Article Text

Abstract
Introduction Identifying design features and implementation strategies to optimise community health worker (CHW) programmes is important in the context of mixed results at scale. We systematically reviewed evidence of the effects of proactive case detection by CHWs in low-income and middle-income countries (LMICs) on mortality, morbidity and access to care for common childhood illnesses.
Methods Published studies were identified via electronic databases from 1978 to 2017. We included randomised and non-randomised controlled trials, controlled before–after studies and interrupted time series studies, and assessed their quality for risk of bias. We reported measures of effect as study investigators reported them, and synthesised by outcomes of mortality, disease prevalence, hospitalisation and access to treatment. We calculated risk ratios (RRs) as a principal summary measure, with CIs adjusted for cluster design effect.
Results We identified 14 studies of 11 interventions from nine LMICs that met inclusion criteria. They showed considerable diversity in intervention design and implementation, comparison, outcomes and study quality, which precluded meta-analysis. Proactive case detection may reduce infant mortality (RR: 0.52–0.94) and increase access to effective treatment (RR: 1.59–4.64) compared with conventional community-based healthcare delivery (low certainty evidence). It is uncertain whether proactive case detection reduces mortality among children under 5 years (RR: 0.04–0.80), prevalence of infectious diseases (RR: 0.06–1.02), hospitalisation (RR: 0.38–1.26) or increases access to prompt treatment (RR: 1.00–2.39) because the certainty of this evidence is very low.
Conclusion Proactive case detection may provide promising benefits for child health, but evidence is insufficient to draw conclusions. More research is needed on proactive case detection with rigorous study designs that use standardised outcomes and measurement methods, and report more detail on complex intervention design and implementation.
PROSPERO registration number CRD42017074621.
- child health
- health services research
- systematic review
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
While many low-income and middle-income countries (LMICs) are adopting community health worker (CHW) programmes as an evidence-based strategy to achieve global health goals, the expected benefits have not been realised in all contexts.
Recent reviews for developing global guidelines to optimise CHW programmes found a scarcity of evidence on best practices for CHW education, deployment and management.
What are the new findings?
Proactive case detection of common childhood illnesses by CHWs in LMICs may reduce infant mortality and increase access to effective treatment compared with conventional community-based healthcare delivery (low certainty evidence).
Studies assessing the effects of proactive case detection showed considerable diversity in terms of participants, interventions, comparisons, outcomes and study quality.
What do the new findings imply?
Proactive case detection may be more effective than conventional community-based healthcare delivery in achieving child health gains.
More implementation research is needed with rigorous study designs and standardisation of outcomes to optimise the design and implementation of CHW programmes for impact.
Introduction
Community health worker (CHW) programmes are experiencing a resurgence as a strategy to achieve health-related sustainable development goals. Many low-income and middle-income countries (LMICs) have implemented integrated Community Case Management (iCCM) of common childhood illnesses,1 2 a package of services delivered by CHWs to diagnose, treat and refer children under 5 with malaria, diarrhoea, pneumonia and malnutrition in the community setting.3 This strategy has shown an increase in access to care and reduced child mortality.4–12 However, the expected benefits have not been realised in all contexts.13–18 Several recent evaluations of national iCCM programmes in Burkina Faso, Ethiopia and Malawi did not find impacts on care-seeking or child mortality.19–22
These programmes shared certain design features that may have contributed to the lack of overall effects by not addressing barriers to care, such as user fees for services,23–25 lack of adequate CHW supervision,26–28 or provision only for patients who sought care from a fixed site. As more countries scale up CHW programmes, it is critical to understand how to best design and implement iCCM, and CHW services more broadly, in order to realise their full potential.
A recent series of systematic reviews to inform WHO guidelines for optimising CHW programmes found a scarcity of evidence on best practices for several key policy areas, including CHW training, supervision and deployment, and calls specifically for more research on CHW workflow.29 We conducted a systematic review of the evidence for the effectiveness of proactive case detection by CHWs to improve access to care and reduce morbidity and mortality. By proactively seeking out patients at home to offer diagnosis and treatment or referral, a proactive workflow has the potential to overcome barriers to care, including direct and indirect costs, distance, mistrust and gender inequality, reduce the time from onset of a condition to services, and consequently reduce disease progression and mortality.
Methods
Inclusion criteria
Study designs
Studies from LMICs involving community-based, proactive case detection of common childhood illnesses were identified. Anticipating that randomised trials of healthcare service delivery would be very few, we included a broader range of study designs in line with Cochrane Effective Practice and Organisation of Care (EPOC) group recommendations.30 These included randomised controlled trials (RCTs) and non-randomised controlled trials (NRCTs), controlled before–after (CBA) studies, interrupted time series (ITS) and repeated measure studies.
Interventions and comparisons
To be eligible for inclusion, studies needed to evaluate a primary healthcare intervention that included proactive case-finding home visits by CHWs for the purpose of searching for and identifying, through history and/or diagnostics, cases of common childhood illness, including malaria, diarrhoea, pneumonia, malnutrition, HIV or tuberculosis. These conditions were chosen because they are covered by international protocols for iCCM of common childhood illnesses31 and/or contribute a substantial disease burden in LMICs. Studies needed to compare proactive healthcare delivery to usual or supplemented primary care available from facilities and/or CHWs that did not involve home visits for the purpose of identifying sick patients.
CHWs and trial participants
In accordance with earlier reviews, a CHW was defined as any lay health worker who received training to perform tasks related to primary healthcare delivery but had not received professional medical or paramedical education.32 Recipients of proactive case-finding home visits had to include children under 5 years of age.
Outcomes
We included studies if they assessed any of the following outcomes: (1) mortality among children under 5 years of age or infants aged 0–11 months; (2) prevalence or incidence of disease; (3) hospitalisation; (4) access to healthcare services; (5) harms or adverse effects; (6) costs or economic effects.
Our review focused on assessing proactive case detection as an adjoint to iCCM. As causes of neonatal deaths in LMICs differ from those of post-neonatal child deaths, we did not include studies that were restricted to neonates, that is, intervening solely in the neonatal period and reporting solely on neonatal outcomes. Nevertheless, we retained studies from our search that assessed childhood illness starting from the first day of life and reported outcomes separately for neonates and infants.
Search strategy
We searched the following electronic databases for studies meeting the eligibility criteria, in addition to contacting researchers with expertise relevant to the review topic:
MEDLINE Ovid (1946 to September Week 4 2017) (searched 10 October 2017);
Embase (1947 to 2017 October 20) (searched 23 October 2017);
Global Health Database (1910 to 2017 Week 41) (searched 23 October 2017);
Cochrane Central Register of Controlled Trials (searched 9 November 2017);
WHO Library (searched 30 November 2017).
The search strategy included terms to capture the following concepts describing the intervention: (i) proactive case detection—broad search terms were used to maximise sensitivity given a lack of MeSH terms for this concept; (ii) CHWs—search terms were adapted from a review by Lewin and colleagues32 and (iii) condition. A combination of two methodological search filters was adapted to capture a fourth concept for appropriate study design: (iv) the sensitivity-maximising Cochrane MEDLINE filter for RCTs and an EPOC filter for non-randomised trials. The search included publications since 1978, the year of the Alma-Ata Declaration, which marked a restructuring of the global health agenda towards primary healthcare provision by CHWs. No language restrictions were applied. Full strategies and results are provided in online supplementary file 1.
Supplemental material
Data collection and analysis
Selection of studies
Studies retrieved from the search were uploaded onto Covidence, a Cochrane technology platform for systematic reviews.33 Two reviewers (CW and JT or JG) independently screened titles, abstracts and full-text articles for eligibility. Inclusion was determined by consensus or in consultation with a third reviewer (JT or JG).
Data extraction and quality assessment
Two reviewers (CW and EW) independently extracted data from included studies related to study identification, methods, population, interventions, implementation of intervention, outcomes and results using a data extraction form designed in Covidence. Two reviewers (CW and EW) independently assessed the quality of included studies using the EPOC risk of bias tool for studies with a separate control group;34 allocation concealment was removed from the quality assessment criteria as reviewers deemed this domain inapplicable due to the nature of the intervention under review. Consensus on data extraction and quality assessment was reached in discussion or in consultation with a third reviewer (JT or JG).
Data synthesis
We reported measures of effect in the same way that study investigators reported them and synthesised them by type of outcome. For studies with a separate control group, we included only the measure of effect derived by comparing the intervention group to the control group, if multiple comparisons were reported. For studies with no separate control group, we included baseline to end-line comparisons. We calculated risk ratios (RRs) for dichotomous data to allow for comparisons across studies. If appropriate denominators (eg, number of live births for mortality outcomes) were not reported, we used population estimates reported in the study to approximate the denominator. We calculated 95% CIs, adjusting for clustering using the intracluster correlation coefficient (ICC) reported in the study, if available.35 If not available, we used a conservative ICC of 0.05 for all studies with a cluster design, as the ICC was <0.001 in the three studies for which it was reported. We assessed heterogeneity across studies for each outcome type both qualitatively and quantitatively using the I2 statistic, which describes the percentage of total variation across studies that is due to heterogeneity rather than chance.36 Two reviewers (CW and JT or JG) independently assessed the certainty of evidence for each analysis using the Grading of Recommendations, Assessment, Development and Evaluation approach,37 38 which takes into account study design, risk of bias, inconsistency, indirectness/applicability, imprecision and strength of association. Consensus was reached through discussion or in consultation with a third reviewer (JT or JG).
Results
Characteristics of included studies
Excluding duplicates, a total of 442 abstracts were screened for eligibility (figure 1 in online supplementary file 2). Fourteen studies were included, including five cluster RCTs (table 1). Complete information on the characteristics and risk of bias for each study is available in online supplementary file 3.
Supplemental material
Supplemental material
Characteristics of included studies evaluating proactive case detection of common childhood illnesses by community health workers
Study settings
Among the 14 included studies, seven were from Africa (three KwaZulu-Natal, South Africa,39–41 two Mali,42 43 one Ethiopia44 and one Senegal.45 The two reports from Mali42 43 and the two from rural South Africa,40 41 respectively, studied the same interventions delivered to the same populations, differing only with regard to when—and in South Africa, how—impact was assessed. Six studies were from Southeast Asia (three India,46–48 one Bangladesh,49 one Nepal50 and one Pakistan.51 Two reports from Haryana, India47 48 evaluated the same intervention delivered to the same population but assessed different outcomes. One study was from the Americas, in Dominican Republic.52 Four studies took place in urban or periurban settings,39 42 43 52 and eight in rural settings;40 41 44–46 49–51 the studies in Haryana47 48 did not indicate whether the setting was rural or urban.
Study designs and outcomes
The KwaZulu-Natal, South Africa39–41 and Haryana, India47 48 studies were cluster RCTs that evaluated a range of access to care, morbidity and mortality outcomes; the rural South Africa study did not report outcomes separately for children under 5 years.40 41 Two studies were NRCTs that measured morbidity outcomes;49 52 the Bangladesh study did not report outcomes separately for children under 5 years.49 The Nepal study50 that used a non-randomised, stepped-wedge design to assess risk of death among infants and children did not compare results between early and late treatment groups. Instead, it compared annual risks to baseline and used a test for trend to assess programme maturity. This study was therefore considered in this review to be an uncontrolled before–after study from baseline to end-line.
Four studies used a CBA design44–46 51 and reported percent differences or difference-in-differences for mortality, morbidity or access to care outcomes. However, some did not use the baseline or control group appropriately. The Pakistan study51 reported different baseline years for intervention and control areas; therefore, this study was deemed a NRCT and only the postintervention comparison between groups was presented in this review. The Ethiopia study44 presented a number of before–after access to care indicators for the intervention group, but only present before–after data for the comparison group for one outcome, the tuberculosis case notification rate; outcomes were not reported separately for children under 5 years. Finally, the Mali studies42 43 were included as ITS designs; yet, with only one baseline, they lacked a comparative preintervention trend and thus were treated in the review as uncontrolled before–after studies from baseline to end-line.
Participants
Half of the studies extended CHW services to the entire population,42–45 49 53 54 among which only the Mali studies42 43 reported outcomes specifically for children under 5 years. Five studies recruited pregnant women and delivered a mother–child intervention during the neonatal period, and in some cases, into infancy and childhood.39 46–48 52 The remaining two studies tested interventions that targeted children under 5 years of age during a period of 3 years.50 51
Characteristics of CHW programmes
The Bangladesh,49 Ethiopia,44 Senegal,45 rural South Africa40 41 and more recent India47 48 studies provided supplemental training in the context of the study (two-half days in Bangladesh, 1 day in Senegal, 8 days in India, 60 days in South Africa and unreported in Ethiopia) to CHWs from an already established CHW cadre. The remaining studies evaluated CHW programmes initiated by a research institute, all of which recruited local, literate community members and trained them for a duration of 60 hours52 to 6 months.46 In half of all programmes, CHWs were exclusively or predominantly female. Reporting of recipient and CHW sample sizes, and therefore CHW to population ratios, was poor.
Eleven studies reported enhanced CHW supervision as an adjunct to the intervention. However, the supervision strategy and frequency were not adequately described. Supervisors included physicians,46 nurses,51 accredited social health activists47 48 or senior project staff42 50 who monitored CHW activities periodically. Other studies employed a dedicated cadre of CHW supervisors, either based at the facility40 41 or in the community.43 44 Eleven studies paid CHWs for their work, with a salary in-line with government standards,39 43 44 50 a performance-linked46 or task-based47 48 remuneration scheme, or some other form of payment.40 41 45
CHWs provided services for the range of conditions eligible for inclusion in the review. CHWs in Mali,42 43 India46–48 and periurban South Africa39 provided integrated management of common neonatal and childhood illnesses. CHWs provided care exclusively for diarrhoea in Bangladesh;49 for pneumonia in Pakistan and Nepal;50 51 for malaria in Senegal;45 for malnutrition and at risk of being overweight in Dominican Republic;52 for tuberculosis in Ethiopia;44 and for HIV, tuberculosis, and sexually transmitted infections in rural South Africa.40 41 In addition to proactive case detection, most studies included doorstep treatment by CHWs and referral to a facility if necessary, with the exception of the studies in Dominican Republic, Ethiopia and periurban South Africa,39 44 52 which limited postdetection activities to referral for treatment and home-based follow-up.
Most studies compared proactive case detection by CHWs to the standard of care—passive case detection at public or private health facilities; six studies also included passive case detection by CHWs in the control arm. The South African studies included control CHWs who conducted home visits for purposes other than proactive case detection. Control arm CHWs conducted one pregnancy and two postnatal home visits to assist with securing identity documents and social grants in the urban study,39 and home visits to promote and refer clients to HIV counselling and testing in the rural studies.40 41
Risk of bias of included studies
Risk of bias summaries are provided in online supplementary file 2 (figure 2 and figure 3). Risk of bias assessments for each study are provided in online supplementary file 3. These assessments were considered when interpreting the results and certainty of evidence for each outcome.
Selection bias
All studies, with the exception of those in Mali,42 43 allocated the study area into intervention and control groups. Five studies used cluster randomisation to assign groups.39–41 47 48 Among seven studies that did not use random allocation, sufficient evidence was provided in only two45 46 that outcome measurements were similar between groups at baseline, and in only three46 50 52 that population-level and/or cluster-level characteristics were similar between groups at baseline.
Performance bias and detection bias
Due to the nature of the intervention, blinding of participants and study personnel to allocation assignment was not possible and was scored high risk for all included studies. All six Southeast Asian studies46–51 and the periurban South Africa study39 blinded outcome assessors to allocation assignment, earning a low detection bias score.
Attrition bias
Reporting of incomplete outcome data varied considerably between studies. Studies involving pregnant women for a neonatal intervention discussed attrition bias with the use of a trial profile.39 47 48 52 A Data Safety and Monitoring Board stopped the Haryana, India trials early after the required sample size had been met, but prior to about half of children completing the 12-month assessment.47 48 Risk of attrition bias was high in the Dominican Republic study where roughly a quarter of mother–child dyads were lost, and there were statistically significant differences in some baseline characteristics that could be associated with the outcome between those who completed follow-up and those who did not.52 Missing survey data for date of birth and death were imputed in the Mali studies, but the extent and patterns of missing data were explicitly reported.42 43 Studies from India46 and Nepal50 did not comment on completeness of outcome data, but data were collected by an independent set of workers and analysed on an intention to treat basis. CBA studies in Pakistan51 and Senegal45 relied on CHWs to collect outcome data in intervention clusters and employed periodic surveys in control clusters. These studies did not discuss incomplete outcome data and were scored high risk due to the differences in data source and methods between the two groups.
Reporting bias
A published protocol was found for only one study.39 No studies reported outcomes in the methods that were then subsequently omitted from the results and, therefore, no studies were scored as being at high risk of reporting bias. Some studies subsequently added outcomes from posthoc analyses, but provided justifiable reasons for inclusion of the additional outcomes that were not prespecified.39 47 48
Protection against contamination
Risk of bias due to contamination was scored as low when large units of allocation were chosen and efforts to minimise contamination were discussed and/or a map was provided showing geographic separation of groups.44 46–50
Effects of interventions
Eleven studies assessed the effects of proactive case detection of common childhood conditions by CHWs on mortality, morbidity or access to curative services and were included in the main analysis. Meta-analysis was deemed inappropriate as the studies in each analysis represented considerable clinical diversity with respect to intervention and participant characteristics, methodological diversity with respect to study design and risk of bias, and statistical heterogeneity as quantified by the I2 statistic. We were unable to explore this heterogeneity by prespecified subgroup analyses due to the limited number of studies. Overall, the certainty of evidence is low or very low because of limitations in study design, indirect measures of effect due to cointerventions or comparisons and unexplained heterogeneity.
Mortality
Seven studies measured mortality outcomes (table 2; Figure 1). Proactive case detection may reduce neonatal mortality (low certainty evidence). However, the effects vary and it is possible that it makes little or no difference to neonatal mortality (calculated RRs: 0.43 to 1.07; I2=79.1%). Proactive case detection may reduce infant mortality (calculated RRs: 0.52 to 0.94; I2=61.9%) (low certainty evidence). It is uncertain whether proactive case detection reduces mortality among children under 5 years (calculated RRs: 0.04 to 0.80; I2=94.4%) because the certainty of this evidence is very low.
Intervention effects on mortality outcomes
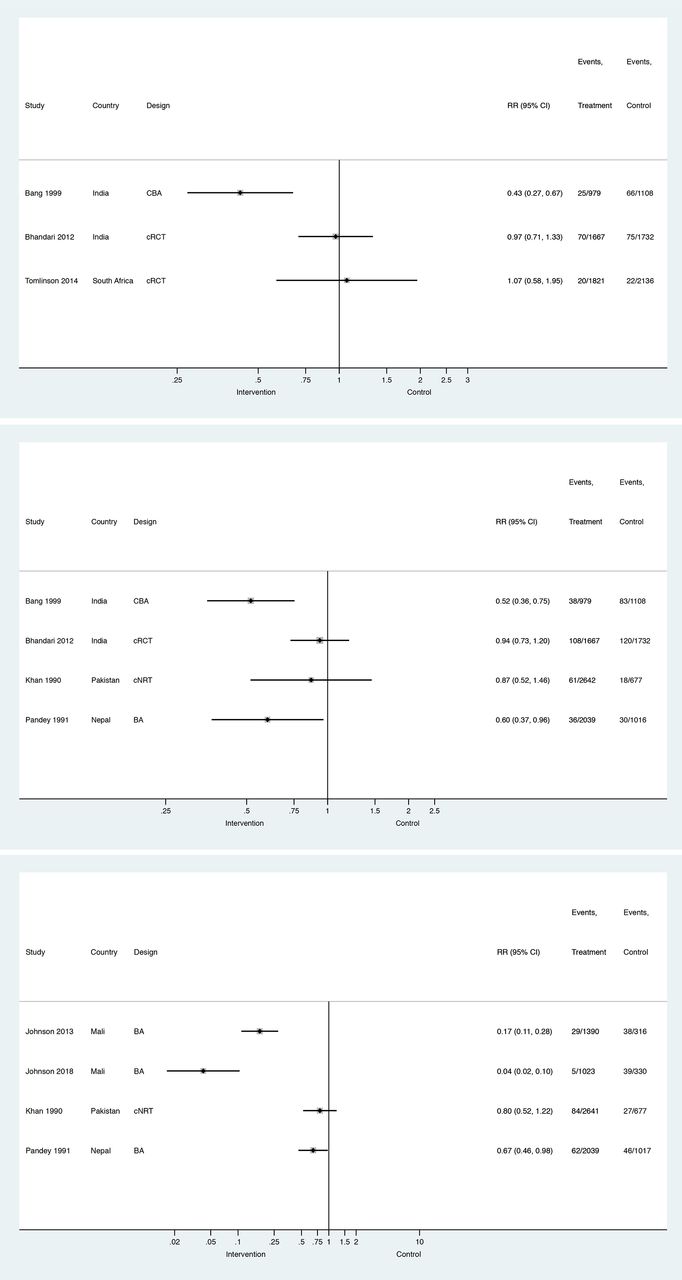
Forest plots for neonatal (top), infant (middle) and under 5 (bottom) mortality. CBA, controlled before–after; RR, risk ratio.
Three studies assessed impact on neonatal mortality over a 2–3 year timeframe (table 2; Figure 1). It was the primary outcome in the Maharashtra46 and Haryana47 studies of proactive case detection of newborn and infant danger signs, infections and illnesses. In rural Maharashtra, there was a 62% reduction in intervention areas compared with control areas (p<0.001).46 In Haryana, the neonatal mortality rate beyond the first 24 hours of life was lower in intervention clusters than in control clusters (adjusted HR=0.86; 95% CIs: 0.79 to 0.95), but not the case for the neonatal mortality rate overall—an effect, they explained, due to the higher than expected proportion of neonatal deaths occurring in the first 24 hours on which the intervention was unlikely to have had an effect.47 In both Maharashtra and Haryana, intervention groups included a mother’s education component and system strengthening in terms of user fee removal for CHW care46 or training of other provider cadres in Integrated Management of Newborn and Childhood Illnesses.47 An exploratory analysis of the effect of a home visit programme in periurban South Africa to improve appropriate infant feeding and HIV-free infant survival39 on neonatal mortality showed an increased risk of death in intervention compared with control clusters, although the effect was not statistically significant (RR=1.07; 95% CIs: 0.69 to 1.63).
Four Southeast Asia studies assessed infant mortality. The Maharashtra46 and Haryana47 studies found significant reductions (respectively, 45.7%; p<0.001 and AHR=0.89; 95% CIs: 0.78 to 1.00) in infant mortality between intervention and controls. Proactive case detection of childhood respiratory infection and doorstep treatment of suspected pneumonia compared with facility-based care led to reductions in infant mortality in rural Nepal,50 where cotrimoxazole was provided at home free of charge, and in rural Pakistan,51 where CHWs treated at home or referred to facilities where treatment protocols had been standardised. In Nepal, the greatest reduction in mortality after 3 years of intervention activities was seen in infants aged 6–11 months (RR=0.36; 95% CIs: 0.24 to 0.56). In Pakistan,51 the infant mortality rate was 74/1000 in the intervention area during the first 2 years of the study compared with 93/1000 in the control area.
A reduction in mortality was seen for all children under 5 years of age in Nepal, with a relative risk reduction of 0.72 from baseline to year 3,50 and in Pakistan, with a 26% reduction between intervention (29/1000) and control (39/1000) areas during the first 2 years of the study.51 In periurban Mali, the under-5 mortality rate declined from 154/1000 at baseline to 25/1000 after 3 years of proactive case detection of common childhood conditions in addition to primary health centre reinforcements and removal of user fees, and to 7/1000 after 7 years.43
Morbidity
Six studies assessed prevalence of disease, and four assessed hospitalisation (table 3; Figure 2). Proactive case detection may improve nutritional outcomes (low certainty evidence), although the effects vary, and it is possible that it makes little or no difference to nutritional outcomes (calculated RRs range from 0.61 to 1.16; I2=61.4%). It is uncertain whether proactive case detection reduces the prevalence of infectious diseases (calculated RRs: 0.06 to 1.02; I2=90.6%) or hospitalisation (calculated RRs: 0.38 to 1.26; I2=94.5%) because the certainty of this evidence is very low.
Intervention effects on morbidity and access to care outcomes

Forest plots for prevalence of common childhood infections (top) and nutritional conditions (middle), and hospitalisation (bottom). BA, before–after; CBA, controlled before–after; RR, risk ratio.
In Mali42 43 and rural Senegal,45 proactive case detection of malaria led to significant reductions in the odds of febrile illness among children under five (adjusted OR (AOR) after 7 years=0.45; 95% CIs: 0.32 to 0.62), and symptomatic malaria among the general population in intervention villages compared with control villages (AOR=0.03; 95% CIs: 0.02 to 0.07), respectively. The Haryana48 study found significant reductions in danger signs (adjusted RR (ARR)=0.82; 95% CIs: 0.67 to 0.99) and local infection (ARR=0.91; 95% CIs: 0.71 to 1.17) among neonates, as well as diarrhoea (ARR=0.63; 95% CIs: 0.49 to 0.80) and pneumonia (ARR=0.60; 95% CIs: 0.46 to 0.78) among infants. The urban South Africa39 and Dominican Republic52 studies found no effects on childhood diarrhoea, a secondary intervention outcome.
The Dominican Republic52 study found that monthly home visits and mother’s groups to promote healthy babies and monitor physical growth during the first 2 years of life led to reductions in stunting (AOR=0.50; 95% CIs: 0.22 to 1.10) and risk of overweight (AOR=0.43; 95% CIs: 0.23 to 0.77), compared with standard facility-based controls. The Haryana48 study found no effect on wasting (ARR=0.99; 95% CIs: 0.94 to 1.04) or stunting (ARR=1.10; 95% CIs: 0.90 to 1.36) at 12 months of age in exploratory analyses. The South Africa39 study found an increase in infant weight-for-age (mean difference (MD)=0.09; SD: 0.00, 0.18) and length-for-age (MD=0.11; SD: 0.03, 0.19) z-scores, but not weight-for-length (MD=0.01; SD: -0.07, 0.09).
In Bangladesh,49 CHW home visits to inquire about diarrhoea and offer oral rehydration therapy packets free of charge were associated with a 29% reduction (p<0.01) in hospitalisation for diarrhoea compared with control villages with CHWs doing ‘surveillance and health work’. In the Haryana48 study, in which CHWs assessed newborns for signs of illness at each visit and treated or referred them, caregivers in the intervention clusters reported fewer hospital admissions during infancy (ARR=0.67; 95% CIs: 0.51 to 0.88). In the South Africa39 and Dominican Republic52 studies, where proactive CHWs did not offer doorstep treatment but referred all cases detected, caregivers reported more hospital admissions for their children, although results were not statistically significant.
Access to treatment
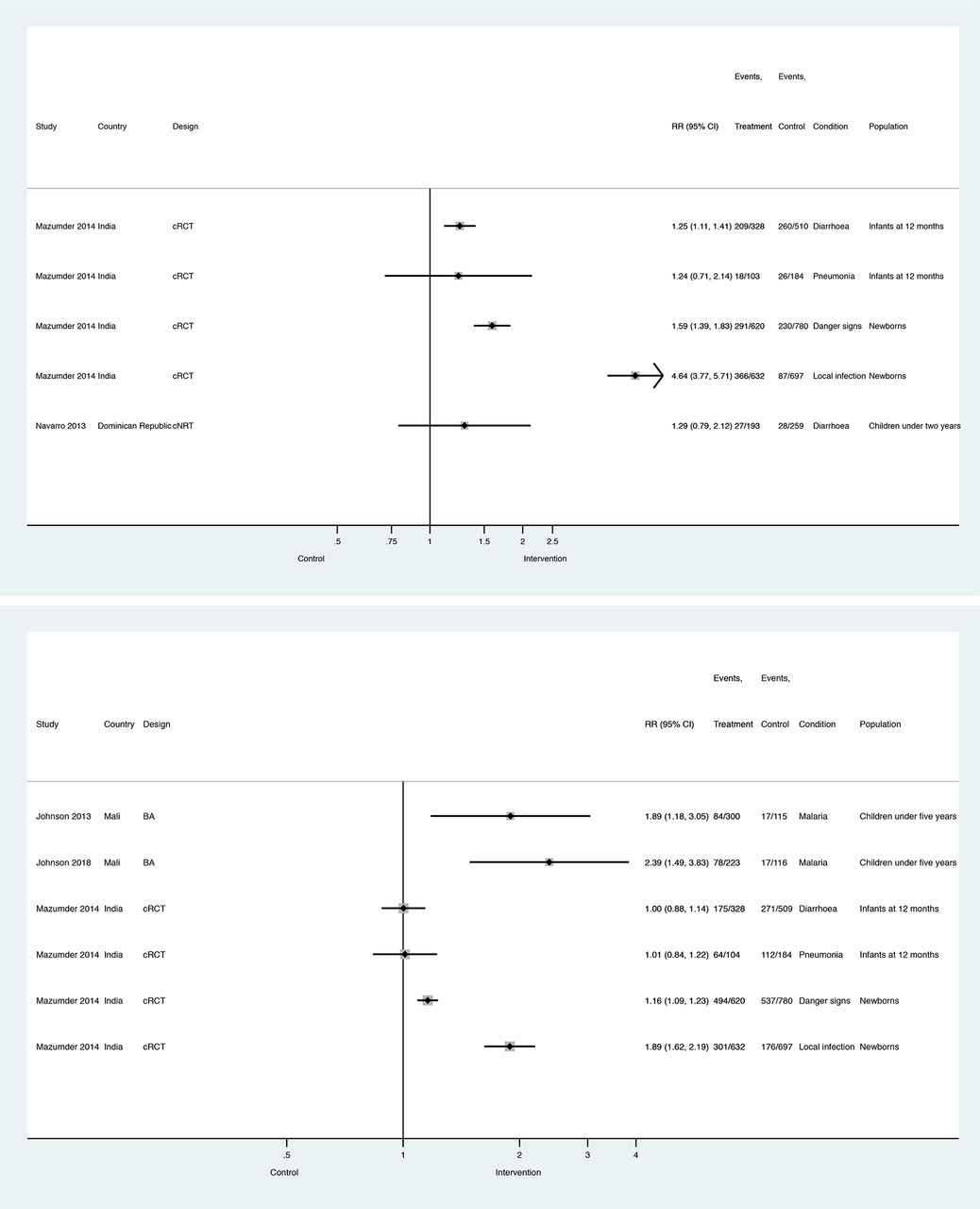
Four studies assessed access to effective and/or prompt treatment (table 3; Figure 3). Proactive case detection may increase access to effective treatment (calculated RRs range from 1.59 to 4.64; I2=97.0%) (low certainty evidence). It is uncertain whether proactive case detection increases access to prompt treatment (calculated RRs range from 1.00 to 2.39; I2=84.9%) because the certainty of this evidence is very low. Three studies assessed the effects of proactive case detection of HIV and/or tuberculosis on access to diagnostic services and/or treatment adherence support; these were excluded from the main analysis and summarised in online supplementary file 4.
Supplemental material
{kind=link}
{kind=link}
{kind=link}
Forest plots for access to effective treatment (top) and prompt access to treatment (bottom). RR, risk ratio.
In Dominican Republic,52 proactive home visits increased the proportion of diarrhoeal children who received oral rehydration solution (AOR=3.86; 95% CIs: 1.14 to 13.02). In Haryana,48 caregivers in intervention clusters were more likely to seek any treatment within 24 hours and treatment from an appropriate provider for newborns with danger signs (respectively, ARR=1.14; 95% CIs: 1.10 to 1.18 and ARR=1.76; 95% CIs: 1.36 to 2.24) and local infections (respectively, ARR=1.97; 95% CIs: 1.71 to 2.27 and ARR=4.86; 95% CIs: 3.80 to 6.21). Caregivers were no more likely to seek any treatment within 24 hours for infants with diarrhoea (ARR=0.99; 95% CIs: 0.89 to 1.10) or pneumonia (ARR=1.10; 95% CIs: 0.96 to 1.25), but more likely to seek treatment from an appropriate provider for diarrhoea (ARR=1.22; 95% CIs: 1.06 to 1.42) or pneumonia (ARR=1.44; 95% CIs: 1.00 to 2.08). In Mali,42 43 a higher proportion of children with fever received antimalarial treatment within 24 hours of symptom onset compared with baseline (AOR=3.20; 95% CIs: 1.75 to 5.85).
Discussion
Summary and quality of evidence
This review identified 14 studies of 11 different interventions involving proactive case detection of common childhood conditions by CHWs in nine LMICs. Findings are summarized in table 4. Proactive case detection may reduce infant mortality and increase access to effective treatment compared with conventional community-based healthcare delivery (low certainty evidence). Although our review suggests that proactive case detection may also reduce mortality among children under 5 years, prevalence of infectious diseases, hospitalisation and improve access to prompt treatment, it is uncertain because the certainty of this evidence is very low. Proactive case detection may reduce neonatal mortality and improve nutritional outcomes (low certainty evidence), although effects vary and it is possible that it makes little or no difference to these outcomes.
Summary of findings for the main analysis
Three high-quality studies from India46–48 provide evidence that proactive case detection of illnesses among newborns and infants reduced neonatal and infant mortality, morbidity, and improve treatment seeking, compared with a conventional community-based approach. Two moderate quality studies in Senegal45 and Bangladesh49 found that proactive case detection and doorstep treatment significantly reduced population-level morbidity, as measured by the prevalence of malarial fever and hospitalisation for diarrhoea, respectively. In these five studies, control groups received passive case detection and management from community-based CHWs and primary health facilities. This provides a more direct assessment of the effectiveness of proactive case detection than studies that had no CHWs in control clusters (which are likely to overestimate its effects) as well as studies with control CHWs who conduct home visits for other purposes (which are likely to underestimate its effects). Activities in control clusters may partially explain the null effects on neonatal mortality and infant morbidity found in the periurban South Africa cluster RCT.39 Home visits by control CHWs for the purpose of procuring identity documents and social grants may have served in practice to proactively identify sick children and encourage caregivers to seek care.
Our review extracted all study outcomes that met our inclusion criteria, even if those outcomes were the result of exploratory or posthoc analyses. This may account for some of the null effects in studies that reported numerous outcomes for which the study was not powered or for which the intervention had no clear pathway for impact. For example, finding no effect on prevalence of diarrhoea for visits targeting nutrition,52 and no effect on stunting for visits to detect disease in infants were the results of exploratory analyses and small sample sizes.47
Although this review found large inconsistencies in results for hospitalisation, the two studies in which CHWs provided doorstep treatment found a significant reduction,47 49 whereas the two urban studies39 52 in which all cases were referred found an increase (although statistically not significant), as might be expected. These were the only studies included in the main analyses in which CHWs did not offer doorstep treatment following proactive detection of uncomplicated cases. In the studies concerning HIV and/or tuberculosis, CHWs referred cases detected and then conducted follow-up home visits for treatment adherence support.
Most studies evaluated complex interventions with multiple components, limiting our ability to draw conclusions about the isolated effects of proactive case detection. At a minimum, all studies likely included—whether or not explicit in the intervention description—health promotion and education messaging by CHWs at the time of home visitation, the benefits of which on child health have been documented.55–57 Other cointerventions included additional support to proactive CHWs in the form of supervision and/or remuneration; systems strengthening such as facility-level improvements and/or user fee removal; community mobilisation and/or women’s groups. Studies that found the intervention effective, such as those in India, Senegal, Bangladesh and Mali, offered more in terms of supportive cointerventions, suggesting these are important design features of successful CHW programmes.
Overall, the quality of studies evaluating proactive case detection was poor. Our review identified only three cluster RCTs that evaluated mortality, morbidity or access to treatment; two of which were the same trial reporting different outcomes.47 48 Our results show clear design effect, with studies at higher risk of bias showing a larger magnitude of effect than the RCTs (tables 2 and 3; Figures 1 and 2). Risk of bias was higher still where inappropriate analytical methods were employed for the study design.50 51 Additionally, studies published before the year 2000 did not account for clustering in their analytical approaches.46 49–51
Limitations
Our synthesis of evidence was limited by the small number of eligible studies, and the considerable diversity between them. With only 11 studies included in the main analyses, we were unable to conduct subgroup analyses that would have tested for differences in effectiveness by features in study and intervention design, including setting, CHW characteristics, target populations, diseases detected or frequency of home visits. We could not explore how different health conditions in different transmission settings or health system contexts would have differential impacts on outcomes. We were also unable to assess publication bias due to the limited number of studies. However, our review included large trials reporting statistically non-significant results, so there are no specific reasons for suspecting a high risk of publication bias.
Our synthesis was further limited by inadequate reporting of methods and results in some studies. We had to make some assumptions in order to calculate a principal summary measure for between study comparisons, such as approximating the denominator or postulating the ICC. Features of CHW intervention design and implementation, including CHW recruitment and training, support and supervision and health system integration, were inadequately described. Comparisons were also inadequately described, making it difficult to understand the differences between the two groups. In some cases, it was not clear whether the control included CHWs at all,44 what services were offered by control CHWs, including whether they conducted home visits for other purposes,40 41 49 or whether they received the additional support, such as supervision or payment, offered to intervention CHWs.45
As there is no universally adopted terminology or strong indexation in health databases for the concept of proactive case detection, it is possible that some published or unpublished evaluations meeting the inclusion criteria were not identified through the search. There is a large body of evidence for the mortality, morbidity and access to care impacts of comprehensive community-based primary healthcare interventions,58 59 including household and community integrated management of childhood illness60–62 that may include home visits by community-based providers for the purpose of health promotion and education, vital registration and/or proactive case detection. Some of these studies56 57 63 may not have been included because insufficient information was available about the role of home visits in disease detection, study designs did not permit comparisons based on workflow and/or study designs were not sufficiently rigorous.
Implications for research and practice
The review process to inform the WHO guidelines for optimising CHW programmes found a scarcity of evidence for several areas reviewed, including recruitment and training, supervision and management, and health system integration.29 64 Our review synthesising evidence around CHW workflow yielded similar conclusions regarding inadequate reporting of programme characteristics and lack of robust evidence. These features merit further consideration by programme architects and evaluators.
Standardising impact metrics for evaluating CHW programmes would greatly facilitate the synthesis of evidence in this field. Possible impact metrics include mortality among vulnerable groups, morbidity, as measured by disease prevalence, and access to prompt, effective treatment. Researchers should also consider process outcomes that provide an understanding of why and how a complex intervention did or did not work. None of the studies identified through the search provided a comparative costing analysis, or reported adverse effects of the intervention to patients, providers or the health system. These are important data points for practitioners and policymakers designing, implementing and scaling-up CHW interventions.
Finally, given that neonatal mortality is becoming an increasingly large proportion of mortality among children under 5 years of age, currently accounting for 45% of under-5 deaths,65 a systematic review dedicated to appraising the evidence of the effects of proactive case detection of neonatal conditions by CHWs in LMICs is merited.
Conclusions
Proactive case detection by CHWs may reduce child mortality and morbidity and increase access to care. The certainty of this evidence is low due to limitations in study designs, inconsistency in results, indirect measures of effect and important diversity between a small number of included studies. More research is needed on proactive case detection with rigorous study designs, standardised outcomes and measurement, and detail on intervention design and implementation.
Acknowledgments
We are grateful to the London School of Hygiene and Tropical Medicine librarians for their tips on devising and executing the search strategy.
References
Footnotes
Handling editor Seye Abimbola
Contributors CW designed the study and wrote the protocol with input from JT, JG, BG, DC, KK and ADJ. CW developed and conducted the database searches. CW, JT and JG screened references for eligibility. CW and EW extracted data from included studies and conducted risk of bias assessments. CW analysed and synthesised data, with input from CL, KK, BG and DC. CW, JT and JG conducted GRADE quality assessments for all outcomes. CW drafted the manuscript. JT, JG, CL, BG and DC provided critical intellectual feedback and assisted in revising the manuscript. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer The findings and conclusions presented in this report are those of the authors and do not necessarily reflect the official position of the CDC.
Competing interests CW, KK and ADJ are coauthors on one (CW and KK) or two (ADJ) of the studies included in the review.
Patient and public involvement statement No patient or members of the public were involved in this study.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available.