Article Text

Abstract
Introduction Samvedana Plus is a multilevel intervention working with sex workers, their intimate partners (IPs) and communities to reduce intimate partner violence (IPV) and to increase condom use within intimate relationships of sex workers in Northern Karnataka, India.
Methods A cluster randomised controlled trial in 47 villages. Female sex workers with IPs in the last 6 months were eligible for baseline (2014), midline (2016) and endline (2017) surveys. 24 villages were randomised to Samvedana Plus and 23 to a wait-list control. Primary outcomes among sex workers included experience of physical and/or sexual IPV or severe physical/sexual IPV in the last 6 months and consistent condom use with their IP in past 30 days. Analyses adjusted for clustering and baseline cluster-level means of outcomes.
Result Baseline (n=620) imbalance was observed with respect to age (33.9 vs 35.2) and IPV (31.4% vs 45.0%). No differences in physical/sexual IPV (8.1% vs 9.0%), severe physical/sexual IPV (6.9% vs 8.7%) or consistent condom use with IPs (62.5% vs 57.3%) were observed by trial arm at end line (n=547). Samvedana Plus was associated with decreased acceptance of IPV (adjusted OR (AOR)=0.62, 95% CI 0.40 to 0.94, p=0.025), increased awareness of self-protection strategies (AOR=1.73, 95% CI=1.04–2.89, p=0.035) and solidarity of sex workers around issues of IPV (AOR=1.69, 95% CI=1.02–2.82, p=0.042). We observed an increase in IPV between baseline (25.9%) and midline (63.5%) among women in Samvedana Plus villages but lower in comparison villages (41.8%–44.3%) and a sharp decrease at end line in both arms (~8%).
Conclusion We found no evidence that Samvedana Plus reduced IPV or increased condom use, but it may impact acceptance of IPV, increase knowledge of self-protection strategies and increase sex worker solidarity. Inconsistencies in reported IPV undermined the ability of the trial to assess effectiveness.
Trial registration number NCT02807259.
- cluster randomised controlled trial
- sex worker
- intimate partner violence
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Prevalence data suggest that between 22% and 27% of female sex workers in Karnataka have experienced sexual or physical violence from an intimate partner in the past year, and condom use within their intimate partnerships is low.
To date, there have been no trials evaluating interventions to reduce IPV among sex workers.
What are the new findings?
We report no effect of the intervention on experience of sexual and/or physical IPV or condom use in this setting.
We report decreased acceptance of IPV, increased knowledge of self-protection strategies and a small effect on greater solidarity around IPV among sex workers.
We note methodological difficulties relating to measuring IPV and tensions between maintaining the strict conditions of a trial in the context of evaluating an intervention for a highly marginalised population living in extreme poverty.
What do the new findings imply?
Strategies to reduce acceptance of violence at macrostructural and community levels are needed to create an enabling environment in which targeted IPV interventions can be implemented to address heightened stigma and violence experienced by devadasi sex workers.
Further research is needed to develop appropriate ways of measuring IPV among this population and working with communities to develop a study design that they can support while still maintaining their ability to provide essential services.
Introduction
Intimate partner violence (IPV) is one of the most serious public health challenges for women in the 21st century. In the last decade, 30% of women aged 15 years and over have experienced physical and/or sexual violence from an intimate partner (IP) during their lifetime.1 Sex workers in low-income, middle-income and high-income settings experience far higher levels of IPV than other women. Evidence from India and Mexico suggests that between 21% and 35% of sex workers have experienced IPV (sexual or physical) in the last 6 months,2 ,3 and 44% of sex workers in Mombasa, Kenya, have experienced sexual violence from IPs in the past 30 days.4 In the UK, USA and Canada, between 14% and 22% of female sex workers working in on-street and off-street settings had experienced sexual and/or physical IPV in the past 6–12 months.5–7 Evidence suggests that sex workers experience higher levels of violence from their IPs than from their clients, and both are equally important in shaping HIV risk.8 For example, in India, while 21%–27% of female sex workers have experienced recent IPV, only 11%–22% have experienced client violence in the same time frame.2 9 Much of the research documenting violence and its determinants among sex workers has focused on clients and not IPs, neglecting a substantial part of the problem.10 IPV among women has multiple adverse health effects, including physical health conditions, unwanted pregnancies, gynaecological complications, depression, post-traumatic stress disorder and increased risk of HIV infection.11–13
Higher rates of participation in sex work in India is associated with belonging to a lower caste, poverty and gender inequality. In some northern parts of Karnataka, sex work is also linked to the ‘devadasi’ system, in which families from the lowest or ‘scheduled’ caste ‘dedicate’ young girls to engage in sex work as part of a religious tradition.14 Although the devadasi system was made illegal in 1988, more than 90% of female sex workers in the Bagalkote district of northern Karnataka come from devadasi families.14 The issue of violence against sex workers in Karnataka, South India, first emerged in the context of large-scale, HIV-related programming with sex workers as part of the Gates-funded ‘Avahan’ programme, which began to address the risks sex workers faced in terms of violence by clients and the police. The ‘Samvedana’ intervention is built on the Avahan programme to focus on violence towards sex workers from all actors (community and police). While Avahan focused on sensitising police, media and policy makers on issues related to sex work and violence, Samvedana focused on strengthening crisis management centres to address incidences of violence among sex workers across 15 districts in Karnataka. During the implementation of Samvedana, the prominence of IPV became clear. Among devadasi sex workers in these districts, 62% reported having long-term relationships with IPs, in addition to having clients. These intimate relationships are modelled on traditional marriages, often involve children and bring some level of social status and financial support for devadasi women, who by tradition are not allowed to marry.14 Data indicated that condom use in these private relationships was low (25.5%), and lifetime experience of IPV was high (60%).15 16 Participatory research conducted with sex workers and their IPs in Karnataka revealed that violence in relationships was widely accepted and that unprotected sex was interpreted as a sign of fidelity.17
The effectiveness of interventions to reduce IPV among sex workers is not well characterised, particularly in low-income and middle-income settings.18 There is some evidence from trials conducted in Mongolia and Kenya where IPV was a secondary outcome but not the focus of the intervention. One trial showed some effect of a brief alcohol intervention on reducing client violence but not IPV at 6 months. The authors attribute this differential outcome to the more complex relationships that sex workers have with their non-paying partners, which make them harder to change.19 The second used motivational interviewing to reduce client violence in the context of an HIV/sexually transmitted infection (STI) intervention. This trial demonstrated an effect on overall risk of violence (client and IPV combined), but there were too few cases of IPV to measure an effect on IPV alone.20 There is also some evidence showing the effectiveness of behavioural and community-based interventions in increasing condom use with clients,21 22 but another trial suggested no effect of individual counselling and peer education on condom use with all partners.23
Although the links between violence and HIV/STI transmission and the need to include IPs in research and programmes are recognised, most violence prevention interventions for sex workers have not focused on IPV.24 25 We sought to address this gap through the design of Samvedana Plus. Building on learning from Avahan and Samvedana, Samvedana Plus was designed to reduce IPV and HIV risk among sex workers and their partners by empowering sex workers. New elements included the introduction of a group-based curriculum addressing IPV and gender inequalities, as well as working with IPs around violence and masculinity norms, improving communications through couple counselling and creating an enabling environment at the village level by challenging current gender norms. The objective of this trial was to ascertain whether Samvedana Plus was effective in preventing IPV and increasing condom use.
Methods
This two-arm cluster randomised controlled trial (cRCT) with wait-list control was conducted in 47 villages in Bagalkote district of Karnataka state, south India. Data collection involved three serial cross-sectional surveys among sex workers aged 18 years or older with a current or recent IP (last 6 months). We defined villages or clusters eligible for participation in the study as (1) where there were sex workers who have one or more IP or who frequently change their IPs, or (2) whose IP has more than one sexual partner. This was in line with the approach taken by the intervention to focus activities. The full trial protocol has been published26 and available online (Clinical Trials NCT02807259.)
Samvedana Plus
The overall aim of Samvedana Plus was to reduce violence and to increase consistent condom use within intimate relationships of sex workers. A theory of change hypothesising pathways of effect for the intervention was developed based on insights from programming to reduce domestic violence among the general population (online supplementary appendix 1).27 In brief, the programme, informed by prior participatory research,17 worked with individuals, couples and at a community level to change the acceptability of IPV as a form of discipline, to challenge assumptions that give men authority over women and to encourage new relationship models based on equality and respect. The intervention, implemented between April 2015 and September 2017, lasted 27 months (table 1). It was led by a local community-based organisation (CBO) sex worker collective, Chaitanya AIDS Tadegattuva Mahila Sangha in collaboration with the Karnataka Health Promotion Trust (KHPT). The CBO was responsible for identifying sex workers and IPs to take part in the intervention; with support from KHPT, they trained outreach workers to facilitate 12 reflection sessions and to provide counselling, training male champions and building alliances with other networks to address violence against sex workers. Peer educators (from the same sex work community) provided ongoing HIV-related counselling throughout the study area independent of Samvedana Plus, but coordinated and trained by the CBO. The CBO did not implement the research but facilitated access to participants for the research team. Villages in the control arm continued to receive standard HIV programming (including condom distribution and HIV prevention information via peer educators) and at month 24 began to receive the intervention.
Supplemental material
Samvedana Plus
Randomisation
Following a mapping and enumeration exercise, 92 villages and 5 towns were identified in Bagalkote with resident sex workers. A total of 27 villages and all 5 towns across the district were excluded since an intensive IPV intervention pilot of Samvedana Plus had been conducted in 2011,27 and a further 18 villages were excluded due to insufficient numbers of sex workers with IPs (<10). The enumeration exercise suggested there were 800 sex workers with an IP in 47 villages. These villages were included in the study and participated in baseline and endline surveys (figure 1). Forty-seven villages were randomly allocated (1:1) to the intervention or control group using a computer-generated sequence in Stata version 15. (StataCorp LP, College Station, TX, USA) using two village-level stratification factors: village population size (<2638, 2639–4604 and >4604) and the number of sex workers with IPs (above 12 or 12 and below). Twenty-four villages were allocated to the intervention arm and 23 to the wait-list control arm. Due to the nature of the intervention, CBO staff, sex workers and individuals delivering the intervention could not be masked to group allocation. A monitoring and evaluation officer was appointed (external to KHPT) to ensure that the protocol was being adhered to and to visit villages to monitor the delivery of Samvedana Plus and the control.

Trial profile. FSW, female sex worker; IPV, intimate partner violence; pop, population.
Recruitment and ethics
The CBO created and regularly updated a list of sex workers and their IPs in order to monitor migration to other states, cessation of sex work or change in relationship status. All eligible sex workers listed from the 47 villages were approached for a face-to-face interview, and those who consented to participate (verbal or written) were interviewed. Research field staff received training on confidentiality. A 5-day training of field staff (n=20) prior to each survey round covered all aspects of the study protocol, informed consent procedures and the survey tool (including interview techniques), as well as confidentiality, understanding of gender inequalities, violence and HIV to prepare them to respond appropriately to participants needs. The field work was overseen by two supervisors who monitored data collection and provided ongoing training to interviewers.
A community advisory board of sex workers was set up to inform all aspects of study design, implementation and consent procedures, to ensure it was acceptable to the community and to help monitor any adverse events (defined as a report of sexual/physical violence). Outreach workers delivering the intervention collected reports of violence during regular sessions with sex workers, completing a report when incidents occurred. These reports were monitored and reported to the crisis management committee, a committee comprising representatives from the CBO and community members providing legal, psychological and emotional support on violence-related issues. Ongoing qualitative interviews across both arms with sex workers and their IPs provided regular insight into how the intervention was working and alerted the team to any harms. Strategies were put in place to minimise risks that might occur as a result of participation in Samvedana Plus or the research. These included ensuring that outreach workers did not refer to a woman’s sex work unless she herself spoke openly of this, not offering condoms in front of IPs to prevent inadvertent disclosure of sex work and ensuring that outreach workers or male champions did not reveal the relationship to the family and friends of IPs.
Outcomes
The primary outcome was were the proportion of sex workers reporting (1) any physical or sexual IPV in the last 6 months, (2) severe physical and/or sexual IPV in the last 6 months and (3) consistent condom use with their IP in the last 30 days. IPV was measured using questions adapted from the WHO Multicountry Study on Domestic Violence and Women’s Health, which has been shown to have high internal consistency in different settings.28 Consistent condom use was defined as the use of condoms during sexual intercourse (every time vs most of the time/sometimes/never).
Secondary outcomes sought to assess the impact of the intervention on the pathways between the intervention and outcome, including changes in (1) reports of acceptance of IPV (in relation to accepting physical violence in response to sex work or domestic transgressions), (2) disclosure of IPV to family and friends of community members, (3) improved knowledge of self-protection strategies (identifying allies or counter measures), (4) self-efficacy (defined as confidence) to negotiate condom use with IPs and (5) solidarity among sex workers around issues of IPV (defined as confiding in other sex workers about IPV).
Behavioural data were collected through a structured questionnaire at baseline (September 2014), midline (September 2016) and end line (September 2017) administered by independent trained field workers who were not involved in the intervention. The full definition of outcomes is included in the supplementary material (online supplementary appendix 2).
Supplemental material
Statistical analysis
Our sample size calculation assumed a mean of 12 sex workers per village, a total of 800 sex workers and a refusal rate of 10%. Power calculations were conducted, assuming an IPV prevalence (past 12 months) of 47% and consistent condom use (past 12 months) of 38% based on initial assessments. The power calculation was performed by analysing simulated data from 800 women, distributed across clusters using empirical data with a range in variance across cluster-level proportions of IPV (15%–25% of the total variation) and a narrow range of effect sizes (risk ratio=0.75–0.80). Power calculations did not account for stratification used in the randomisation or include adjustment for baseline levels of the outcome, since the correlation over time was not known. Results suggested that the trial had >80% power to detect a risk ratio of 0.77, if the coefficient of between-cluster variation was between 0.15 and 0.25.27
The primary analyses used an adjusted, individual-level intention-to-treat analysis, comparing outcomes among sex workers in intervention and control villages at end line. The statistician conducting the analyses was blinded to study group allocation. We included all women surveyed at end line even if they were not interviewed at baseline. All comparative analyses allowed for the clustering of sex workers within villages using a likelihood-based random-effects regression model. All of the outcomes were binary and logistic regression models were fitted. All primary comparative analyses were adjusted for the two village-level stratification factors (village size and sex worker population size) and the baseline cluster-level value of the outcome under consideration. A priori confounders and other characteristics that could affect the outcome but are unlikely to be on the causal pathway were adjusted for using endline individual-level data if they were judged to be imbalanced at baseline. ORs (intervention vs control) with corresponding 95% CIs were calculated for all outcomes. A sensitivity analysis was conducted to assess the effect of covariates that were measured at end line but not at baseline (ie, alcohol and mobility) but judged to be associated with the outcome. Unadjusted between-group mean differences (intervention minus control) were reported for completeness. In order to explore pathways to effect, we describe the prevalence of our primary outcomes at baseline, midline and end line. We report cluster-level summaries (mean of the cluster-level means) by trial arm for each primary and secondary outcomes as an additional sensitivity analysis.
Role of the funding sources
The funders had no role in study design, data collection, data analysis, data interpretation or writing of the report. PJ, LP and SI had full access to all the data. All authors commented on drafts and approved the final report.
Results
At baseline, 328/405 sex workers were interviewed in Samvedana Plus villages (equivalent to 81% of eligible sex workers with IPs registered with the CBO) and 292/404 in control villages (72%). At midline, 322/352 sex workers were interviewed in the Samvedana Plus villages (92%) and 189/223 in the control villages (85%). At end line, 288/323 sex workers were interviewed in Samvedana Plus villages (89%) and 259/346 in control villages (75% of list). The main reason for non-participation across both arms and survey rounds was due to temporary unavailability, migration and refusal to participate in the study (figure 1). During the course of Samvedana Plus, no serious adverse events were reported, but seven deaths occurred unrelated to project activities.
Sociodemographic, sex work and partner-related characteristics of sex workers were similar across trial arms at baseline (table 2). The mean age of the participants was 34.5 years (SD=7.3), and only 10% were literate. The majority (82%) had an alternate source of income other than sex work, such as agricultural (57%) or other manual (17%) labour. The mean duration of sex work was 19 years (SD=7.8), the mean number of clients per week was three (SD=2.7), and 77% sold sex at their home. At baseline, almost all participants (97%) reported just one current IP; only 1% reported more than one; and 2% did not have a current IP but had one within the last 6 months (table 2). Overall, IPs were older than sex workers. A slightly higher proportion of IPs in the Samvedana Plus villages visited their partners daily/weekly compared with monthly or less often in the control arm (67.6% vs 62.5%), and a higher proportion of women said their IPs knew about their sex work status in Samvedana Plus villages compared with the control arm (19.6% vs 12.0%). A higher proportion of sex workers were members of the CBO in Samvedana Plus compared with the control villages (63.9% vs 58.2%). Alcohol use by an IP during sex was lower in the Samvedana Plus compared with the control arm (21.4% vs 25.5%).
Baseline characteristics of sex workers and trial outcomes by trial arm
At baseline, we observed a lower prevalence of recent physical or sexual IPV (31.4% vs 45%) and recent severe IPV (23.7% vs 33.8%) in the Samvedana Plus villages compared with control. Consistent condom use was lower in Samvedana Plus villages compared with control (38.9% vs 46%). Among secondary outcomes, acceptance of IPV was higher in the Samvedana Plus villages compared with control (59.2% vs 55.1%); disclosure of IPV (46.3% vs 52.1%) and solidarity among sex workers around issues of IPV were lower (15% vs 22 %). There was no difference in other secondary outcomes across arms (table 2).
Programme monitoring data showed that Samvedana Plus reached 425 sex workers and their 528 IPs. At end line, survey responses show that 76% of participants in the Samvedana Plus villages had received one of the three key intervention components: 57% of sex workers received individual counselling; 12% received couple counselling; and 69% attended one or more group reflection sessions on various issues or aspects within IP relationships. Among the total sample, 47.6% had ever received between three and five individual counselling sessions; 31.5% had had between three and five sessions in the last 6 months; 10% received more than two couple counselling sessions; and 47.9% had attended more than four group reflection sessions. In addition, 41% had attended a folk media show; 21% had attended a campaign or rally at which aspects of IP relationships were discussed; and 13% had attended a training session on leadership (table 3).
Exposure to Samvedana Plus intervention among FSWs from intervention arm
Reported IPV
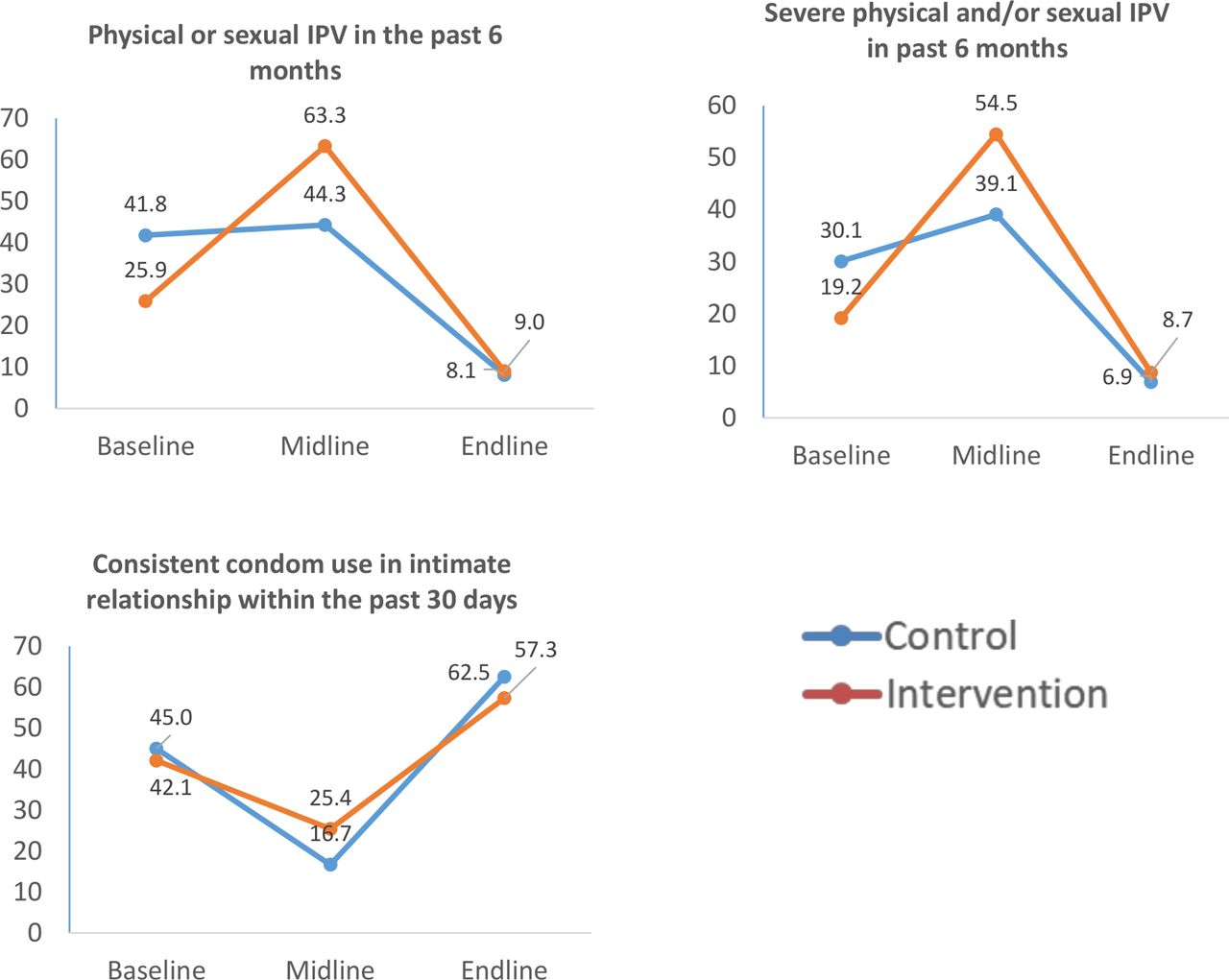
We observed increased reporting of IPV between baseline and midline and then a sharp decrease at end line in both study arms (figure 2). In the Samvedana Plus villages, any sexual/physical IPV in the last 6 months increased from 25.9% at baseline to 63.3% at midline and then dropped to 9.0% at end line. Likewise, severe physical and/or sexual violence increased from 19.2% to 54.5% and then dropped to 8.7%. For both violence measures, prevalence increased more sharply in the Samvedana Plus arm compared with control at midline and then declined sharply at end line in both arms. Consistent condom use decreased between baseline and midline but less sharply in the Samvedana Plus arm (42.1%–25.4%) compared with control (45.0% vs 16.7%). It then increased at end line but with little difference between Samvedana Plus (57.3%) and control (62.5%).
{kind=link}
{kind=link}
Prevalence of primary outcome by intervention arm and survey round. IPV, intimate partner violence.
Individual-level analysis of trial outcomes
Table 4 Presents the individual-level analysis of primary and secondary outcomes at end line by study arm. Findings suggest no evidence of a difference in IPV or consistent condom use across arms.
Effects of the intervention on outcomes at end line
Results suggest that Samvedana Plus was associated with a 5.6 percentage point decrease in acceptance of IPV (adjusted OR (AOR)=0.62, 95% CI 0.40 to 0.94, p=0.025), an 8.8 percentage point increase in awareness of self-protection strategies to address IPV (AOR=1.73, 95% CI=1.04 to 2.89, p=0.035) and a 7.6 percentage point increase in solidarity (defined as confiding or turning to peers around issues of IPV) (AOR=1.69, 95% CI=1.02 to 2.82, p=0.042). There was no statistically significant effect associated with disclosure of IPV (AOR=2.07, 95% CI 0.42 to 10.26) or self-efficacy to negotiate condom use with IPs (AOR=0.96, 95% CI 0.61 to 1.50). Sensitivity analyses showed that findings did not change after adjusting for covariates not measured at baseline (sex worker alcohol use or migration).
Cluster-level summaries of trial outcomes at end line
As with the individual-level analysis, we found little difference in the unadjusted cluster-level summaries for sexual or physical IPV from an IP in the last 6 months (8.7% vs 6.0%) or for severe physical/sexual IPV (5.1% vs 3.5%) between the Samvedana Plus and control arms. There was also little difference in reported consistent condom use in Samvedana Plus communities compared with control communities (61.5% vs 57.8%). Similar to the individual-level analysis, findings suggested a small difference in acceptance of IPV in the Samvedana Plus arm compared with the control arm (68.6% vs 73.2%), a larger effect of Samvedana Plus on knowledge of self-protection strategies against IPV compared with the control arm (20.6% vs 9.3%) and disclosure of IPV (76.7% vs 54.7%). Contrary to the individual-level analysis, the cluster-level summaries suggested that self-efficacy to negotiate condom use with an IP increased in communities receiving the Samvedena Plus intervention compared with those in the control (65.4% vs 58.3%). There was no evidence of differential reports of solidarity around IPV issues among sex workers at a cluster-level in intervention compared with control communities (37.6% vs 36.8%) (table 5).
Cluster-level summary of the outcomes at end line
Discussion
This is the first cRCT to evaluate an intervention to reduce IPV among sex workers in India and globally. We found no evidence of effect of the Samvedana Plus intervention on IPV or consistent condom use. Findings show that the intervention influenced attitudes and responses to violence in terms of reducing acceptance of IPV and increasing awareness of self-protection strategies to address IPV, as well as some evidence it increased sex worker solidarity to talk about IPV. These positive effects did not translate into an actual reduction in IPV or an increase in condom use associated with Samvedana Plus.
Levels of physical and sexual IPV increased from baseline to midline in both the intervention and comparison communities, more pronounced in the intervention communities. This raised the possibility that the intervention itself may have increased IPV in the short term. However, careful monitoring for adverse events throughout the implementation of Samvedana Plus was not consistent with the intervention having caused harm. Neither the crisis management teams nor the outreach workers received reports from sex workers of violent episodes linked specifically to the programme. Similarly, there was no difference in the proportion of relationships that ended during the study period between arms. As an added assurance, we undertook a rapid assessment postunblinding of the trial results to explore the possibility that the intervention caused harm. We conducted interviews with the CBO, outreach workers and selected participants alongside a review of programme data. Monitoring data suggested that reports of IPV did increase slightly following the start of the intervention and more sharply after the module on IPV was introduced in group sessions and then remained steady through the study implementation period (online supplementary appendix 3). One explanation of this could be that the initial escalation represented increased reporting by sex workers due to expanded awareness of what constitutes violence or increased empowerment, a theory endorsed by CBO workers and in other evidence.29–32 This leads us to conclude it unlikely that the higher levels of IPV reported at midline represents a true programme-induced increase in violence frequency.
Supplemental material
We further believe methodological factors may have contributed to the increase in IPV and the decline in condom use at midline and the decline in IPV and the increase in condom use observed at end line. The tension between maintaining the trial conditions and the desire of implementing agencies to address the immediate needs of the population can undermine the strict conditions of randomisation required in trials. Similar problems have been observed in other RCTs conducted among women living in poverty.33 We believe that there was a spillover from Samvedana Plus to comparison villages, with the CBO and existing peer educators providing HIV-related counselling, enlisting assistance of more highly-trained Samvedana Plus staff to assist women experiencing violence, irrespective of study arm, and thus undermining the randomisation process. Second, when facilitating researchers’ access to participants, outreach workers and peer educators may have instructed participants on how to respond to key questions in order to register a positive effect of the intervention and to guarantee the wider availability of the intervention and further funding for their work.
We know from the evaluation of the earlier Avahan programme that engagement with the CBO and visits from peer educators were associated with a reduction in violence experienced by sex workers from clients and the police.19 34 The positive engagement of the CBO during Avahan’s non-randomised implementation and the problematic engagement of the same CBO during Samvedana Plus implementation raise the question of whether it is wise to undertake a randomised trial in collaboration with a community-based group whose loyalty falls naturally with the well-being of its members. At the very least, we should have invested greater effort in helping peer educators, CBO leadership and Samvedana Plus outreach workers to better understand the logic and importance of maintaining separation between intervention and control villages. While the action undermined the impact evaluation of Samvedana Plus, it does indicate the positive views of the CBO to the intervention, as well as highlight the importance of embedding qualiative work to understand the complex mecahnisms through which the intervention might or might not work, that an RCT cannot explain. This is explored in depth in a linked process evaluation.29
Other lessons from Avahan highlight that changing the structural and normative environment around sex work is critical to the success of antiviolence efforts, for example, through advocacy with policy makers and sensitisation of police and media towards violence against sex workers.26 Trial evidence from women in the general population in Uganda likewise emphasises the importance of multilevel community mobilisation strategies that work with policy makers, community leaders and activists, police, young people, and men and boys to challenge attitudes towards IPV, to decreasing physical and sexual IPV.35 This suggests the need to focus more broadly on changing societal and community norms that sustain violence in order to reduce IPV. This is particularly relevant in this context where domestic violence is the norm in marriage and where devadasi women seek to achieve cultural legitimacy by emulating aspects of traditional marriage in their intimate partnerships.29 While Samvedana Plus included mobilisation at the community level through street theatre, this was not the key focus of the intervention.
The lack of intervention effect on consistent condom use with intimate partners speaks to the difficulties in encouraging condom use within intimate relationships,21 particularly among sex workers where non-use of condoms is often used as a way to symbolically differentiate their personal relationships from purely commercial encounters.36 Condomless sex is also used by sex workers in this setting to demonstrate intimacy and fidelity to their partner, who frequently demand exclusivity as a condition of the relationship. This is particularly relevant here where sex work was often concealed from partners and the lack of condoms used to prove that individuals were not engaging in sex work.29 37 We found some evidence to suggest that the intervention had a small effect in reducing acceptance of violence. This, alongside increased awareness of self-protection strategies and some evidence of increased solidarity, raises the possibility that the intervention had a small positive impact on challenging social norms and attitudes towards violence. However, acceptance of violence remained high (67%), particularly with respect to transgressions of gender norms, roles and responsibilities ‘belonging to’ women. Linked qualitative data suggested violence in a relationship is a normative expectation of marriage and, as such, is welcomed by some devadasi women engaged in sex work as an endorsement of their relationship being ‘real’.17 29
Our theory of change posited that reduction in IPV would be facilitated by building trust and communication between sex workers to foster increased support for each other and changing social norms. Evidence from a systematic review documents that community-based ‘empowerment’ interventions working on similar principles to mobilise communities of sex workers have achieved impressive reductions in HIV and violence, both internationally and in India.38 Evidence from sex workers in China suggests that having financial and social support from peers was the single largest protective factor against IPV.39 Ethnographic research has shown that the success of interventions that seek to mobilise communities is dependent on long-term commitment, strong community organising and adopting an integrated social model of health, with sex workers taking on increased decision-making responsibilities.40 In the context of the devadasi community of sex workers in rural areas with high levels of poverty and stigmatisation, this poses particular challenges. Secrecy surrounding IP relationships means that women were often reluctant to speak out for fear of disclosing the relationship, making it harder to seek support from the community. Sustained funding for the CBO is imperative to build on the increased solidarity around IPV that the Samvedana Plus intervention began to cultivate.
In addition to concerns about the validity of violence reporting, the study has several other important limitations. The increased solidarity around IPV observed in the individual-level analysis was not reflected in the cluster-summary approach that was applied to check the robustness of estimates. The direction of the effect was comparable in both models, although the magnitude of effect was far lower in the cluster-level summary, possibly due to reduced power.41 However, 76% of sex workers participating in the surveys had received at least one component of the intervention by end line, and this is in line with other community evaluations of interventions to address violence and HIV among low-income women.42 43 It is also possible that we have not captured the entire sex worker population in the study area but only those in contact with the CBO in both arms. For example, migration among sex workers for work in the region is common. At baseline, 18% of the sample did not go on to participate in the surveys as they had temporarily migrated to neighbouring cities in Maharashtra state for work. During the study period, cuts to government-funded HIV programming led to a reduction in the numbers of HIV peer educators working in control areas, so recruitment in control areas had to rely more on people already known to the CBO and thus missing those not exposed to any intervention.
In summary, while the intervention did not result in a reduction in IPV or an increase in condom use, it did have a small effect in reducing acceptance of violence, increasing awareness of self-protection strategies and showing some evidence of solidarity around IPV among sex workers. However, any certainty with which we can interpret these secondary outcome effects is challenged by our uncertainty in the measurement of IPV. Participatory qualitative research is needed to develop more accurate and appropriate ways of measuring IPV among this population for future evaluations, including working with the CBO to develop a study design that they can support without influencing violence reporting or jeopardising their ability to provide essential services. The high acceptance of IPV that remained, alongside lessons learnt from Avahan and other IPV intervention studies, suggests that more effort should be expanded at structural and policy levels to challenge acceptance of gender-based violence within communities. This is necessary in order to create an enabling environment within which targeted interventions to address the heightened stigma and violence experienced by devadasi sex workers can be implemented. In the meantime, interventions to mobilise and further empower the devadasi community are paramount. The direction and content of these interventions have to be led by sex workers, facilitated by CBOs and sustained through long-term commitment and investment.
Acknowledgments
The views expressed here are those of the authors and do not necessarily reflect the official policy or position of the Department for International Development, the South African Medical Research Council or the University of Manitoba. We thank all members of Chaitanya AIDS Tadegatwa Mahila Sangha for their tireless work delivering the intervention and helping to reduce violence among sex workers. We also thank Mr Gautam B Sudhakar and Mr Raghavendra Kamati for supervising the data collection work, Mr Raj Kamur, Ms Anushia Anbalagan and the finance and administrative staff for providing other logistical support, and the efforts of field research investigators in data collection.
References
Footnotes
PJ and LP are joint first authors.
Handling editor Kerry Scott
Twitter @prakashpj13
Contributors LH, SI CW were coinvestigators and supported conceptual development and study implementation and write-up. LP, PJ, RP and SI designed the statistical analysis, and PJ and LP led the data analysis. LP led the manuscript development. PB, TSB, MC CD, MG, RJ and SR supported the data analysis, interpretation and manuscript development. SI, RP and PJ managed oversight of data collection. PB, SR KDL and RT were responsible for assisting in tool development and study implementation. All authors reviewed and approved the final manuscript prior to submission. SI and LH are joint last authors.
Funding Project Samvedana Plus is funded by UKaid through the Department for International Development as part of STRIVE, an 8-year programme of research and action tackling the structural drivers of HIV (http://strive.lshtm.ac.uk/) led by the London School of Hygiene & Tropical Medicine and the What Works to Prevent Violence Against Women and Girls Global Programme (https://www.whatworks.co.za/) led by the South African Medical Research Council. Samvedana Plus research is led by the Karnataka Health Promotion Trust with the involvement of the University of Manitoba.
Competing interests None declared.
Patient and public involvement statement Sex workers were involved in the design of the intervention through the community-based organisation (Chaitanya AIDS Tadegattuva Mahila Sangha (CATMS)) that is a collective of sex workers who work to empower sex workers. There was close collaboration between CATMS, Karnataka Health Promotion Trust and London School of Hygiene & Tropical Medicine throughout the course of the study in the development of the study design, the research instruments and the interpretation of results.
Patient consent for publication Not required.
Ethics approval Ethics approval was given by the St. Johns Medical College and Hospital Institutional Ethics Committee (reference number 110/2013) and the London School of Hygiene & Tropical Medicine (reference number 8658).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.