Article Text

Abstract
Introduction Tanzania is one of the 14 priority countries in sub-Saharan Africa scaling up voluntary medical male circumcision (VMMC) for HIV prevention. In this study, we assessed the progress of VMMC by evaluating changes in the spatial structure of male circumcision (MC) prevalence and identifying age groups with low MC uptake.
Methods We use data from two waves of the Demographic and Health Survey (DHS) conducted in Tanzania in 2011–2012 and 2015–2016. MC incidence rate was estimated using a method developed to calculate incidence rates from two successive cross-sectional surveys. Continuous surface maps of MC prevalence were generated for both DHS waves and compared with identified areas with high MC prevalence changes and high density of uncircumcised males.
Results National MC prevalence in Tanzania increased from 73.5% in 2011–2012 to 80.0% in 2015–2016. The estimated national MC incidence rate was 4.6 circumcisions per 100 person-years (py). The lowest circumcision rate was observed in males aged 20–24 years, with 0.61 circumcisions per 100 py. An estimated 1 567 253 males aged 15–49 years residing in low-MC prevalence areas were uncircumcised in 2015–2016.
Conclusion Tanzania has shown substantial progress in the implementation of VMMC. However, extensive spatial variation of MC prevalence still exists in the country, with some areas having an MC prevalence <60%. Here, we identified locations where VMMC needs to be intensified to reach the ~1.5 million uncircumcised males age 15–49 living in these low-MC areas, particularly for men aged 20–34.
- geographic information systems
- HIV
- cross-sectional survey
- public health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Tanzania was among the first countries to establish a national voluntary medical male circumcision (VMMC) programme in 2009, with the goal of reaching about two million circumcised males focusing in the northwestern region of Tanzania, where only about 26% of males are circumcised.
What are the new findings?
While Tanzania has shown impressive progress in the implementation of VMMC, reaching the desired national level of 80% male circumcision (MC) prevalence, there is still extensive spatial variation of MC prevalence in the country, with some areas having MC prevalence below 60%.
Most circumcision procedures were performed in male adolescents aged 15–19 years, with more than 13 circumcisions per 100 person-years (py), but males aged 20–24 years had low VMMC uptake with less than one circumcision per 100 py.
A total of 2 514 724 males aged 15–49 years are still uncircumcised in Tanzania; among these males, 1 567 253 (62.3%) reside in only eight districts, comprising 20.2% of the total area of the country.
What do the new findings imply?
There are still several barriers for VMMC that need to be overcome, particularly for males aged 20–34 years, who are vulnerable individuals at high risk of HIV infection but low MC uptake.
Therefore, efforts need to be oriented towards the male population located in high-HIV burden areas with low MC prevalence.
Introduction
In 2007, the WHO and the Joint United Nations Programme on HIV/AIDS (UNAIDS) acknowledged that male circumcision (MC) should be considered a key programme intervention for HIV prevention.1 2 Accordingly, UNAIDS launched the ‘Joint Strategic Action Framework to Accelerate the Scale-Up of Voluntary Medical Male Circumcision (VMMC) for HIV Prevention’ in eastern and southern Africa, where it was expected to have the highest impact. As a result, 14 countries in sub-Saharan Africa have implemented VMMC programmes designed to achieve 80% circumcision prevalence among males aged 15–49 years.3
In 2009, Tanzania was among the first countries to establish a national VMMC programme. The programme goal was to increase MC by 2017, specifically to about two million circumcised males aged 10–34 years,4 the age group for which MC was predicted to achieve the greatest impact at preventing HIV infections.5 Previous studies have identified substantial variability of MC prevalence in Tanzania.6 MC prevalence in the eastern part of the country is as high as 95%–100%. Conversely, only about 26% of males in the southwestern region of Tanzania, including the districts of Rukwa, Songwe and Mbeya, are circumcised,7 8 which also is the area with the highest burden of HIV.9 10 Hence, Tanzania has been scaling up MC services in areas where MC prevalence is low and HIV prevalence is high. Therefore, an updated evaluation and spatiotemporal assessment of programme effectiveness in terms of current and recent trends in MC prevalence in Tanzania are needed.
In a previous study, we used data from the Tanzania Demographic and Health Survey (TDHS) conducted during 2003–2004, 2007–2008 and 2011–2012 to investigate spatial and temporal patterns in MC prevalence.6 The current study updates results to 2015–2016 and compares them with MC prevalence in 2011–2012. Using two nationally representative surveys conducted in 2011–2012 and 2015–2016 in Tanzania, we implemented a geospatial analysis to evaluate the impact of the national VMMC strategy on the spatiotemporal dynamics of MC prevalence in Tanzania. We aimed to identify age groups with low MC prevalence, as well as changes in the spatial structure of the MC prevalence distribution to identify areas where vulnerable male populations lacking MC reside and where access to and/or use of VMMC health services could be improved.
Methods
Data sources, prevalence estimation and spatiotemporal analysis
We obtained data from the TDHS conducted in 2011–201211 and 2015–2016.12 TDHS conducts surveys about every 5 years with large sample sizes (usually over 5000 households) to collect nationally representative data while using standardised procedures to ensure comparability of results over time. These two TDHS surveys enrolled subjects by using a two-stage sampling procedure to select households and to reduce sampling errors. Stratification occurred by separating each region into urban and rural areas. The primary sampling unit (PSU) used for the first stage of selection was a census enumeration area (EA) or a subset of an EA. The 2015 TDHS used information from the 2012 Tanzania Population and Housing Census to generate a sampling frame. In rural areas, a PSU is a village, a portion of a large village or a group of small villages, whereas a PSU is a street or a city block in urban areas. In the first stage, 608 PSUs (180 PSUs were from urban areas and 428 PSUs were from rural areas) were selected with probability proportional to the PSU size (figure 1). Many past Demographic and Health Surveys sampled a fixed number of households per PSU (about 25–30 households); for the 2015 TDHS, 22 households were systematically selected from the sampling frame for each PSU. Additionally, TDHS includes sampling weights at the household and individual levels in order to restore representativeness of the sample and to prevent bias due to oversampling and undersampling, depending on region population size. A total of 10 040 and 12 563 households were included in the survey in 2011–2012 and 2015–2016, respectively. Males and females in the selected households aged 15–49 years were eligible to participate. Because our focus was on the prevalence of MC, female participants were excluded from both surveys to generate the dataset to conduct our analysis. Our final dataset consisted of 8352 males (89% participation rate) from the 2011–2012 TDHS and 3514 males (92% participation rate) from the 2015–2016 TDHS.

Geographical sample locations for the Tanzania Demographic and Health Survey conducted in 2011–2012 and 2015–2016. Maps were created using ArcGIS by Esri V.10.5 (http://www.esri.com),21 and basemaps were obtained from Esri and National Geographic, available at ArcGIS Online basemaps.22
The binary answer to the question ‘Is the respondent circumcised?’ was used as the measure of MC status. Further details related to the TDHS methodology, study design and data can be found elsewhere.11 12 National MC prevalence in Tanzania for all males and by the 5-year age group was estimated for both surveys.
MC incidence rates were calculated during the two time periods (2011–2012 and 2015–2016) using a methodology developed to estimate HIV incidence from data on HIV prevalence,13 but the method can be applied to estimate the incidence of MC. Briefly, this method estimates incidence (MC incidence in this study) using two cross-sectional surveys conducted at different time periods, under the assumption that observed changes in prevalence over time can be decomposed into contributions due to incident cases and mortality. Individuals of age a years in the first survey correspond to individuals aged a+γ in the second survey, where γ is the time interval (in years) between surveys. Therefore, the change in MC prevalence between these two age groups could be attributed to the combination of new circumcisions and mortality. Age-dependent mortality rates were obtained from the WHO Global Health Observatory data repository.14
Spatiotemporal dynamics of MC
We used the MC cold spots identified in our previous study to define areas with low MC prevalence in Tanzania in 2011–12. The method used to identify geographical regions with low MC prevalence in Tanzania and an epidemiological description of these regions are detailed elsewhere.6 The current study updates and extends the investigation to 2015–2016 and compares this time period with 2011–2012 to investigate the impact of the VMMC programme to increase MC prevalence by 2017.
Briefly, we used spatial scan statistics for the detection of local areas (clusters) that have lower numbers of cases (ie, circumcised males) than expected under the assumption of a spatially random distribution of cases. For this analysis, we aggregated the numbers of circumcised (cases) and uncircumcised (controls) males and chose the Bernoulli model for cluster detection implemented in the SaTScan15 software for the detection of statistically significant clusters with low numbers of uncircumcised males (MC cold spots). The software uses a scanning window (predefined here to be circular and non-overlapping) that moves systematically across geographical space and with varying radius. The statistical significance of potential clusters was determined by gradually traversing the study region with circular windows.16 The circular windows varied continuously in both location and radius. The radius ranges from slightly above 0 km to a fixed maximum value, thus creating and testing a large number of distinct potential clusters throughout the study region. A maximum radius that covered 50% of the study region was used. Each potential cluster was tested using a likelihood ratio test to determine the statistical significance against the null hypothesis of spatial randomness.15 Clusters with a p value of <0.05, calculated using Monte Carlo simulations, were identified as statistically significant MC cold spots. Lastly, differences of MC rates within and outside the MC cold spots of the two sampled years were examined.
Continuous surface maps of MC prevalence in 2011–2012 and 2015–2016 were generated to identify spatial and temporal changes in the MC prevalence distribution. First, the prevalence of MC was estimated at each TDHS sample location. MC prevalence (pMC) at location i was defined to be pMCi=ni/ Ni, where ni denotes the number of circumcised males and Ni denotes the total number of males at location i. Second, kernel interpolation was used to generate continuous surface maps of MC prevalence.17 Each map was generated in raster format of 5×5 km pixel resolution. Third, spatial differences in the MC prevalence over time were estimated by comparing the MC prevalence maps generated for 2011–2012 and 2015–2016.
Density map of uncircumcised males
The WorldPop database18 19 was used to extract estimates of the 2015 population density in Tanzania in the form of a raster image with a resolution of 100×100 m pixel. For consistency with the resolution of the MC prevalence maps generated in this study, we reduced the resolution of the raster file to 5×5 km pixel. Population density maps for males aged 15–49 years were generated using estimates from the Tanzania Population Distribution by Age and Sex Report.20 Lastly, a 5×5 km pixel resolution map of the density of uncircumcised males was generated by multiplying values from the males aged 15–49 population density map with values from the MC prevalence map for 2015. Maps were created using ArcGIS by Esri V.10.5 (http://www.esri.com),21 and basemaps were obtained from Esri and National Geographic, available at ArcGIS Online basemaps.22
Patient and public involvement statement
There were no patients involved in this research.
Results
General results
The national MC prevalence in Tanzania increased from 73.5% (95% CI 72.5% to 74.4%) in 2011–2012 to 80.0% (95% CI 79.3% to 81.9%) in 2015–2016. Figure 2A presents the MC prevalence by age group in 2011–2012 and 2015–2016. MC prevalence increased over time for all age groups, and the MC prevalence was >70% for all age groups in 2015–2016. The largest increase in MC prevalence was observed in males aged 15–19 years, from 67.7% in 2011–2012 to 81.3% in 2015–2016.

MC prevalence by age group in 2011–2012 (blue bars) and 2015–2016 (orange bars) (A). MC incidence per age groups (B). MC, male circumcision.
In terms of incidence, the estimated national average was 4.6 circumcisions per 100 person-years (py). The highest incidence was identified in males aged 15–19 years, with 13.2 circumcisions per 100 py, followed by males aged 25–29 years, with 9.9 circumcisions per 100 py (figure 2B). The lowest circumcision rate was observed in males aged 20–24 years, with only 0.61 circumcisions per 100 py.
Spatiotemporal dynamics of MC
Maps of the spatial distribution of MC prevalence are presented in figure 3 for 2011–2012 (figure 3A) and 2015–2016 (figure 3B). In general, eastern Tanzania had high MC prevalence above 80%. Conversely, northern and southwestern Tanzania had a substantially lower MC prevalence. Comparing the continuous surface maps generated for the distribution of MC in 2011–2012 (figure 3A) and 2015–2016 (figure 3B), we estimated that the area of the country with at least 80% MC prevalence increased from 43.7% in 2011–2012 to 54.5% in 2015–2016, while areas with MC prevalence lower than 60% declined from 31.1% to 15.9% of the total area of the country over time (figure 3C).
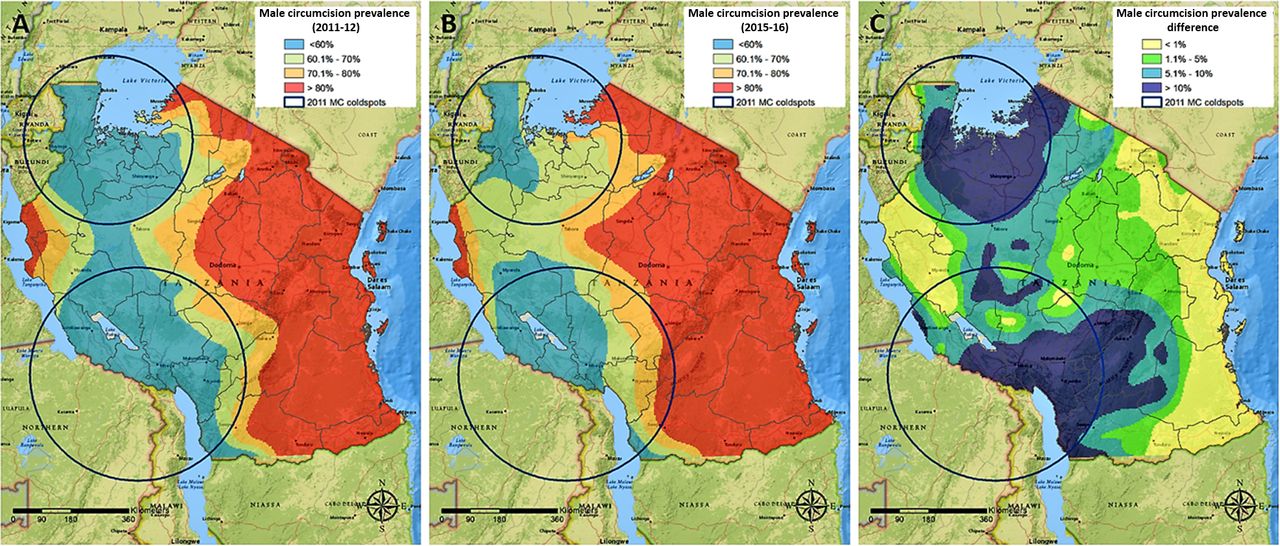
Continuous surface maps of MC prevalence in Tanzania in 2011–2012 (A) and 2015–2016 (B) and the difference in MC prevalence (C). Blue circles indicate the location of the MC cold spots identified by spatial scan statistics. Maps were created using ArcGIS by Esri V.10.5 (http://www.esri.com),21 and basemaps were obtained from Esri and National Geographic, available at ArcGIS online basemaps.22 MC, male circumcision.
We estimated that 43.3% of the country had at least a 10% increase in MC prevalence over time (figure 3C). Areas with the largest gains in MC prevalence were located in the MC cold spots identified in a previous study6 (figure 3C, blue circles). MC prevalence within the cold spots significantly increased from 42.5% (95% CI 40.8% to 44.2%) in 2011–2012 to 58.4% (95% CI 55.7% to 61.1%) in 2015–2016 (p<0.05), while the MC prevalence outside the cold spots remained stable over time (93.7% in 2011–2012 and 93.9% in 2015–2016). Some areas located in the districts of Songwe, Geita and parts of Kagera showed a noticeable increase in MC prevalence over time. However, there were areas within the cold spots located in the districts of Kagera and Rukwa that still had substantially low MC prevalence (~40%) after implementation of the VMMC programme. Similarly, the MC prevalence in the southern area of the Rukwa district, the area with the lowest MC prevalence of the southern cold spot, did not increase from 2011 to 2016.
Density map of uncircumcised males
We estimated that a total of 2 514 724 males aged 15–49 years were uncircumcised in Tanzania in 2015–2016 (figure 4). Among these males, 1 567 253 (62.3%) reside in eight districts located within the MC cold spots, comprising 20.2% of the total area of the country. The districts of Rukwa, Songwe and Mbeya located within the MC cold spot at the western part of the country were home to 21.5% of the total male population lacking circumcision, whereas the districts of Kagera, Geita Mwanza, Shinyanga and Simiyu, located within the MC cold spot at the northern part of the country, contained 40.8% of the total uncircumcised males in Tanzania in 2015–2016.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Density distribution of uncircumcised males in Tanzania in 2015–2016. Maps were created using ArcGIS by Esri V. 10.5 (http://www.esri.com),21 and basemaps were obtained from Esri and National Geographic, available at ArcGIS online basemaps.22
Discussion
Tanzania has made substantial progress towards UNAIDS strategic goals for MC coverage since the implementation of the Tanzania National Strategy for Scaling Up Male Circumcision plan. As a result, the national MC prevalence increased from 74% in 2011 to 80% in 2016. The largest increase in MC prevalence was observed in areas with the greatest need (MC cold spots), where MC prevalence increased from 43% in 2011 to 58% in 2016. However, this MC prevalence is far from the desired 80% coverage in these areas.
According to our results, MC prevalence has increased in all age groups from 2011 to 2016, and MC prevalence was >80% in males aged 15–34 years. Estimates of MC incidence indicated that most circumcision procedures were performed in males aged 15–19 years, with more than 13 circumcisions per 100 py, followed by males aged 25–29 years, with more than 10 circumcisions per 100 py, a result that is consistent with the strategic plan of the country to target males aged 10–34 years.3 However, the lowest MC incidence was observed in males aged 20–24 years, with less than one circumcision per 100 py, which is much lower compared with age groups that were not prioritised in the VMMC strategy in Tanzania (males aged 35–39 years and 40–44 years, with about two circumcision per 100 py). These older males usually perceive themselves as low-risk individuals for HIV infection and thus are relatively less receptive to VMMC.4 The estimated low MC incidence in males aged 20–24 years can be associated with previous findings in which most VMMC clients in Tanzania were younger males, with about 76% of VMMC performed for males under 20 years of age in 2014.23 24
Previous studies have been conducted to identify reasons for a disproportionate age difference in VMMC and the barriers that prevent males older than 20 years to have VMMC. Barriers identified included myths regarding loss of sexual competence post circumcision and inadequate service delivery, in addition to concerns about abstinence in the postsurgical period, loss of income and fear of pain associated with postsurgical erections. As males get older, the cost of circumcision increases; however, stakeholders from the Ministry of Health and Social Welfare in Tanzania ensure MC at minimal cost. In addition, older males have expressed concerns about loss of income because the process of circumcision takes time.25 26 Moreover, financial, social and cultural perceptions place barriers on older males seeking MC. For example, older males preferred services provided after work hours or on weekends, and they were concerned about lack of privacy and feeling stigmatised when they encounter a younger man in a medical setting that includes predominantly adolescent clients.25 27 The underlying cultural perception is that MC is most appropriate before or during puberty. Thus, older males prefer separate services that do not accept younger clients.25–27 Sexual concerns for older males are related to partner infidelity during the postsurgical abstinence period and fear of pain associated with postsurgical erections, in addition to the myth regarding loss of sexual competence.25 26 28 Moreover, across multiple locations, VMMC has been perceived as shameful for older males and/or married males.25 29 As our results suggest, these barriers could negatively affect VMMC uptake for individuals aged 20–25 years, a sexually active group that is vulnerable to high incidence of HIV infections. Therefore, males aged 20–24 years should be targeted to overcome these barriers to enhance VMMC uptake.
We estimated that 55% of the total area of the country had an MC prevalence above 80%, and more than 41% of the total area of the country had more than 90% of males circumcised by 2016. Conversely, 16% of the total area of the country had an MC prevalence below 60%. Such extensive variation of MC prevalence generated by areas with almost universal MC prevalence inflates the national MC prevalence, masking the low MC prevalence in the western part of the country, a region that is still far from achieving the 80% MC prevalence goal.
Despite the significant increase in MC prevalence in the low prevalence districts, there is still a large number of uncircumcised males aged 15–49 years in these areas. We estimated that more than 62% of the uncircumcised males aged 15–49 years in Tanzania are concentrated in eight districts, five of them previously prioritised for VMMC, namely, Rukwa, Mbeya, Kagera, Mwanza and Shinyanga. We also identified three districts, Songwe, Geita and Simiyu, in which VMMC services should be intensified. These geographical areas displayed a high density of uncircumcised males, identifying the locations in need of VMMC programme intensification and the implementation of strategies aimed to overcome barriers for MC healthcare use. These areas were previously identified as high-HIV incidence areas for females.6 Therefore, an important strategy that can be strengthened in these regions is the expansion of the role of females in VMMC uptake strategies,30 such as counselling and education services to female partners of VMMC clients. Several studies have shown that females influence their partners’ decision to be circumcised.30 31 Therefore, involving females in VMMC campaigns would allow them to play a key role to reach and persuade their male partners to enhance VMMC uptake in these low-MC prevalence areas.
Several study limitations could have affected our results. Given the multiple logistical difficulties in conducting the TDHS, some of our measures could have been affected by inherent biases in the data, such as the variability in response rates and undersampling of mobile individuals and key male subpopulations at risk.32 33 Moreover, the methodology used to calculate MC incidence rate and prevalence changes over time did not take into account migration, and the sources of data used did not include information regarding mobile individuals. Estimates of regional MC incidence rate and prevalence changes could be affected by patterns of migration. It is not clear though whether the inclusion of mobile populations could affect our findings, and it would be necessary to include more determinants to address the potential impact of migration.34 An additional potential bias is the global positioning system displacement process of the TDHS sampling data points, used to preserve their confidentiality.35 This process could have an impact on the precision of the geographical location of the MC cold spots by a few kilometres. Lastly, data for circumcised males were derived from self-reported circumcision status rather than physical examination. Some studies have reported the validity of self-reported MC data,36 37 but others have found less satisfactory accuracy, partly due to differences in the amount of foreskin removed, which may vary between populations or by ethnic group.38
Conclusion
In conclusion, Tanzania has shown impressive progress in the implementation of VMMC, reaching the desired national level of 80% MC prevalence by 2016. However, extensive spatial variation of MC prevalence still exists in the country, and although substantial increases in MC prevalence have been achieved in areas where MC prevalence was predominantly low, cold spots with MC prevalence below 60% still persist. Here, we identified locations where VMMC programmes need to be intensified to reach the 1.5 million uncircumcised males aged 15–49 years living in these areas. There are still several barriers for VMMC that need to be overcome, particularly for males aged 20–34 years, who are vulnerable individuals at high risk of HIV infection but low MC uptake. Therefore, efforts need to be oriented towards the male population located in the high HIV burden areas with low MC prevalence in Tanzania.
Acknowledgments
The authors thank Measure Demographic and Health Surveys for releasing these national surveys in the service of science, and the United States Agency for International Development and other donors supporting these initiatives.
References
Footnotes
Handling editor Sanni Yaya
Contributors HK and DFC contributed to the study and its design, conducted the statistical and spatial modelling analyses, and wrote the first draft of the paper. AB and FDWM contributed to the study conception and design, conduct of the statistical modelling analyses, interpretation of the results and writing of the manuscript. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The data that support the findings of this study are available from the Demographic and Health Surveys (http://www.measuredhs.com), but restrictions apply to the availability of these data, which were used under licence for the current study and so are not publicly available. However, data are however available from the authors on reasonable request and with the permission of Demographic and Health Surveys. Procedures and questionnaires for standard Demographic Health Surveys have been reviewed and approved by the ICF International Institutional Review Board (IRB). The ICF International IRB ensures that the survey complies with the US Department of Health and Human Services regulations for the protection of human subjects, while the host country IRB ensures that the survey complies with laws and norms of the nation (http://dhsprogram.com/What-We-Do/Protecting-the-Privacy-of-DHS-Survey-Respondents.cfm%23sthash.Ot3N7n5m.dpuf). We sought and were granted permission to use the core dataset for this analysis by Measure DHS.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available in a public, open access repository.