII-9; KII-11). These participants reported the availability of remaining funds mobilised by donor countries and institutions for the fight against Ebola. From their perspective, policymakers and development partners were highly receptive to the use of these remaining funds for the future implementation of health systems' policies designed in the post-Ebola environment.
Additionally, the Ebola outbreak allowed the training and contracting of staff across all levels of the health system, especially in underserved areas (KII-2; KII-13). This made all actors agree that the recruitment of this staff by the MoH would strengthen the health system in the short term (KII-1; KII-8; KII-15). Some international partners even made governmental recruitment of contracted staff a condition for mobilising funds in support of the post-Ebola health system recovery plan.
…Partners temporarily recruited staff for Ebola control and asked the government to employ them (as civil servants)… We were forced to do so and that is why there was this additional list (of recruited staff) who worked in the Ebola response… (KII-6; KII-11).
Nevertheless, participants reported that the unpredictability of external funds was an important hindrance in sustaining this policy (KII-2; KII-12).
The politics stream: managing risks
Two main factors might explain the receptivity of politics for this agenda-setting: external and internal factors.
First, at a global level, the high perception of EVD-related risks led to considerable fundraising to support EVD-control activities and, beyond the outbreak, sustain reforms for strong and resilient health systems. Moreover, a converging point for actors interviewed was the catastrophic cost of managing the outbreak compared with what the system required for its reforms (KII-9; KII-11; KII-18).
…Guinea, by making prevention efforts in fighting the Ebola outbreak, averts the whole world (and thus France and Europe) from being contaminated by this terrible virus. (media records, François Hollande, President of France, Guinea, November 2014.)
Second, at a national level, this policy resonated with a political agenda, which, apart from taking advantage of it for vote-seeking purposes, had seen it as an opportunity to attract more funding to the country.
…The end of Ebola corresponded to another presidential term, so launching a recruitment process was strategically advantageous for the President… It could help on the electoral side but also to ease the social tensions generated by Ebola… [KII-2; KII-8].
Plausibly, the social crises in addition to the faltering national economy triggered by the Ebola outbreak had changed the political perception of health issues.
Yet, an obstacle has been identified in the politics stream relative to political instability at the MoH. Illustratively from 2014 to 2018, in the period during and after the Ebola outbreak, there was the turnover of four health ministers along with two important cabinet reshuffles (KII-3; KII-19). This high turnover could have been linked to the preparations of the presidential (2015) and legislative (2018) elections, or the implementation of the resulting electoral agreements (KII-3; KII-17).
Policy windows: funding and fiscal space for investing in HCWs for remote areas
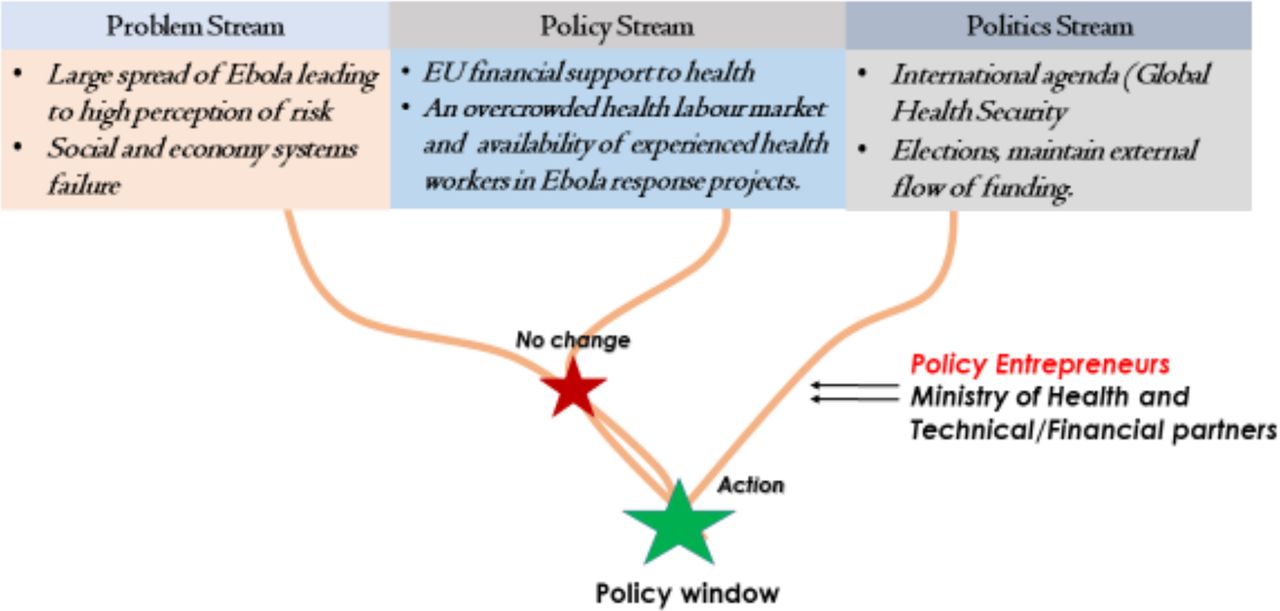
As stipulated by Buse et al, policy entrepreneurs play a substantial role by linking the problem with possible solutions and creating a political momentum for policies’ agenda-setting (figure 1).27 In this case study, the Ebola outbreak was the enabling event that generated opportunities for actors in the health sector to propose solutions for national health system reforms. In June 2014, following the declaration of the Ebola outbreak, a national conference on health was organised. Although aimed at revising the national health policy and development plan, policy entrepreneurs — actors of the MoH and technical and financial partners such as WB, WHO and UNFPA — quickly used this momentum, through a health system assessment, to attract the attention of high-level politicians such as the President of Guinea and representatives of the European Union (EU) in Guinea. This conference quickly turned into a commitment for an emergency need to strengthen the national health system.
{kind=link}
Kingdon’s policy window and three streams applied to healthcare workers' policy in Guinea.8
…You have to be blind not to see that our health system is sick… as macroeconomic performance changes, the state will play its role in improving health financing… (media records, Alpha Conde, President of Guinea, Guinea, June 2014).
…Health financing is weak even out of norms… I reaffirm the commitment of my Institution to continue efforts through the 10th European Development Fund (EDF) which grants Guinea 20 million Euros… we are available to continue and consolidate the on-going efforts under the 11th EDF… (media records, Gerardus Gielen, EU representative in Guinea, Guinea, June 2014).
Afterwards, a health sector committee and a thematic group on human resources for health were established to update national health policies and develop the HSS policy. These platforms were predominantly composed of technical and financial partners — all advocating for rural staffing projects — and national institutions such as the Ministries of Health, Education, Decentralisation, Public Services and Finances.
Via this HSS programme, 5000 HCWs have been recruited (an increase in the HCW ratio per 1000 inhabitants from 0.73 in 2014 to 1.18 in 2019), deployed in rural areas and their salary increased by 40%. In addition, 33 centres for epidemic treatment and prevention have been constructed across all health districts and a network of laboratories for infectious diseases' surveillance established. Furthermore, several health centres have been rehabilitated and logistics support provided to health districts for field activities, such as vaccination campaigns and training, and local contracting of 10–15 community health workers per sub-district for potential epidemic diseases surveillance. Finally, a national agency for health security was established to coordinate eight regional and 33 prefectural teams to manage alerts and respond to epidemics.
To support the salary payment of the 5000 newly recruited HCWs, government health expenditure has increased from 4% in 2015 to 8% in 2017 partly resulting from the EU and the WB financial support for the HSS policy (KII-2; KII-11). Actual salary payment is being controlled by the MoH representatives at the district level.
A governance structure for HRH, the National Directorate of Human Resources for Health, has been created at the MoH with more responsibilities in the planning of HCWs' recruitment, supervision and management.
However, some obstructions have remained in sustaining the policy momentum. First, the government investment plan in the health sector has not been executed as planned in 2015. According to participants, the budget allocated to the health sector should have increased from 8% in 2017 to 10% in 2018 and eventually to 15% in 2020 to sustain a progressive health system development (KII-5; KII-9). However, the government health expenditure to date (July 2019) remains at 8%. It is possible that the policy window has closed as political priorities are directed towards improving other sectors such as electricity and road networks which malfunctioning constitute the main reason for social protests (KII-6; KII-10). Second, the MoH deals with both the supervision of HCWs and their salary payment. In the context of international pressure (medium- and long-term external financial support to the health sector is conditional) and poor health financing and governance, such issues might create a conflict of interest within the MoH (KII-2; KII-9). This might distort the correct reporting of the HCWs' retention rate (KII-9). Assigning HCWs' salary payment to local communities would have contributed to accelerating Guinea’s path towards the decentralisation of the health system (KII-9; KII-11; KII-13). Third, the policy window generated opportunities for health coverage expansion for epidemic preparedness and response incompatible with communities’ financial affordability at the point of care — as the Ebola outbreak hampered an already low-health services attendance and utilisation in Guinea.28–30 This may not favour the synergistic scope of GHS and UHC.1
Discussion
This article draws on Kingdon’s multiple streams theory of agenda-setting to understand the role of policy actors and the processes by which the health sector became prioritised in Guinea after the Ebola outbreak. Our analysis shows that the generation of opportunities for health system reforms in a poor-resource setting is substantially linked to the 'problem framing' and how this is influenced by international actors. By crossing West African borders, the Ebola outbreak became a threat to global health security and put the spotlight on the necessity for building a resilient national health system. Additionally, it confirms the fact that policy entrepreneurs should prioritise the alignment of proposed policy change between the national (socio-economic and political) and international actors’ interests. Finally, in the HSS programme, disproportionate attention was given to health coverage expansion for epidemic preparedness and response in comparison to health reforms aimed at reducing the financial inaccessibility of essential healthcare.
While other studies8 31 report that poor health indicators and epidemics often shift health policy agenda-setting, our study revealed that it is mainly epidemics triggering trans-national impacts that prompt political actions towards the national health sector. One plausible explanation of this finding could be the lack of political prioritisation of the health sector and international financial support for national health initiatives. For instance, besides the multiple challenges the Guinean health system faced a decade ago in achieving international targets (such as the Millennium Development Goals and UHC), the national budget allocated to health remained low (3%) compared with other sectors such as defence (10%) and decentralisation (8%). Additionally, despite its significant contribution to the health system, external funding was hardly used to support the budget allocated to the health sector – it was used rather to run temporary donors’ projects. Also, because of bureaucracy, incoherent programming of activities and delays in reception of funds from the MoF, only approximately half of the national budget allocated to health is absorbed and executed.21 Second, diseases associated with excess mortality and threats which affect nations regardless of their social or economic levels facilitate mobilisation of external financial resources.10 32 By spreading to nations such as Spain and the United States, the Ebola outbreak prompted Western governments to provide financial support in strengthening the West African health system to make it resilient.33 Moreover, the possible use of the Ebola virus for bioterrorism purposes, given its high mortality rate and lack of effective treatment, could also explain this result.34
As stated by Buse et al,27 politicians buy into solutions that coincide with their interests. Our finding shows that international support in the agenda-setting of a health policy does not solely suffice for its effective implementation. Rather, the policy agenda-setting has to comply with national actors’ interests. For instance, several rural staffing projects initialled in Guinea by the WB and the UNFPA have been confronted with political reluctance during their implementation phase — when it comes to the application of clauses such as the recruitment of contracted HCWs by the MoPS.21 However, post-Ebola HSS programme actions that were fully implemented included: direct recruitment of HCWs who worked in the Ebola response; HCW salary increase by 40%; massive deployment of HCWs in rural settings; and governmental health budget increase to 8%.24 Several possible explanations exist for this finding. First, the social instability generated by the Ebola outbreak might have hindered national security objectives along with the state actors’ political power. Additionally, the Ebola outbreak caused an estimated loss of USD 600 million to the economic system.35 External financial support to the health system could have been perceived by state actors as a springboard for the boost of economic and political plans. Second, from a global health perspective, this financial support served to implement policies such as raising epidemic awareness which could reduce the perceived risk felt by Western citizens.36 McPake et al in their estimates of fiscal space projections in West African Ebola-affected countries report a declining projection (6%) of total health expenditures between 2020 and 2030 in Guinea.37 This suggests that policy actors in the MoH should develop strategies to overcome this situation which may impede the achievement or sustainability of the current GHS goals.37 Therefore, they should prioritise efficiency management of HCWs by decentralising recruitment, removing ghost workers and communicating effectively on the outcomes of HSS on health indicators. They should also foresee a scenario building on a potential resurgence of an Ebola outbreak, that might occur as a result of a reduction of health expenditure, including its socio-economic and political implications.
This study analyses that epidemic preparedness and response were highly prioritised in this HSS programme, although financial inaccessibility to healthcare remains the bottleneck to expanding health services coverage in Guinea. In early 2013, studies revealed a decline of healthcare utilisation as a result of increased spending on healthcare: the high cost of care, out-of-pocket expenditure and private practice within the public sector (for example, the sale of private pharmaceutical drugs).21 To date (2019), initiatives aiming at protecting the population against financial barriers to accessing care include free obstetrical care (antenatal care, delivery and caesarean section), provision of antiretroviral HIV-treatment, management of malaria, tuberculosis and leprosy, and vaccination. However, the implementation of these policies, particularly those of obstetrical care and malaria management, encounter several dysfunctions including lack of necessary support measures (financial and human resources), lack of equipment and medicines, and delays or irregular transfers of subsidies to health facilities.38 39 These facts have led to ignoring free-cost policies and the existence of non-official pricing which may be 10 times higher than government set prices.21 Notwithstanding this evidence, investments in the post-Ebola period have not helped to advance these issues. One plausible reason for this could be the lack of advocating policy entrepreneurs. As stated by Kingdon, the technical and financial feasibility of policies highly influence their agenda-setting.8 The promotion of social health insurance, to be put back on the political agenda in Guinea after 20 years, still faces challenges of technical appropriation, coverage of populations, dissatisfaction, financial inability to honour contributions and underfunding by the state.21 As a result, until 2019, only 7200 people were covered by a mutual-type social insurance system.35 The successful scale-up and implementation of complex interventions such as a national social health insurance require active engagement and financial support of state actors.1
This study raised several questions related to policy window sustainability. The on-going research on the follow-up of rural deployment of HCWs recruited in the post-Ebola HSS context should provide more evidence on this.
Study limitations
This study suggests some potential limitations of Kingdon's agenda-setting theory which should be taken into account in health policy and system research in a similar context. First, Kingdon described his framework as a result of three distinct and independent streams. Our research revealed an interdependent function between the streams: the construction and ‘framing’ of the problem strongly impact on the policy and politics streams.40 Second, the Kingdon framework, with an original focus on agenda-setting issues in the United States, tends to minimise the role and power of international agendas and actors. This framework describes policy entrepreneurs as national actors with greater ‘independent’ power to push issues to the top of agendas.
Moreover, the study has some limitations. First, our target population for this study (actors included in national policies development, and the agenda-setting of this HSS programme) was limited. This represents a methodological weakness as it might have impacted on data saturation. Moreover, we could not interview key informants from the Ministries of Finances and Budget. This hampered our analysis on the government financial contribution to this policy agenda-setting and sustainability. Second, the Ebola epidemic was unique to West Africa and the international community. Thus it might be disproportionate to compare an agenda-setting process in this context with other epidemics. Third, our context analysis excluded data sources dated before 2000 which might have narrowed our timeframe analysis. However, to our knowledge, this is the first study to use Kingdon’s theory to explain why the Ebola crisis generated a political prioritisation of the health sector in Guinea and, thus, might contribute to generating evidence on health policy agenda-setting in the WestAfrican region and beyond.
Conclusion
Our study highlights that the international health security agenda was the main enabler of the current HSS programme agenda-setting in Guinea. And as such, this programme mainly focuses on epidemic preparedness and response, leaving aside issues related to the overall healthcare affordability. External financial support has importantly contributed to creating the momentum for political prioritisation of the health sector but the donor dependency character of the current programme, and also the high turnover of cadres at the MoH, were identified as potential threats to the sustainability of this programme. It is unlikely that investments in GHS will lead to advancing UHC and social protection issues in Guinea because of the lack of active policy advocates and the engagement of state actors. There is a need for a shared responsibility between national governments and the international community,thereby sustaining the current HSS programme in Guinea.
Footnotes
Handling editor Seye Abimbola
Contributors DK, AD, RvdP and WVD conceived and designed the study and received feedback from AHB, AK and AMD. DK, AD, RvdP, ND and PB were involved in data acquisition, analysis and interpretation, and revising it critically for important intellectual content. DK drafted the manuscript with inputs from AD, RvdP, WVDP, AHB and WVD. All the authors have given final approval for the version to be published.
Funding This study is financed as part of a Fourth Framework Agreement (FA-IV) programme (2017–2022) between the Belgian Directorate of Development Cooperation and government of Guinea pertaining to scientific capacity building.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available in a public, open access repository. Data are available upon reasonable request. Data may be obtained from a third party and are not publicly available. All data relevant to the study are included in the article or uploaded as supplementary information.