Article Text

Abstract
Introduction While there is substantial evidence for the benefits of exercise-based rehabilitation in the prevention and management of non-communicable disease (NCD) in high-resource settings, it is not evident that these programmes can be effectively implemented in a low-resource setting (LRS). Correspondingly, it is unclear if similar benefits can be obtained. The objective of this scoping review was to summarise existing studies evaluating exercise-based rehabilitation, rehabilitation intervention characteristics and outcomes conducted in an LRS for patients with one (or more) of the major NCDs.
Methods The following databases were searched from inception until October 2018: PubMed/Medline, Embase, CINAHL, Cochrane Library, PsycINFO and trial registries. Studies on exercise-based rehabilitation for patients with cardiovascular disease, diabetes, cancer or chronic respiratory disease conducted in an LRS were included. Data were extracted with respect to study design (eg, type, patient sample, context), rehabilitation characteristics (eg, delivery model, programme adaptations) and included outcome measures.
Results The search yielded 5930 unique citations of which 60 unique studies were included. Study populations included patients with cardiovascular disease (48.3%), diabetes (28.3%), respiratory disease (21.7%) and cancer (1.7%). Adaptations included transition to predominant patient-driven home-based rehabilitation, training of non-conventional health workers, integration of rehabilitation in community health centres, or triage based on contextual or patient factors. Uptake of adapted rehabilitation models was 54%, retention 78% and adherence 89%. The majority of the outcome measures included were related to body function (65.7%).
Conclusions The scope of evidence suggests that adapted exercise-based rehabilitation programmes can be implemented in LRS. However, this scope of evidence originated largely from lower middle-income, urban settings and has mostly been conducted in an academic context which may hamper extrapolation of evidence to other LRS. Cost-benefits, impact on activity limitations and participation restrictions, and subsequent mortality and morbidity are grossly understudied.
- noncommunicable disease
- rehabilitation
- developing countries
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
The burden of non-communicable disease (NCD) is increasing exponentially in low-resource settings (LRS), where health systems are least equipped to manage these conditions.
Exercise-based rehabilitation is an evidence-based, essential component in the management of NCDs.
What are the new findings?
Sixty studies were identified that evaluated exercise-based rehabilitation, predominantly in urban LRS, and embedded in an academic context.
Research on exercise-based rehabilitation for patients with cancer in LRS is in its infancy.
The majority of outcomes included in these studies pertained to the level of body function (eg, blood pressure), whereas outcomes on the level of activity and participation were reported less, and specific outcomes relevant for policy and guideline development were scarce.
What do the new findings imply?
Important evidence gaps exist in terms of the type of LRS in which exercise-based rehabilitation for NCD has been studied, as well as the specific outcomes included in these studies.
Feasibility of using alternative delivery models to circumvent resource restrictions encourages a wider implementation and study of exercise-based rehabilitation for NCDs in LRS.
Introduction
While there is substantial evidence for the benefits of exercise-based rehabilitation in high-resource settings,1–4 it is not evident that these evidence-based programmes can be implemented in a low-resource setting (LRS), and correspondingly it is not clear whether the same outcomes can be achieved. For example, how is exercise provided effectively in settings where exercise facilities are limited, and patient safety during outdoor exercise is not guaranteed? Moreover, how can a benefit be established using gold-standard methods when, for instance, randomisation to usual care is ethically questionable based on the established evidence of benefit from high-resource settings? Are different outcomes more relevant to patients with non-communicable diseases (NCD) living in an LRS, yet scantly considered in high-resource settings?
NCDs are the leading cause of death globally; almost three-quarters of NCD-related deaths occur in low and middle-income countries (LMIC).5 As of 2017, cardiovascular disease (CVD) accounts for most of these deaths (17.8 million people annually) globally, followed by neoplasms (9.56 million), respiratory diseases (3.91 million) and diabetes (1.37 million).6 These four conditions account for 82% of all NCD deaths and for 54% of loss in disability-adjusted life years (DALY) globally. The burden of NCDs is growing; the WHO projected that by 2030, NCDs in LMICs will be responsible for three times as many DALYs and nearly five times as many deaths compared with deaths caused by communicable diseases, maternal, perinatal and nutritional conditions combined.7 The increasing burden of NCDs is likely to burden health systems least equipped to tackle the challenge,8 and likely to impede poverty reduction initiatives.7 9 While nationwide policies for NCD risk factors such as tobacco use, alcohol and nutrition exist (less so for physical activity), these policies have rarely been adequately implemented due a multitude of factors including inadequate political commitment and resources.8 Rehabilitation is an evidence-based intervention for the management of NCDs,2 10 for which the current need far exceeds the availability, particularly in LRS.11–15
As outlined in the WHO call for action (#REHAB2030), there is a dearth of evidence from randomised controlled trials (RCT) evaluating the effects of rehabilitation in LMICs.7 Understanding the contextual factors which have been reported when investigating exercise-based rehabilitation programmes for the management of NCDs in LRS could inform the planning of future RCTs in this context. Therefore, the objective of this scoping systematic review was to summarise and analyse existing studies evaluating exercise-based rehabilitation, in terms of quality of evidence/methodology, rehabilitation intervention characteristics and outcomes conducted in an LRS for patients with one (or more) of the major NCDs.
Methods
Given the comprehensive nature of this inquiry, a scoping review was conducted based on the model described by Arksey and O’Malley,16 and reported in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analysis for Scoping Reviews (PRISMA-ScR).17 A PROSPERO-based review registration template is publicly available on the Open Science Framework (https://osf.io/5hu3w/).
Inclusion criteria
The focus of this review was on rehabilitation for patients with NCDs of lifestyle conducted in an LRS. Inclusion and exclusion criteria were revised iteratively based on increasing familiarity with the literature, and related to the participants, concepts and context. All original research study designs reported in English were considered, excluding case studies.
Participants
The four major NCDs related to lifestyle considered were: CVD (International Classification of Diseases (ICD): I0–99), malignant neoplasms (ICD: C00–97), chronic respiratory disease (ICD: J30–98) or diabetes (ICD: E10–E14; excluding those with complications (minus E10.2–E10.29, E11.2–E11.29, E12.2, E13.2–E13.29, E14.2)).18 We also considered studies in which the study sample had at least one of these medical conditions in co-occurrence with other medical conditions due to the high prevalence of multiple medical conditions in LRS (eg, HIV/AIDS).19
Concepts
Rehabilitation was defined in line with the WHO as ‘a set of measures that assist individuals who experience, or are likely to experience, disability to achieve and maintain optimal functioning in interaction with their environments’.7 To be included, the rehabilitation delivered in the studies had to consist of the following: (1) assessment of NCD risk factors, (2) structured exercise (supervised or unsupervised), and (3) at least one additional strategy to control risk factors (eg, education).20 This further specification of rehabilitation was warranted due to the common risk factors (eg, physical inactivity, poor nutrition) associated with the incidence and burden of the four major NCDs studied.
Context
Studies were considered to be conducted in an LRS if they were undertaken in a low-income country (LIC) to lower middle-income country (LM) as per World Bank criteria (83 of 218 countries),21 or in an upper middle-income country (UM) or high-income country (HIC) yet explicitly in a context indicative for an LRS (eg, rural areas, minority populations).
Data sources and search strategy
Six electronic databases were searched on 12 October 2018 and without date limitations: CINAHL (Cumulative Index to Nursing and Allied Health Literature), Cochrane Central Register of Controlled Trials, Embase, Medline (Ovid), PsycINFO and PubMed (excluding Medline records). The search strategies were developed in collaboration with an information specialist (MP), the inclusion of subject headings as appropriate for each database and free-text terms relevant to each key concept. The search results were limited to humans and no language limits were applied. Reference lists of included studies were hand searched for additional materials. The full Medline search strategy is included as online supplementary file 1.
Supplemental material
Study selection
A rough initial screening of titles was conducted by one reviewer (MH), and titles clearly ineligible were excluded at this stage. Subsequently, potentially eligible titles and abstracts were screened independently by two reviewers (MH and ALS) to determine the inclusion or exclusion of studies for full-text review. Any disagreements were discussed and used to refine inclusion and exclusion criteria. In case of irreconcilable disagreements, a third reviewer was consulted (SDH). An identical process was used to determine final inclusion of full-text articles obtained. The citation inclusion and exclusion consideration process and data extraction were performed within an online review management platform (https://www.covidence.org).
Data extraction and synthesis
A charting form was developed to characterise the thematic focus of each paper, study design (eg, type, patient sample, geographical context, setting, outcome measures), rehabilitation intervention characteristics (eg, delivery model, risk factors addressed, exercise prescription), deliberate choices made to accommodate the LRS, utilisation (uptake (eligibility vs inclusion), loss to follow-up and adherence), as well as qualitative and quantitative results. Included articles were equally allocated among two reviewers (MH and ALS). The first reviewer performed the data extraction, while the second reviewer verified the data extracted and vice versa (as opposed to extracting all data independently). This process was considered a pragmatic way to share the workload while maintaining scientific rigour. An exception to this process was the risk of bias of the included clinical trials, based on the Cochrane Risk of Bias tool, which was conducted by two reviewers (MH and ALS) independently.22 Studies were considered of high quality when meeting all criteria (ie, low risk of bias) except blinding of participants, which was deemed unfeasible in most rehabilitation-type interventions.23 The extraction form was developed a priori, and revised after each included study until no further changes to the form were considered necessary.
Reported outcomes for each study were extracted and pooled according to the WHO International Classification of Functioning, Disability and Health (ICF) model.24 The ICF model describes the relation and interaction between the health condition, impairments of body function and structures (eg, lung function, lipid profile), activity limitations (eg, mobility, balance) and participation restrictions (eg, productivity, quality of life), personal factors (eg, stress, anxiety, depression) and environmental factors (eg, social support, access to technology). The ICF model is the WHO preferred framework for the assessment of health and disability at an individual and population level.24 Grouping the outcomes under specific ICF brackets was done by two authors independently (MH and ALS), and discussed in the case of disagreement. A narrative qualitative synthesis of results was undertaken for all included studies and supported by descriptive statistics of metadata. A secondary analysis, not a priori specified, was included to determine if specific outcome types are assessed in different settings using a χ2 test for categorical data.
Patient and public involvement
Patient or public were not involved in the design, conduct or reporting of this scoping review.
Results
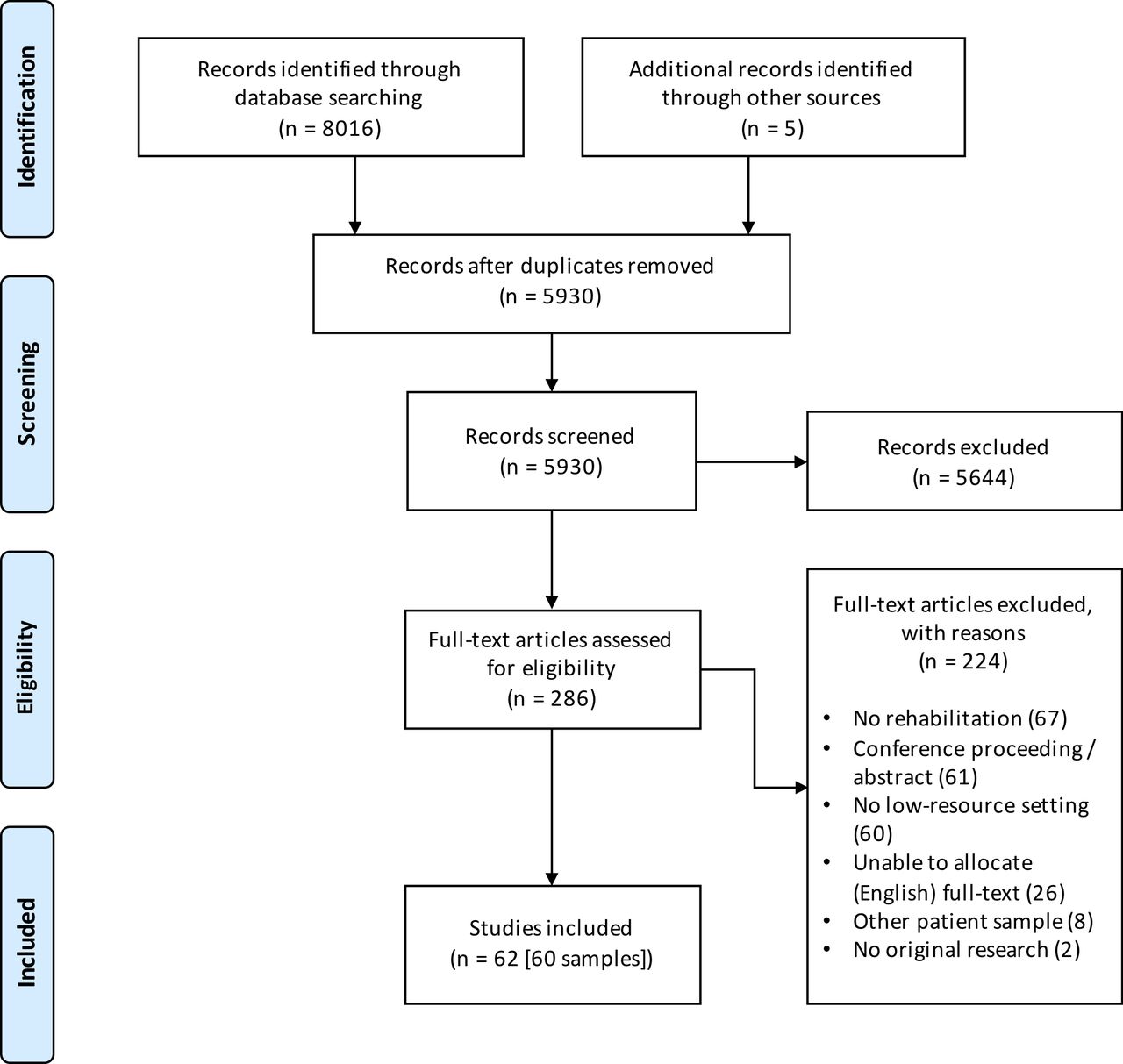
See figure 1 for a PRISMA flow chart. Of the 8021 records identified, 5930 remained after elimination of duplicates. An initial screening of titles in stage I and title/abstracts in stage II (n=1229) reduced this number to 286. The full-text versions of the remaining articles were reviewed for eligibility resulting in the exclusion of 224 for the reasons noted. Ultimately, 62 studies were included from the search, reporting on 60 unique patient samples.23 25–86

Study selection process.
Disease profile and geographical characteristics
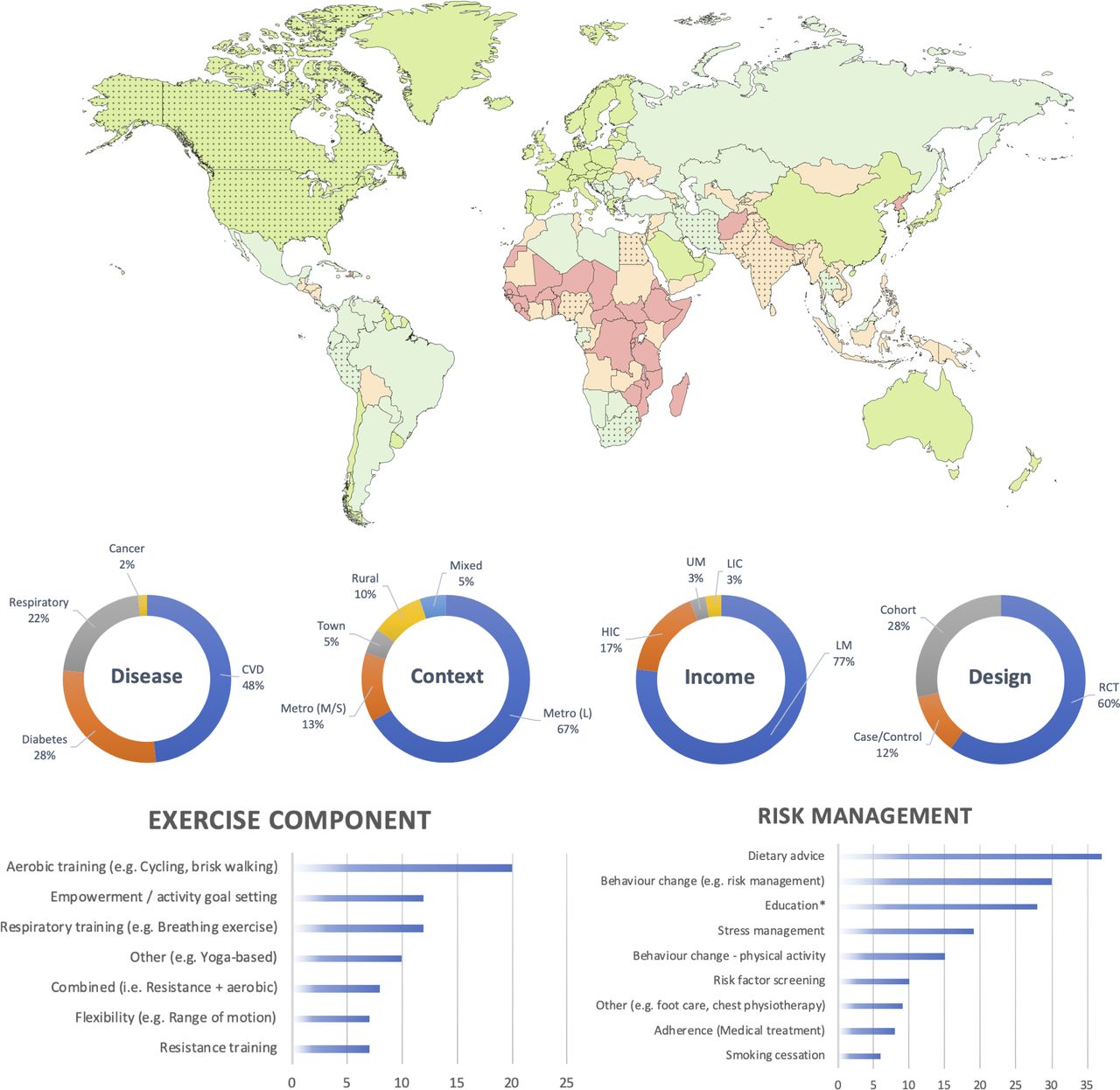
Figure 2 provides a graphical synthesis of the study characteristics including disease profile, geographical context, income classification, study design, exercise and risk management components included in the sample. A full table with all individual studies, their characteristics and rehabilitation programmes can be found in the online supplementary file 2. Twenty-nine studies included patients with CVD (48.3%), 17 studies (28.3%) included patients with diabetes, 13 studies (21.7%) involved patients with respiratory disease and a single study (1.7%) was found on patients with cancer. Studies were predominantly conducted in large metropolitan cities (n=40 (66.7%)) of LMs (n=46 (76.7%)). Two studies (3.3%) were identified in an LIC (both India) at the time of the conduct of the study (India later promoted to LM). In addition to studies in LICs and LMs, a proportion of studies were conducted in a low-resource context of either a UM (n=2 (3.3%)), or in an HIC (n=10 (16.7%)). The 10 studies in HICs targeted underserved or minority populations living in a poor socioeconomic context. Countries that were often represented included India (n=22 (36.7%)), Egypt (n=12 (20.0%)) and the USA (n=7 (11.7%)). Few studies were undertaken in sub-Saharan Africa (n=3 (5.0%)) and on the South American continent (n=1 (1.7%)). Thirty-seven (61.7%) studies were conducted in an academic setting or academic capacity (eg, university hospital, research providing intervention). A majority of studies (n=36 (60.0%)) did not receive or report funding; where studies were funded, most had national/government funding (n=19 (31.7%)), with fewer having international funding (n=3 (5.0%)), and 2 (3.4%) being self-funded.
Supplemental material
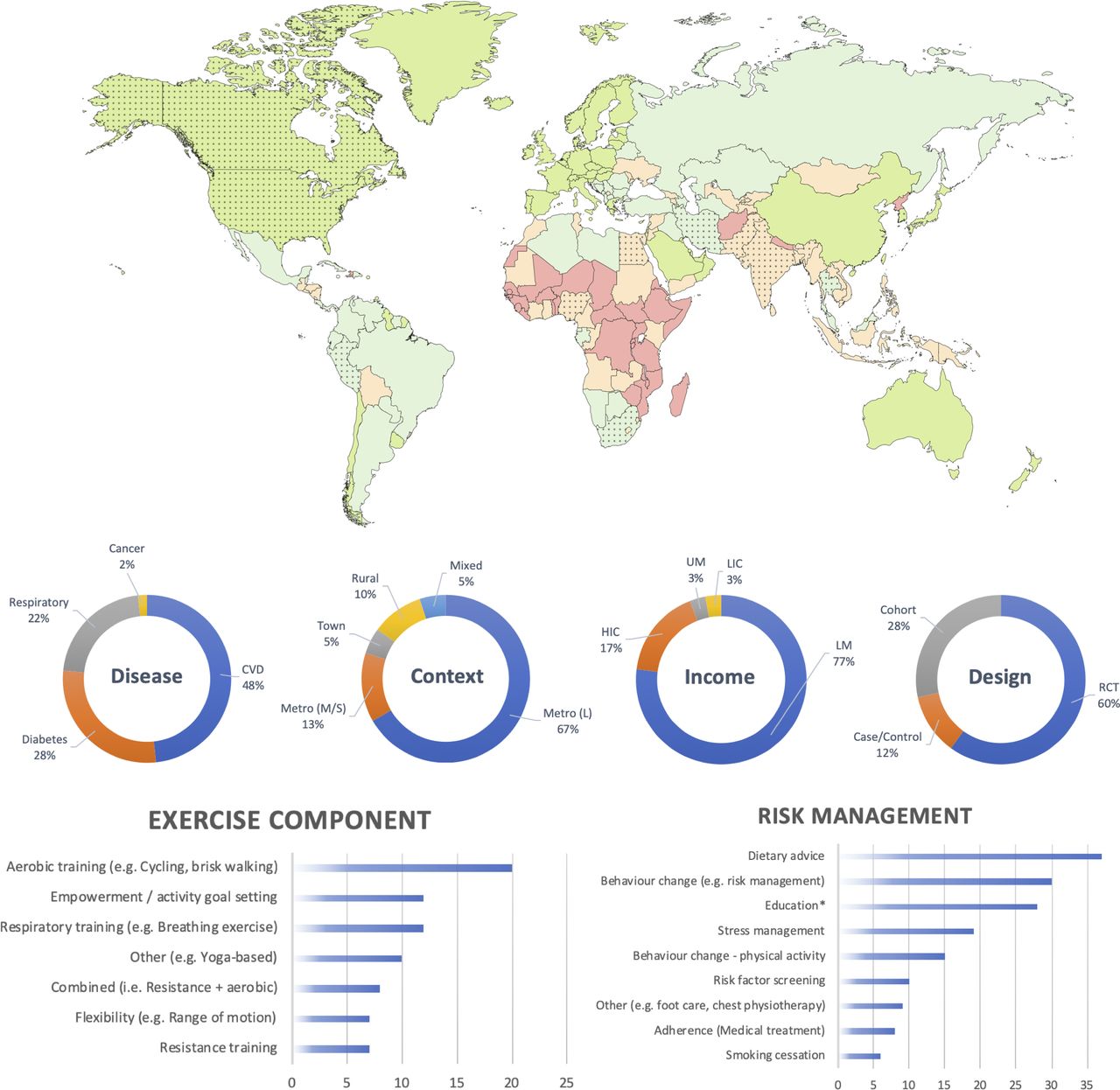
Graphical synthesis of results extracted from online supplementary file 2 (characteristics of included studies). Top: the world map of countries per 2016 World Bank income classification (low-income country (LIC), red; lower middle-income country (LM), orange; upper middle-income country (UM), light green; high-income country (HIC), dark green). Dotted countries are countries in which one or more studies were undertaken. Middle: percentage (%) of studies per disease group, geographical context, income classification and study design. Bottom left: number of studies that included a specific exercise component. Bottom right: number of studies that included specific other methods to control for risk factors. *Education pertains to, for instance, self-management, or knowledge of underlying pathology. CVD, cardiovascular disease; Metro, Metropolitan (S, Small; M, Medium; L, Large); RCT, randomised controlled trial.
Methodological characteristics
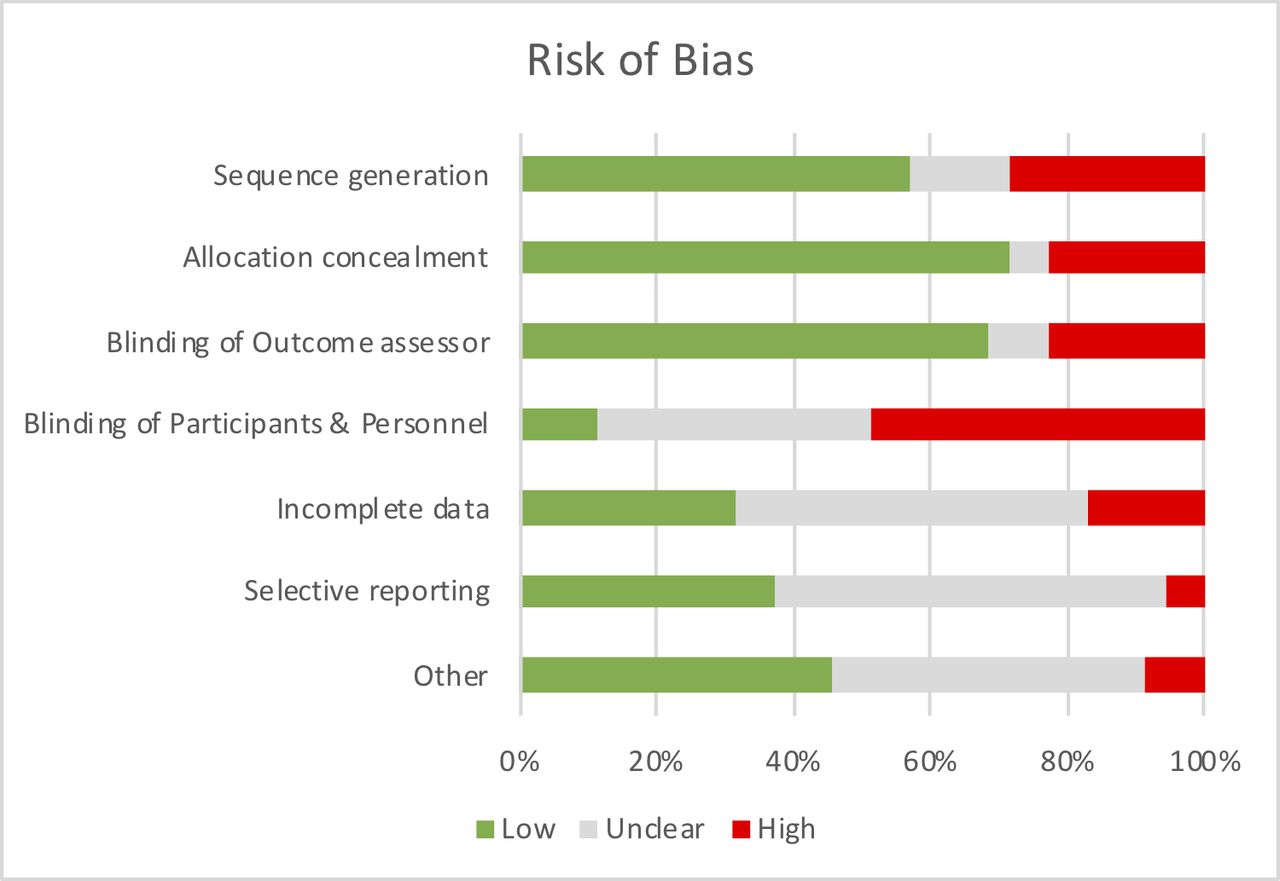
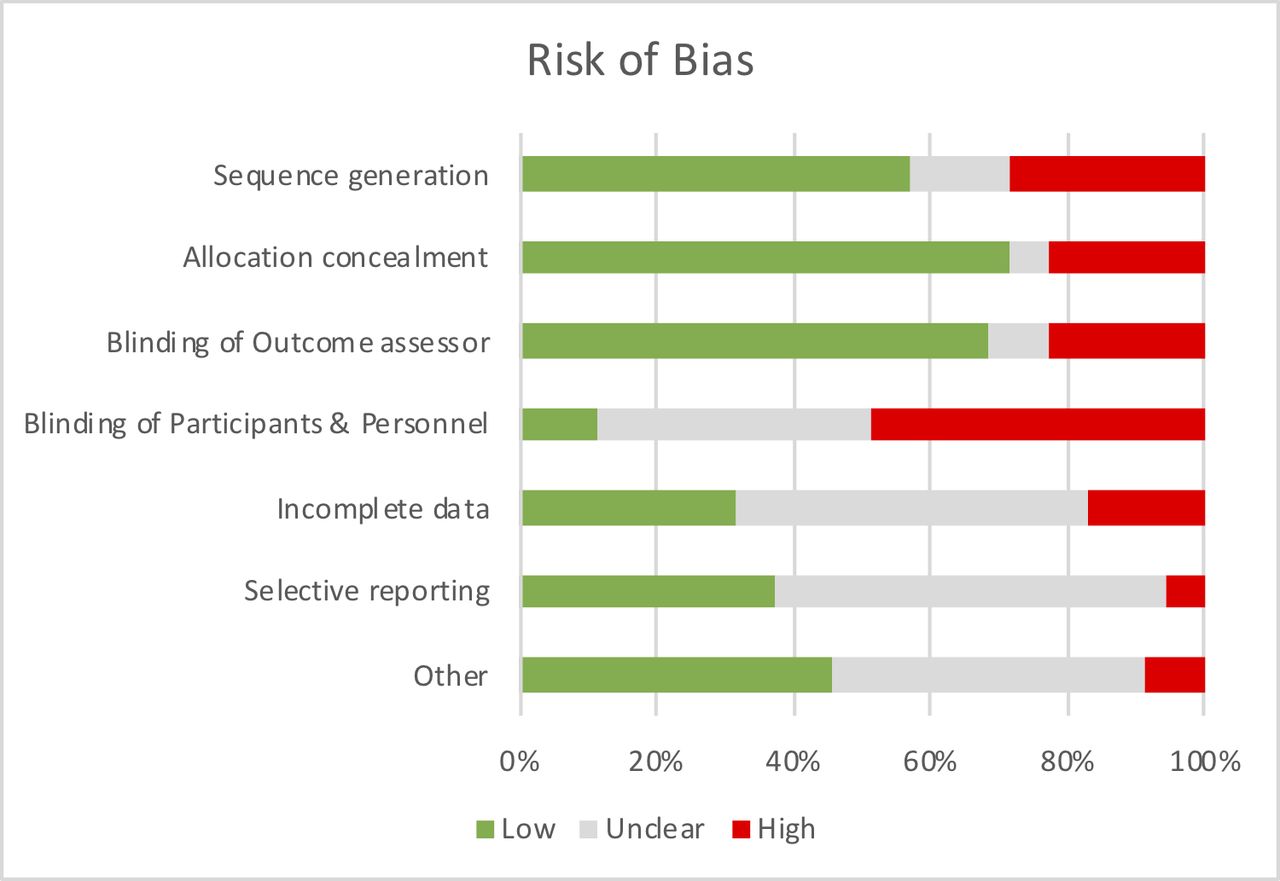
Seven (11.7%) of the studies used a case–control design, of which six were prospective (mean±SD=73.8±35.9 participants/study) and one retrospective (30 participants). Seventeen (28.3%) cohort studies were included, of which 15 were prospective (mean±SD=116.6±146.6 participants/study), and two were retrospective in design (mean±SD=463.5±598.9 participants/study). The remaining 36 studies (60.0%) were RCTs (mean±SD=94.0±80.7 participants/study). Nine RCTs (25.0%) reported a clinical trial registration. Fifteen (41.7%) reported a sample size calculation, of which nine achieved the calculated sample size (60.0%). Two studies (5.6%) were of high methodological quality (figure 3; online supplementary file 4). Risk of bias was found predominantly in the randomisation and allocation concealment (or reporting thereof). Two studies (3.4%) reported specific considerations in terms of the research methodology (eg, randomisation at study site level to enable focused allocation of resource, for instance,76 in the light of a rural context where individuals are geographically far apart).
Supplemental material
{kind=link}
{kind=link}
{kind=link}
Risk of bias of included randomised controlled trials (RCT) (n=36); see online supplementary file 4 for judgement per individual study.
Rehabilitation model and model adaptations
Online supplementary file 2 provides a per-study overview of the rehabilitation interventions delivered, their primary exercise component (eg, walking) and methods to manage risk factors (eg, smoking cessation). Figure 2 provides a graphical synthesis of online supplementary file 2. Table 1 provides a quantitative synthesis of the intervention delivery model (eg, outpatient). In most cases, rehabilitation was delivered on an outpatient (n=25 (41.7%)) or ‘hybrid’ (n=17 (28.3%); that is, supervised transitioning to unsupervised setting) basis. Most programmes comprised exercise and education (n=37 (61.7%)). Most rehabilitation was delivered by a variety of healthcare professionals including physiotherapists or community health workers (n=38 (63.4%); see online supplementary file 2 for details regarding the types of healthcare professionals). The mean duration of programmes was 18 weeks (SD=21; range=0.7–104.0); programmes offered a mean of 27 supervised sessions (SD=40; range 0–224) of 75 min in duration on average (SD=56; range=4–360). The nature of control groups differed across the studies. Eleven out of 36 RCTs (27.8%) had an active comparison group (eg, different exercise paradigm), 11 (30.6%) had a usual care control, 6 (16.7%) usual care plus a low-intensity add-on, 6 (16.7%) reported ‘no intervention’ for the control group, and for 2 (5.6%) studies it was not reported. Detailed reporting on the nature of usual care was often limited. However, based on 32 (94% of RCTs) studies, usual care generally consisted of pharmacological management plus an add-on component to control for attention (eg, dietary consultation (n=9, 26.5%)), pharmacological management only (n=6; 17.6%), education only (n=5; 14.7%), no management (n=4; 11.8%), medical management (n=4; 11.8%), conventional rehabilitation (n=3; 8.9%) or other (n=1; 2.9%).
Rehabilitation intervention characteristics by country income classification
Table 2 provides an overview of strategies to optimise the methodologies and intervention characteristics to accommodate contextual restraints. These strategies were either explicitly mentioned by the authors or were independently (MH and ALS) identified adaptations during data extraction. The most commonly reported strategies to accommodate such a setting were the adoption of alternative delivery models (eg, text messaging, home-based models, use of ‘non-conventional’ healthcare workers) and incorporating cultural aspects into the design of the intervention (eg, introducing yoga as an exercise component).
Considerations for rehabilitation in an LRS implemented in included studies
Outcomes
A total of 432 outcomes were extracted across the 60 studies (see online supplementary file 3); these were grouped according to the ICF24 into outcomes relating to body function and impairments (n=284 (65.7%)), activity limitations and participation restrictions (n=120 (27.8%)), personal factors (n=26 (6.0%)) or environmental factors (n=2 (0.1%)). Outcome measures that were reported most often included the 6 min walk test (n=20), body mass index (n=19) and blood pressure (n=17). There was no significant difference in the types of outcomes measured based on World Bank income classifications or study design. However, there was a significant difference in outcome types measured by NCD (χ2=39.7 (p<0.01)). A higher proportion of studies in patients with respiratory disease assessing outcomes related to activity limitations and participation restrictions compared with CVD and diabetes.
Supplemental material
Four studies (6.7%) reported specific feasibility outcomes (eg, participation rates, referral rates, hospitalisation) in relation to their study objective(s). When considering the included RCTs, uptake was on average (SD; number of studies) 54% (SD 32%; n=17), retention was 78% (SD 31%; n=35) and adherence to the experimental intervention 89% (SD 12%; n=5).
Discussion
Through this review, 60 studies were identified across four key contributors to the burden of NCDs. Alternative delivery models tested in the LRS were practical in circumventing resource-related barriers as indicated by the retention and adherence reported. Among others, these delivery models included transition to predominantly patient-driven, home-based rehabilitation, training of non-medical or non-conventional health workers (eg, community or auxiliary health workers, nurses), integration of rehabilitation in community (primary) health centres, or triage patients based on contextual factors (eg, distance to centre) or medical profile (eg, risk stratification, comorbidity profile). However, the methodological quality of the included studies was low, and often lacked outcomes that can drive policy and guideline development. Surprisingly, only a single study on the exercise-based rehabilitation of patients with cancer in an LRS was found, indicating that this particular field is still in its infancy. In addition, if we consider the increasing burden of NCDs in LRS, the small body of evidence for exercise-based rehabilitation in South America and (sub-Saharan) Africa particularly is concerning. In addition to the evidence that was not found, three important gaps could be derived from the research included in this review.
First, while a number of studies conveyed the need for low-cost or cost-effective models of rehabilitation to address the increasing burden of NCD in LRS, the studies in this review failed to include economic measures in their evaluations. In line with this, there was a paucity of studies reporting mortality and morbidity outcomes, which are typically used in health economic analyses to calculate DALYs. Also, none of the included studies administered the EuroQol-5 Dimension, a common outcome measure of health-related quality of life used for quantifying quality-adjusted life years (QALY). Unfortunately, the lack of these health economic measures (DALYs, QALYs) may hamper the incorporation of rehabilitation into policy guidelines and initiatives (eg, national health insurance). A synthesis of 19 studies on the cost-effectiveness of cardiac rehabilitation, all in UM or HIC, suggested that cardiac rehabilitation is cost-effective, especially with exercise as a component.87 There may be a myriad of reasons as to why health economic analyses are absent in LRS. First, there may be limited academic capacity in LRS to conduct and advise on health economic analyses as this is a relative new field within rehabilitation medicine. Second, the scarcity, quality and accessibility of data often attributable to the absence of financial cost registration and limited patient information systems to obtain rigorous data in morbidity and mortality, may impose significant challenges in the conduct of economical evaluations in LRS. A way forward may be to contest the notion that the cost-benefits of rehabilitation for NCDs in LRS should be expressed in relation to morbidity and mortality. Other indicators including socioeconomic parameters, equity measures, societal participation or food security may be considered more applicable alternatives. The other indicators may be more easily accessible to express the benefits relative to the cost, for both the provider as well as the direct (eg, out-of-pocket expenses for exercise equipment) and indirect (eg, transport) costs to the patient. With respect to the latter, only few studies (n=2) were identified in LICs where low cost-to-patient models are essential to prevent patients from falling into a medical poverty trap.88
Second, most studies included outcome measures related to body function and impairment whereas few studies reported (primary) outcomes on the level of activity (eg, mobility, physical activity) or participation (eg, productivity). While these physiological outcomes are essential in terms of reducing mortality, morbidity and, therefore, drive health policy, one may postulate that outcomes on the level of activity limitations and participation restrictions may be particularly of interest in low-resource environments, and more relevant to the field of rehabilitation medicine. With the average age for patients with NCD in LRS versus HIC being ~10 years younger,89 reporting on outcomes that measure participation restrictions could highlight the potential value of physical rehabilitation as an intervention. As patients suffering from NCD could still actively provide an active economic contribution, demonstrating the impact of rehabilitation on limiting productivity years lost may accelerate initiatives to increase access to rehabilitation in LRS.
Finally, there are few studies that detail the effect of alternative delivery models on access and uptake of rehabilitation interventions for NCDs. This is in addition to other potential external mechanisms that may increase uptake (eg, clinician education, financial incentives).90 The uptake of rehabilitation interventions reported in this review ranged substantially (11%–100%) and hampered by the large proportion of studies that was embedded in an academic setting. Going forward, it is therefore important that future studies in this field operate outside of the academic setting to increase the knowledge transfer and implementation from research to community, and better understand the impact of a particular delivery model on uptake and adherence measures.91 In the light of universal health coverage, and upscaling rehabilitation access in general, understanding contextual knowledge translation is an essential step in addressing the dearth of evidence on rehabilitation for NCDs in LRS as identified in the REHAB2030 call for action.
There are a number of limitations to this review. First, the data sources search for this review has been restricted to major databases (eg, Medline) and literature published in English. Subsequently, the 62 reports included in this review may not be entirely inclusive for the entire scope of work done. The absence of the Latin American and Caribbean Health Sciences Literature (LILACS) and Africa Wide literature database, for instance, may have resulted in a failure to identify studies specifically in the South American and African continents. However, despite the variety of populations included in this review (eg, diabetes, CVD), similar ‘themes’ emerged from these studies. Hence, the 62 studies included in this review provide a compelling overview of the scope of evidence.
Second, the concept of rehabilitation is ambiguous and there are a variety of definitions and models. This often involves individualised, person-centred elements that defy easy standardisation.92 This is also reflected in the broad search strategy used, and consequently the high number of exclusions/ineligible articles found. A sensible operationalisation of what constitutes rehabilitation may have improved the reliability when judging eligibility for this review. In this specific review, an exercise component was a prerequisite for inclusion as (A) particular rehabilitation models with an exercise component have been shown to be cost-effective,87 and (B) it would strengthen the agreement between reviewers during the inclusion process. While the mandatory inclusion of an exercise component as part of comprehensive rehabilitation is plausible in high-income contexts, we also need to consider that (1) physical inactivity may not always be the primary working mechanism behind the prevalence of NCDs and as such, this inclusion criterion may have resulted in a failure to identify studies relevant to this review,93 and (2) specifically in the context of alternative delivery models, even the definition of what constitutes exercise training (or rehabilitation in general) needs to be broadened.
A third construct that is ambiguous is that of a ‘low-resource setting’. Studies and reviews with a similar scope often opt to consider either LMIC (ie, World Bank classification) or developing countries (eg, Gini index) as more objective constructs to classify countries or study context. However, various studies in this review confirm that access and uptake of rehabilitation in a resource-constrained context is not limited to LMICs; challenging and complex circumstances are found both in HIC and UM as well. Conversely, also high-resource programmes are found in LMs. Hence, the definitions chosen in this review to some extent drive the generalisability of the results.
Conclusions
Various innovative considerations to address contextual factors of providing exercise-based rehabilitation within an LRS have been reported. In addition, the review highlights the paucity of data available on the potential impact of exercise-based rehabilitation on key policy drivers including mortality and morbidity, cost-benefits and outcomes on a participation level. The information summarised in this review can now be used by researchers in the planning of high-quality experimental studies to address the evidence deficit for exercise-based rehabilitation in the management of NCDs in LRS.
References
Footnotes
Handling editor Seye Abimbola
Twitter @m_heine01, @sherrylgrace
Contributors MH conceived the review. All authors (MH, ALS, MP, SG, WD, SDH) developed the methods. MH and ALS had primary responsibility for the analysis and initial draft of the manuscript. All authors contributed substantially to the analysis, interpretation of the results and completion of the manuscript. All authors approved the final manuscript.
Funding This study is funded by the AXA Research Fund (S005459).
Disclaimer The funder (AXA Research Fund) of the study had no role in study design, data collection, data analysis, data interpretation or writing of the report. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.