Article Text

Abstract
Liver disease is a significant public health burden in both high-income and low-income countries, accounting for over 2 million annual, global deaths. Despite the significant mortality burden, liver diseases are historically a neglected problem due to a lack of accurate incidence and prevalence statistics, as well as national and international programmes targeting these diseases. A large portion of deaths due to liver diseases can be treated (eg, chronic hepatitis B), cured (eg, chronic hepatitis C) or prevented (eg, acute liver failure due to medications) if prompt diagnosis is made, but currently diagnostic methods fall short. Therefore, there is a critical need to fund the development of prompt, effective diagnostics for liver function, specifically in low-income and middle-income countries where the landscape for this testing is sparse. Here, we review and compare available and currently emerging diagnostic methods for liver injury in low-income and middle-income settings, while highlighting the opportunities and challenges that exist in the field.
- low- and middle- income countries
- point-of-care diagnosis
- liver disease
- drug induced liver injury
- alanine-aminotransferase
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- low- and middle- income countries
- point-of-care diagnosis
- liver disease
- drug induced liver injury
- alanine-aminotransferase
Summary box
Liver disease poses a significant global public health burden and accounts for over 2 million deaths per year. The burden is significantly acute in low-income and middle-income countries.
There is a lack of diagnostic tests to screen for liver injury at the point-of-care in low-income and middle-income countries.
This lack of diagnostic development for global health can be attributed to a lack of funding and incentives.
Looking forward, we should borrow lessons from the vaccine and pharmaceutical industries to incentivise diagnostic development and create funding for the purpose.
Liver diseases and the global burden
Liver disease poses a significant public health burden in both high-income and low-income countries, accounting for over 2 million annual, global deaths.1 2 Despite this significant mortality burden, liver diseases remain a neglected problem due to a lack of accurate evaluation of incidence and prevalence, as well as a lack of national programmes targeting these diseases.2 3 A large portion of deaths due to liver diseases can be treated (eg, chronic hepatitis B), cured (eg, chronic hepatitis C) or prevented (eg, medication driven liver failure) with prompt diagnosis; therefore, there is a need for effective actions enabling prompt diagnosis, specifically in low-income and middle-income countries (LMICs) where the current diagnostic landscape is sparse.
Types of liver disease
Liver disease is a broad term referring to any general disorder of the liver, including many conditions with a wide variety of causes. In high-income countries, liver disease is commonly caused by alcohol and obesity—resulting in conditions such as alcoholic hepatitis and fatty liver disease. In LMICs, liver injury is usually caused by infectious diseases, such as infectious hepatitis (typically B or C) and the side effects of HIV and TB medicines, which are toxic to the liver and result in drug-induced liver injury (DILI). Hepatitis prevalence,4 diagnosis5 6 and treatment7 8 are well studied. DILI is less understood in terms of burden statistics, diagnostic options and the prevention plans.
In high-income countries, retrospective studies show that 8.5%–23% of patients on antiretroviral therapies (ARTs)9 10 and 5%–28% of patients on anti-TBs11 experience hepatoxic side effects. In LMICs, there are little data, but a potential for increased rates of hepatotoxicity given the higher prevalence of both HIV and TB. In Ethiopia, 14%–20% of adults on ART show elevated serum liver enzymes as a marker of hepatocellular injury.12 In Uganda, 30% of symptomatic patients with acute liver disease showed markers of DILI due to TB medications.13
To prevent DILI, patients on HIV and TB medicines require consistent screening of liver function as part of their routine treatment. Unfortunately, for HIV-positive and TB-positive patients with limited resources, the need for regular screening remains acute due to the scarcity of diagnostic facilities offering ultrasound, blood biochemistry and liver biopsy tests. Even when offered, a shortage of skilled staff makes testing and interpretation of results challenging.14
The standard of care and associated barriers
Typically, liver health is evaluated through a liver function panel, measuring blood levels of total protein, albumin, bilirubin and liver enzymes. Elevations in alanine aminotransferase (ALT) and aspartate aminotransferase (AST), two biomarkers of liver injury, are the most common abnormality seen on liver function panels15 and enter the bloodstream due to hepatocellular injury or death. ALT is found primarily in the liver, while AST is found in the liver, kidneys, brain, heart and skeletal muscle. Therefore, to preliminarily detect hepatocellular injuries, the liver function panel can be narrowed to just ALT.16
In high-income settings, the standard of care includes monitoring of ALT through a venipuncture blood draw, followed by centrifugation to separate serum or plasma, and then testing of the serum or plasma through an absorbance-based assay on a large, automated platform in a centralised laboratory.14 In LMICs, this testing is near impossible due to a lack of trained phlebotomists, equipment and reagent shortages. Supply chain issues add major delays in clinical decision-making and a substantial loss for patient follow-up.14
To combat some of these challenges and bring ALT testing (from the centralised facility) to the point-of-care (POC), two FDA-approved devices exist on the market (Roche Reflotron Plus and Alere Cholestech LDX). However, both are arguably too expensive for LMICs and require technical capacity that may not be locally available.14 For situations like these, WHO has created a benchmark for technology development in LMICs, enumerating the ideal design targets into the ASSURED criteria (figure 1): affordable, specific, sensitivity, user-friendly, rapid/robust, equipment free and delivered/accessible.17
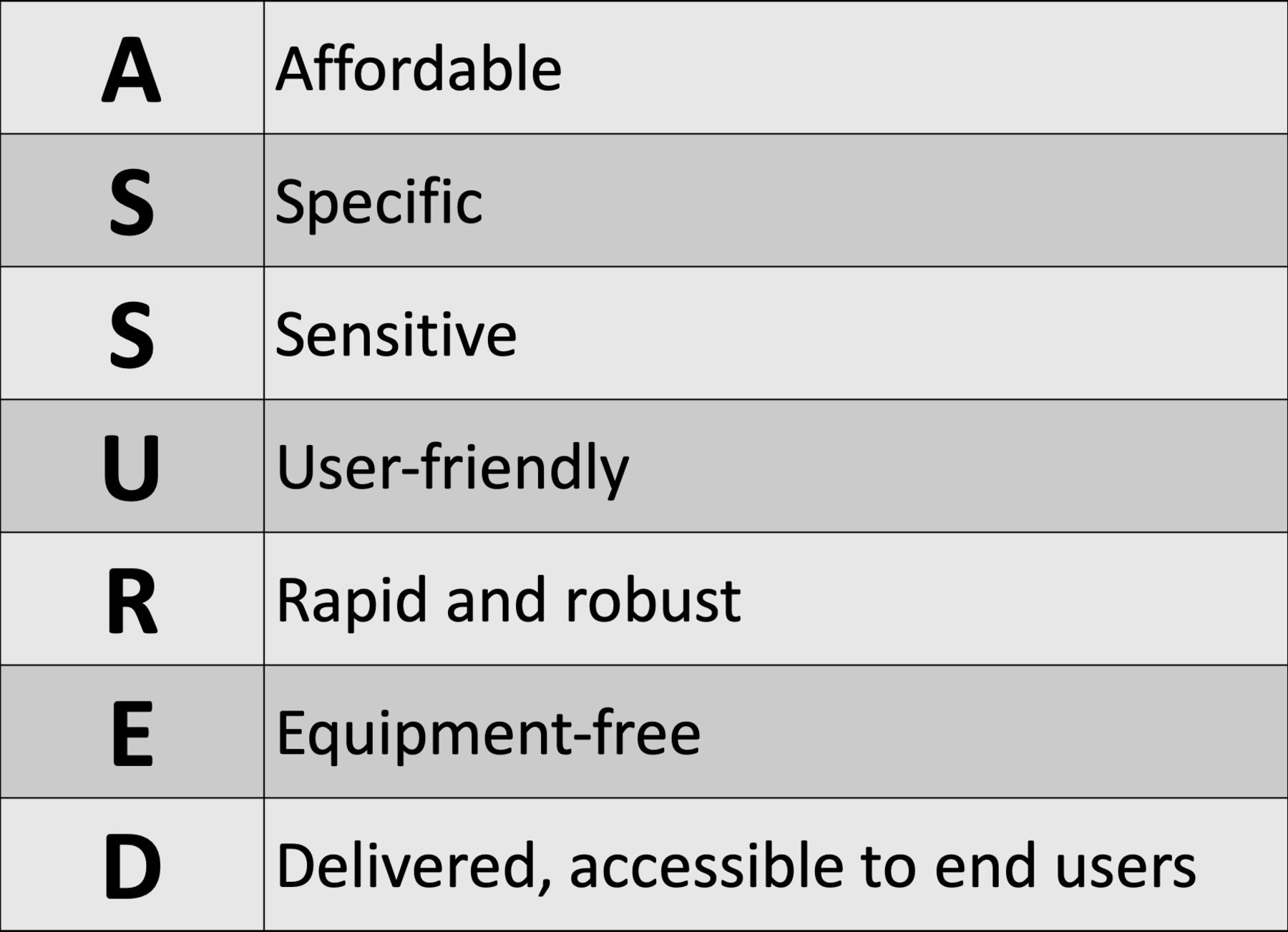
WHO assured criteria for successful point-of-care diagnostics in low-income and middle-income countries.
The following sections review the current technologies in the pipeline, their challenges and ways to overcome the bottlenecks for better outcomes in LMICs.
Academic research
Several research groups have reported detection techniques for measuring ALT in blood samples through a variety of methods, including colorimetry, spectrophotometry, chromatography and electrochemistry. Some radiochemical methods have been used historically, but less so now due to the known harmful impact on human health.18 These technologies and methods each offer specific advantages, but none of the assays discussed in this section have yet been commercialised in LMICs.
Academic research: Colorimetric and spectroscopic assays
Colorimetric assays for ALT rely on chemical reactions that produce colour visible to the naked eye. The assay is sometimes paired with use of a spectrophotometer or colorimeter for quantification of the colour intensity. Without use of a spectrophotometer or colorimeter, colorimetric assays are very inexpensive and are equipment free. However, these assays are considered only semiquantitative, as the user interpretation can be subjective and variable.
Colorimetric assays date back to the 1960s and typically used coupling enzymes and diazonium salts,19 20 producing colour according to extent of ALT activity. Despite the promise, these assays still require extensive sample preparation and expensive readout equipment. A streamlined process to be used at the POC was never pursued, a common trend among many of the assays discussed here.
In other work, researchers developed a biochip to quantify ALT from serum using a colorimetric reaction.21 The chip consisted of a mixing and measurement sub-chips. Despite integration, the system still required input of serum, not whole blood, and would therefore still require use of a centrifuge. The chip also contained many expensive, miniature parts including a tungsten lamp, photodiode and picoammeter.21
More recently, a semiquantitative ALT scheme was used to group ALT concentration into three ranges: >5× upper limit of normal (ULN), 3–5× ULN and <3× ULN.22 23 This assay was developed into an integrated paperfluidic platform that could be used with a drop of whole blood and no spectrophotometer was required. This device underwent field testing at the Hospital for Tropical Diseases in Ho Chi Minh City, Vietnam, with an average of 91.5% agreement with the gold standard method.23 Although this assay found great success in field testing, no information was found as to further development and commercialisation of this device post 2013.
Moving away from colorimetry due to the semiquantitative nature, many research groups shifted towards spectrophotometric assays, capable of absolute quantification over a wide measurement range including wavelengths invisible to the naked eye (eg, UV and IR light).24–26 However, spectrophotometric assays are generally not suitable for the POC as they require expensive instrumentation. Additionally, the sensitivity of these assays can be a challenge due to presence of other components in blood that may absorb or fluoresce at similar wavelengths.
Academic research: Chromatographic assays
Quantification of ALT has also been demonstrated through chromatography, specifically gas–liquid chromatography.27 Gas–liquid chromatography offers the advantage of direct quantification, with no need for coupling enzymes and the ability to quantify multiple markers of interest, including ALT. However, chromatography is a slow, equipment-heavy process and has not been developed yet for a portable, LMIC-friendly set-up.
Academic research: Electrochemical assays
More recently, there has been an increased interest in electrochemistry due to the increased sensitivity of measurements and lack of expensive machinery.28–34 The glucometer, which is often affordable (US$30 for the reader, US$0.14 per test for the electrode chips), requires only an electrode chip, handheld electrochemical reader and involves minimal interaction from the user, is often touted as a success story.
For ALT detection, most electrochemical assays couple ALT to either an electrode immobilised pyruvate oxidase (POX) or glutamate oxidase (GOX), relying on subsequent detection of hydrogen peroxide (H202), as shown in figure 2. These assays typically use platinum or palladium modified working electrodes coupled to the secondary detection enzyme (POX or GOX), demonstrating assay sensitivity in the picoampere to nanoampere (U/L mm2) range.

{kind=link}
{kind=link}
Methods for electrochemical detection of alanine aminotransferase (ALT). ALT catalyses the transamination of l-alanine and alpha-ketoglutarate to pyruvate and glutamate. Since neither glutamate nor pyruvate are electrochemically active, ALT is coupled to either (1) pyruvate oxidase or (2) glutamate oxidase, relying on subsequent detection of H2O2 at a modified electrode.
Researchers have demonstrated an electrochemical assay to detect ALT levels by coupling ALT to POX and subsequently detecting the accumulating peroxide directly at an electrode; however, the high overpotential needed to detect the peroxide directly led to unwanted electron transfer when working with human serum samples.28 Easily oxidised species in blood (eg, ascorbic acid, uric acid) reacted with the electrodes and caused interfering signals. Therefore, research groups started to use a mediator (figure 2) or an electrochemically active species to act as a shuttle between the species being detected and the electrode. With a mediator, detection at lower potentials is possible with less interference from other analytes in blood.
Subsequently, other groups built on this research, using a range of creative mediators coupled to a POX or GOX.29–31 34 These assays, however, were never formulated into integrated devices that could be used at the POC, as they required extensive user preparation, equipment and set-up,29 and the need for cold chain storage in LMICs.30 31
We have recently demonstrated a quantitative assay for ALT without the use of POX or GOX. This electrochemical design exploits the ability of an ALT reactant, alpha-ketoglutarate, to react with hydrogen peroxide, which is detected electrochemically using Prussian blue modified electrodes.33 A novel aspect of this assay is the absence of immobilised enzymes on the electrode test strips. This contributes to major cost savings and easier fabrication techniques, creating the potential for less expensive testing at the POC in LMICs.
The sensors discussed in this section all vary in their specifications, trading off between improvements in sensitivity, limit of detection, linear range, response time, sample volume and fabrication complexity, but overall, none were developed into integrated biosensors for use at the POC in LMICs. Therefore, although recent movement in this space has been positive, there is a lack of translation from the academic realm to the field.
Patents and clinical trials
An ongoing clinical trial through the University of Pennsylvania and Group K Diagnostics is testing the accuracy of a POC device to test liver function within 20 min. Their proposed device uses paper microfluidics and results in a colorimetric response to liver enzymes in whole blood. A mobile phone application is used to record the colour change and output results. This study is still recruiting patients.35
Additionally, two patents were filed in February 2019. A patent titled ‘Quantitative Electrochemical Assay for Liver Injury’ was filed on 8 February 2019.36 This patent was based on the assay demonstrated in Moed and Zaman33 mentioned above. Second, a patent titled ‘Systems and Methods for Electrochemical Aspartate Transaminase (AST) and Alanine Transaminase (ALT) Detection and Quantification’ was filed on 28 February 2019.37 This patent puts forward an integrated device for quantification of ALT and AST from a fingerprick of whole blood. The device should be capable of all process steps starting with sample collection through quantification but has only been demonstrated to quantify pyruvate at this moment in time. This proof of concept is promising, but quantification of ALT and AST has yet to be demonstrated.
These clinical trials and patents are promising steps towards translation into the field but still have yet to make impact.
Barriers and bottlenecks
While there are positive steps among the research community towards novel assays for ALT detection, field testing and deployment in LMICs remains a challenge. In this section, we analyse possible barriers to field deployment and translation.
Why do laboratory technologies fail to translate to the field?
Funding proves to be a major problem as there is a lack of clear, feasible funding pathways for bringing products to the market. Specifically for global health, the funding pool remains very small relative to what high-income countries spend on their own health, representing only 1% of high-income health expenditure.38 Additionally, funding priorities (both governmental and foundation based) often change with administrations and with public health trends.38–40 This generates insecurity in long-term funding for specific public health challenges, creating a difficult environment to make any true impact.38 39 For example, currently global public health policies and funding agencies are concentrated on health conditions due to infectious diseases.40 This means that funding opportunities for other areas of health are much less lucrative and much less stable.
Aside from the funding landscape, there are many other pronounced barriers to implementation. First, inventors from high-resource settings often find it challenging to determine whether to seek regulatory approval in their own country, which could potentially lead to design changes and increases in cost and time to implementation.41 This is compounded by the challenge of attracting investors to low-margin medical devices for global health. Traditional (ie, financial) return on investment is often low or even negative in global health; therefore, it is difficult to make a business case for going to market. Additionally, to secure global intellectual property (IP) protection, patent applications need to be filed in each country that the device will be used in. A lack of IP protections in many LMICs further discourages investment in this area.41
Lastly, many technologies are developed in the academic space by technically strong-minded individuals, but these same individuals often have no experience in commercialisation and other business aspects of medical devices. Therefore, it is nearly impossible for them to scale up the device alone.41 It is often hard for this strong academic to partner with industry—this intensifies the already prominent discontinuity between the discovery stage of technology development (often in academia) and the trial/eventual marketing stage (often in industry).42 43
For all of these reasons combined, there is a need for appropriate funding and effective incentives towards prompt diagnosis of liver disease, specifically in LMICs.
Creating better incentives
In the last few years, academics and industry professionals have begun to bridge the polarising divide between them and enter into mutually beneficial relationships.42 This continued partnership could be key to bridging the gap between the discovery and marketing stages of technology development, therefore helping to propel technologies from the academic space into the field. Creative incentives could help to further bridge this gap; incentives of this type exist in the vaccine and pharmaceutical industries and could be applied here as well.
Looking at recent research from the neglected field of vaccine development, two promising incentivisation campaigns stand out: (1) the Advanced Market Commitment (AMC) model and (2) the Call Options for Vaccines (COV) method. These models aim to make vaccine sales more profitable and development costs less burdensome.
In the first model, for a qualifying vaccine, the AMC guarantees a certain price for a specified number of units.44 This incentivises development of novel vaccines by guaranteeing a profitable market, post development. With the COV model, purchasers make payments during the early stages of development in exchange for reduced future prices.45 This provides the developing company an early incentive to continue development, as dollars come in specified for the task.45
In the pharmaceutical space, the Options Market for Antibiotics model combines the principals of both the AMC and VOC models.44 46 This model aims to incentivise antibiotic development for applications in global health, where returns will be low. Here, a third party, typically an NGO or government agency, will purchase ‘options’ for an antibiotic, that they could redeem if/when the drug goes to market.44 If they purchase the options early in development, the price would be low, but the risk of the drug failing would be comparatively high. If they purchase the options near the end of development, the price would be much higher but the risk of failure lower.44
These methods, though examples of incentives outside of the diagnostic space, can pose as valuable models to help rally appropriate funding and execute on development of diagnostics for the POC. With better incentives and funding, we can bypass many obstacles to technology development in LMICs.
Conclusion
Liver disease is a pressing public health problem in both high-income and low-income countries and accounts for over 2 million annual, global deaths.1 2 Overall, there is a shortage of information on liver diseases of concern to HIV-infected and TB-infected individuals in LMICs; the dominant problem is the scarcity of diagnostic facilities offering liver function tests. Even when offered, these tests most likely cannot be carried out or interpreted due to a severe shortage of skilled pathologists.14
Academic movement in the ALT detection space has been trending towards electrochemistry, based on the ability to meet the ASSURED criteria and the potential to create an effective, integrated diagnostic. Despite this academic assay development, none have been integrated into wholistic devices for use at the POC. This is likely due to a lack of incentives and a lack of funding for research of this kind. Therefore, there is a need for appropriate funding, better business models and effective actions towards prompt diagnosis of liver disease at the POC, specifically in LMICs.
Acknowledgments
We are grateful to Katie Clifford and Mackenzie Hall for many discussions and for meticulous reading of the manuscript.
References
Footnotes
Handling editor Seye Abimbola
Contributors SM engaged in researching and writing the original draft, including creation of visuals. MHZ was responsible for project administration, supervision, and reviewing and editing of the manuscript.
Funding This research and programme was supported in part by a grant to MHZ at Boston University from the Howard Hughes Medical Institute Science Education Program.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No additional data are available.