Article Text

Abstract
Background The global prevalence of diabetes mellitus is increasing alarmingly. However, the quality of vital medicines and medical products used to treat and monitor diabetes remains uncertain but of potential great public health significance. Here, we review the available evidence on the quality of antidiabetic medicines and supplies for self-monitoring of blood glucose (SMBG) and discuss their potential impact for the patients and society.
Methods Searches were conducted in PubMed, Embase, Google Scholar, Google and relevant websites in English and French. The Medicine Quality Assessment Reporting Guideline (MEDQUARG) was used to assess the quality of medicine quality surveys.
Results 52 publications on the quality of antidiabetic medicines, including 5 medicine quality prevalence surveys and 20 equivalence studies, were analysed. The prevalence surveys and equivalence studies included 674 samples of which 73 (10.8%) were of poor quality. The median (Q1–Q3) concordance with MEDQUARG items was 30.8% (19.2%–42.3%). No prevalence surveys on SMBG supplies’ quality were found, but 29 publications, including falsified products and incorrect results due to strip degradation or contamination, were identified.
Conclusion There is little accessible evidence on the quality of antidiabetic medicines and SMBG supplies. Surveys were poorly designed and reported, making data aggregation and interpretation problematic. Despite these caveats, these results suggest that there are important issues with the quality of medical products for diabetes that need focused monitoring. There is an urgent need to achieve consensus protocols for designing, conducting and reporting medical product quality surveys.
PROSPERO registration number CRD42016039841.
- medicine quality
- substandard and falsified medicine
- diabetes
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Substandard and falsified medical products for managing diabetes will negate the benefits of modern diabetes treatment and the public benefit of reduced complications.
Better understanding of the epidemiology of substandard and falsified diabetes medications and self-monitoring of blood glucose (SMBG) supplies and their potential impact on patients and society is needed.
What are the new findings?
Our study demonstrated that of 674 samples analysed, about 1/10 were substandard or falsified but this prevalence is not generalisable globally.
Issues with the quality of SMBG supplies were identified (including falsified products and incorrect results due to strip degradation or contamination).
What do the new findings imply?
Our findings showed that, despite the scarcity of the data, there are important issues with the quality of medical products for diabetes that need to be tackled.
Besides increasing the quality of the surveys, consensus would facilitate evidence pooling and summarising to better understand the global burden of this problem.
Introduction
Diabetes mellitus (hereafter diabetes) is a growing threat to global health with significant mortality and morbidity related to myriads of non-communicable and communicable disease consequences. In 2015, diabetes afflicted ~415 million people globally and this is predicted to reach 642 million by 2040, equivalent to 1 in 10 adults.1 The direct annual global cost of diabetes is estimated at US$827 billion.2
In the USA, approximately four in five adults with diabetes rely on antidiabetic medicines to control their glucose levels.3 Insulin is required for type 1 diabetes treatment, and is also used widely for advanced type 2 diabetes. In 2015, insulin was within the top 10 best-selling medications globally (in terms of number of prescriptions and sales value).4 5 It is estimated that globally ~100 million people need insulin.6 Type 2 diabetes treatment involves lifestyle change encouragement, but antidiabetic medicines are often required for the control of hyperglycaemia and prevention of long-term complications.1 7 8 Oral antidiabetic sale in 2016 was estimated to reach close to US$20 billion.9 There has also been a surge in innovative expensive oral therapies such as gliptins.
There are key public health issues with cost and access to antidiabetic medicines, especially insulin,5 and to specialised diabetes care. With huge price variation between countries and increasing demand, insulin and new oral antidiabetic medicines are likely to be attractive targets for falsification and are at risk of substandard production.10 High prices of some antidiabetics may prompt patients to look for more affordable options, including illegitimate sources such as unregistered physical and internet pharmacies.11
Nearly 60% of the global costs of diabetes are borne by low-income and middle-income countries (LMICs), with substantial treatment costs paid out-of-pocket and insufficient medicines regulation. This limits access and thus risks use of poor quality medical products, exacerbating financial hardship and impairing peoples’ lives and productivity.12
Patients with diabetes often need to check their blood glucose concentration multiple times per day using strip-based hand-held glucose meters. The cost for such self-monitoring of blood glucose (SMBG) can account for approximately one-third of the total cost of consumables, including insulin and needles, for type 1 diabetes management.13 This expense has prompted both falsification of glucose strips and reselling of secondhand unused glucose strips at reduced price.10 14 15 In 2008, the US Food and Drug Administration (FDA) and the American Diabetes Association warned against using resold strips as they may give incorrect results.14 16
Due to their vital role in diabetes management, poor quality antidiabetic medicines and SMBG supplies will inevitably have adverse health impacts for patients, both short and long term. Low active pharmaceutical ingredient (API) content and, for oral preparations impaired gastrointestinal dissolution, will increase the incidence of macrovascular and microvascular complications due to compromised glucose control, and hence increase individual and societal economic costs.17–19 High API content may also bring grim immediate consequences. Deaths have been linked to falsified antidiabetic medicines in China containing dangerously high amounts of the oral antidiabetic agent glibenclamide.20 21 Poor quality SMBG supplies will impair patients with diabetes from receiving correct medication doses, potentially causing life-threatening hypoglycaemia, hyperglycaemia and long-term consequences. Poor quality antidiabetics and SMBG supplies will also decrease faith in the health system, confuse patient and clinical decision-making and risk use of unapproved treatments.
The circulation of poor quality medicines and medical products, whether falsified, substandard or degraded, is a major global public health problem. No country is immune.22–28 A recent WHO report suggested that in LMICs, ~10.5% of medicine samples (mainly anti-infectives) analysed were substandard or falsified (SorF).28 Although medical product regulatory systems are usually reliable and functional in high-income countries, poor quality medicines and medical devices have been identified.11 15 27 29 The extent of the problem seems more pronounced in financially poor countries where regulatory systems are often weak.24 26 27 30 Rising concern about the consequences of poor quality medicines over the last decade has focused on anti-infectives.31 However, there is growing awareness of this issue for chronic non-communicable diseases, for example, a recent survey described that 16.3% of cardiovascular medicines sampled in ten sub-Saharan African countries were poor quality.32 These will have significant public health impact and if poor quality diabetes medical products are also prevalent they will have an additive global toll on health. The recent WHO report stated that seven member states reported 11 substandard and falsified (SF) diabetes medicines between 2013 and 2017 but details are not given.28 As there is no global understanding of the epidemiology of poor quality medical products for diabetes, we reviewed the available evidence and discuss the potential impact for patients and society.
Methods
Search strategy
Reports were identified through systematic searches in PubMed, Embase, Google Scholar in English and French up to 30 April 2018, using the search terms (online supplementary file 1) ‘diabetes’, ‘antidiabetics’, the names of active pharmaceutical ingredients (eg, ‘insulin’, ‘metformin’, ‘glibenclamide’), ‘glucose meter’, ‘strip’; combined with terms relevant to medicine quality (eg, ‘falsified’, ‘counterfeit’, ‘substandard’, ‘degraded’). Reports were also identified in Google from the first 20 pages of results and other sources such as websites of international organisations interested in medicine quality and medicines regulatory authorities (online supplementary file 1). After removal of duplicates, the titles and abstracts were first screened, and full text of the identified articles were then assessed for eligibility. The reference lists of the eligible articles were also manually screened for inclusion.
Supplemental material
Eligibility criteria
Published scientific articles and grey literature assessing or discussing the quality of antidiabetic medications were included. Articles describing the development or assessing the performance of chemical techniques for the analysis of antidiabetics quality were excluded. Articles without clear conclusion on the quality of the assessed products or with uninterpretable results (eg, conflicting quality results for the same samples analysed in two different laboratories)33 were excluded. Articles on the quality of SMBG supplies found through the searches were included. However, articles describing the accuracy and performance of glucose meters and strips were excluded, as were reports on the quality of insulin syringes, pens and needles.
Key definitions
‘Falsified’ refers to products that ‘deliberately/fraudulently misrepresent their identity, composition or source’.28 30 34 In this review, ‘fake’, ‘counterfeit’, ‘spurious’ and ‘falsely labelled’ medicines are regarded as synonyms of falsified, a term that emphasises public health rather than intellectual property issues inherent in the term ‘counterfeit’. ‘Substandard’ medicines, also called ‘out of specification’, are authorised medical products that ‘fail to meet either their quality standards or their specifications, or both’.34 This may result from negligence or errors during the manufacturing process by authorised manufacturers,28 35 or degradation through deterioration because of inappropriate storage/transport in the supply chain.11 Information is usually insufficient to distinguish errors within factories from those in the supply chain, a key evidence gap as the solutions for the two differ.22 As it is not possible to reliably classify a medicine as substandard or falsified without packaging analysis,22 in this review products that failed at least one quality test without information on packaging authenticity, and falling outside the acceptance range of the specifications chosen as reference by the authors (either specific pharmacopoeia monograph or in-house specifications), are defined as ‘substandard or falsified’ (SorF).
‘Prevalence surveys’ are studies in which samples were collected within the pharmaceutical supply chain to assess their quality, in order to describe the prevalence of circulating SF medicines. ‘Equivalence studies’ are those whose main objective is to assess the quality of different marketed brands of the same API(s) assuming that the collected samples would represent the quality of the brand and not an estimate of the frequency of individual samples of different quality. In most cases, equivalence studies aim at providing information on brand(s) as a whole, whereas prevalence surveys aim at evaluating individual samples of marketed medicines to give an estimate of their frequency in a community.
Risk of bias assessment
The prevalence surveys methodology and reporting were assessed using Medicine Quality Assessment Reporting Guidelines (MEDQUARG). MEDQUARG is a comprehensive checklist composed of 26 items proposed to be included in the reporting of medicine quality surveys.36 For each item, all criteria are to be fulfilled to be awarded one point. Prevalence surveys were assessed independently by two investigators with a third person resolving any disagreement. Since there were no standardised tools available to assess lay types of publication, their risk of bias was not specifically assessed.
Data collection, analysis and reporting
The data extracted included year of publication, publication type, definition used for medicine quality, location of survey, sampling strategy, sample size and failure rate (with additional description of the type of failure when applicable). A ‘data point’ is defined as a location where medicines were collected for quality analysis, at a given time and during a given study. A Microsoft Access database 2013 used in a similar review from our group was adapted for the purpose of the study.22 Microsoft Excel 2013 and RStudio V.0.99.486 were used for the data analysis. Qualitative variables were expressed as numbers and percentages (n (%)). Quantitative variables were expressed as median, as well as first and third quartiles (Q1 and Q3, respectively).
This review is reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (online supplementary file 2).37
Supplemental material
Patient and public involvement
This research was done without patient or public involvement.
Results
After removal of duplicates, 11 989 out of 15 653 publications gathered through electronic searches and other sources identified in the methods were screened by title and abstract (figure 1).

PRISMA flow diagram of the selection process of the publications on antidiabetic medicine quality. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Of these, 286 full-text publications were reviewed and 38 were included. Fourteen additional publications identified through manual reference screening were also included, yielding a total of 52 publications. Twenty-four (46.2%) of the included publications were original research articles published in scientific journals (figure 2). The number of publications increased from one publication in 2008 to nine in 2016 but decreased to three in 2017 (figure 3). Two publications (3.8%) had unstated year of publication. All publications will be mapped on the Infectious Diseases Data Observatory Medicine Quality Surveyor system (www.iddo.org).
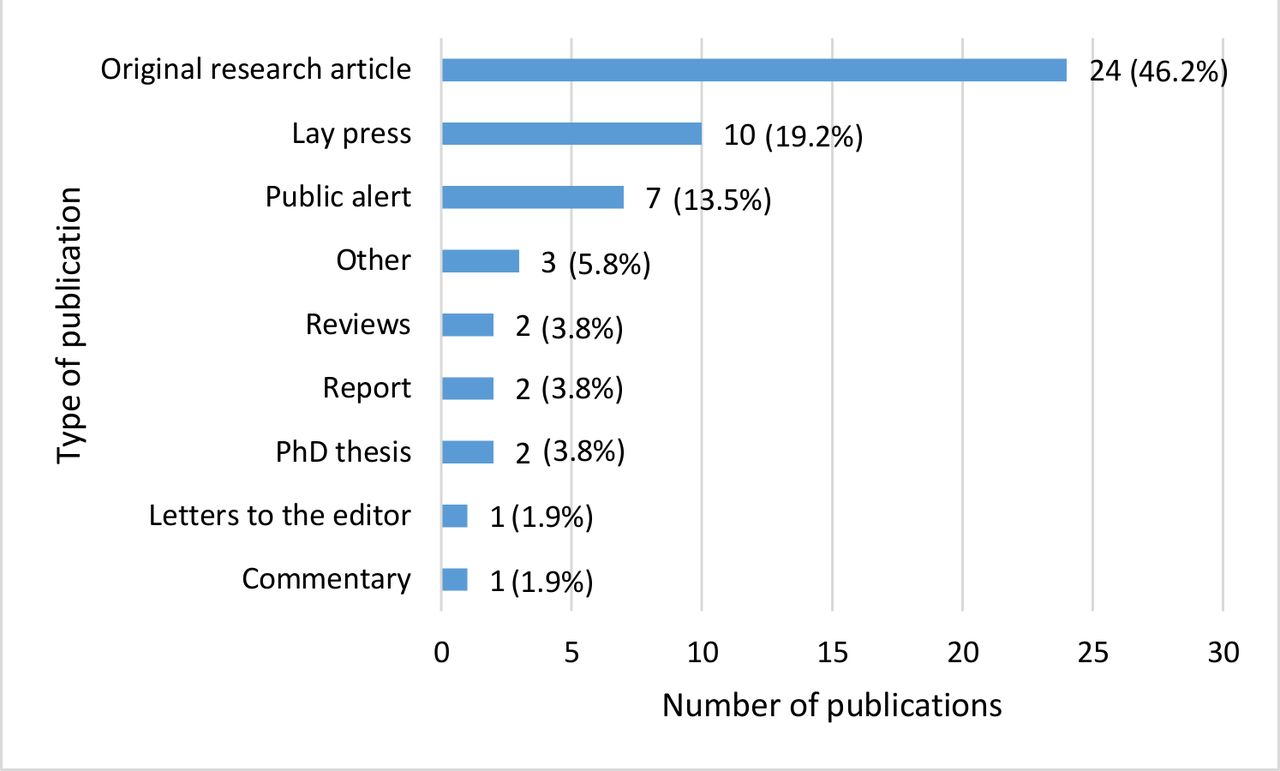
Types of publications related to the quality of medicines for diabetes.
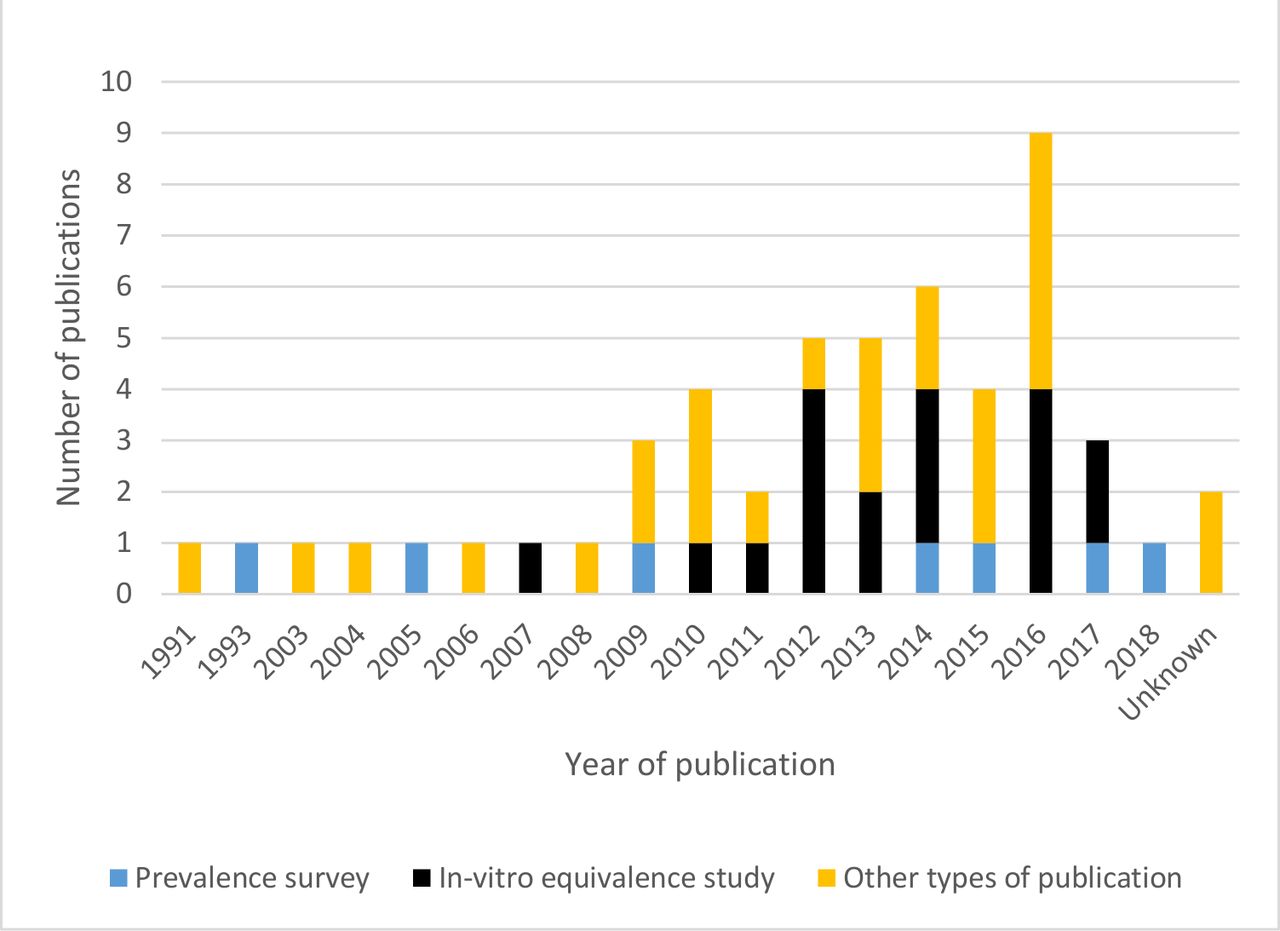
Number of publications over time related to the quality of medicines for diabetes.
Out of the 52 publications, 5 were prevalence surveys (9.6%) and 20 (38.5%) were equivalence studies (table 1). All surveys and studies included evaluated oral antidiabetics. The most commonly assessed are metformin (in four prevalence surveys and 13 equivalence studies) and glibenclamide (in two prevalence surveys and five equivalence studies). We found one survey investigating the quality of 84 insulin samples in 1979.38 However, due to the absence of reference to the acceptance range of the specifications chosen for the ‘conventional insulin preparations’ at the time of the study, we decided to exclude this article from this review.
Main characteristics of prevalence surveys and equivalence studies of antidiabetic medicines included in the reviewBecause of the limited number of samples tested for quality in the studies included in this review, the numbers should not be interpreted as representative of the prevalence of specific SF antidiabetics (please refer to the discussion section of the current paper for more details)
High-performance liquid chromatography (HPLC) and thin-layer chromatography analyses were conducted in four and one prevalence surveys, respectively. Various technologies were used in equivalence studies such as HPLC or UV-visible spectrophotometry (online supplementary file 3). The British Pharmacopoeia and United States Pharmacopeia (USP) were the most commonly followed standards (in 12 and 11 articles, respectively).
Supplemental material
In total, 674 samples were collected in 38 countries; 527 (78.2%) from 31 countries for prevalence surveys and 147 (21.8%) from 9 countries in equivalence studies (table 2). The median (IQR) number of samples collected in prevalence surveys and equivalence studies were 112 (45–179) and 5.5 (5–8), respectively. Of the 57 data points, there were seven (12.3%) for India, five (8.8%) for Nigeria, four (7.0%) for Saudi Arabia, two (3.5%) each for Jordan and Cambodia, and one (1.8%) each for the other countries (table 2). The country where samples were collected was not specified for 5.5% (n=37) of samples.
Failure rate per country in prevalence surveys and equivalence studiesBecause of the limited number of samples tested for quality in the studies included in this review, the numbers should not be interpreted as representative of the prevalence of specific SF antidiabetics (please refer to the discussion section of the current paper for more details)
Thirty-six out of 527 (6.8%) and 37 out of 147 (25.2%) samples failed at least one quality test in the prevalence surveys and the equivalence studies, respectively. A total of 73 out of 674 samples (10.8%) analysed were thus SorF. The highest proportion of SorF antidiabetic medicines was observed in Asia and Middle East (11.5%, 29/253), and the lowest proportion was observed in Australia and Oceania with no samples failing, although only one data point was available and six samples were tested for quality. The frequencies of failures in Africa, the Americas and Europe were 9.8% (22/224), 6.8% (3/44) and 2.7% (3/110), respectively. There were 4 out of 57 data points with unknown sampling location.
The largest number of samples collected in prevalence surveys and equivalence studies were of metformin (n=345, 45.5%) and glibenclamide (n=266, 35.1%) (table 3).
Quality of medicines per API in the included prevalence surveys and equivalence studiesBecause of the limited number of samples tested for quality in the studies included in this review, the numbers should not be interpreted as representative of the prevalence of specific SF antidiabetics (please refer to the discussion section of the current paper for more details)
Among samples identified in prevalence surveys, the most common reason for failure was API content analysis (n=26/36, 72.2%) (online supplementary file 4). Dissolution, disintegration or drug release failures were the most common failures in equivalence studies (online supplementary file 4), with 54.1% (n=20/37) of samples in equivalence studies failing.
Supplemental material
Out of 40 samples failing API content analysis in the surveys and studies, 16 (40.0%) had low API content and 13 (32.5%) had high API content. The API content was unstated for 11 (27.5%) samples. Twenty-two (55.0%) and 17 (42.5%) samples failing API content analysis were metformin and glibenclamide, respectively. The lowest API content, in comparison to that stated on the packaging, was 82.3% (metformin) and the highest was 111.5% (glibenclamide). Out of 258 samples that had dissolution and/or disintegration and/or drug release testing performed, 27 (10.5%) failed at least one of these tests. Further details on the number of failing samples can be found in online supplementary file 4.
Seven out of 73 samples failing at least one test (9.6%) were substandard, while the rest (n=66, 90.4%) were categorised as SorF medicine since packaging analysis was not performed. In one study, packaging analyses were performed by sending survey findings to manufacturers, but the packaging analyses results pertaining to the authenticity of the medicines were not described.39
MEDQUARG was mentioned and followed in one of the three (33.3%) prevalence surveys published after the publication of these guidelines in 2009 (figure 4, online supplementary file 5). Only one out of three was published in a scientific journal, with MEDQUARG score of 19.2% and failure rates of 0.0% (0/4 samples).40 Four (80.0%) out of five prevalence surveys scored positively on less than half of the MEDQUARG items. The median MEDQUARG score of all surveys was 30.8% (IQR 19.2%–42.3%).
Supplemental material

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Percentage of concordance of the prevalence surveys with 26 items included in the MEDQUARG checklist. MEDQUARG, Medicine Quality Assessment Reporting Guidelines.
The time frame, definitions of medicine quality used, ethical considerations, chemical analysis method validation and whether blinding at analysis was performed were described only in one prevalence survey (20.0%) while the sampling methodology and statistical methods were described in two (40.0%). Only two prevalence surveys (40.0%) used random sampling of outlets. Comparative packaging analysis (ie, comparing packaging with that of the authentic medicine from the manufacturer) was performed in three prevalence surveys (60.0%). In one study, label and ‘non-comparative’ packaging analyses were conducted by comparing the samples with the standard US FDA packaging requirements (eg, using label text and package insert requirements).40 The outlets types sampled per data point were detailed in four prevalence surveys (80.0%). However, none gave details on the outlet size such as their turnover. The stated manufacturer’s name and address of the collected medicines were given in two prevalence surveys (40.0%), while the rest of the surveys neither give this information nor the reason why the information was not released.
In addition to scientific papers, nine seizures (17.3%), five recalls (9.6%) and two case reports (3.8%) were found (table 4); eight (15.4%) described medicines falsification. Other types of publications discussing antidiabetic medicine quality are presented in online supplementary file 6, including the entries in US Pharmacopeia Medicines Quality Database that lists two reports of the quality of gliclazide from Cambodia in 2008, both samples passed screening tests.41
Supplemental material
Summary of seizures, recalls and case reports of medical products for diabetes management
We found no prevalence surveys of the quality of SMBG supplies. Of the 29 publications (table 5) on SMBG quality, the majority were recalls/alerts (n=17, 58.6%).15 42–56 Sixteen publications described inaccurate blood glucose strip results, resulted in under and overestimation of blood glucose levels, risking wrong treatment doses.42 48 52 53 55–59 These quality issues arose through imperfect transportation conditions or sealing, causing glucose strip degradation due to exposure to humidity and/or temperature.45 51 53 Contamination by chemical substances during manufacturing resulted in inaccurate results and a recall of 62 million strips.54 One manufacturer released an online alert system to monitor falsified products in which poor quality glucose strips with inaccurate/potentially inaccurate test results were reported between 2006 and 2015, in Bangladesh, China, Egypt, Greece, India, United Arab Emirates, Pakistan, France, Singapore and the USA.60 61
The main characteristics of the reviewed publications on the quality of SMBG supplies
Discussion
We synthesised, from diverse publicly accessible sources, the available evidence on the quality of antidiabetic medicines and SMBGs. The data available are very meagre and do not allow an accurate synthesis of the current situation. However, these findings raise concern and suggest that more evidence is needed to inform policy and interventions. Around 1/10 of the antidiabetic medicines analysed in 5 prevalence surveys and 20 equivalence studies failed analyses. Quality issues related to SMBG supplies included falsified products and incorrect results due to strip degradation or contamination. With the large and increasing global burden of diabetes and the increasing use of antidiabetics globally, the published evidence clearly shows the lack of available evidence to assess the extent of the problem and to identify actions towards ensuring good quality antidiabetics and SMBG. Efforts to increase access to antidiabetic medicines and consumables, especially insulin in LMICs,5 need to be linked to ensuring their quality.
We found no prevalence surveys on SMBG supply quality and only five publicly available surveys aiming to assess the quality of antidiabetics available in the market. Only three published since 2010, among which only one was published in scientific journals.40 The total number of antidiabetic medicine samples analysed in the five included surveys was very small (674 samples) in comparison to the vast use of antidiabetic medicines worldwide, estimated to be worth >US$50 billion in 2017.62 63 This number fell down to four if considering only the single survey published in scientific journals after the publication of MEDQUARG, with none of the four samples failing any tests.
For insulin alone, the demand in 2014 was 2.15 billion vials.6 However, we retrieved only one publicly available report on insulin quality. This report, published in 1979, showed that the 64 ‘conventional insulin preparations’ tested contained ‘considerable amounts’ of several hormonal peptide contaminants including pancreatic glucagon, pancreatic polypeptide, vasoactive intestinal peptide and somatostatin.38 In the past, insulins were extracted and purified from animals. These contaminants are now avoided through newer manufacturing methods, for example, recombinant human insulin.64 This report reminds us that medicines deemed standard today may be deemed substandard in the future, as the standards applicable to medicines evolve. As there were uncertainties regarding the reference acceptance ranges for the amount of contaminants found, this study was excluded from our analysis.
The recent description of suspected illegal insulin seized by inspectors in Belgium is of concern.65 The quality of insulin delivery devices such as insulin pens and pen needles is outside of the scope of this review. However, the finding of falsified insulin pens in Argentina, and insulin pen needles in the UK, Poland and the Netherlands are worrying–highlighting the need for postmarketing surveillance of the quality of these products.66–69
We only included five prevalence surveys, in which glibenclamide, metformin, gliclazide and glimepiride were assessed, with none for numerous other antidiabetic medicines (see table 3). With a median of 112 samples collected in the five prevalence surveys analysed in this review—only two using random sampling—a global estimate of the prevalence of poor quality antidiabetics is thus not possible. However, since there should be no poor quality medicines or medical products circulating, the finding of any poor quality samples indicates a problem that needs further investigation.
There were only four data points from the Americas, despite North America and the Caribbean having the highest age adjusted adult prevalence of diabetes.1 Seven countries with high adult diabetes prevalence (20% or more) have no data points (ie, Kuwait, Qatar, Cook Islands, Marshall Islands, Nauru, Palau and Tokelau).1 China has the largest number of patients with diabetes globally1. No published prevalence survey of the quality of antidiabetic medications in the Chinese pharmaceutical supply chain was identified, although lethal cases of falsified glibenclamide, containing dangerously high glibenclamide content, were reported in 2009.20 21
The quality of reporting was poor, as reflected by the low MEDQUARG scores. Survey design and results were not well described, making it difficult to judge the evidence. Random sampling, that will minimise bias, was used in only two of the prevalence surveys reviewed, probably because random surveys require more resources compared with convenience surveys. A more economical but objective approach would be to use lot quality assurance sampling (LQAS), as a ‘screening’ step, to determine if the prevalence of poor quality medicines exceeds a predefined threshold, but LQAS cannot give an accurate estimate of prevalence.36
Only one of the surveys clearly delineate the classification of samples as SF. In most of the surveys and all the equivalence studies, quality was determined only by chemical analysis, without packaging analysis which is vital for distinguishing falsified and substandard medicines, essential data for determining actions.
Limitations of this review include that searches were conducted only in English and French, and that medicine regulatory authorities and the pharmaceutical industry are likely to have significant amounts of data not shared with the public. There may be unpublished data if no SF antidiabetics were identified in a survey, or if SF antidiabetics were found but public release may have been considered damaging to the country or pharmaceutical company.22 The publicly available data on antidiabetics quality included in this review are scarce, of low quality, and the studies varied greatly in methodology. Only two surveys were conducted using random sampling. Therefore, the summary presented in this work should be considered with caution. One of the variation is the reference standard used. In one study, manufacturer specifications of the innovator’s product were used as a reference to assess the quality of generic products. However, if acceptance ranges of the USP monograph from 2017 had been followed, the number of samples failing dissolution test would be reduced from 12 out of 23 (52.2%) to 8 out of 23 (34.8%).70 In most prevalence surveys, we found limited detailed information on samples and/or samples quality with breakdowns by outlet sampled (eg, licensed vs unregistered outlet), cost of medicines or country of manufacture. We thus did not perform causal factors analysis that, although crucial to better inform policy, could lead to misleading results and interpretation.
Poor quality antidiabetic medicines containing lower amounts of API than stated, or poor dissolution rate engendering reduced bioavailability will, as for non-adherent patients, risk developing macrovascular and microvascular complications,17 71 and severe infections, such as pneumonia, tuberculosis or melioidosis.17 72 73 Complication-related hospitalisations will further increase costs to patients and society.74
The USP 40 and the Chinese Pharmacopoeia (2010) percentage API acceptance range is 95%–105% for metformin and 90%–110% for glibenclamide tablets.75 76 There is limited evidence for the dose–response relationship for either medicine,77–79 making it hard to predict the relative risk of acute or regular underdosing and overdosing for either medicine. However, underdosing is likely to impair glycaemic control and with the inherent risk of hypoglycaemia with most of the oral antidiabetic medicines (especially with sulfonylureas such as glibenclamide) at normal doses, those containing high percentage API are especially dangerous.80 Glibenclamide has also been found in falsified erectile dysfunction drugs with devastating lethal hypoglycaemic consequences.81 Unexplained hypoglycaemia with new medicines, brand or batch numbers should prompt investigation of their contents.
Higher failure rates were found in previous reviews.22 23 82 83 Almost one-third of antimalarials tested failed either packaging or chemical tests in a review published in 2014.22 Failure rates of 19.1% and 12.4% were observed in a review of 96 articles for antimalarials and antibiotics, respectively.83 Although the number of publications gathered for these reviews were much larger than for our review, authors also concluded that the estimate of the prevalence and distribution of SF medicines could not be accurate because of the heterogeneity of study methodology, as illustrated by an I-square parameter of 0.99 in a recent meta-analysis.83
The evaluation of glucose meters and strips quality is complex since glucose readings are influenced by multiple factors, including the analytical properties of the device, the calibration and setting of the device and user compliance with testing procedures.84 The currently available standards for glucose meter and strip performance and scientific literature mainly focus on the accuracy of the device, overlooking user error or the clinical impact of inaccuracies.84 As with medicines, consensus on a standardised definition and methods to evaluate the quality of SMBG supplies and other medical devices must be established to enable a more valid prevalence estimation.27 30
Another notable issue is the unauthorised reselling of unused glucose strips. The advocates of this practice argue that this facilitates strip access for the poorest, as resold glucose strips are sold for less than the standard market price.10 However, it has been argued that unauthorised reselling risks improper storage, exposing strips to humidity and heat potentially affecting accuracy. One company strategy of proactively detecting circulating poor quality SMBG supplies and coordinating with governmental agencies to enforce regulation61 has resulted in detection of falsified products.60 Such models of surveillance and coordination are needed to effectively tackle the problem of SF medicines and medical products.
Conclusion
The currently available data on the quality of antidiabetic medicines and consumables are sparse and of variable quality, suggesting that aggregated data should be interpreted cautiously. However, despite the relatively small number of publicly available studies, poor quality antidiabetic medicines and SMBG supplies were identified on four continents, suggesting that this is an important public health issue and should be further investigated, through factory inspections and postmarket surveillance, to ensure that the benefits of modern diabetes management are fulfilled for the burgeoning global population with diabetes.
Acknowledgments
We are very grateful to the MSc in International Health and Tropical Medicine team, Bodleian Libraries, and Lao-Oxford-Mahosot Hospital-Wellcome Trust Research Unit Director and staff for their support throughout this work, especially Vayouly Vidhamaly, Phonepasith Boupha, and Kem Boutsamay. We also thank Proochista Ariana, Peter Horby, Nia Roberts and Eric Ohuma. We would like to thank the Indonesia Endowment Fund for Education (LPDP) for supporting KS throughout her MSc.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.
- 86.
- 87.
- 88.
- 89.
- 90.
- 91.
- 92.
- 93.
- 94.
- 95.
- 96.
- 97.
- 98.
- 99.
- 100.
- 101.
- 102.
- 103.
- 104.
- 105.
- 106.
- 107.
- 108.
- 109.
- 110.
- 111.
- 112.
- 113.
- 114.
- 115.
- 116.
- 117.
- 118.
- 119.
- 120.
- 121.
- 122.
- 123.
- 124.
- 125.
- 126.
Footnotes
Handling editor Seye Abimbola
Contributors PN, CC and KS designed the review. KS and CS conducted the literature review in English and French, respectively. Screening and extraction were performed by KS under the supervision of CS and CC. KS, CS and CC assessed the quality of surveys. KS performed the analysis under the guidance of PN and CC. KS prepared the first manuscript draft. PN and CC provided revision and guidance on the overall direction of the study. All authors approved the final version for publication.
Funding Wellcome Trust of Great Britain MAPQAMP grant 202935/Z/16/Z.
Disclaimer The funder of the study had no role in study design, data collection, data analysis, data interpretation or writing of the report.
Competing interests CS, PN and CC are supported by the Wellcome Trust.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available in a public, open access repository. All data relevant to the study are included in the article or uploaded as online supplementary information.