Article Text

Abstract
Introduction Disparities in tuberculosis (TB) rates exist between Indigenous and non-Indigenous populations in many countries, including Australia. The social determinants of health are central to health inequities including disparities in TB rates. There are limitations in the dominant biomedical and epidemiological approaches to representing, understanding and addressing the unequal burden of TB for Indigenous peoples represented in the literature. This paper applies a social determinants of health approach and examines the structural, programmatic and historical causes of inequities for TB in Indigenous Australia.
Methods Aboriginal Australians’ families in northern New South Wales who are affected by TB initiated this investigation. A systematic search of published literature was conducted using PubMed, PsycINFO, Scopus and Informit ATSIhealth databases, the Australian Indigenous Health, InfoNet and Google. Ninety-five records published between 1885 and 2019 were categorised and graphed over time, inductively coded and thematically analysed.
Results Indigenous Australians’ voices are scarce in the TB literature and absent in the development of TB policies and programmes. Epidemiological reports are descriptive and technical and avoid analysis of social processes involved in the perpetuation of TB. For Indigenous Australians, TB is more than a biomedical diagnosis and treatment; it is a consequence of European invasion and a contributor to dispossession and the ongoing fight for justice. The introduction and spread of TB has resulted in the stealing of lives, family, community and cultures for Indigenous Australians. Racist policies and practices predominate in the experiences of individuals and families as consequences of, and resulting in, ongoing structural and systematic exclusion.
Conclusion Development of TB policies and programmes requires reconfiguration. Space must be given for Indigenous Australians to lead, be partners and to have ownership of decisions about how to eliminate TB. Shared knowledge between Indigenous Australians, policy makers and service managers of the social practices and structures that generate TB disparity for Indigenous Australians is essential.
A social determinant of health approach will shift the focus to the social structures that cause TB. Collaboration with Indigenous partners in research is critical, and use of methods that amplify Indigenous peoples' voices and reconfigure power relations in favour of Indigenous Australians in the process is required.
- tuberculosis
- public health
- systematic review
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Disparities exist in tuberculosis (TB) rates between Indigenous and non-Indigenous populations in many countries, including Australia.
The social determinants of health have a profound influence on TB incidence.
What are the new findings?
Indigenous Australians’ voices are scarce in the TB literature and absent in the development of TB policies and programmes.
Australia’s Eurocentric social and health systems have influenced, and continue to impact, TB experiences for Indigenous Australians and have contributed to the unequal TB burden.
What do the new findings imply?
A reconfiguration in the relations of power of governing Indigenous Australians’ affairs is required to improve the TB experiences for Indigenous Australians.
Addressing the sociocultural issues influencing TB must include the integration of Indigenous Australians as leaders, partners and collaborators in TB research, policy development and service provision.
Introduction
Tuberculosis (TB) is the leading cause of infectious disease deaths globally.1 However, the burden of TB is not homogenous across populations. Disparities in TB rates exist between countries and within counties. Differences in TB rates also exist between Indigenous and non-Indigenous populations.2 Many historical, structural and programmatic drivers perpetuate inequities in TB rates for Indigenous peoples. The 2008 Global Indigenous STOP-TB Expert Meeting proposed an Indigenous Strategic Framework and Action Plan with action driven by Indigenous peoples, respect for Indigenous worldviews and prioritising cultural perspectives.3
The social determinants of health are the circumstances in which people are born, grow, live, work and grow old, as well as inequities in power and resources, and these are central to health inequities for Indigenous peoples.4 Social processes are underpinned by history, culture and government policy,5 all of which have a profound influence on TB incidence.6–11 Indigenous-specific social inequities contribute to TB and impede the human rights of Indigenous peoples to be free from TB.12 We highlight the need to address the social determinants of health, including the relations and practices between individuals, groups, organisations, institutions and governance bodies. A social determinant of health approach enables investigation of the ‘causes of the causes’, or the structures of social practice, responsible for the unequal burden of TB in Indigenous populations.
Australia has achieved one of the lowest rates of TB incidence in the world with a notification rate of 5.3/100 000 in 2015.13 This positions Australia as a nation to eliminate TB in the coming decades.14 The majority of TB cases are in people born outside Australia, with migration from high-TB incidence countries flagged as Australia’s most significant TB control challenge.13 However, deeply entrenched TB incidence disparities continue to exist between Indigenous Australians (Aboriginal and Torres Strait Islander Peoples) and the non-Indigenous Australian-born population. The number of notified cases and rates of TB in Australia from 2005 to 2014, by population subgroup, is shown in figure 1. TB in the Australian-born non-Indigenous population is very low (0.8 per 100 000 in 2015),13 and clustered cases are rare.15 In 2015, TB incidence in Indigenous Australians (4.8/100 000), who represent only 3% of the Australian population, was six times higher than the notification rate for the non-Indigenous Australian-born population.13 This disparity exists in the context of Australia being a high-income country with universal healthcare, free TB treatment and social insurance schemes. TB in Indigenous Australians must be redressed to achieve the elimination goal for all Australians.
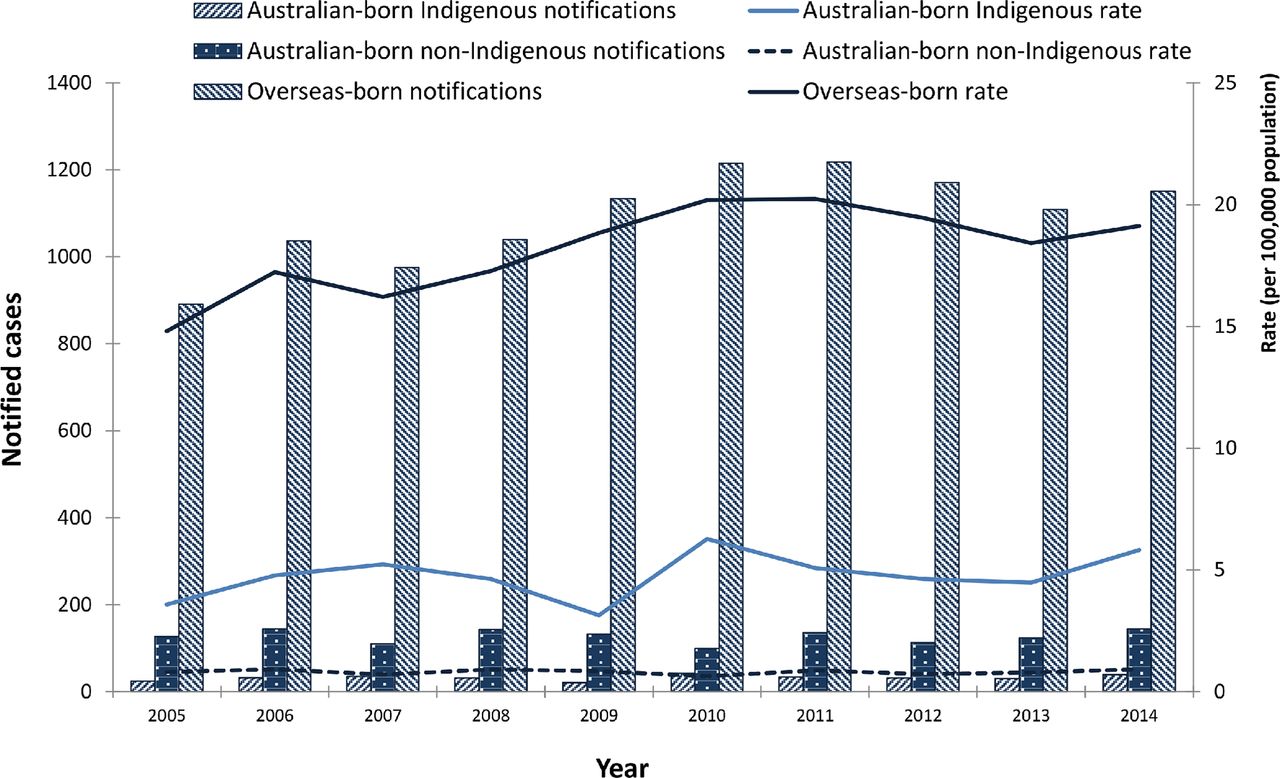
Notified cases and rates of tuberculosis, by population subgroup, Australia, 2005-2014 (adapted fromToms et al, pE25187).
Indigenous Australians are prioritised in Australia’s Strategic Plan towards the elimination of TB,13 but ongoing TB transmission in specific families and social groups continues despite the implementation of clinical and public health actions.16–25 Current TB control activities exist within the context of the Australian Government’s ‘Close the Gap’ Indigenous Health Campaign that aims to close the health and life expectancy gap between Indigenous Australians and non-Indigenous Australians within a generation.26 Despite highlighting socioeconomic indicators, Close the Gap is criticised for its individualistic focus; for defining Indigenous Australians by their limitations, disadvantage or deviance; and for not addressing the structural power imbalances that impact the health of Indigenous Australians.27–29
Understanding of social, cultural and historical experiences of TB with Indigenous Australians is essential to inform different directions and strategies. In this study, we investigate TB experiences for Indigenous Australians beyond the predominant discourse of burden and risk by identifying what has been documented about TB and Indigenous Australians whose perspectives are evident; and look to the causes of the causes in the disparities in TB between Indigenous Australians and the non-Indigenous Australian-born population.
Methods
Research questions and aims
Aboriginal Australians’ families in northern NSW who have been affected by the ongoing transmission of TB since 200023 requested that our Participatory Action Research (PAR) collaborative investigate the published literature with the following broad questions:
What is the history of TB for Indigenous Australians in other parts of Australia, and what is the impact of this history today?
How do other Indigenous Australian individuals and families experience TB?
How has TB control been approached with other Indigenous Australians?
The review aimed to develop an understanding of social patterns and social meanings of TB for Indigenous Australians and to consider how these understandings can contribute to reducing the disparities in TB incidence faced by Indigenous Australians.30 31
Review methodology
An integrative literature review methodology was used. This methodological approach allowed for the inclusion of diverse methods and data from the empirical and theoretical literature32 33 and enabled the integration of Indigenous and Western knowledge systems and worldviews, a space referred to as the ‘cultural interface’.34
Search strategy
A systematic review of literature in English, including Indigenous Australians and TB, was performed in July 2018. An electronic search of online databases including PubMed, PsycINFO, Scopus and Informit ATSIhealth, was undertaken to increase access to diverse health, public health and social sciences literature. Llt.search (www.lowitja.org.au), evidence-based search functions developed by The Lowitja Institute and Flinders University,35 was used for retrieving literature about Indigenous Australians. The PubMed search strategy is shown online supplementary appendix 1. There were no limits applied to any of the searches. The TB collection in the Australian Indigenous HealthInfoNet bibliography and the first 100 websites in Google were searched to increase access to relevant grey literature.36 We scrutinised reference lists for articles missed by electronic searching.
Supplemental material
Eligibility criteria
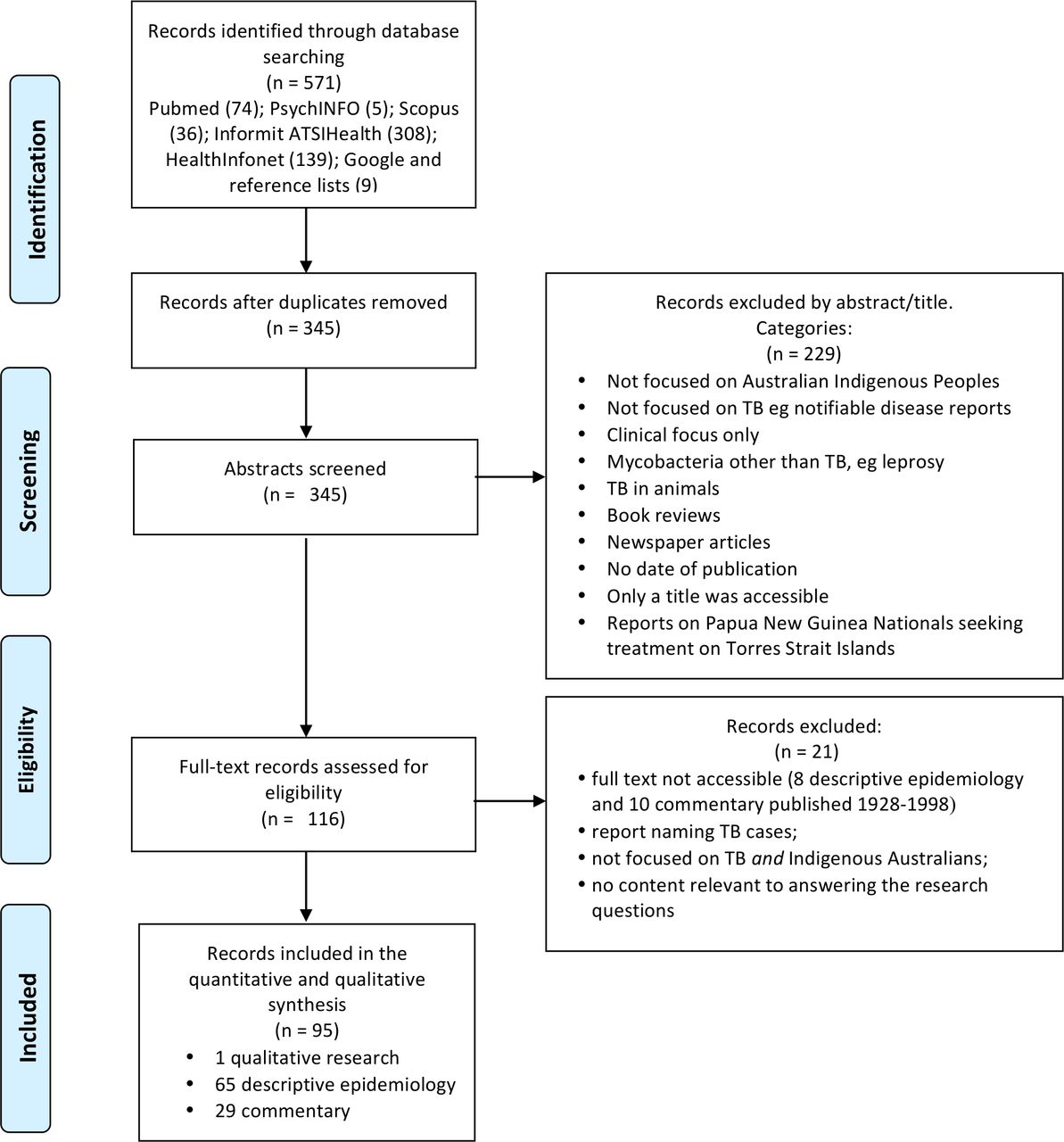
Literature eligible for inclusion in the review included a focus on Australian Indigenous peoples and a focus on Mycobacteriumtuberculosis. Literature excluded by title and abstract included notifiable disease reports; literature that focused on other mycobacteria such as leprosy; reports with a clinical focus only, such as autopsy reports; reports on Papua New Guinea Nationals seeking treatment on the Torres Strait Islands; newspaper articles; book reviews; and a report without a date of publication. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement37 guided the search. The PRISMA flow diagram is shown in figure 2.
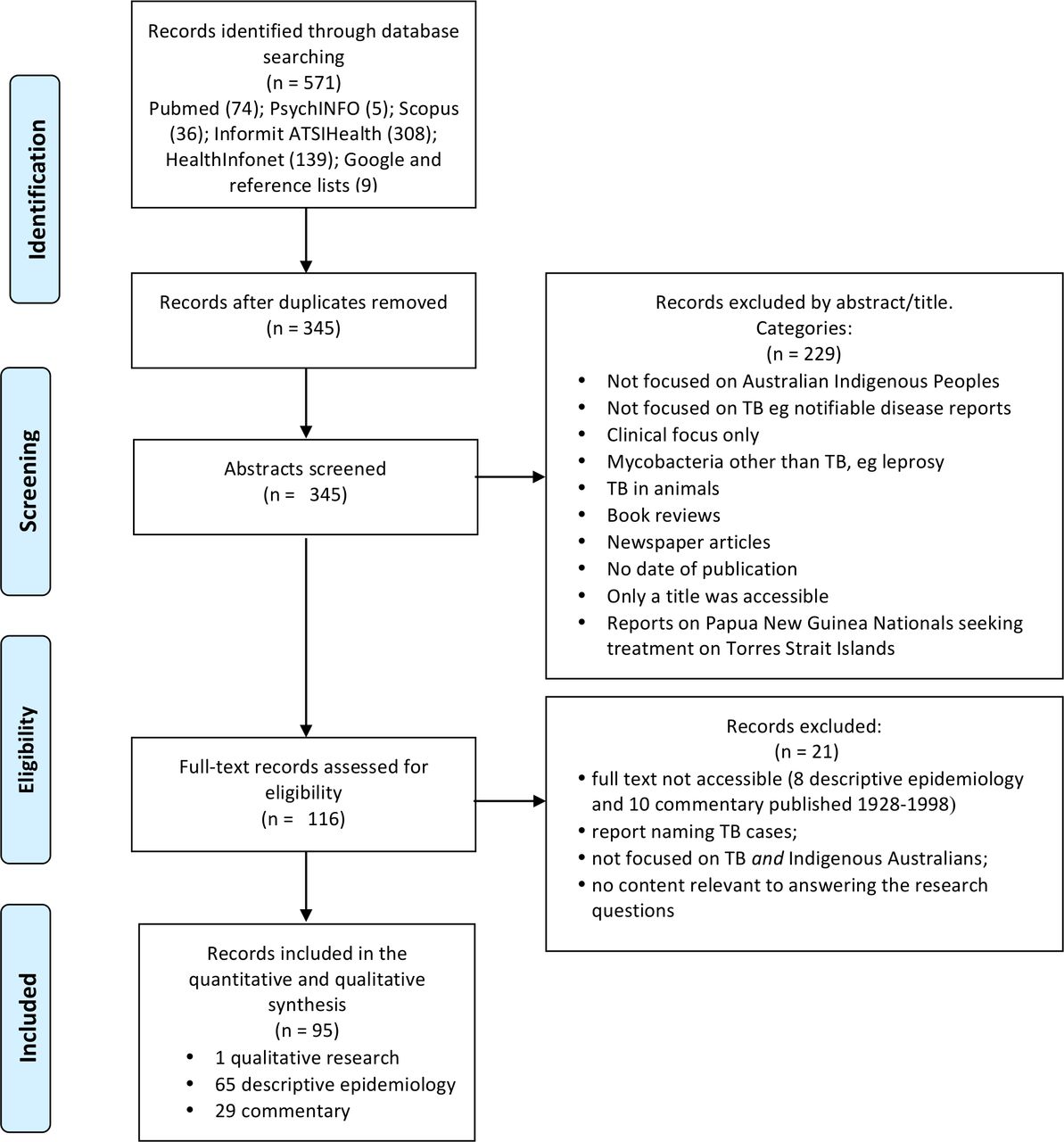
PreferredReporting Items for Systematic Reviews and Meta-Analyses 2009 flow diagram. TB, tuberculosis.
Data collection and analysis
Eligible publications available in full text were extracted and screened (by SD) for content relevant for answering the three research questions. The selected publications were categorised as (1) descriptive epidemiology, (2) qualitative research or (3) commentary describing Indigenous Australians’ TB history, TB experiences and approaches to TB control. The categorisation was based on the primary focus of the text and agreement by SD, JJ and PM. To clarify how the TB experience for Indigenous Australians has been expressed in the literature, we adapted Sanson-Fisher et al’s methodology,38 where the number of texts in each category was graphed in 10-year groupings between 1878 and 2019, shown in figure 3. Considering the types of publications over time assists with understanding what knowledge exists and how this knowledge of TB in Indigenous Australians has developed.

Literature reviewed on TB and Indigenous Australians by publication category, 1879–2018. TB, tuberculosis.
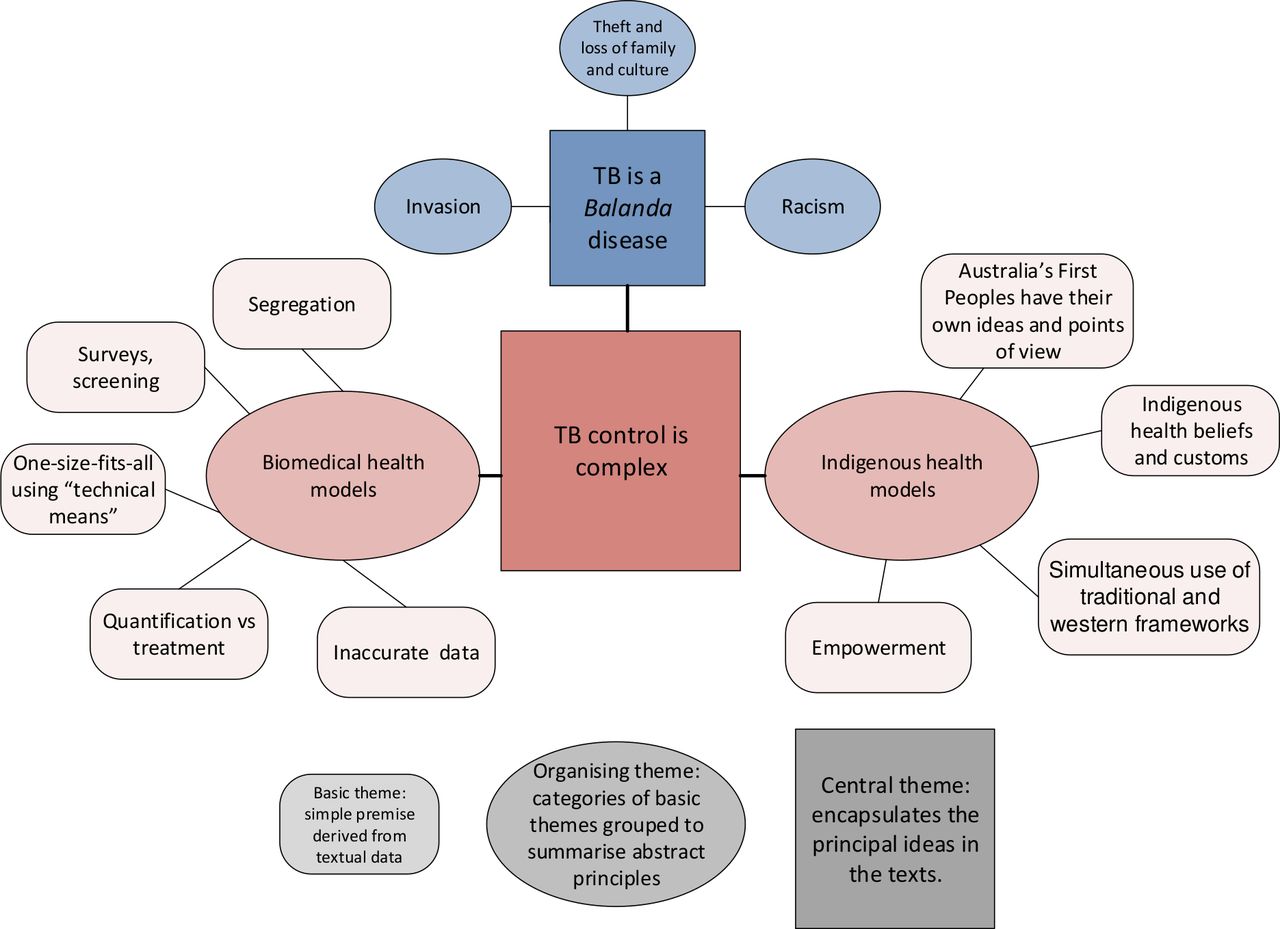
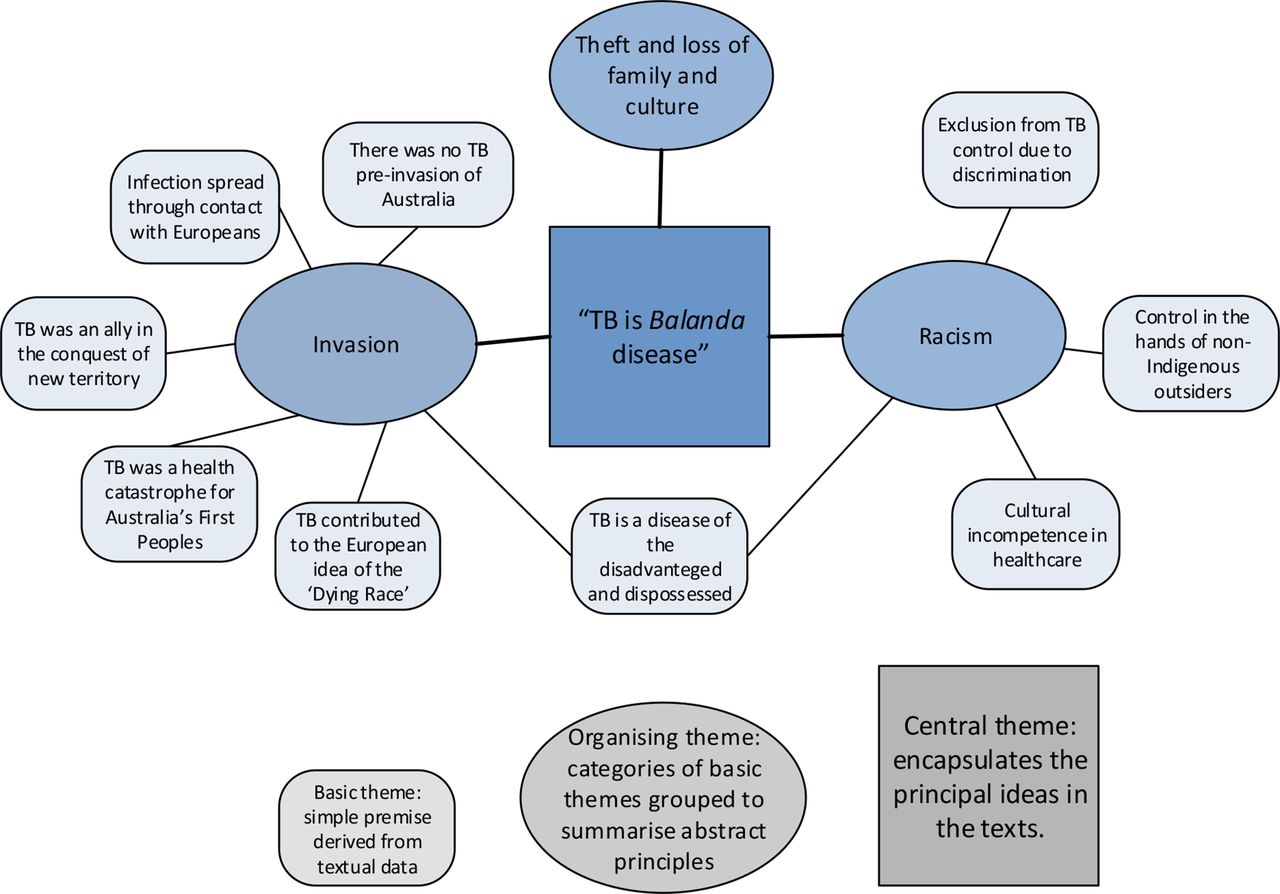
All the full-text publications were synthesised under the three research questions using an adapted thematic analysis method.39 Following inductive coding of each document (by SD, JJ and PM), the extracted data were examined for relationships among themes and how these relationships linked to the overall cultural context (by Indigenous researcher RW and SD). Thematic networks reported by Robinson and Spilsbury (Robinson, p18)39 consisting of basic themes (simple premises derived from the text), organising themes (categories of basic themes grouped together) and global themes (encapsulating the principal idea in the text) were constructed for (1) history of TB and impacts today (2) lived experience and (3) approaches to TB control for Indigenous Australians. Visual constructs of the thematic networks are provided in figures 4–6 to explain the concepts, categories and propositions used to interpret the text.
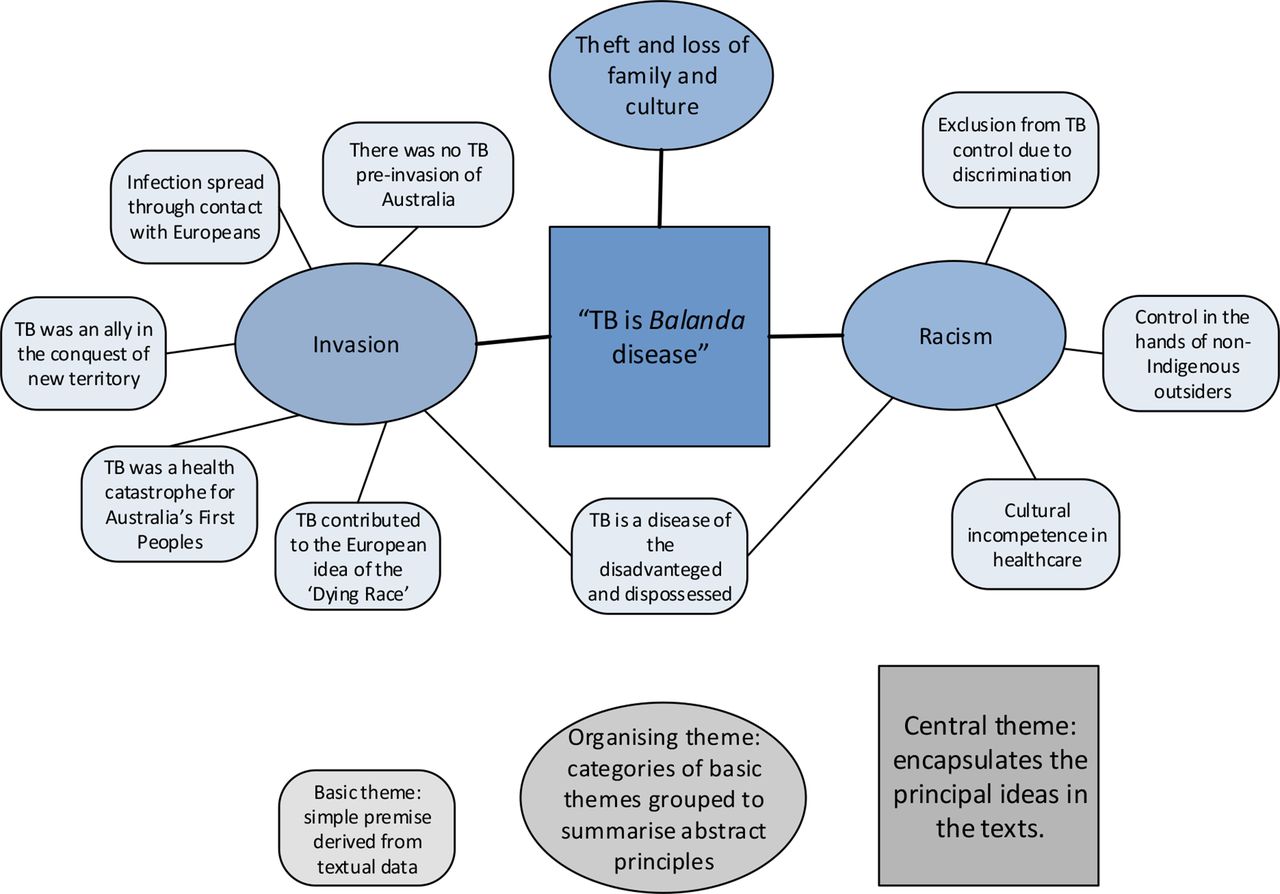
Thematic network 1: the history of TB for Indigenous Australians and how it impacts today. TB, tuberculosis.
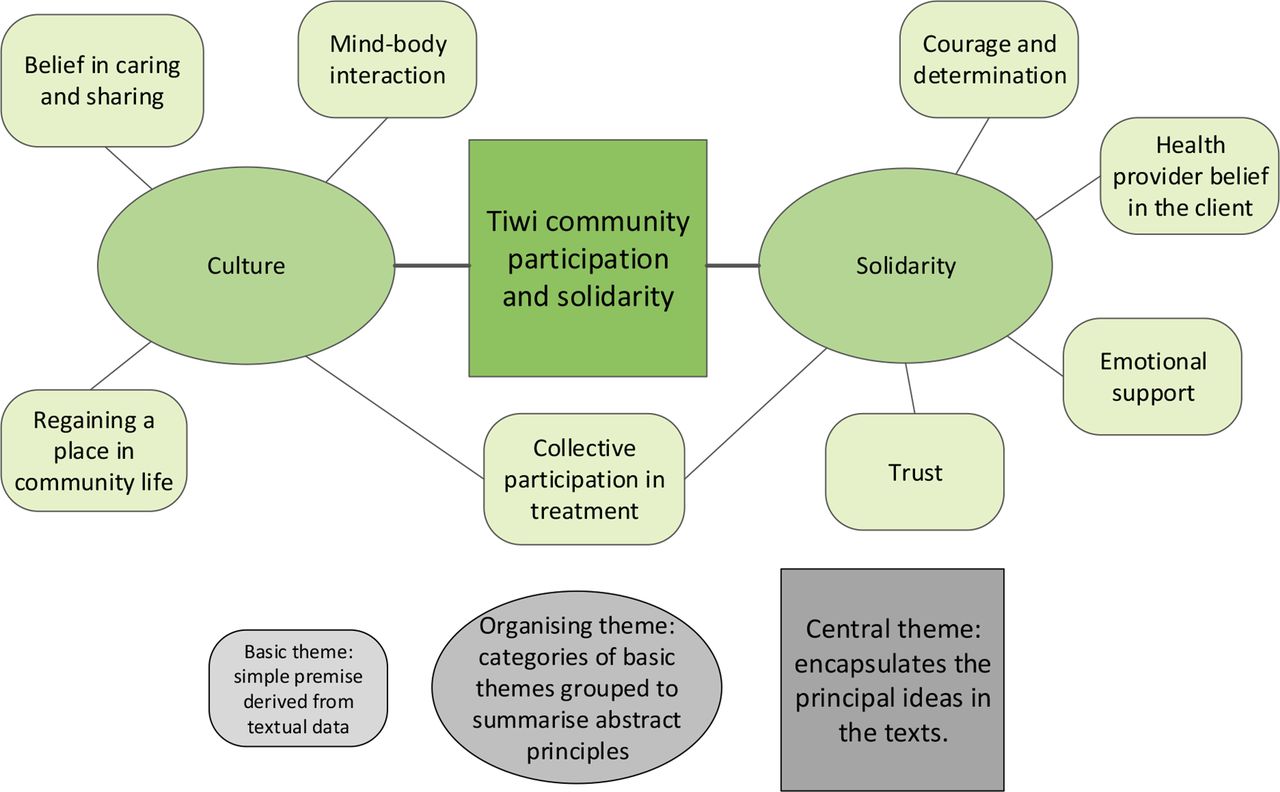
Thematic network: the lived experience of tuberculosis for Indigenous Australians.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Thematic network: approaches to TB control for Indigenous Australians. TB, tuberculosis.
Patient and public involvement
This review is an action within PAR that explores different ways of dealing with TB control with Aboriginal communities in northern NSW, Australia. This PAR aims to connect TB policy and practice with the health beliefs, knowledge and experiences of Aboriginal peoples. This PAR is a collaboration between Aboriginal communities, health services and academics. Aboriginal communities have ownership of the research, and the findings are shared with the respective communities during the plan–act–observe–reflect cycles. The research partners from the health service are positioned to present these findings for consideration in TB policy and programming in Australia. The research findings have influenced NSW TB policy and practice guidelines to be inclusive of Aboriginal peoples as leaders and partners.
Results
Search results
We identified 571 records, with 345 remaining when duplicate records were removed. Two hundred and twenty-nine were excluded after screening abstracts against the inclusion criteria. A further 21 records were excluded as 18 full texts were not available (8 descriptive epidemiologies and 10 commentaries published between 1928 and 1998); one record was not focused on TB and Indigenous Australians; one record did not contain content relevant to answering the research questions; and one report named TB cases. Ninety-five publications were included in the quantitative and qualitative syntheses. The PRISMA flow diagram37 is shown in figure 2.
Study characteristics and distribution
The 95 records were categorised as descriptive epidemiology (n=65), qualitative research (n=1) or commentary on TB history, TB experience and approaches to TB control (n=29). The number of records in each category was graphed in 10-year groupings between 1878 and 2019 (figure 3). Online supplementary appendix 2 summarises the records reviewed by year of publication, geographical focus, a brief description of the content, category for the survey and contribution to organising themes in the qualitative synthesis.
Supplemental material
Only one qualitative research publication was identified.40 The absence of Indigenous Australians’ voices is a crucial gap in the TB literature. Accordingly, this review can only offer understandings of Indigenous Australians’ TB experiences as they are represented in the literature. A limitation of this review is that it will be affected by mainly Eurocentric perspectives, as most of the literature was not authored by Indigenous Australians, and this review is undertaken by mainly non-Indigenous Australians.
The 29 commentary records include seven publications relating to the discriminatory clauses in the TB Act of 1948,41–47 five on Indigenous health,48–52 six commentating on TB in Indigenous Australians,53–58 four on Australian history publications,59–62 three on TB in Australia,63–65 one TB narrative,66 one government newsletter,67 one anthropological description of Indigenous Australians in South Australian region in 188668 and one TB treatment guideline.69 The majority of the commentary describing TB history, TB experience and approaches to TB control was published between 1990 and 2009.
Descriptive epidemiological studies dominate the research literature. Of the 65 descriptive epidemiology reports, 18 are national TB surveillance reports70–87; 12 are State/Territory TB surveillance reports88–99; and four are regional TB reports from far north Queensland100–102 and the Northern Territory (NT).103 The surveillance reports consistently demonstrate the higher TB burden for Indigenous Australians compared with the non-Indigenous Australian-born population. Fifteen records examine TB incidence, outbreaks or TB control with Indigenous Australians in the NT,16–22 24 104 105 northern NSW,23 25 northwest Western Australia106 107 and South Australia.108 One report published in 1975 is a comparison of manifestations of TB comparing Indigenous and non-Indigenous Australians.109
The increased TB burden and risk for Indigenous Australians are also documented in 12 studies that included prisoners,110 111 homeless people,112 people on dialysis,113 people with diabetes,114 school students115 116 and children.117–121 From 2003 to 2012, annual TB notification rates were three times higher in Indigenous children than in non-Indigenous Australian-born children.120 In Queensland, 75% of the Australian-born children diagnosed with TB between 2005 and 2014 were of Aboriginal or Torres Strait Islander descent, even though people of Aboriginal or Torres Strait Islander descent are less than 4% of Queensland’s population.121 The remaining three records include one literature review reporting the burden of TB in Indigenous people globally,2 one Close the Gap report from the NT122 and one health transition analysis from Victoria.123
The pattern of descriptive studies reflects the history of Indigenous statistics: pre-1967 monitoring was for purposes of protection and assimilation of Indigenous Australians, and after the 1967 referendum, when Indigenous Australians were granted the right of citizenship, improved data were expected to improve health and well-being.124 The increase in descriptive epidemiological studies from the 1990s corresponds with the ideological shift to a ‘population health approach’ that is characterised by reliance on data and a preference for quantitative research methods.27 Australia’s National Mycobacteria Surveillance System commenced in 1991, initiating regular national TB surveillance reports.70 The rise in epidemiological studies in 2000–2009 is influenced by nine studies from the NT, the region of Australia with the highest proportion of Indigenous Australians in the population, and with the highest TB notification rate for Indigenous Australians.78 The dominance of epidemiological studies comparing Indigenous and non-Indigenous populations in the last decade corresponds with the focus on statistical equity of the Close the Gap campaign that commenced in 2008.26
Thematic analysis
Theme 1: the history of TB for Indigenous Australians and how it impacts today
The history of TB for Indigenous Australians was described as intertwined with the European invasion of Australia and the subjugation of Indigenous Australians due to racist and protectionist policies.
TB is a Balanda (European) disease and they brought it - we were healthy before the Balanda came – Aboriginal community member Maningrida (Grace and Chenhall, p390).40
TB was positioned as a Balanda or white man’s disease in 30 records.40–68 123 The central theme for the history of TB is ‘TB is a Balanda disease’. A visual depiction of the thematic network is shown in figure 4.
Invasion is an organising theme. Of the 95 records, 20 portrayed TB as an invader.40 42–44 48–55 57–59 61–64 68 TB was described as coming from elsewhere. Before the invasion by Europeans, TB was not a disease experienced by Indigenous Australians.48 49 51 54 58 62 However, 30 or 40 years after the land and water in a district had been seized by Europeans, TB became a significant disease for the Indigenous Australians of that district.62 In colonial Australia, TB was noted as a leading cause of illness and death for Indigenous Australians.48 50 51 54 60 62 68 By the late 1800s, TB had become entrenched in Indigenous Australians and ‘one would hardly see any old people—their remarkable freedom from sickness seemed to disappear’ (Campbell, p134).51 The susceptibility of Indigenous Australians to TB was considered by Europeans to be a consequence of their isolation from world diseases and race-based physiological vulnerability.51 54 61 TB was a major ally in the conquest of new territory and in the demoralisation and destruction of Indigenous Australians.51 59 61 TB was also described as a ‘racial health catastrophe’, (Smith, p135)62 and depopulation from TB contributed to the image of Indigenous Australians as a ‘dying race’, doomed to extinction.51 58 61 Commenting on the disinterest in the health of Indigenous Australians in the influential Medical Journal of Australia before the 1950s, Thomas stated,
Any research on Aboriginal and Torres Strait Islander peoples before the 1960s was…about collecting information about Aboriginal people for science before the race became extinct (Thomas, p521).44
Racism is an organising theme. In 22 of the 95 records, racism was identified in Indigenous Australians’ TB experiences.40–48 50 53 54 57–59 61–66 123 Racism was documented as central to the history of TB history for Indigenous Australians. Racism continues as a dominant social context for TB for Indigenous Australians today. Race-based policies that forced the congregation of Indigenous Australians onto missions and government settlements caused social disruption and adverse environmental conditions which were fertile for TB transmission.50 54 58 Across the literature, the significance of the oppression of Indigenous Australians underpins the past and ongoing social inequities contributing to TB affecting Indigenous Australians.40 41 47 48 50 54 58 62 64 123
Exclusion from TB control due to discrimination was evident across the literature review. In early religious and ethnocentric beliefs of the European invaders, TB was often not recognised in Indigenous Australians because of prevailing racist views on human unity and questions of whether disease could jump species.59 61 There was no clear division between medicine and religious tenets, with Indigenous Australians’ traditional TB treatments opposed on moral grounds by some missionaries.61 At the time, European medicine could not cure TB. The portrayal of TB as afflicting immoral or intemperate people61 63 perpetuated the underlying racist views towards Indigenous Australians.
During the 1948–1976 Australian Tuberculosis Campaign (ATC), Indigenous Australians missed out on medical and financial support. The electoral roll was used to administer the ATC, in the era when Indigenous Australians were neither registered to vote nor counted in the official Australian Census. Also, Indigenous Australians were not considered by bureaucrats as responsible citizens.42 47 The TB financial allowance was denied to Indigenous Australians because of how bureaucrats interpreted the wording in the Tuberculosis Act.47 It was not until the rewording of the Act that benefits were paid,42–45 despite there being no statutory provisions excluding Indigenous Australians eligibility to the TB allowance.46
Cultural incompetence in healthcare negatively affecting Indigenous Australians was apparent throughout the documents. Indifference by non-Indigenous Australians to the impact of TB for Indigenous Australians and the slow or absent government response was also evident.40 47 54 57 58 62 63 65 Until the mid-20th century, TB control in Australia was informed by the White Australia Policy, rather than evidence-based medicine.65 Throughout the literature, it was clear that TB control was managed by non-Indigenous outsiders, first through colonialism then through paternalistic policies.40 47 54 A 2003 anthropological assessment of TB in a remote Northern Territory community documented cultural incompetence at all levels in the health service.40 Interactions with non-Indigenous clinic staff implied ‘a relationship of distrust and poor communication, with residents feeling victimised and powerless’ (Grace and Chenhall, p392).40
Theft and loss of family and cultures is an organising theme caused by the invasion and racism described previously. Seven of the 95 records specifically highlighted theft and loss of family and cultures as a result of TB.51 52 56 60–62 67 The 1881 passing of an Indigenous man from TB was narrated as ‘ending the patrilineal line of guardians of the land’ (Smith, p13)62 The TB Indigenous activist Harry Penrith (known as Burnum Burnum)60 was removed from his mother’s care because she had TB, the implications being
Within the space of three months Harry Penrith suffered a three-fold loss that was to profoundly affect his formative years: the loss of his mother, the loss of his family and the loss of his Aboriginal culture. He thus became part of the 'stolen generation' of the 1930s and 'removed' by the state to become 'a displaced person' with no family, no ancestry, no cultural tradition (Ramsland, p36).60
Theme 2: the lived experience of TB for Indigenous Australians
The lived experience was interpreted as knowledge and understanding from the first-hand experience with TB. Only one first-hand TB story, Florrie’s story,66 was identified in the literature search. Despite the history of invasion, racism and loss, Florrie’s story is strength-based. Florrie, her family and her community possessed resources to respond to manage and eliminate her illness on a day-to-day basis. The central theme for Florrie’s lived experience of TB is ‘Tiwi community participation and solidarity’. A visual depiction of the thematic network is shown in figure 5.
Solidarity is a major organising theme. The story describes the collective participation of Florrie and her family in Florrie’s rehabilitation and recovery. The solidarity of Florrie’s social and healthcare environment involving Indigenous health workers contributed to strengthening her resilience. Florrie emphasises the essential role of emotional support, as well as practical assistance, from her family and her healthcare team. Florrie actively participated in her rehabilitation and trusted her local health service, which reflected the health staffs’ belief in her.
Culture is a major organising theme. Florrie’s Tiwi culture has a ‘strong belief in sharing and caring’, (Puautjimi et al, p7)66 and this is credited for Florrie regaining independence. An Aboriginal health worker stated, ‘The community welcomed Florrie back home and made her yet again one of its important members’ (Puautjimi et al, p7).66
Florrie’s positive experience contrasts with TB experiences from other locations. People from the Lockhart River Mission with TB in the 1950s were sent away from their traditional land to the distant Thursday Island sanatorium. On discharge from the sanitorium, ‘women and children and old people were left to their existence of makeshift’, (Tennant, p6)67 which contributed to the theft and loss of family and cultures outlined in theme 1, TB is a Balanda disease.
Theme 3: approaches to TB control for Indigenous Australians
Because TB manifests as a social disease, TB has been a challenge across many societies for many centuries. There has never been a simple method of control offered by Indigenous or biomedical health models. Therefore, TB control is complex. Of the 95 publications reviewed, 86 described approaches to TB control involving Indigenous Australians.2 16–18 23 25 40 42–44 47–51 53 56–59 61–67 69–123 The central theme for approaches to TB control is ‘TB control is complex’. This thematic network intersects with theme 1, ‘TB is a Balanda disease’. A visual depiction of the thematic network is shown in figure 6.
Indigenous health models is an organising theme. Of the 95 records, 21 described Indigenous health models for the control of TB.2 16–18 23 25 40 43 48–51 53 57 59 61 64 66 69 102 103 Indigenous Australians’ approaches to health and illness, including TB, are recognised as holistic with spiritual, physical and biological causes and therapies, including magic or religious beliefs.50 Indigenous Australians initially adapted traditional health models to treat TB, such as rubbing people with dugong oil.51 59 Later, both traditional and Western medicines were used simultaneously.40 53 61 A study in the NT found Indigenous Australians were more likely to accept antibiotic treatment for latent TB infection than overseas-born and non-Indigenous Australians.103 Indigenous Australians resident in remote Maningrida recommended culturally appropriate clinical services through actively discussing service decisions, improving social relations with clinical staff and the inclusion of Aboriginal health workers in delivery of health services.40
Empowerment is a key social dynamic distinguishing the Indigenous health models from biomedical health models. There are examples where Indigenous people’s transformations through their individual TB experiences influenced the people and systems around them. Florrie’s Story conveys how Florrie and the Aboriginal health workers felt more control over their own lives by participating in her rehabilitation.66 Publication of Florrie’s strength-focused story provided an opportunity for an Indigenous Australian from the Tiwi Islands to voice her experiences. Amendment to the discriminatory clauses in the Tuberculosis Act empowered the Indigenous Australians who lead the campaign and the families who had previously been denied the benefits.43
TB services for Indigenous Australians that are ‘innovative, and tailored towards individual needs’ with ‘full and voluntary community participation and leadership’ are recommended in TB control guidelines (Patel and Streeton, p66).69 Attempts to realise this that are documented in the literature included community engagement; the participation of Aboriginal health workers; TB education developed by Indigenous Australians16–18 23 25 102 and TB services ‘guided by the principles of cultural respect, equity and partnership with Aboriginal communities’ for shared ownership of solutions (Devlin and Passmore, p41).23 The involvement and active participation of Indigenous communities in the organisation and delivery of services link to the community participation and solidarity findings for theme 2.
Biomedical health models is an organising theme. Of the 95 records, 82 described biomedical approaches to control of TB in Indigenous Australians.2 16–25 40 42 44 47–50 56–58 61–63 65–67 69–123 TB services have been controlled by non-Indigenous outsiders and have rarely been designed to meet the needs of Indigenous Australians resulting in the marginalisation of Indigenous Australians from TB programmes. In the 20th-century, sanatoria were used for non-Indigenous Australians but were not universally accessible to Indigenous Australians who were mostly segregated in missions and reserves where disease spread further.61 Although there were TB surveys of Indigenous Australians in the 1940s and 1950s, these primarily resulted in quantification of TB infection, not the delivery of TB treatment.63 104 106–109
In the 1980s, there was an expectation that an improved socioeconomic situation for Indigenous Australians would eventually result in a decline in TB came with a one-size-fits-all approach using ‘technical means’ for TB control in Australia.69 These technical means included case finding, diagnostics, treatment, contact tracing and vaccination. These strategies still endure as TB control today. In the 1990s, directly observed treatment (DOT) became synonymous with TB treatment, which further complicated Indigenous Australians’ interaction with non-Indigenous healthcare providers. Authoritarian implementation of DOT reminds Indigenous Australians of invasion, systemic racism and theft of family and cultures.
As previously discussed, descriptive epidemiological studies have dominated the research literature since the 1990s. Epidemiological reports are descriptive and technical, and avoid analysis of social processes involved in the making and perpetuation of TB.
Discussion
This review reveals that for Indigenous Australians, TB is more than a diagnosis and a treatment; TB is a consequence of, and a contributor to, European invasion, dispossession and the ongoing fight for justice. The introduction and spread of TB have resulted in the stealing of lives, family, community and cultures for Indigenous Australians. Racism is a dominant feature of the TB experiences of Indigenous Australian individuals and families. The health model used for TB treatment and control in Australia is a further expression of the Eurocentric mindset where the one-size-fits-all biomedical health model is privileged. Indigenous health models have been, and continue to be, dismissed. The population health focus comparing Indigenous Australians to the non-Indigenous population has dominated the development of public policy,29 an approach that may generate anxiety to help that may then manifest as authoritarian Eurocentric solutions imposed on Indigenous Australians.27
These realities point to the power differential in Australian society, where the invading European society places itself as superior. A reconfiguration in the relations of power in the governing of Indigenous Australians’ affairs is required to improve the TB experiences for Indigenous Australians. The power reconfiguration must include the integration of Indigenous Australians as leaders, partners and collaborators in TB research, policy development and service provision.
Fundamentally, higher rates of TB among Indigenous Australians is socially determined. However, the social determinants of TB are not just about economic or financial barriers in absolute terms. For Indigenous Australians, the social determinants of TB are linked to deep-rooted social, cultural and historical experiences. The international TB movement with a focus on directly addressing economic conditions that underpin extreme poverty in low-income and medium-income countries is essential in these contexts. However, the relative poverty experienced by Indigenous Australians, in a high-income country with a very high overall human development index,125 needs to be understood in context. The disparity in TB rates for Indigenous Australians has not changed with Australia’s overall economic development. Universal healthcare with free TB treatment has not automatically resolved the fact that TB disproportionally infects and affects Indigenous Australians. A reconfiguration in the relations of power governing Indigenous Australians’ affairs is required to improve Indigenous Australians’ TB experiences. Policy makers and service managers need to recognise the failure of prevailing institutional approaches and instead move to integration of Indigenous Australians as leaders, collaborators and partners in TB research, policy development and service provision.
TB is a complex problem requiring nuanced approaches for elimination, including embracing the strengths of Indigenous health models; enabling the best of the biomedical approaches; and importantly, strength-based approaches that build on community participation and solidarity. Indigenous Australians’ cultures are smart, strong, engaged and connected with the past, present and future. Health models that embrace and celebrate the strengths of cultures to address the complex interactions underlying the social determinants of TB for Indigenous Australians are required.
Indigenous Australians’ voices are scarce in the TB literature and absent in the development of TB policies and programmes. Enabling people affected by TB to have a real say in finding new ways to control TB is not a new idea; it has been undertaken through decolonising research with Aboriginal communities in Canada12 126 and remote Solomon Islands.127 The approach has also been proposed in other TB contexts such as for young people who have a different, but often unrecognised, experience of TB,128 and to understand and address how gender influences TB.129
Addressing the sociocultural issues influencing TB requires research that incorporates narratives and experiences and uses methodologies that contribute to shifting the power balance towards Indigenous Australians. Decolonising research methodologies, such as PAR, are founded on the relocation of power to the community of interest. Our group is undertaking PAR in northern NSW, Australia, to develop a better understanding of TB with Indigenous Australians in this context. Our research is in response to ongoing TB transmission in Indigenous Australian families so that locally appropriate strategies and interventions can help to reduce the burden of TB in this area. The PAR is an example of a beginning for Indigenous Australians to have a real and ongoing say about TB and directly engaging with ‘the causes of the causes’ of TB transmission.
Conclusion
The literature on TB in Indigenous Australians highlights that the inequity in disease rates is a result of the ongoing European invasion; that racism is a significant factor; and that the TB has caused loss of family and culture. The links between TB and Indigenous Australians’ dispossession, disempowerment and cultural effacement since colonisation highlight that TB is inherently a social disease. Complex individual, community and environmental interactions all influence TB transmission and outcomes. The current approach to eliminate TB in Australia comprises one-size-fits-all guidelines that do not reflect the social and historical contexts for many Indigenous Australians. The next step in TB care with Indigenous Australians is to acknowledge that in this complex space, little is understood. New and shared knowledge between Indigenous Australians, policy makers and service managers on the social determinants of TB is required, which reflects local realities and the specific local contexts in which they are played out. To connect TB policy with health beliefs, knowledge and experiences, Indigenous Australians must have a real say in the development of TB policies and programmes and ownership of decisions about how to eliminate TB. Collaboration with Indigenous partners in research is critical, using methods that amplify Indigenous peoples' voices and reconfigure power relations in favour of Indigenous Australians in the process.
Acknowledgments
Our sincere thanks to the Aboriginal Australians engaging in the Participatory Action Research in northern New South Wales, Australia, for sharing their wisdom and knowledge. We thank Kirsty Browne and Paul Corben for their assistance and support with the Participatory Action Research. Our research and this paper were strengthened by the generous feedback of four anonymous reviewers, for which we are thankful.
References
Footnotes
Handling editor Seye Abimbola
Contributors The corresponding author SD attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer The lead author, SD, affirms that the manuscript is an honest, accurate and transparent account of the study being reported, and no important aspects of the study have been omitted.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Approval for the research was granted by the Aboriginal Health and Medical Research Council (1043/14), James Cook University (H6315), and the North Coast Health Service (LNR098) Human Research Ethics Committees.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.