Article Text

Abstract
Introduction Supportive supervision remains a key challenge to the sustainability of community health worker (CHW) programmes globally. The aim of the study was to identify critical actors and patterns of relationships in the supervision of ward-based outreach teams (WBOT) in a rural South African district.
Methods A cross-sectional study of social and professional relationships of WBOTs with other primary health care (PHC) system actors was conducted using a social network analysis (SNA) approach. A structured questionnaire was distributed to CHWs (37), WBOT team leaders (3), PHC facility managers (5) and PHC local area managers (2) (total n=47) assessing interaction patterns of supportive supervision, namely management, development and support.
Results The supportive supervision system pivoted around team leaders, who were nurse cadres and who ensured internal cohesion and support among WBOT members. The network patterns also showed the extent of peer support between CHWs in WBOTs. PHC facility staff and middle managers in the subdistrict did not appear to play active roles in the supervision of CHWs and their team leaders. However, there were exceptions, with WBOTs drawing on sympathetic cadres identified among the PHC facility staff for support.
Conclusion Supportive supervision of CHWs can be thought of as a system of horizontal and vertical relationships that go beyond just one supervisor–supervisee interaction. In this study, supervisory relationships within teams functioned better than those between teams and the rest of the PHC system. Understanding these relationships is key to designing effective supportive supervision in CHW programmes. SNA can be a valuable approach in identifying the relationships to be strengthened.
- community health workers
- ward-based outreach team
- support
- supervision
- social network analysis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Supportive supervision is critical for the performance and sustainability of community health worker (CHW) programmes.
The performance of CHWs is affected by the quality of their relationships with formal health system actors.
What are the new findings?
Team leaders were critical actors and the main source of supportive supervision for CHWs.
There was dense communication and cohesion among CHWs themselves.
Although there were notable exceptions, most other actors in the primary health care (PHC) system were not actively engaged in the supervision of CHWs and their team leaders.
What do the new findings imply?
Actors in the formal PHC and district health system could be better mobilised to play a supportive role to CHWs and their supervisors, especially in orienting front-line PHC facilities to support ward-based outreach teams and creating enabling environments for community-based services.
A wider conception of supportive supervision of CHW programmes through the PHC system is required, with supervision understood as a set of horizontal and vertical relationships spanning system levels that goes beyond just one supervisor–supervisee interaction.
Social network analysis is a valuable tool to identify meaningful relationships and strengths and weaknesses in CHW programmes.
Introduction
In its recent guidelines on system support for community health workers (CHW) programmes, the WHO1 identified supportive supervision as one of 15 key priorities. It further highlighted the ‘low certainty of evidence’ and the ‘need to adapt supervisory strategies to the requirements of different contexts’.1
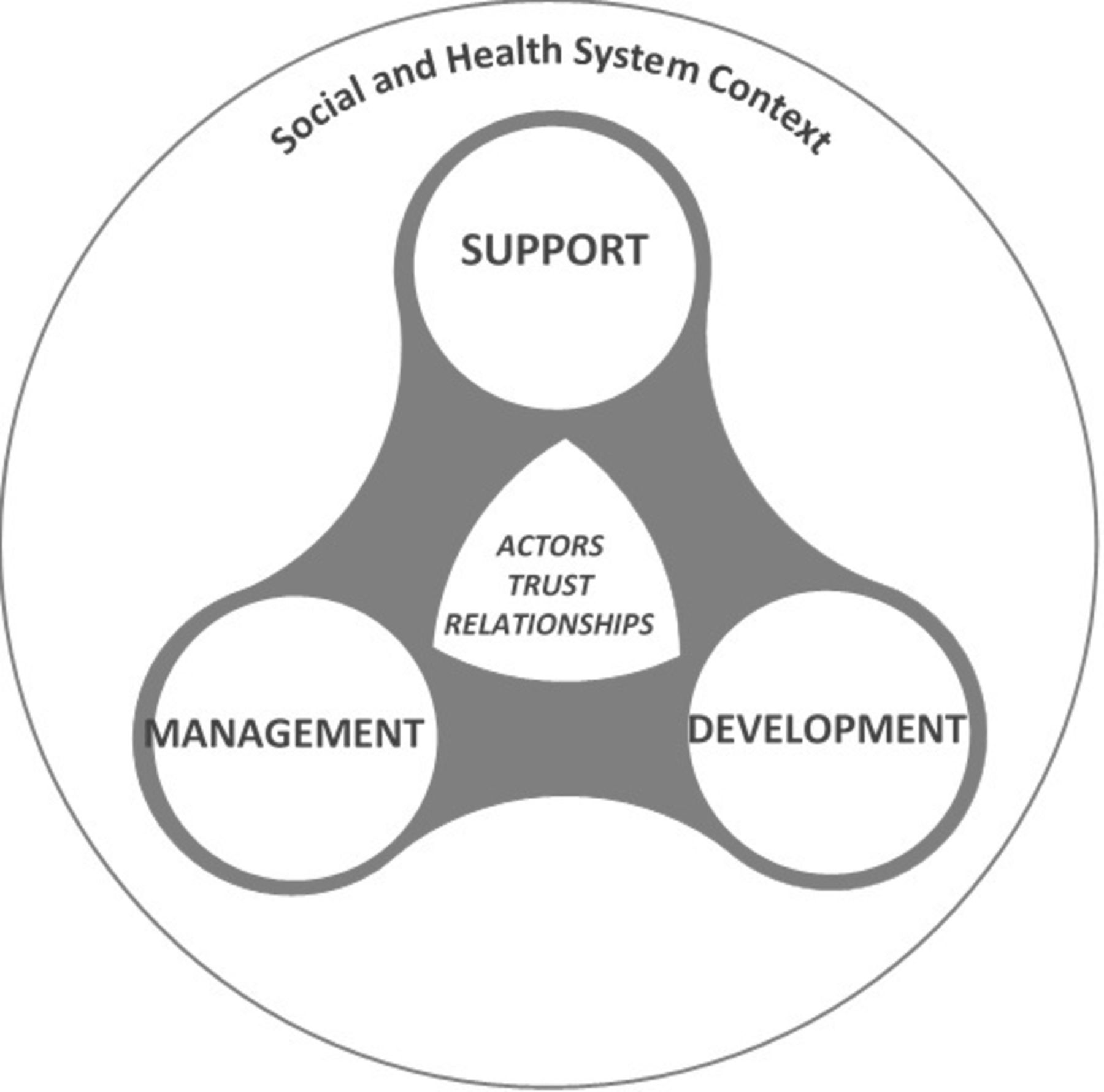
Supervision is a process that ensures support, guidance and feedback within the work environment.2 3 The traditional approach (often the dominant form) to supervision is typically characterised as a hierarchical relationship of control, involving discipline and surveillance between supervisor and supervisee.4–7 Supportive supervision is achieved in processes that strengthen relationships, and which promote among others: teamwork, joint problem solving, two-way communication, mentoring, feedback and participatory decision-making alongside formal performance monitoring.3 8 A holistic approach to supportive supervision would thus include managerial, development and support elements (figure 1). The management element involves the compliance to organisational standards, monitoring of work processes and allocation of resources; development refers to technical support to improve skills and knowledge through formal and informal training; and the support element addresses morale and motivation, which includes strengthening relationships and attending to supervisee needs, both instrumental and emotional.4 9
Such a holistic conception requires viewing supervision not just as a dyadic relationship between a supervisee and their immediate line supervisor,10–14 but rather as a system operating at several levels with a range of functions involving different actors and relationships and forms of interaction, for example, one-on-one, group and peer supervision, and so on, simultaneously.7 9 In this sense, supervision can be thought of as a set of relationships embedded in the wider context of social and professional relationships and hierarchies within the health system. Specifically, with respect to CHWs, their performance is determined by the quality of relationships with the formal health system on the one side and communities on the other side.15 This paper builds on to a prior study evaluating South Africa’s policy and practice with respect to supervision of CHWs in the ward-based outreach team (WBOT) strategy.16 As with other studies, one of the key gaps identified was the often dysfunctional and strained relationships between CHWs and the local primary health care (PHC) facilities, staff and line managers.16–18 This study explores these relationships quantitatively using social network analysis (SNA) of WBOT members and PHC health workers in a North-West (NW) Province district. The Province was chosen as it was an early adopter of the programme. Ngaka Modiri Molema (NMM) district was selected because at study inception it had the highest WBOT coverage in the province. The aim of the study was to identify the critical actors and the patterns of relationships within the supportive supervision system of WBOTs. These teams provide preventive and promotive services at community and household levels within a municipal ward. Each team is attached to and refers clients to a PHC facility. In terms of the policy, all PHC facilities should be associated with at least one WBOT and some facilities have more than one WBOT linked to them. A WBOT consists of an average of six CHWs, led by a professional nurse called a team leader (TL). At the time of the study, the CHWs in the NW Province were employed in contracts renewed every 3 months and received a stipend of R3500 (±US$236). There is a formalised accredited training divided in three phases, addressing HIV/tuberculosis (TB), maternal and child health and chronic disease care.
SNA is ‘a research methodology and theoretical paradigm concerned with explaining social phenomena using the structural and relational features of the network of actors involved’.19 Using mathematical software, SNA analyses and map entities, people or events (nodes) and their relationships (edges), in this instance the social and professional interactions of actors in a supervisory system. The method involves asking respondents (egos) to identify key members (alters) in their network in relation to a question of interest, where responses to the questions may be binary, indicating the presence of a relationship, or on a continuum, reflecting the strength of the relationship.20
Methods
A cross-sectional study of social and professional networks and interactions constituting the supervisory system of WBOTs in NMM District, NW Province, was conducted.
Study setting
NMM (population 0.86 million) is one of four districts in the NW Province and the subdistrict where the study was conducted had 23 PHC facilities, 20 WBOTs and 7 TLs at the time of the study. TLs are required to report to PHC facility managers. PHC facilities, depending on size and location, have a staff complement of professional nurses, assistant nurses, facility information officers, administrative clerks, lay councillors and cleaners. Professional nurses at facilities attend to clients referred by CHWs, and referrals from either side are supposed to be recorded in the relevant referral forms. A cluster of PHC facilities form a local area, headed by the local area manager (LAM) to whom the PHC facility managers report. School health nurses, who are responsible for screening reproductive and child health services at schools, also report to LAMs and refer clients to the PHC facility within their catchment area. Three local areas together with a district hospital form the subdistrict headed by the subdistrict manager who in turn reports to a district manager. Prior to the WBOT programme, CHWs were attached to non-profit organisations (NPO) providing HIV-related home-based care and support services in communities. CHWs are still paid from a special grant through the NPOs, and the CHWs report to an NPO coordinator located at the subdistrict office, to facilitate the payment process. WBOTs also interact with disease programme managers at the subdistrict level responsible for mental health, HIV and TB, maternal and child health and environmental health, to name a few. These managers are required to provide support to PHC in their specific areas of expertise and usually report to one of the LAMs who is also responsible for community health services (assistant director community health services (CHS)). Finally, most subdistricts have delegated a professional nurse as a WBOT ‘Focal Person’, also reporting to the assistant director-CHS. Due to the dearth of professional nurses, most focal persons also act as TLs. In some districts, as in the NMM district, there is a district focal person delegated to support subdistrict focal persons (see online supplementary file 1 for a diagrammatic representation of these relationships). The key actors directly and indirectly involved in the supportive supervisory system of WBOTs and their acronyms are listed in table 1.
Supplemental material
Inventory of people in the WBOT programme supervision system
The NMM district has had the highest WBOT coverage of wards (84%) in the Province with 129 teams, but at the time of the study there were far fewer TLs21 than required and most TLs thus supervised more than one WBOT. The district hired seven TLs specifically for the position, while the rest had more than one mandate (eg, facility based, managerial or other roles).
Study population and sampling
The subdistrict that, overall, had TLs and PHC facility managers who had been in their position and working with WBOTs since the start of the programme or shortly after, was purposefully selected for the study. This allowed the researcher to elucidate meaningful information based on the respondents’ extensive knowledge and experience (ie, information rich). The study population included the CHWs, TLs, PHC facility managers and LAMs who form the ‘core unit’ involved in the immediate supervision system of WBOT in the district. Two of the three local areas in the selected subdistrict with the longest serving TLs were further selected. The WBOTs and managers of five (of 17) facilities in the two local areas consented and were available to participate on the day of the study, resulting in a sample of 37 CHWs (clustered into five WBOTs), 3 TLs, 5 PHC facility managers and 2 LAMs (total 47 respondents). (See online supplementary file 1 for the reporting lines, sampled facilities and officials.)
Data collection and analysis
A structured questionnaire was distributed to the 47 respondents (online supplementary file 2). The first part of the tool included questions on respondents’ characteristics and perceptions related to the WBOT programme. CHWs often have challenging relationships in PHC facilities, therefore this background context sought to establish their perceptions about the PHC facilities as well as the rest of the health system. The second part of the questionnaire surveyed social and professional networks within the WBOT/CHW supervision system using five questions representing the elements of supervision (management, development and support) outlined in figure 1. The questions posed were on general communication (I communicate about WBOT work with each of these people), line authority (The person who checks that I do my work as expected is…), feedback (The person who gives me useful feedback on WBOT work is…), workplace challenges (The person who helps me resolve challenges in my work (eg, staff relations, difficult community, stipend payments)) and personal matters (I speak about sensitive personal issues with…) within the work environment. The ‘communication’ variable sought to establish the frequency of interaction on issues related to the WBOT programme among actors within the WBOT supervisory system. ‘Line authority’ represented the management element of the supervision system from CHWs up to middle management within the subdistrict. ‘Feedback’ was used as an indicator of the development element of supervision with examples of feedback relating to quality of referrals, household visits and data collection. ‘Resolving challenges’ was related to the support element and examples given to respondents included staff relations, difficult community interactions and inadequate supply of resources. Finally, ‘personal matters’ represented the interpersonal or emotional element of support. Examples of this were problems with drug abuse affecting their children, or in their marriages/relationships. The examples were applied consistently to all respondents.
Supplemental material

Elements of supportive supervision.
As there were no pre-existing, validated tools to draw on, the indicators/questions and accompanying examples posed for each element of the framework were generated by the first author, based on the typical challenges and difficulties identified in a first phase of qualitative research,16 her knowledge of the cultural context, an assessment of face validity with her supervisors and discussions with an expert in organisational SNA. Given the rigours of completing the SNA, we were advised to limit the number of questions and to phrase them specifically. Various iterations of questions were pilot tested.
Questionnaires were individualised for each facility. Prior to data collection, WBOT TLs, who were considered the pivotal and information-rich actors, were consulted to provide a list of names of people in the WBOTs, local facility and local area making up their support/supervisory system and any other relevant officials directly or indirectly linked to the system. CHWs, TLs and PHC facility managers in one facility were given the same list. LAMs were given a list of names in all facilities in their respective local areas from PHC facility managers down to TLs. The questionnaire made provision for space (other) where respondents could add additional names not on the list that were considered to have relationships with the WBOT programme. The ‘other’ category was completed three times and health workers named were CHWs and a cleaner. The survey was conducted at the respondents’ workplace. Respondents familiarised themselves with the study by reading the information sheet and provided signed consent for their involvement in the study. All consenting respondents completed the questionnaire individually, seated away from the researcher and other respondents. The first author (TA) was present in the room to take respondents through the questionnaire and on how to complete it but did not influence responses in any way.
Each respondent (ego) was requested to identify relevant persons (alters) for each question, drawing from the list of names on the tool. For communication, egos had to indicate with a corresponding number, how often (daily=5, once a week=4, once a month=3, once a quarter=2, never=0) they communicated with each person listed. For the other four questions, egos only indicated with a tick the most relevant person/s for each question. Data were captured into Excel 2019 (Microsoft, USA) matrix, with communication data as is from the questionnaires, while the data for the four binary questions were captured with a ‘1’ representing a link and ‘0’ representing no link. The data were checked for errors and inconsistencies were corrected. The aim of the study was to map the social networks from the point of view of CHWs, TLs, PHC facility managers, and LAMs, and alters named by these respondents were not contacted for confirmation. The Excel spreadsheets were formatted to comma delimited (.csv) sheets and imported into the Gephi V.0.9.2,21 which was used to generate directed and undirected sociographs of social and professional networks among WBOT members and PHC facility staff. The graphs were generated at team, facility and local area levels. The actors in the network are represented by the coded circles (nodes). The higher the number of respondents who identified the node, the bigger the node and the darker the shading. The lower the number of respondents who identified the node, the smaller the node and the lighter the shade. All the sociographs except for communication are directed ties indicated with a single headed arrow. The direction of the arrow (edges) between the nodes moves from the ego (tail of arrow) pointing to the alter (head of arrow). The communication sociographs are undirected ties. The direction of the edge is represented by the colour of the ego, moving from the ego to the alter.
Patient and public involvement
As this study was focused principally on relationships within the PHC system, it was done without patient involvement.
Results
Characteristics and perceptions of respondents
The majority of the 47 respondents were aged 40–60 years (n=38) and female (n=41). Just over half (n=25) had been attached to the WBOT programme since its inception in 2012, with an average of 6 years in the programme. All three TLs and 37 CHWs indicated that they performed the work of the WBOTs daily, while the five PHC facility managers did WBOT related work at least once a week, and the two LAMs at least once a month. All but two respondents (PHC facility manager and CHW) believed that the WBOT programme ‘is important for communities’, although only two-thirds believed the health department viewed WBOTs as important or felt respected as part of health system (table 2). All 14 respondents who indicated they did not feel respected were CHWs.
Characteristics of respondents (n=47)
Socionetwork graphs
The findings which follow report on the structure of social networks in the WBOT supervision system. The figures are of individual separate facilities (see online supplementary file 3 for all facility diagrams). The acronyms of nodes in the figures represent actors as listed in table 1.
Supplemental material
General networks of communication
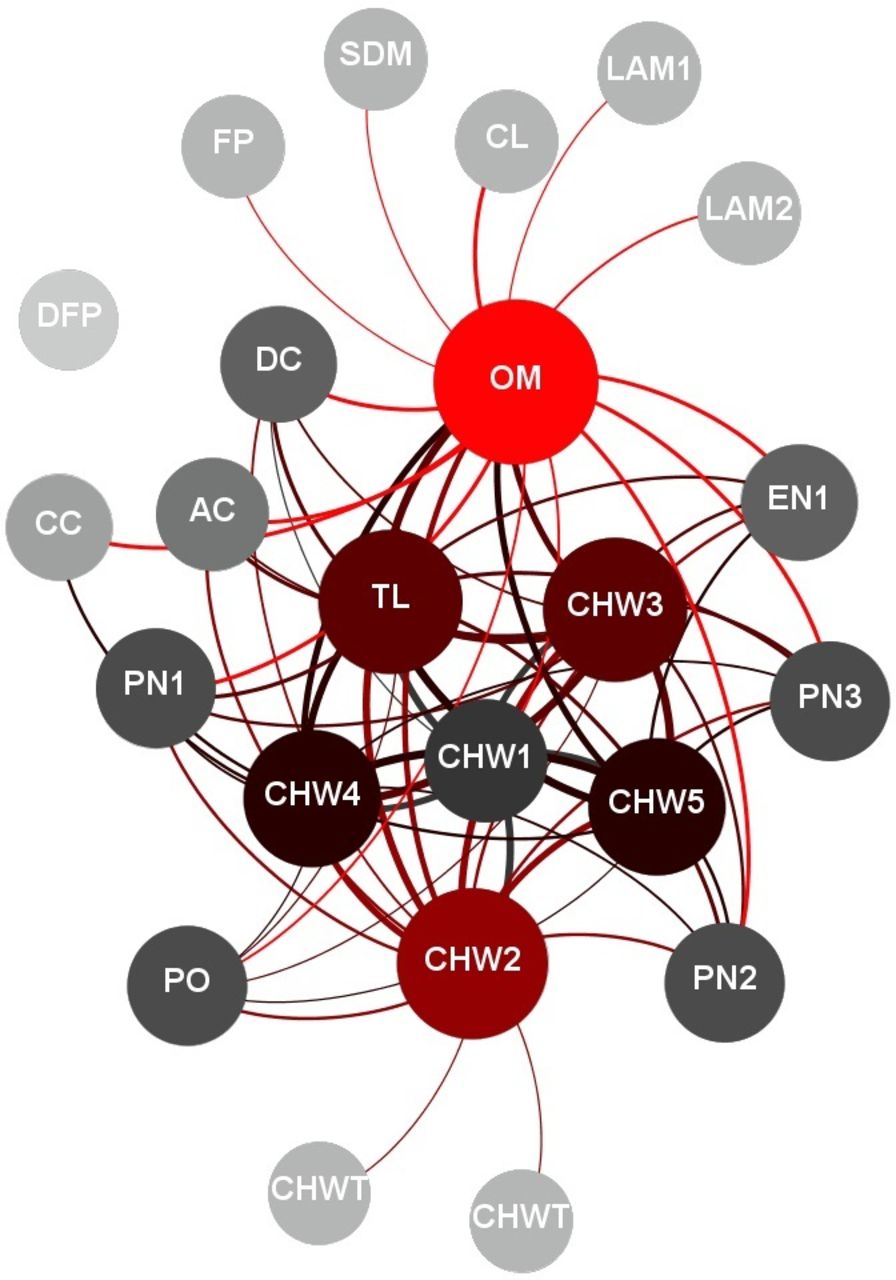
The communication network diagram (figure 2) shows the frequency of communication between actors associated with the local WBOT programme in one health facility. The lines between the nodes indicate presence of interaction, with more frequent interaction indicated by thicker lines. The lines move from the egos to alters, with the ego node matching the colour of the line. The size of the node indicates the number of interactions the person had with others—the bigger the node the larger the number of interactions the person had.
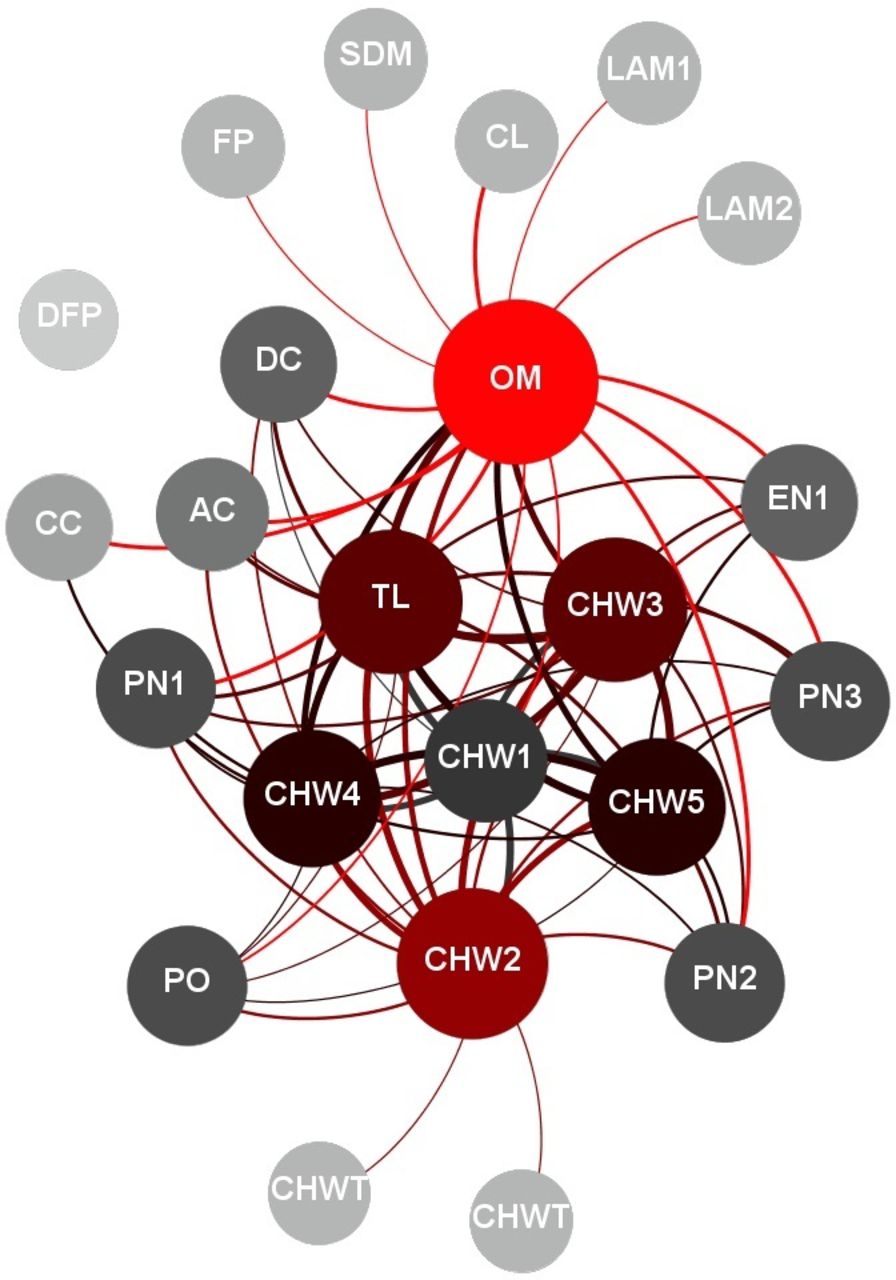
Communication network diagram in facility 4. AC, administrative clerk; CC, councillor; CHW, community health worker; CHWT, community health worker in another team; CL, cleaner; DC, data capturer; DFP, district WBOT focal person; EN, enrolled nurse; FP, subdistrict WBOT focal person; LAM, local area manager; OM, PHC facility manager; PN, professional nurse; PO, NPO coordinator; SDM, subdistrict manager; TL, team leader.
This figure shows a typical dense local communication network in the PHC system regarding the work of WBOTs. Across all facilities, the PHC facility manager and TL were at the centre of the communication network, indicated with their relatively larger nodes. Frequent (daily to weekly) communication between CHWs and others (represented by the thickness of lines) was mainly with other CHWs (76%) and TLs (75%), followed by PHC facility managers (53%). Although present, communication networks between WBOTs and other PHC staff were less dense, while in some instances the communication networks extended to actors beyond the local facility (represented by community health worker in another team in figure 2).
Supervisory relationships
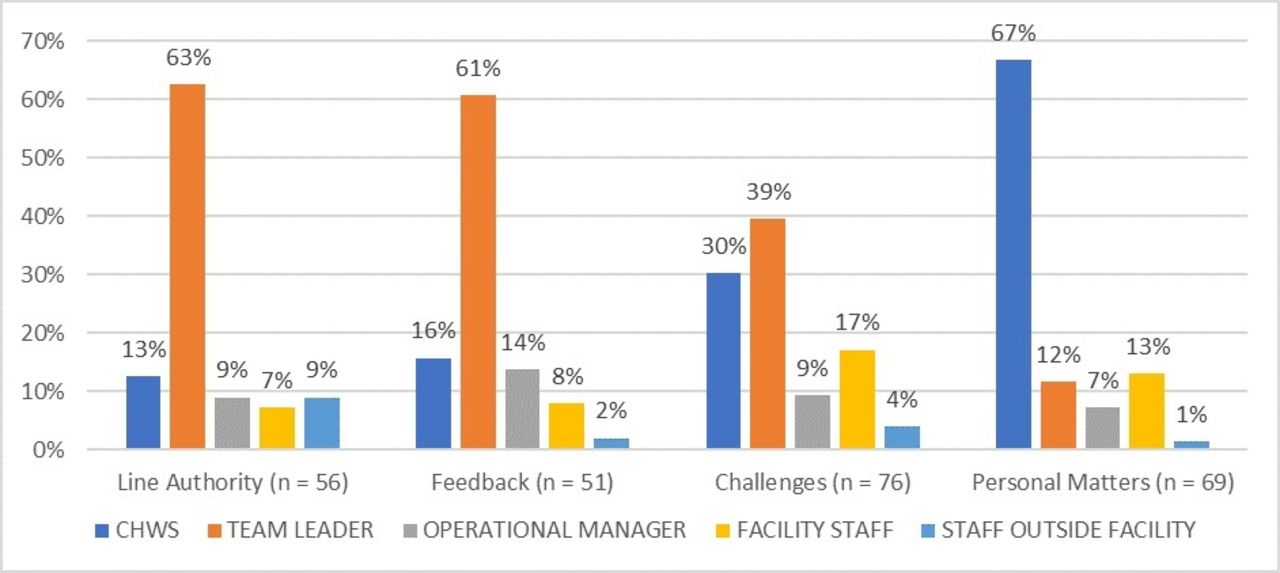
The summary findings on the interactions relating specifically to supervision (line authority, feedback, workplace challenges and personal matters) are presented in figure 3. The number (n) in brackets on the legends indicates the total number of actors (alters) identified by CHWs (egos) as fulfilling that function (ie, per question). Over 60% of CHWs identified the TLs as actors who checked their work and who they relied on for capacity building, and less so other CHWs, facility staff and staff outside the facility. With regard to workplace and interpersonal support, CHWs turned mainly to other CHWs or TLs.

Professional and social interactions related to supervision of community health workers (CHW) in all facilities (n=37 CHW respondents).
Management: line authority
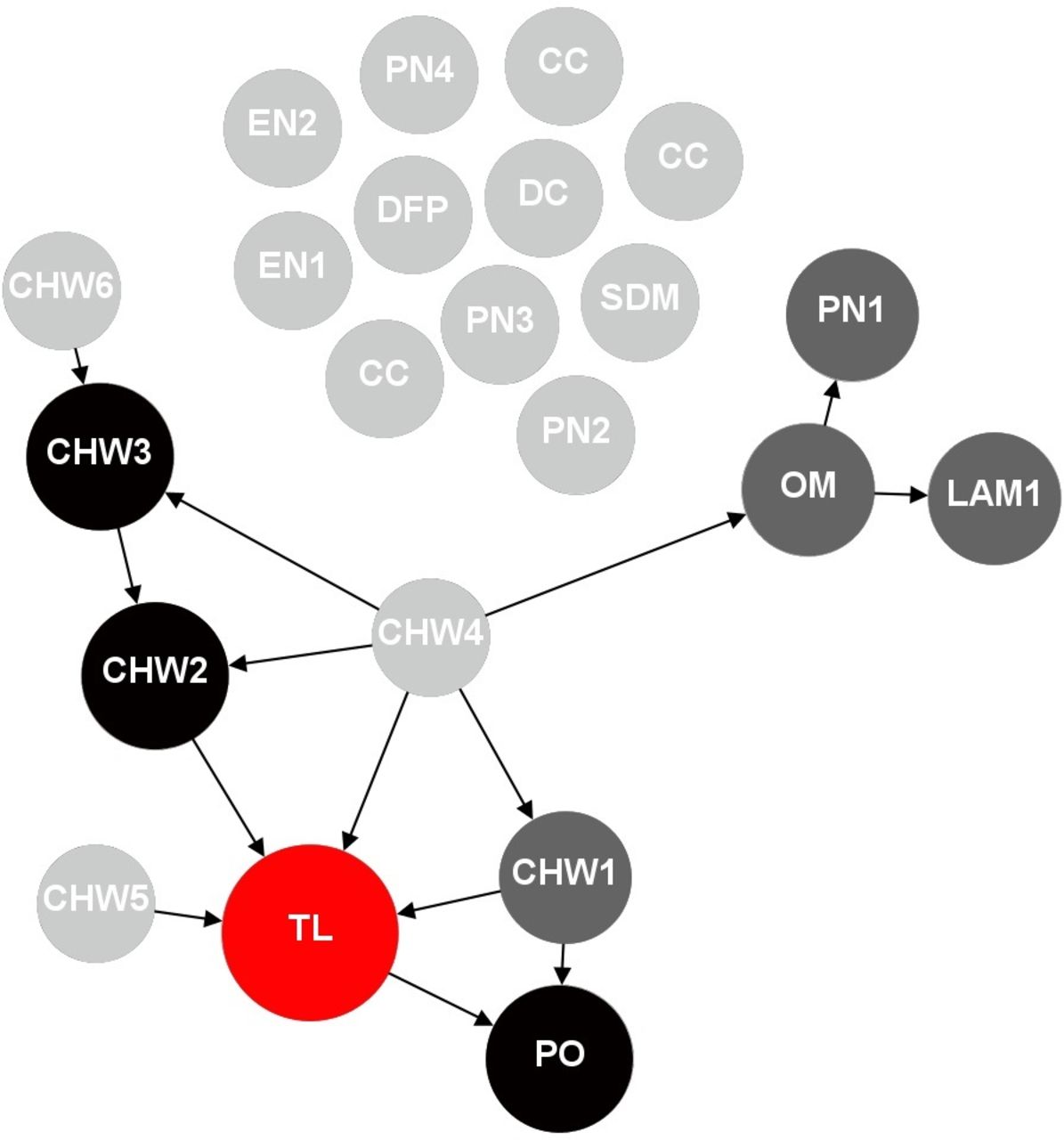
While for the most part, CHWs identified the TL as the person who checked their work (figure 4). TLs themselves reported a more diverse set of actors they were accountable to, which included the PHC facility manager, LAM and the NPO coordinator. On the other hand, all PHC facility managers reported that mainly LAMs checked their work. In general, facility staff did not play much of an oversight role in the WBOT programme.
Management (line authority) network diagram (facility 3). AC, administrative clerk; CHW, community health worker; DC, data capturer; DFP, district WBOT focal person; EN, enrolled nurse; FP, subdistrict WBOT focal person; LAM, local area manager; OM, PHC facility manager; PN, professional nurse; PO, NPO coordinator; SDM, subdistrict manager; TL, team leader.
Figure 4 illustrates the line authority relationships in facility 3, which had two WBOTs linked to it. In this instance, besides for the TLs, some of the reported actors who reportedly checked the work of the CHWs were an enrolled nurse, facility information officer (data capturer, DC) and other CHWs. In this facility, the PHC facility manager (OM) checked the work of the TL and vice versa.
Development: feedback
As with the line authority, TLs were the central actors in providing feedback to CHWs and fulfilling the developmental role, while TLs drew from a variety of actors—the LAM (2), NPO coordinator (1), PHC facility manager (OM) (1) and facility information officer (DC) (1).
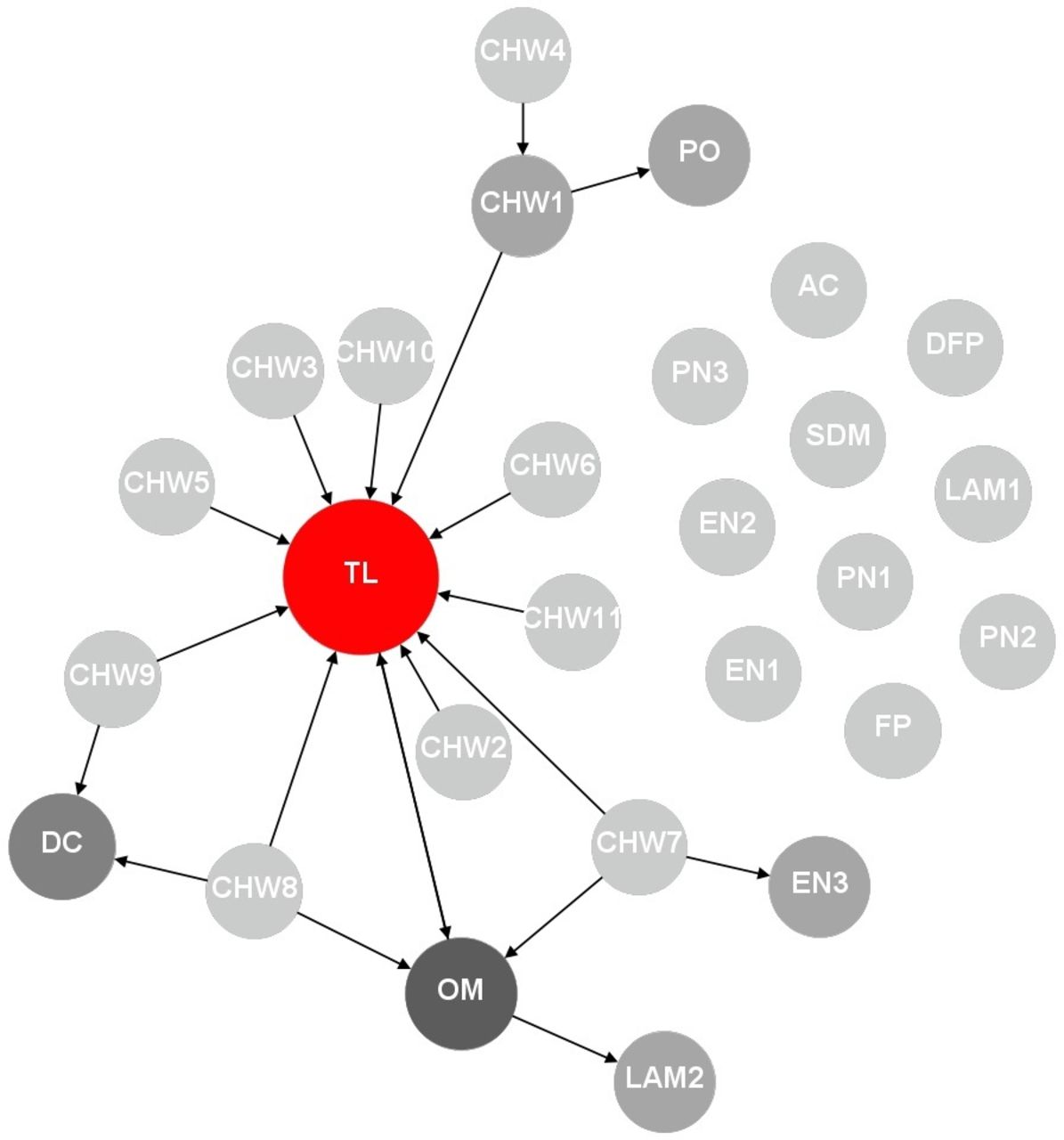
Apart from one facility, TLs and PHC facility managers did not seek feedback from each other. PHC facility managers mainly sought feedback from CHWs (16) and identified other actors like the district focal person (1), TL (1), facility information officer (1) and the NPO coordinator (1). Some CHWs were key actors within their teams. However, interaction between WBOTs across teams was minimal, even when they reported to the same TL and facility. Very few actors from WBOTs received feedback from facility staff. An illustration of this can be seen in the network diagram (figure 5) of a facility with two WBOTs (WBOT1: CHW 1–6 and WBOT2: CHW 7–12) under the same TL.
Development (feedback) network diagram (facility 1). CHW, community health worker; DFP, district WBOT focal person; EN, enrolled nurse; FP, subdistrict WBOT focal person; LAM, local area manager; OM, PHC facility manager; PN, professional nurse; PO, NPO coordinator; SDM, subdistrict manager; TL, team leader.
Support: challenges
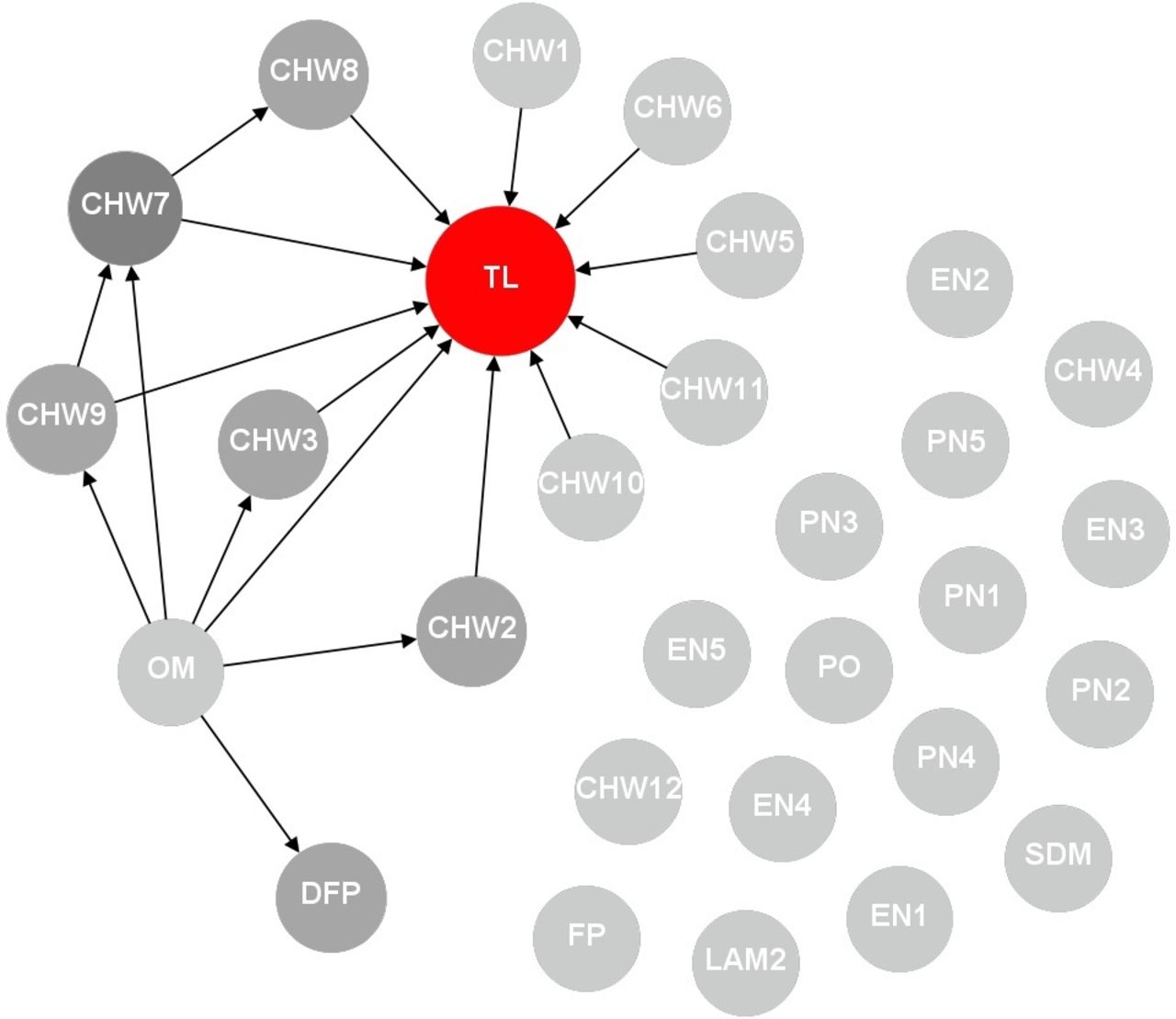
With respect to workplace challenges, the TL was once again the main actor and most CHWs (30 out of 37) reported that the TL helped resolve their challenges. In all five of the WBOTs, there was also a degree of reliance among CHWs to resolve challenges. TLs identified the LAM (2), PHC facility manager (1) and NPO coordinator (1), with one indicating that they could rely on no one to resolve workplace challenges. PHC facility managers generally relied on their facility staff although they also identified the LAM (2), TL (1), subdistrict manager (1) and the NPO coordinator (1). The link between facility staff and WBOT members was weak, illustrated in figure 6, which shows the facility staff and WBOT represented by two separate clusters.

Support (challenges) network diagram (facility 2). CC, councillor; CHW, community health worker; DC, data capturer; DFP, district WBOT focal person; EN, enrolled nurse; LAM, local area manager; OM, PHC facility manager; PN, professional nurse; PO, NPO coordinator; SDM, subdistrict manager; TL, team leader.
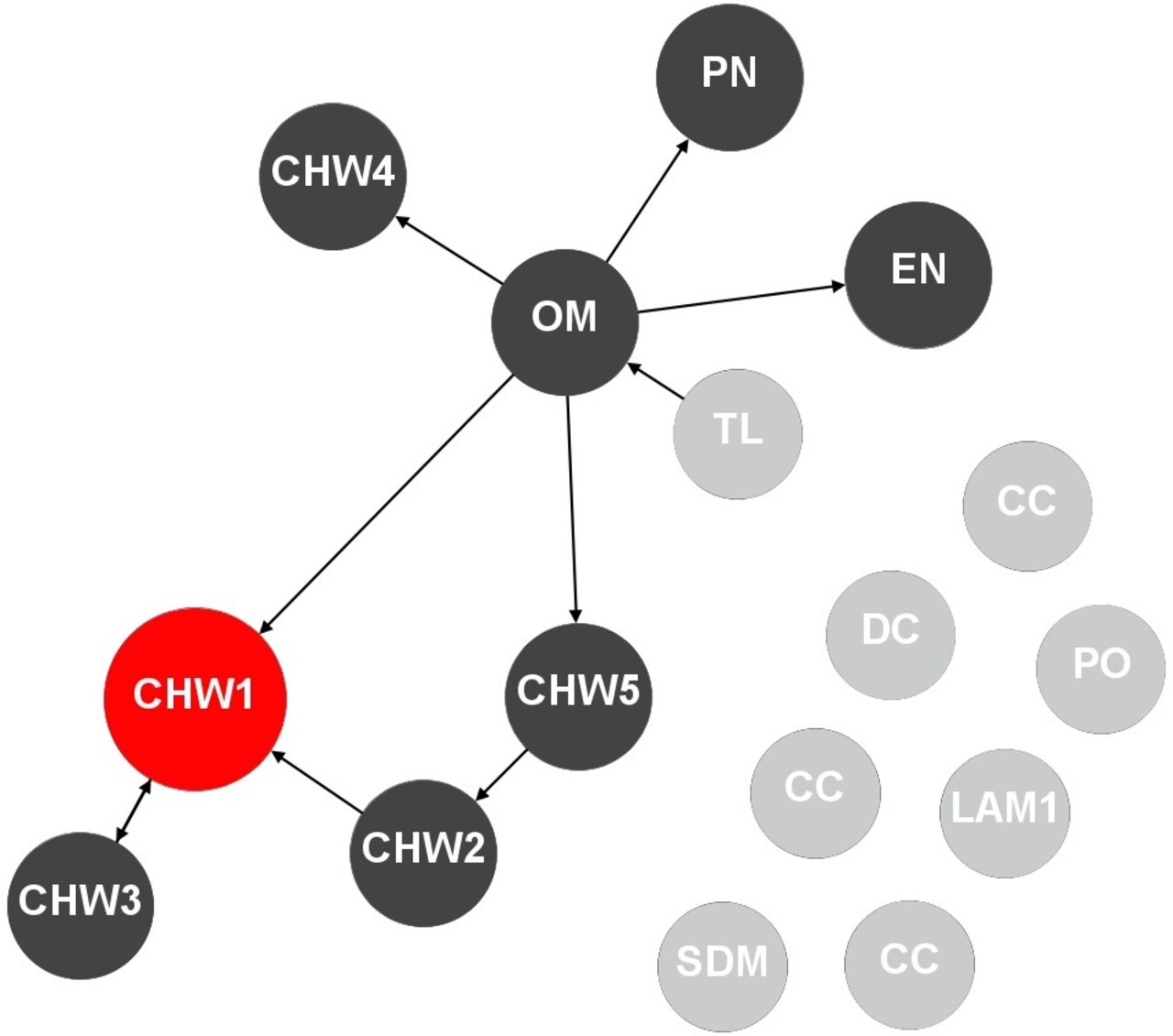
Support: sensitive
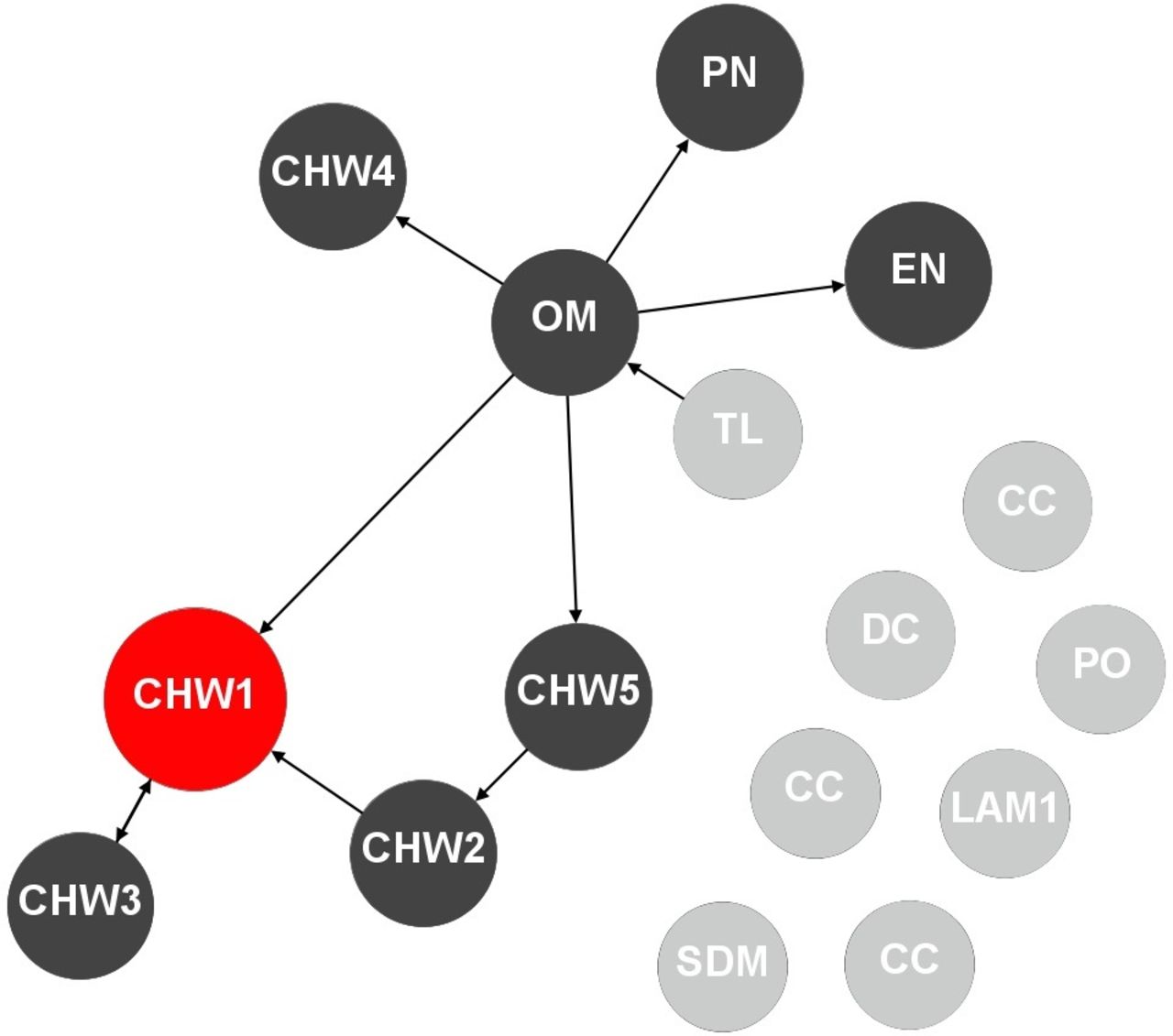
CHWs mostly discussed personal matters with other CHWs (46) with limited reliance on TLs (8), PHC facility managers (5), facility staff (9) and staff outside the facility (1). In figure 7, the TL was a marginal player, not identified by any actor. Similarly, the TLs relied on a few people (focal person (1), facility staff (1), CHWs (3)) to discuss personal matters, with one TL indicating that they did not rely on any of the actors to discuss personal matters. PHC facility managers identified CHWs (4), facility staff (2), LAM (1) and the subdistrict focal person (1) as people with whom they could discuss a personal matter. In the facility represented in figure 7, one CHW was identified more than the TL or PHC facility manager.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Support (personal matter) network diagram (facility 5). CC, councillor; CHW, community health worker; DC, data capturer; EN, enrolled nurse; LAM, local area manager; OM, PHC facility manager; PN, professional nurse; PO, NPO coordinator; SDM, subdistrict manager; TL, team leader.
In sum, network patterns suggest that TLs are critical actors, who ensure internal cohesion and the most important sources of support to WBOT members, except for personal matters. The patterns also show that there is cohesion and support among WBOT members. Facility staff such as PHC facility managers, other professional nurses and middle managers in the subdistrict do not appear to be active actors, with a low degree of involvement in the WBOT supervisory system. However, there are certain cadres among the PHC facility staff from whom CHWs can draw support.
Discussion
Supervision is often thought of as a dyadic relationship between the supervisor and the supervisee, leaving out other actors within the system. Yet the evidence from this study shows that approached holistically, supportive supervision involves a wide range of actors and relationships within a system.9 There is considerable evidence, from both the NW and elsewhere, that CHWs/WBOTs are often treated as outsiders by actors in the PHC system and perceive themselves as exploited and unacknowledged by the broader system.16 22–25 On the other hand, respondents were almost unanimous on the importance of the WBOT programme for communities.
In describing the relationship patterns of WBOTs in a local district, the study found that there were dense networks of communication within WBOTs, among team members, with their TLs and PHC facility managers and to some extent with PHC staff. There was also communication, though less frequent, with subdistrict and even district actors like NPO coordinators and the district focal person. The density of the networks indicates that there are opportunities for actors to engage with each other. However, the study findings suggest this interaction was not structured towards providing supportive supervision.
The majority of CHWs indicated that the TLs ‘checked their work’, corresponding with policy documents stipulating that TLs oversee activities of CHWs.16 26 According to policy, TLs, in turn, are to be supervised by PHC facility managers: ‘the quality of the work delivered by the WBOT will be monitored by the PHC facility manager’, and ‘CHWs must become part of the multi-disciplinary primary health care team within the district health system’.26 In practice, TLs reported to a number of actors, especially where a shortage of professional nurses required them to oversee several teams across PHC facilities. This created confusion on supervisory lines into the PHC system, a situation which can impact on the functioning of WBOTs.23 27
TLs had a central role in providing feedback to CHWs, but WBOTs also drew on other actors for this role. In the absence of formally designed frameworks of support supervision, WBOTs and district actors engaged and sought feedback from each other in largely informal processes.16
Most CHWs also identified the TL as the main actor to resolve their workplace challenges, with limited reliance on PHC facility staff. Only one of the three TLs identified other actors in response to this domain, indicating that TLs are limited in their choices on who they can rely on to resolve their workplace challenges. Similarly, PHC facility managers mostly turned to other PHC facility staff rather than actors at other levels in the subdistrict to resolve WBOT-related problems. On personal matters, CHWs relied largely on each other, and the TLs, in this instance, were marginal actors. The TL had a few CHWs and PHC facility staff she could share her challenges with, while the PHC facility staff, including the PHC facility manager, generally shared among themselves.
On the whole, PHC facility staff and middle managers at subdistrict and district levels did not have much of a role in supporting and overseeing the work of the WBOTs. This resonates with previously documented problematic relationships between CHWs and the PHC system, poor organisational support in PHC facilities and a prevalent perception of not being respected.1 16 22 23 27 While the immediate supervisor of the CHWs is the TL, the PHC facility managers and staff have a pivotal role in supporting, overseeing and integrating the work of the WBOTs. Local area and other middle managers have supervisory responsibilities over facilities and are thus key to orienting and enabling PHC facility staff to fulfil their roles towards the WBOTs. In light of this, many of the actors in the PHC system could be better mobilised to directly and indirectly, play a supportive role to the WBOTs. This support would ensure that WBOTs’ resourcing, monitoring and support are integrated into processes at all levels of the district health system, thus improving their integration into the formal health system and performance outcomes.16 22 27 The study findings suggest key gaps in this wider supervisory cascade.
The goal of supportive supervision is to improve the performance and quality of service delivery and human resource development and supporting those delivering the service.
With respect to the WBOTs in South Africa, this analysis suggests several recommendations. First, while the TL function is key, critical gaps in the middle management layers of the PHC system, supposed to provide supervision of and support to the supervisors, also need to be addressed. The roles and responsibilities of all actors in the wider WBOT supervisory system need to be clarified and formalised, including facility staff other than managers, LAMs, health programmes and subdistrict managers. These roles would encompass clear lines of communication in resolving challenges, reviewing and giving feedback on performance, and in-service training.
Second, the centrality of TLs needs to be recognised, and their numbers and mandates protected to ensure they focus on the WBOT programme. TLs are critical actors and provide regular support to CHWs, and as found in other studies, support and supervision from professional staff motivates CHWs.22 28 Given their centrality as actors, the dire shortage of TLs (ratio of 1 TL to 6 teams in the district), increasingly with dual community and other roles, poses a major threat to the WBOT programme. As recommended in the WHO guidelines, committing to clear ratios of supervisors is clearly key to an effective supervision system.1
Third, the district needs to recognise and capitalise on the coherence, cohesion, natural leadership and peer support among CHWs, with careful consideration on developing their career paths into supervisory levels.
Finally, SNA provides a valuable tool to analyse relationships and identify key actors who may be influencers and bridges. The SNA validated and served to quantify previous qualitative observations on the limits of the supervisory system. A follow-up qualitative phase is being conducted, in which the findings of the SNA are presented to the participants in phase 1 and findings probed in more depth.
This study had several limitations. Given that the survey required that all the CHWs, their TLs and the facility manager complete the survey, only a limited number could be sampled. This limits the generalisability of findings. However, since programme implementation has been steered by provincial processes, it is possible that the results observed in this study would be similar in other districts. Although the primary focus of the study was supportive supervision within the formal PHC and district health system, including community members in the study population would have added valuable perspectives. Finally, the conclusions that we draw accord with prior work16 and observations elsewhere in South Africa.22 24 29–31
Conclusion
Supportive supervision of CHWs can be thought of as a system of horizontal and vertical relationships that go beyond just one supervisor–supervisee interaction. In this study, supervisory relationships within teams functioned better than those between teams and the rest of the PHC system. Understanding these relationships is key to designing effective supportive supervision in CHW programmes. SNA can be a valuable approach in identifying the relationships to be strengthened.
Acknowledgments
The authors are thankful to all the participants for providing valuable insights on their experiences. The authors also acknowledge Dr Vera Scott and Mr Paul Currie for providing comments and guidance in the conception and analysis of the study.
Footnotes
Handling editor Stephanie M Topp
Twitter @schneider_helen
Contributors The study design was developed by TA and HS. TA performed the analysis under the supervision of HS. TA drafted this article and both authors revised the manuscript.
Funding The work reported herein was made possible through funding by South African Medical Research Council through its Division of Research Capacity Development under the National Health Scholarship Programme from funding received from the Public Health Enhancement Fund/National Department of Health. The content hereof is the sole responsibility of the authors and does not necessarily represent the official views of the SAMRC or the funders.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Ethical approval for the study was obtained from the University of the Western Cape Research Ethics Committee (registration number BM/17/3/3) and the North-West Provincial Department of Health Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available in a public, open access repository. Data are available upon reasonable request.