Article Text

Abstract
Background Brazil faces huge health inequality challenges since not all municipalities have access to primary care physicians. The More Doctors Programme (MDP), which started in 2013, was born out of this recognition, providing more than 18 000 doctors in the first few years. However, the programme faced a restructuring at the end of 2018.
Methods We construct a panel municipality-level data between 2008 and 2017 for 5570 municipalities in Brazil. We employ a difference-in-differences empirical approach, combined with propensity score matching, to study the impacts of the programme on hospitalisations for ambulatory care sensitive conditions and its costs. We explore heterogeneous impacts by age of the patients, type of admissions, and municipalities that were given priority.
Findings The MDP reduced ambulatory admissions by 2.9 per cent (p value <0.10) and the costs by 3.7 per cent (p value <0.01) over the mean. The reduction was driven by infectious gastroenteritis, bacterial pneumonias, asthma, kidney and urinary infections, and pelvic inflammatory disease. The results held on the subsample of municipalities targeted by the programme. By comparing the benefits of the programme from the reduction in the costs of ambulatory admissions to the total financial costs of the MDP, the impacts allowed the government to save at least BRL 27.88 (US$ 6.9 million) between 2014 and 2017.
Conclusion Addressing inequalities in the distribution of the medical workforce remains a global challenge. Our results inform the discussion on the current strategy adopted in Brazil to increase access to primary healthcare in underserved areas.
- health inequality
- medical workforce
- primary care
- ambulatory admissions
- cost–benefit analysis
- more doctors programme
- Brazil
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- health inequality
- medical workforce
- primary care
- ambulatory admissions
- cost–benefit analysis
- more doctors programme
- Brazil
Key questions
What is already known?
Inequalities in the distribution of the medical workforce remain a global challenge especially in low-income and middle-income countries.
The Mais Médicos Programme (More Doctors Programme) started in 2013 to address the shortage of doctors in deprived regions, but it was deeply restructured at the end of 2018 despite evidence of its effectiveness.
What are the new findings?
The MDP reduced hospitalisations for ambulatory care sensitive conditions and their costs, allowing the Brazilian government to save at least BRL 27.88 (US$ 6.9 million) between 2014 and 2017.
What do the new findings imply?
The results inform the discussion on the current strategy adopted by the Brazilian government.
Assuring the continuity of the efforts of medical workforce provision is necessary to protect deprived communities.
Introduction
The need to address inequalities in the distribution of the medical workforce was in the spotlights of policy discussions for several years. Despite its importance, few initiatives, aimed to improve attractiveness, recruitment, and retention of medical workforce, provided effective approaches to overcome this problem.1–5 The inequality in the distribution of health professionals remains a global challenge. The WHO identified a minimum density threshold of 22.8 skilled health professionals (doctors, nurses and other staff) per 10 000 people to provide basic health coverage.6 Yet, several countries worldwide do not reach this standard. Countries that reached the minimum recommended still face inequalities considering the workforce distribution between the most urbanised and remote corners. The global challenge of human resources for health is especially present in low-income and middle-income countries (LMICs).
Compared with developed countries, LMICs face more challenges regarding a multiple burden of diseases such as infectious diseases, high volumes of injuries, and increasing non-communicable conditions. To address this issue a strong primary care network is necessary.7 However, an adequate structure of primary care demands human resources policies capable of assuring the distribution of professionals where they are needed. Many countries conducted efforts to increase physicians’ availability using policies in four domains: education, financial incentives, regulation and service delivery reorganisation.5 Notwithstanding, new approaches are needed to attract and retain medical workforce in deprived and remote areas.
One novel example of a recent national programme, which addressed, in the short-term, inequalities in human resources for health, is the Brazilian Mais Médicos Programme (More Doctors Programme, MDP hereafter). The MDP was instituted by Law No. 12871, in 2013, and its primary objectives were to reduce the shortage of doctors in deprived regions of the Brazilian Unified Health System (Sistema Único de Saúde, SUS).8 The MDP encompassed three strategic strands: emergency provision of physicians to primary care teams, reorientation of medical training providing more undergraduate medical school places, and improvements in the infrastructure of primary care facilities.9 Part of the emergency supply effort of physicians was supported by the cooperation among the Cuba Ministry of Health, the Pan-American Health Organisation/WHO (PAHO/WHO) and the Brazilian Ministry of Health. This agreement was responsible for the deployment of Cuban doctors in underserved areas in Brazil.9–11
The Ministry of Health defined the profile municipalities eligible to enrol in the MDP, by taking into account the percentage of population living in extreme poverty, the gross domestic product (GDP) per capita, social vulnerability, and locations categorised as Special Indigenous Sanitary Districts (DSEIs). Municipalities that fitted these criteria were able to express interest in the participation to the MDP and adhere to it. The MDP was responsible for guaranteeing primary care access to 63 million people in more than 4000 municipalities, achieving a provision volume of 17 625 physicians in 2 years of programme.9 In October 2018, Cuban doctors were filling at least 8539 positions that became vacant the month after (figure 1). After the Ministry of Health gave a withdrawal notice of the Cuban doctors from the MDP in December of 2018, it published several calls aiming to recruit Brazilian physicians to replace the Cuban vacant positions. However, these calls were not successful as the number of places not filled kept increasing in 2019, leaving 1961 vacant positions as of April 2019 (figure 1).

Vacant positions in More Doctors Programme (MDP) (November 2018–April 2019). The figure shows the vacant positions in MDP, after the Brazilian Ministry of Health gave a withdrawal notice on 14th of November 2018. Data source: CNES: http://cnes.datasus.gov.br/
Several evaluative studies investigated the effectiveness of the MDP.9 12–15 Descriptive research12 14 15 showed that the MDP guaranteed access to and decreased health inequalities in the first years of the programme, by reducing physicians’ shortage and increasing access to primary care, especially in those municipalities who met the priority criteria.13 Lima et al 13 conducted a cross-sectional study, comparing physicians included or not in MDP in 2014, and showed that the programme increased medical appointments and referrals and community education activities.9 Santos et al 9 used a quasi-experimental, before-and-after evaluation of the MDP in remote and deprived populations, to show higher physician density and primary care coverage and decreased avoidable hospitalisations in enrolled municipalities after the start of the programme. A bibliometric study,16 analysing data from 81 manuscripts, also confirmed that 62% of the articles on MDP emphasise the positive results achieved.
Yet, there exist few rigorous quantitative evaluations, which attempted to estimate the causal impacts of the MDP on health indicators. Carrillo and Feres17 showed that the programme increased doctor visits and led to greater utilisation of doctors for prenatal care. However, they do not find evidence of gains in infant health, including birth weight, gestation and mortality. The closest study to ours is Fontes et al, 18 which estimated the impact of MDP on all types of hospitalisation for ambulatory care sensitive conditions (ACSH), and found a reduction in admissions.
However, despite these positive findings, the MDP was deeply restructured at the beginning of 2019 due to the termination of the cooperation among the Cuban government and PAHO/WHO. By 12 December 2018, 8568 Cuban doctors withdrew from the MDP, leaving several deprived regions without primary care.19 The Brazilian Ministry of Health was capable of filling 76.84% of the Cuban vacant places by April 2019, by mainly attracting doctors from regular Primary Care teams through better salaries and an installation grant. Nonetheless, the most deprived areas (more than 20% of the population living in extreme poverty) are still those facing the hard challenge to attract the interest of primary care physicians. The current Brazilian government aims at addressing the same challenges of the MDP through a new programme called Médicos pelo Brasil (Doctors for Brazil).20 Its objective remains the internalisation of doctors throughout the country, especially in the most remote and underserved regions, in addition to develop and intensify the training of medical professionals.
The goal of this paper is multifold. First, ACSH are a set of conditions for which access to effective primary care can reduce the likelihood of hospitalisation. Several studies show that high rates of ACSH are associated with poor service coverage and/or low primary care resolution for certain health problems, and thus ACSH remain a valuable indicator to monitor and evaluate healthcare policies.21 Using a mixed quasi-experimental approach, combining the use of difference-in-differences (DiD) and propensity score matching, we estimate the effectiveness of the MDP, between 2014 and 2017, on ACSH. We expect a negative relationship between the MDP—which increases access to primary healthcare—and ACSH, as shown in several studies.18 22–25 Furthermore, we estimate whether specific age groups or type of admissions explain the reduction in ACSH. Investigating the heterogeneity of the impacts is key for policy makers to direct resources more efficiently to where are needed. We argue that the MDP, which provide access to basic primary health services to 63 million people, might be more effective in reducing hospitalisations for children under 5 years old. If this is the case we would expect to find stronger impacts towards those groups of hospital admissions considered sensitive to the first level of children care, such as respiratory diseases or asthma, infectious gastroenteritis or other infectious diseases, compared with adult diseases such hypertension, diabetes or hearth failures.26 27 Second, we quantify the equivalent reduction in costs for ACSH for the Brazilian Ministry of Health. Third, the estimates of the impacts on these indicators (ACSH and its costs) are used as input to conduct a cost–benefit analysis exercise. By comparing the benefits from the reduction in ACSH and thus a reduction in costs of hospitalisations, to the total financial costs of the MDP, we estimate whether the MDP provided savings to the Brazilian government.
Methods
Data
To assess the impact of the MDP we used four data sources: (1) the Hospital Information System (SIH) from which we accessed ACSH and their costs; (2) the National Register of Health facilities (CNES)28 from which we obtained data on the doctors part of the programme yearly since 2013, (3) the Brazilian Institute of Geography29 from which we gathered economic and sociodemographic characteristics of municipalities, and (4) the publicly available financial report of PAHO/WHO for the volume of resources invested in the MDP.22
First, the SIH is responsible for processing information from hospital admission authorisation forms.30 The records at patient level, which are sent on a monthly basis to the Ministry of Health per each health facility, contain all admissions in the Brazilian public hospital system and their costs. A list of ACSH was developed by Alfradique et al,21 defining 19 different groups of admissions considered sensitive to the first level of care, based on the WHO international classification of diseases (ICD). We reconstructed the total number of ACSH and their costs per each municipality, by age and ICD group from the patient-level database.
Second, we built the age-standardised rates of ACSH for each of the 5570 Brazilian municipalities, comprising the time span from 2008 to 2017 by age group, and adjusted by the population (per 1000 people). The population size for each municipality was obtained through the Brazilian Health Data System (DATASUS) that includes the resident population by age range. We computed total population size for under 5 years old, between 5 and 19 years old and 20 or above years old. Since records are up to 2015, projections based on a population growth of 0.08%31 are implemented for the years 2016 and 2017.
Third, the CNES contains information about every facility providing care in Brazil. Among the indicators monitored there is a register of each professional providing assistance in a specific unit. It was then possible to categorise which health facilities had a physician enrolled in the MDP. We aggregated these data at the municipality level to determine which municipality received the MDP at each point in time starting from 2013.
Finally, the financial report published by PAHO details the investment performed to mobilise the Cuban doctors to the underserved municipalities. This report is published annually, detailing the amount of financial resources spent in the emergency provision of doctors. This information was used to support the cost–benefit analysis.
Online supplementary table S1 shows that over the period 2014–2017, 74% of the municipalities received the MDP, with the majority (68%) receiving at least one MDP doctor. On average each municipality has 2.73 MDP doctors, covering 38% of the population. Age-standardised ACSH are higher for under 5 years old children (19.6 over 1000 people) and similar for 20 or more years old people (16.2). Age-standardised ACSH for 5–19 years old people are instead 7.08 over 1000. Costs for ACSH in each municipality are on average 11 329 BRL (US$ 2795), with ACSH for adults (11 635 BRL, US$ 2870) costing about nine times the ACSH for under 5 years old children, and 26 times the costs of ACSH for 5–19 years old people. About 30.31% of the municipalities in the data are defined as priority.
Supplemental material
Patient and public involvement
Patients or member of the public were not involved in this study. The study only uses the publicly available data sources described in previous section (see Data section).
Empirical analysis
To estimate the impact of the MDP on the number of ACSH and their costs, we implement a DiD empirical strategy, which compares changes in the outcome of interests over time for municipalities which participate and do not participate in the MDP. Specifically, we use the timing of the MDP as the source of time variation, and the availability of at least one MDP doctor as the source of cross-sectional variation. The basic empirical specification is as follows:

where  refers to the outcomes of interest, such as ACSH and costs, in municipality
i
in year
t
.
refers to the outcomes of interest, such as ACSH and costs, in municipality
i
in year
t
.  is an indicator variable equal to 1 if the year is 2014, 2015, 2016, 2017, while
is an indicator variable equal to 1 if the year is 2014, 2015, 2016, 2017, while  is equal to 1 whether the municipality has at least one MDP doctor. The empirical model also includes municipality (
is equal to 1 whether the municipality has at least one MDP doctor. The empirical model also includes municipality ( ) and time (
) and time ( ) fixed effects, which absorb fixed differences across municipalities and across years.
) fixed effects, which absorb fixed differences across municipalities and across years.  are standard errors clustered at the level of the municipality.32
are standard errors clustered at the level of the municipality.32
This basic empirical specification is then extended to an event-study model, where we capture the full dynamics of the programme, by studying the effects of the MDP on our outcomes of interest, relative to the start of the programme (October 2013 is the first month of the MDP), as follows:

where  is an indicator taking value 1 if it is year
k
relative to the first year of the MDP and the municipality received the programme (
is an indicator taking value 1 if it is year
k
relative to the first year of the MDP and the municipality received the programme ( ). We make the normalisation
). We make the normalisation  , so that all coefficients represent differences in outcomes relative to the first year of the MDP (2013). The interpretation of
β
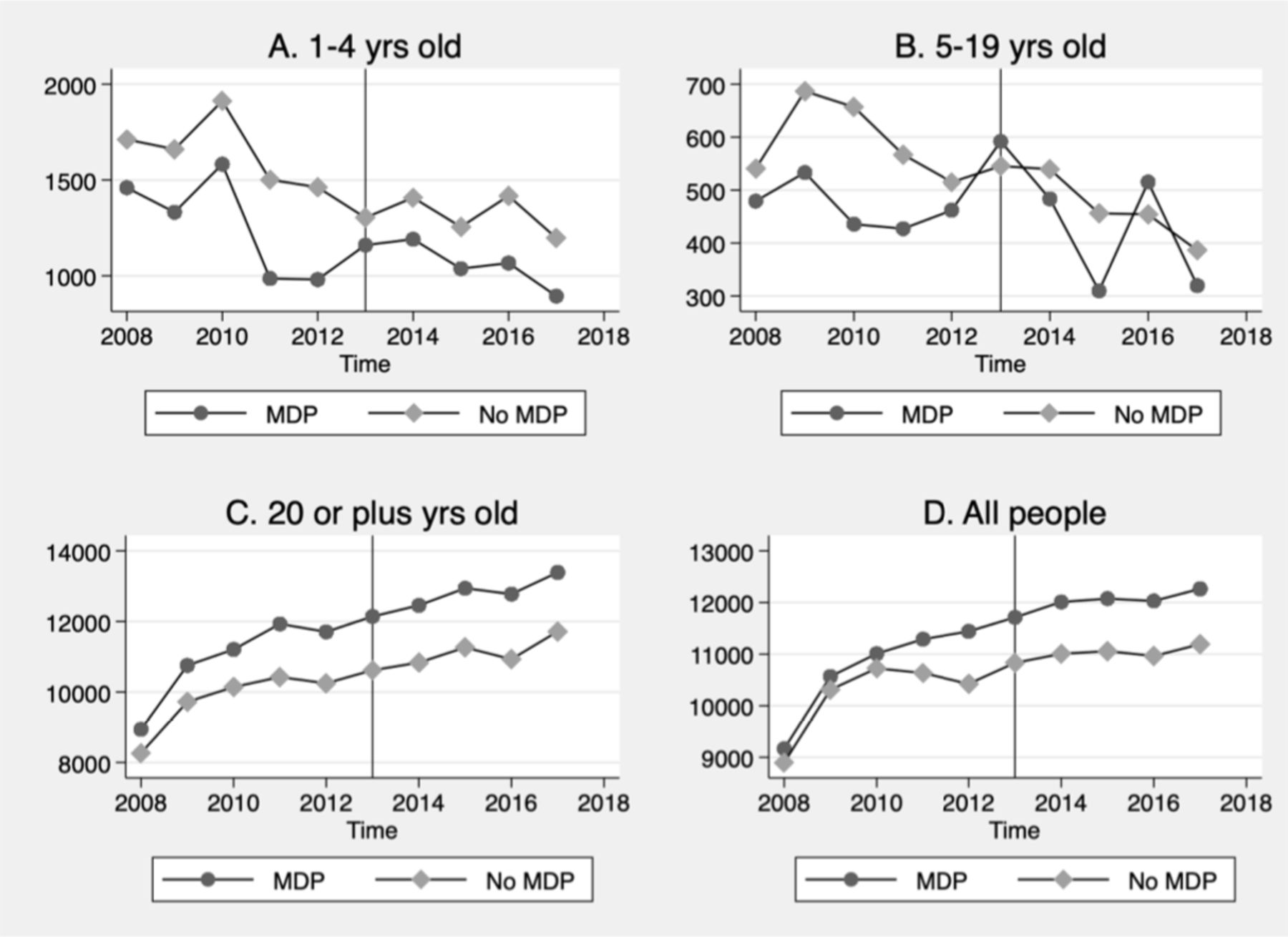
as causal impact of the MDP relies on the identifying assumption that, in the absence of the programme, treated and untreated municipalities have similar trends in the outcomes of interests. Figures 2 and 3 explore this assumption by showing the trends in the number of ACSH (figure 2) and costs (figure 3) over time. The graphs suggest that the trends are overall parallel between treated and untreated municipalities with the exception of figure 2C and figure 3B age groups. The second test of the identification assumption relies on analysing the dynamics in the coefficients in equation 2, conditional on time and municipality fixed effects. Specifically, the treated and untreated municipalities should follow parallel trends in the years before the MDP, which implies that
, so that all coefficients represent differences in outcomes relative to the first year of the MDP (2013). The interpretation of
β
as causal impact of the MDP relies on the identifying assumption that, in the absence of the programme, treated and untreated municipalities have similar trends in the outcomes of interests. Figures 2 and 3 explore this assumption by showing the trends in the number of ACSH (figure 2) and costs (figure 3) over time. The graphs suggest that the trends are overall parallel between treated and untreated municipalities with the exception of figure 2C and figure 3B age groups. The second test of the identification assumption relies on analysing the dynamics in the coefficients in equation 2, conditional on time and municipality fixed effects. Specifically, the treated and untreated municipalities should follow parallel trends in the years before the MDP, which implies that  coefficients should not be statistically different from zero. Results in online supplementary figures S1 and S2 show the coefficients before and after the programme. The graphs suggest that the
coefficients should not be statistically different from zero. Results in online supplementary figures S1 and S2 show the coefficients before and after the programme. The graphs suggest that the  coefficients are not always 0 before the beginning of the programme. However, this is not surprising since more disadvantaged municipalities were targeted by the MDP and were more likely to adopt it than advantaged areas.
coefficients are not always 0 before the beginning of the programme. However, this is not surprising since more disadvantaged municipalities were targeted by the MDP and were more likely to adopt it than advantaged areas.

Pretrends of the number of age-standardised ambulatory admissions (1000 people) for 1–4 years old, 5–19 years old, 20 and plus years old and all people. The figure represents the number of age-standardised ambulatory admissions in treated (more doctors programme, MDP) and non-treated (no MDP) municipalities over time from 2008 to 2017, by age group: the top-left panel (A) includes 1–4 years old; top-right panel (B) includes 5–19 years old; the bottom-left panel (C) includes 20 or plus years old, and the bottom-right panel (D) includes all people.

Pretrends of the costs of age-standardised ambulatory admissions (in BRL, per 1000 people) for 1–4 years old, 5–19 years old, 20 and plus years old and all people.The figure represents the costs of age-standardised ambulatory admissions in treated (more doctors programme, MDP) and non-treated (no MDP) municipalities over time from 2008 to 2017, by age group: the top-left panel (A) includes 1–4 years old; top-right panel (B) includes 5–19 years old; the bottom-left panel (C) includes 20 or plus years old, and the bottom-right panel (D) includes all people.
We then decide to improve this empirical specification, by combining the DiD with a propensity score approach (PSM).33 34 Given the existing differences in observables between treated and untreated municipalities, we aim at creating a better match between these two groups based on economic and sociodemographic characteristics. Despite a reduction in sample size, this method increases our confidence that the two groups of municipalities (on the matched sample) are more comparable.
We proceed by matching municipalities based on observable characteristics at the beginning of our panel (2008). These characteristics, for a total of 43 covariates, include: (1) economic indicators: GDP per capita, governmental expenditures (in log, total and by type—health, infrastructure, education, welfare, agriculture), transfers to municipalities (in log), exports (in log, million); (2) health indicators: infant mortality, low-weight and premature births, births with low APGAR (Appearance, Pulse, Grimace response, Activity, Respiration) score (less than 7 over 10) at 5 min, and births with anomalies; (3) healthcare access: number of health facilities (total, private, public, other), total number of health staff (total, private, public, other), including number of doctors and nurses (expressed in 100 000 people); (4) employment: percentage of people employed (total, female and male), monthly payroll, number of plans and firms; (5) sociodemographics: population and working age population (total, female and male), population by age group (1–4 years old, 5–19 years old, 20 or plus years old), total fertility rate, crude birth rate, and crude death rate. To improve the propensity score matching, we imposed a calliper of 0.0005 in the logit regression of being an ever-treated municipality on these covariates. The procedure resulted in 47 230 municipalities (32 650 treated) matched by propensity score with replacement, considering the entire panel of 5570 municipalities from 2008 to 2017.
Figure 4 shows that the bias across these covariates is reduced when we implement the PSM. Online supplementary table S2 assesses the comparability of the matched and unmatched samples, by presenting summary statistics of the covariates in the two samples and testing the statistically significance in the percentage reduction in bias. Online supplementary figure S3 also shows the distribution of the probability (p score) for the treated and untreated municipalities, after the propensity score matching approach. This evidence suggests that the matched sample is much more similar than the unmatched one on these observable characteristics. We argue that this identification strategy is the best to analyse the effects of the programme, as done in other past studies.17 18

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Bias reduction in propensity score approach implementation (unmatched vs matched sample). The figure represents the standardised bias across each of the economic and sociodemographic covariates of the municipalities, comparing the unmatched with the matched sample. Covariates in 2008 include: (1) economic indicators: gross domestic product per capita, governmental expenditures (in log, total and by type—health, infrastructure, education, welfare, agriculture), transfers to municipalities (in log), exports (in log, million); (2) health indicators: infant mortality, low-weight and premature births, births with low APGAR score (less than 7 over 10) at 5 min, and births with anomalies; (3) healthcare access: number of health facilities (total, private, public, other), total number of health staff (total, private, public, other), including number of doctors and nurses (expressed in 100 000 people); (4) employment: percentage of people employed (total, female and male), monthly payroll, number of plans and firms; (5) sociodemographics: population and working age population (total, female and male), population by age group (1–4 years old, 5–19 years old, 20 or plus years old), total fertility rate, crude birth rate and crude death rate. All the variables are reported in online supplementary table S2.
Cost–benefit analysis
This study will use the impacts estimated of the MDP on ACSH and the reduction in the costs as inputs in a cost–benefit analysis exercise. The goal of this last part of the analysis is to compare the benefits generated in term of reduction in number of ambulatory admissions and the corresponding reduction in costs, with the total financial costs of the MDP, to investigate whether the impacts of the MDP represented—in net—a benefit or a cost to the Brazilian government. The total costs of the MDP will include costs for (1) international flights; (2) local flights; (3) scholarships monthly training stipend and (4) documents’ management and training of Cuban doctors.22 The analysis will estimate the total benefits (as reduction in costs of ACSH) for the government as a percentage of the total financial costs of the MDP.
Results
Effects of MDP on ambulatory admissions and costs
Results in table 1 shows a statistically significant effect of 1.159 as a reduction in the number of age-standardised ACSH per 1000 people for under five children over the duration of the programme (2014–2017). This effect corresponds to a reduction in the number of ACSH of about 5.3 per cent over the mean of 21.76 admissions per 1000 people (column 1). Similar results are reflected in the total number of age-standardised ACSH (3.1 per cent, column 4). We find statistically significant results for 20 or plus years old people (column 3), but not for 5–19 years old age group (column 2). The results are driven by negative changes (not always statistically significant) year by year from 2014 to 2017. More interestingly, we find that this reduction in ACSH corresponds to a statistically significant reduction in costs. Over the duration of the programme, we find a reduction in costs for all admissions (column 8) of 483.909 BRL (4.4 per cent over the mean). These estimates are primarily driven by reductions in costs of adults (column 7). Overall, ACSH are reduced following the implementation of the MDP and this corresponds to a reduction in costs.
The effects of More Doctors Programme (MDP) on the number of age-standardised ambulatory admissions (1000 people) and costs (1000 people, in BRL) for 1–4 years old, 5–19 years old, 20 and plus years old and all people
Estimates are similar if we restrict our sample to municipalities which were prioritised in the implementation of the MDP (table 2), as defined by those who have at least 20% of the population in extreme poverty or were among the 100 with more than 80 000 inhabitants, with lowest level of per capita public revenue and high social vulnerability of inhabitants (see online supplementary figures S4 and S5 for pretrends on this subsample of municipalities). Table 2 shows a statistically significant reduction in the number of age-standardised ACSH mainly for the subsample of children under 5 years old (table 2, column 1). However, all coefficients on ACSH and costs are negative as expected. Online supplementary table S3 also shows similar negative, but not statistically significant, coefficients for the subsample of municipalities without priority. Online supplementary table S4 includes a linear time trend for each municipality and shows that the estimates of the impacts of the MDP on ACSH and costs are not statistically significant, confirming that treated and untreated municipalities might be different to start with.
The effects of More Doctors Programme (MDP) on the number of age-standardised ambulatory admissions (1000 people) and costs (1000 people, in BRL) for 1–4 years old, 5–19 years old, 20 and plus years old and all people, for the subsample of municipalities with priority
Effects of MDP on ambulatory admissions and costs, by type of admissions
To support our argumentation that the results are primarily driven by the MDP, and not by other observable factors that could be correlated with the type of municipalities treated, we present similar results using a PSM in addition to the DiD empirical model. Table 3 shows that the estimates on the matched sample (our preferred specification) are similar to the DiD results (table 1), confirming the results that the MDP reduced both the age-standardised ACSH and the costs associated to it. We find a reduction of 0.874 ACSH, corresponding to 4.1 per cent over the mean for children under 5 years old (column 1). We find similar statistically significant reduction for the sub-sample of 20 or plus years old people and the full sample (2.7 and 2.9 per cent over the mean). We also find a statistically significant reduction in costs of 415.263 BRL over the duration of the programme (column 8), corresponding to about 3.7 per cent change over the mean of 11 093 BRL for the entire sample of people.
The effects of More Doctors Programme (MDP) on the number of age-standardised ambulatory admissions (1000 people) and costs (1000 people, in BRL) for 1–4 years old, 5–19 years old, 20 and plus years old and all people, for the subsample of municipalities matched by the propensity score approach
Focusing on ACSH for the entire sample of people, we explore which types of admissions explain the results. Among the 19 different categories of admissions, we describe that the reduction in ACSH and costs are driven by infectious gastroenteritis and complications, bacterial pneumonias, asthma, kidney and urinary infections and pelvic inflammatory disease (table 4). Admissions decrease by eight per cent over the mean for infectious gastroenteritis and complications, by 18 per cent for bacterial pneumonias, and by 39 per cent for pelvic inflammatory disease. These findings are in line with the fact that the MDP lead to reductions in admissions for the first level of children care (columns 1 and 3), and for an adult women’s disease (column 9). Similarly, costs decrease by 9.7 per cent for infectious gastroenteritis and complications, by 26 per cent for bacterial pneumonias, by 20 per cent for kidney and urinary infections, and by 34 per cent for pelvic inflammatory disease. We do not find statistically significant evidence on any other group (not shown).
The effects of More Doctors Programme (MDP) on the number of age-standardised ambulatory admissions (1000 people) and costs (1000 people, in BRL) for all people, by international classification of diseases (ICD) group
Cost–benefit analysis
This section aims at evaluating the costs and benefits from the MDP, in terms of ACSH, for the sample of all people. We find that the programme reduced the number of ambulatory admissions (table 5, column 2), and this corresponded to a reduction in costs (table 5, column 4). What are the benefits for the Brazilian government implementing the programme, compared with the total costs of the MDP? Table 5 estimates the total benefits (the reduction in costs) for the government from 2014 to 2017 (table 5, column 6), as a percentage of the total costs of the MDP, which account for more than $1 billion per year (Table 5, column 1 and as computed in Silva et al 35).
Cost–benefit analysis
From our data, we assume that the average population per treated municipality is 42 400 and the number of ever-treated municipalities is 4103. In table 5, we compute the estimated reduction in number of ambulatory admissions for all people (column 3): the average over the period 2014–2017 is a reduction of 85 420 ACSH per treated municipality. Additionally, we evaluate the estimated reduction in costs (column 5) in the treated municipalities, based on the average population and the estimated impacts of the programme (columns 2 and 4). We find that the MDP costs in total about BRL 5.7 billion from 2014 to 2017 (column 1), while the reduction in ambulatory admissions costs for all people amounts to BRL 84.18 million over the same period (column 5). Thus, the benefits for the Brazilian government, in term of savings from the positive effects of the MDP, correspond to about 24.21% of the total costs, which, in absolute value (BRL 84.18 million, US$ 20.7 million), are economically important. The results are similar, but muted, if the same calculations are computed from the estimates of the impacts of MDP on ACSH and costs on the matched sample (panel B). The benefits for the Brazilian government, in this latter case, correspond to about 8.07% of the total costs, for a total of BRL 27.88 (US$ 6.9 million).
Discussion
This paper finds evidence that the MDP in Brazil provided benefits to strengthen primary healthcare. In line with previous evidence, we find a statistically significant reduction in the number of ACSH due to the MDP emergency medical provision strand. Through a DiD estimation, combined with a PSM, the MDP reduces ACSH by 2.9 per cent and the costs by 3.8 per cent over the means. We also conduct a cost–benefit exercise, by comparing the benefits from the reduction in ACSH and its costs, to the total financial costs of the MDP. We find that the impacts of the programme allowed the Brazilian government to save at least BRL 27.88 (US$ 6.9 million) between 2014 and 2017.
The MDP is a pioneer national initiative to reduce the shortage of medical workforce, by providing access and ensuring coverage in primary healthcare to underserved areas. There is no other programme worldwide of a similar size, in terms of volume of professionals deployed and the amount of resources invested.9 19 However, the Cuban withdrawal from the MDP at the end of 2018 could negatively impact the healthcare provision in remote communities.19 Despite the attempt of the Ministry of Health to open emergency selection processes to replace Cuban doctors with Brazilian ones, by the end of April 2019 several vacancies were still unfilled.
The recent political changes in Brazil demanded a rearrangement of the programme logic. The MDP, as similar programme in other countries (Mission Barrio Adentro in Venezuela,36 National Health Services Loan Repayment Programme in the USA,37 and Overseas Trained Doctors in Australia38) represents a short-term solution to address the problem of scarcity and inequality in the distribution of the primary care physicians. However, in the long-term, the governments need to solve the inherent problems related to the access to primary healthcare with more comprehensive national policies. The Brazilian Ministry of Health released on 1 August 2019 a new programme called Médicos pelo Brasil (Doctors for Brazil), aimed at replacing the MDP,39 which has the goal to improve the availability of primary physicians throughout the country, especially in the most remote regions. However, as it is structured today, this programme does not plan to replace the same sustainable parts of the MDP. Among the three strands of the MDP, Médicos pelo Brasil fully includes the emergency provision of physicians in underserved areas. It also includes the expansion of post-graduate medical training, but it does not provide more undergraduate medical school places, and it does not include improvements in the infrastructure of primary care facilities.
More specifically, the Médicos pelo Brasil programme aims to fill 18 000 vacancies in municipalities facing a lack of primary care. The new criteria for enrolment divide municipalities into five categories, considering population size, demographic density and distance from large urban centres: remote rural, adjacent rural, remote intermediate, adjacent intermediate and urban. Priority will be given to remote rural, adjacent rural and remote intermediate municipalities, which comprise 3400 cities, as well as DSEIs. Adjacent and urban intermediate municipalities will receive physicians if located in regions considered highly vulnerable, based on the proportion of registered persons receiving financial or social security benefits. During the first 2 years in the Médicos pelo Brasil Programme, all physicians will join a post-graduate training in primary care. Each doctor will receive a net worth monthly salary of BRL 12 000.00 with a bonus of BRL 3000 if the doctor is based in rural and intermediate locations, and an additional BRL 6000 for the doctors in DSEIs. At the end of the training, the physicians will receive the title of specialist in Family and Community Medicine, allowing them to be hired through the Consolidation of Labour Laws (CLT). Contracting through CLT will allow physicians to grow in their career with four-level salary progression (from BRL 21 000 to BRL 31 000). They will also potentially receive a bonus for performance (between 11% and 30% of their salary), linked to the achievement of indicators of quality of care and satisfaction of people served. This evaluation of physicians in the programme will help to strengthen the quality of primary healthcare in Brazil.
Our analysis is not without limitations. First, we used data on the costs of each admission as registered through the SIH system. The SIH registers the costs of admissions covered by the Brazilian Ministry of Health, but states and municipalities with their own financial resources cover other costs. Thus, the costs used in this analysis are under-estimated. Second, we use the municipality as the unit of analysis. However, each municipality is characterised by multiple realities.40 The physicians involved in the MDP usually are allocated in more deprived regions within each municipality. Future research should explore differences within each municipality. Third, when fitting a municipal linear time trend for each municipality, the additional allowed heterogeneity and the loss of statistical power make the estimates overall not statistically significant. The main finding in the reduction of ACSH remain robust only for the group of children under 5 years old. Finally, since our analysis only focuses on ACSH and its costs, the cost–benefit analysis underestimates the benefits of the MDP. Including the positive effects of the programme on other health indicators may increase the cost-savings of the programme.
Strategies similar to the MDP could be used to overcome temporary challenges in inequalities in human resources for health. However, fostering the health system to achieve universal health coverage requires more complex and long-term strategies. The Brazilian Ministry of Health is taking steps forward to replace the MDP, and the release of the Médicos pelo Brasil programme may represent a first step for another solution to the inequality in the medical workforce distribution. We hope that the results of this study inform the discussion on possible pathways to improve the access to primary healthcare and to assure universal health coverage.
References
Footnotes
Handling editor Sanni Yaya
Twitter @CatherineStato1
Contributors EMM, TAHR, JRNV conceived the idea of the study. EMM and TAHR extracted the data. EMM did the analysis. EMM and TAHR drafted the manuscript. GV, CR, CS, JRNV revised the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data are publicly available.