Article Text

Statistics from Altmetric.com
Summary box
African countries are not on track to achieve global targets for non-communicable disease (NCD) prevention, driven by an insufficient focus on ecological drivers of NCD risk factors, including poor urban development and the unbridled proliferation of the commercial determinants of health.
As the risk factors for NCDs are largely shaped outside the healthcare sector, an emphasis on downstream healthcare service provision to the exclusion of upstream population-level prevention limits the goals of universal health coverage (UHC) and its potential for optimal improvements in (achieving) health and well-being outcomes in Africa.
The political will for UHC in Africa will miss the opportunity to turn the tide of this emerging NCD epidemic in Africa, if not oriented to a systems for health rather than a solely healthcare-centric approach. A successful approach needs to proactively incorporate wider health determinants (sectors)—housing, planning, waste management, education, governance and finance, among others—in strategies to improve health. This includes aligning governance and accountability mechanisms and strategic objectives of all ‘health determinant’ sectors for health creation and long-term cost savings.
Researchers have a vital role to play, collaborating with policy makers to provide evidence to support implementation and to facilitate knowledge sharing between African countries and globally.
The third sustainable development goal (SDG), ensuring healthy lives and well-being for all at all ages, although comprising multiple components, is often strongly linked with the concept of universal health coverage (UHC) and its underlying principles of equity, quality and financial protection. The importance of addressing the upstream determinants of health as a vital accelerator of progress in achieving the SDGs has been recognised1; however, in practice, the implementation of UHC has often been restricted to a disease-fighting, healthcare-centric approach. This constrains the ability to achieve WHO’s definition of health as the attainment of ‘complete physical, mental and social well-being’. Vast amounts of experience and research show that health outcomes are shaped by multitiered and multifaceted factors that do not stem solely from the healthcare sector.
The WHO recognises the importance of health determinants, noting that UHC comprises much more than just healthcare and that taking steps towards UHC means steps towards equity, health-promoting development priorities, social inclusion and cohesion, and including public health campaigns.2 Building on this, we argue that improved upstream planning and policy may even reduce the need for public health campaigns. Implementation of this more comprehensive and holistic approach to UHC is essential to ensure the full realisation of demographic dividends, particularly in an era of non-communicable diseases (NCDs), many of which can be prevented through upstream interventions that are not typically considered as healthcare.
Africa is experiencing a double burden of disease,3 with the burden of NCDs like type 2 diabetes increasingly borne by disadvantaged populations. In addition to mortality and morbidity, NCDs strike people during their economically productive years,4 5 with significant implications on wealth of individuals, their families and their countries. Sub-Saharan Africa has the largest cohort of young people in history,6 coupled with challenges related to rapid urbanisation, climate change and insecurity. Efforts to optimise the benefits of health and wealth need to be prioritised.
NCDs are fundamentally related to behavioural risk factors, which are affected by complex ecological drivers intersecting in local social, cultural, policy and economic contexts. They are further impacted on by global dynamics, such as the globalisation of unhealthy diets and lifestyles, short-term donor-driven governance priorities and the unbridled proliferation of industries that produce harmful substances, such as tobacco, alcohol and ultraprocessed high sugar, and high-salt foods. Additionally, existing public awareness programmes are often not effective, and advocacy for NCDs is weak compared with the support given to other epidemics such as HIV/AIDS.
Fragile health systems conspire with these other factors to ensure that African countries are way-off track to achieve global targets for NCD prevention and management.4 In 2001, African nations adopted the Abuja Declaration, pledging to allocate at least 15% of their national annual budgets to health spending. Yet, only three countries in the African region have attained the goals of the Abuja Declaration and the High-Level Taskforce on Innovative Financing for Health.7 Where healthcare spending is low, healthcare spending on NCD is even lower; in a region where donors drive health financing, most donor finance is still oriented towards communicable diseases, with about 1%–2% dedicated to NCDs.7 Out of pocket expenditure results, where NCD care is needed, with poorer households spending more of their per capita household income on NCDs.8
The result? An exemplar is diabetes. Even if countries meet the SDG goal of decreasing mortality from diabetes by one-third, or if they reduce age-specific and sex-specific prevalence to their 2010 levels (a key aim of the WHO NCD Global Action Plan), the economic burden of diabetes in 2030 will still be 61% higher than that in 2015.9 In South Africa, the estimated costs for implementation of local guidelines to achieve reasonable access to care for cardiovascular diseases would substantially impact on the ability of the health system to care for other illnesses.10 For most African countries, to achieve true UHC to manage NCDs by 2030 would require an unprecedented investment in healthcare services.
So, what can be done? (See box 1.) The crippling cost implications of waiting to address NCDs downstream in the healthcare system are clear. In the context of limited resources, addressing upstream determinants will translate to long-term savings by ultimately reducing the burden of diseases that needs to be addressed within the healthcare system. Countering the notion that this is impossible, given that African countries are struggling to achieve narrow definitions of UHC, we argue that these countries cannot afford not to explore innovative approaches to reduce the need for healthcare to reduce healthcare costs in the long term. It is imperative to evolve the implementation focus of UHC from one of solely reactive provision of health services to one that incorporates primary prevention to flatten the current trajectory of the NCD epidemic in Africa. Sectoral silos need to be broken down to achieve this. For example, obesity, an important risk factor for diabetes, is related to access to infrastructure that encourages an active lifestyle: transit systems, built environment features that promote walking, cycling and green spaces.11 This infrastructure needs to be safe, clean, functional and of reasonable quality. This is the remit of urban planning, waste management and local governments. Smoking, which acts synergistically with diabetes to cause disability and death, is driven by access to cigarettes, harmful advertising and messaging from the tobacco industry that encourage adoption of smoking by young people and stressful living conditions that predispose people to take up unhealthy habits, among others. These factors are within the areas of responsibility of housing, trade policies and government sectors responsible for advertising. Ensuring access to environments that promote healthy eating to prevent obesity is predominantly a matter for policies largely developed outside the healthcare sector. Therefore, beyond healthcare delivery, healthcare practitioners should be encouraged to advocate for such policies that protect health through addressing upstream determinants.12
Recommendations for action to breakdown non-communicable disease (NCD) silos
Policy makers
Systems for health must work alongside healthcare services: Reducing the burden of NCDs is a complex problem requiring healthcare services to intersect with multiple other systems that affect health.
Health financing should be focused on producing health rather than managing disease: Multisectoral action to reduce the NCD burden requires long-term (extending beyond one policy cycle) budgeting structures and accountability mechanisms for co-benefits across the multiple systems that drive health.
Health creation must be central to development: Africa has the opportunity to redefine urban development to ensure inclusion of health promotion solutions. Measures of success should be grounded in the health of the populations.
Policies should align to create health as an outcome: Policies directly or indirectly resulting in disease have no place alongside those that promote access to care for those diseases.
Policies and spending should reflect country needs: Spending and policies should not reflect richer donor country interests but should be reoriented to address health outcomes more systematically and sustainably, including through upstream, multisectoral action.
Research community
Research and policy collaborations should be the norm: Academics and policy makers should come together to discuss policy priorities for reducing NCDs and how to provide evidence to support those priorities.
Investment in platforms for knowledge sharing: South–South and North–South learning should be facilitated to ensure rapid learning between cities and countries in Africa.
Support frugal innovation for health (beyond healthcare): Long-term frugal innovation is needed to make growing cities and societies spaces that promote health and equitable thriving. African philanthropists can play a role in this innovation.
External research funders and donors
Research funders and development assistance for health donors: should prioritise funding in line with disease burden and recipient country defined need, which encourages long-term approaches to health creation.
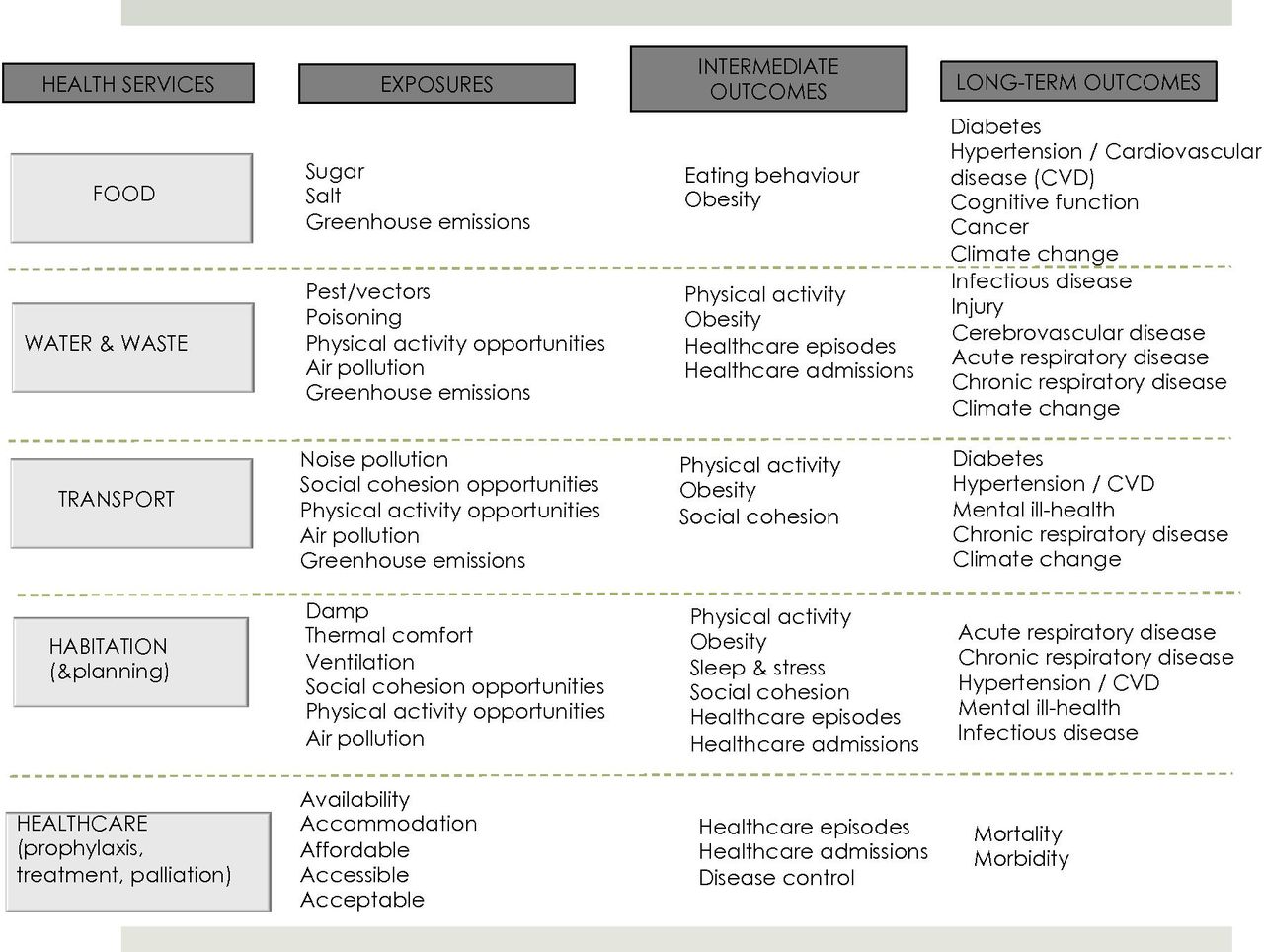
Achievement of UHC that does not bankrupt health budgets or restrict disease coverage so much as to be worthless rhetoric requires innovative policy making, intersectoral accountability mechanisms and financing structures, which encourage multisectoral action. Figure 1 highlights the importance of intersectoral action by proposing a diverse range of services that can be considered ‘health services’ by virtue of the impact they have on population health. This shows the familiar healthcare service that ultimately aims to reduce morbidity and mortality from all diseases; this is usually assessed at an intermediate level using indicators such as disease control, admissions and other healthcare episodes. The figure also highlights how transport and planning, for example, could be considered health services by virtue of the services these systems provide for health. For example, transport and planning policies that prioritise obesity and cardiovascular risk reduction by equitably creating physical activity opportunities and reducing air pollution exposure can measurably contribute to reducing diabetes and cardiovascular disease burden in the long term; thus providing a health service. While this action does not necessarily need to be implemented under the ‘UHC’ umbrella, the political momentum behind UHC provides an opportunity to raise the profile of such approaches to achieving health for all. To be clear, we argue that for long-term healthcare savings and population health, there is a need for a focus on upstream prevention for health creation and protection, not limited to early detection in those already at risk of NCDs, alongside current strategies to treat existing disease. Other examples of such upstream approaches include tax on sugar-sweetened beverages and aligning performance goals of urban development policies with improving healthy food consumption and increasing active living.

{kind=link}
Examples of multisectoral action for disease prevention.
There are promising developments and policy opportunities that can be leveraged to ensure that development produces health as an outcome in Africa. There has been a history of Healthy Cities Initiatives in Africa13 with some cities such as Dar es Salaam and Cape Town developing healthy city programmes without the support of international organisations. In addition, there is an Inter-ministerial Taskforce on Health and the Environment in Africa, which convenes health sector and environment sector experts and ministers across Africa to address the environmental threats to human health.14
The first and second WHO Africa Health Forums in 2017 and 2019 have recognised NCDs as an emerging threat in Africa and the need for intersectoral action to address the social determinants of these diseases.15 The Commonwealth Ministers of Health meeting and World Health Assembly in May 2019 also provide an opportunity to build on these initial calls to action to critically engage with constraints and enablers of implementing intersectoral approaches to NCD prevention and to foster transdisciplinary partnerships with researchers to develop and evaluate knowledge-based, contextually relevant, innovative and bold interventions to create health that leaves no one behind.
Footnotes
Handling editor Seye Abimbola
Contributors TO and JID conceptualised the manuscript. TO conceptualised and developed the figure and wrote the first draft of the panel recommendations. TO and EM drafted the first version of the manuscript. All authors contributed to writing and finalising of the manuscript.
Funding TO is supported by an Iso Lomso Fellowship of the Stellenbosch Institute for Advanced Study (STIAS). JID is also a visiting fellow at STIAS. This work was in part supported by a grant to TO from the LIRA 2030 Africa Programme, implemented by the International Council for Science in partnership with the Network of African Science Academies and the International Social Science Council, with support from the Swedish International Development Cooperation Agency. This funding supported the writing of the manuscript. The funders had no role in the design or writing of the manuscript.
Competing interests None.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available.