Article Text

Abstract
Recent years have seen increasing momentum towards task shifting of basic health services, including using community health workers (CHW) to diagnose and treat common childhood illnesses. Yet few studies have examined the role of traditional healers in meeting families’ and communities’ health needs and liaising with the formal health system. We examine these issues in Tshopo Province in the Democratic Republic of the Congo, a country with high rates of child mortality (104 deaths per 1000 live births). We conducted 127 in-depth interviews and eight focus group discussions with a range of community members (mothers, fathers and grandmothers of children under 5 years of age) and health providers (CHWs, traditional healers, doctors and nurses) on topics related to care seeking and case management for childhood illness and malnutrition, and analysed them iteratively using thematic content analysis. We find significant divergence between biomedical descriptions of child illness and concepts held by community members, who distinguished between local illnesses and so-called ‘white man’s diseases.’ Traditional healers were far less costly and more geographically accessible to families than were biomedical health providers, and usually served as families’ first recourse after home care. Services provided by traditional healers were also more comprehensive than services provided by CHWs, as the traditional medicine sphere recognised and encompassed care for ‘modern’ diseases (but not vice versa). Meanwhile, CHWs did not receive adequate training, supervision or supplies to provide child health services. Considering their accessibility, acceptability, affordability and ability to recognise all domains of illness (biomedical and spiritual), traditional healers can be seen as the de facto CHWs in Tshopo Province. National and international health policymakers should account for and involve this cadre of health workers when planning child health services and seeking to implement policies and programmes that genuinely engage with community health systems.
- child health
- health policy
- public health
- health systems
- community health
- traditional medicine
- traditional healers
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- child health
- health policy
- public health
- health systems
- community health
- traditional medicine
- traditional healers
Key questions
What is already known?
Community health systems are increasingly understood as the ecosystems in which high-quality health services are delivered.
Task shifting to community health workers (CHW) can be an effective way to deliver treatment and care to sick children in the community.
What are the new findings?
In Tshopo Province, Democratic Republic of the Congo, traditional healers fulfil many of the functions nominally ascribed to CHWs, including by providing affordable, socially acceptable care that is close to the home, and liaising with the formal health system via referrals.
Traditional healers also treat many illnesses not recognised by the formal health system.
What do the new findings imply?
Traditional healers may be acting as de facto CHWs in many settings.
Policymakers should engage with and consider this cadre of health workers when planning child health services.
Introduction
In the worldwide effort to achieve universal health coverage (UHC), community health workers (CHW) play a key role in the provision of health services due to their close proximity to end users, socially adapted service delivery and engagement with families and communities.1 2 CHWs’ contributions to reaching global and national health goals have been recognised since the 1978 Alma-Ata Declaration, which was strongly influenced by China’s ‘barefoot doctors’ and similar programmes and policies.3 More recently, successful models in Brazil, Ethiopia, Iran, Malawi, Rwanda and elsewhere have provided further impetus to promote CHWs and conceptualise them at the centre of a ‘full-fledged sub-system’ of primary healthcare called the ‘community health system.’4 Yet the nature of health action at community level remains poorly understood, particularly as this extends beyond care seeking from formalised cadres, which represents only one dimension of families’ experience of healthcare and health seeking. This knowledge gap persists despite increasing calls for a ‘people-centered’ approach to ensure health systems provide equitable access, high quality of care, patient responsiveness and participation, and efficiency and resilience in service delivery, as in the 2016 World Health Assembly ‘Framework on integrated people-centered health services.’5
Globally, traditional and complementary medicines are practised in almost every country, and there are indications that a large proportion of care seeking worldwide includes treatment pathways involving traditional healers or other alternative practitioners.6 7 In Africa, studies suggest that majorities of the population depend on healers for everyday healthcare.6 We define traditional healers as people using indigenous knowledge and practices to prevent, diagnose and treat illness. Traditional healers are part of a larger category of informal providers, which also includes drug vendors and biomedical practitioners (such as CHWs) dispensing care beyond their level of professional certification.8 In rural areas, the number of traditional healers is much higher than the number of doctors and nurses, estimated in Africa to be 1:500 traditional healers per population versus 1:40 000 for medical doctors.6 9 In the public health literature, the traditional medical sector is largely framed as a problem for health systems, usually as a source of substandard care or delays in care seeking.10 Few studies examining the roles of CHWs in their communities specifically include traditional healers as part of their analysis, or compare cadres along dimensions of quality of care, dignity and/or respect, cultural competency and social or community cohesion. Yet traditional healers would seemingly fall under standard definitions of CHWs as ‘any health worker carrying out functions related to health care delivery; trained in some way in the context of the intervention, and having no formal professional or paraprofessional certificate or degree in tertiary education.’11
Integrated Community Case Management (iCCM) is an equity-oriented strategy endorsed by the WHO and Unicef to bring care for childhood illness closer to the community, using trained CHWs to classify and treat common illnesses, namely malaria, diarrhoea, pneumonia and malnutrition.12 13 iCCM has been implemented in over 50 countries, notably in sub-Saharan Africa, where policymakers have seen it as a solution to the lack of reach of the formal health system.14 However, lack of demand from the community and low utilisation of services have limited impact and cost-effectiveness of iCCM programmes, possibly due to insufficient community engagement.15 16
In the Democratic Republic of the Congo (DRC), where the population suffers from high rates of child illness and under-five child mortality (104 deaths per 1000 live births), as well as high rates of child malnutrition (43% of children under 5 years suffer from stunting), only 35% of the Congolese population lives within 5 km of a health facility.17 Recent efforts to expand iCCM coverage have included integration of nutrition counselling alongside screening and treatment of acute malnutrition into services provided by CHWs. A recent study aimed to provide guidance to strengthen nutrition counselling and prevention and treatment of malnutrition in the context of iCCM, as well as to understand community perspectives on child health and nutrition.18 The objective of this article is to provide further analysis of the qualitative data from this study to elucidate local understandings of child illness, determine families’ care-seeking behaviours in case of child illness and provide a descriptive analysis of the role of traditional healers and the community health ecosystem from the perspective of community members in the DRC’s north-central Tshopo Province.
Methods
This mixed methods study was conducted in four health zones in DRC’s Tshopo Province (Bengamisa, Ubundu, Yakusu and Yaleko) chosen to be representative of the regional geography and population’s sociodemographic characteristics, including religion, ethnicity, culture and geography, all of which can influence child health and nutrition practices. The study team received permission from local government authorities in Kisangani and village chiefs in study communities. Sensitisation activities were organised 2 days prior to data collection to inform local authorities and permit community members to name local guides, who worked with study coordinators to establish a list of potential interviewees.
Data collection was carried out from January to March 2017. We conducted in-depth interviews with mothers (n=48), fathers (n=21) and grandmothers (n=20) of children under 5 years of age to determine behaviours and perceptions around child feeding, illness and care seeking. Most community members were farmers with primary or occasionally secondary education. Additional interviews were performed with facility-based healthcare providers (n=18) and traditional healers (n=20), alongside focus group discussions (FGD) with CHWs (n=8 FGDs, n=56 participants). The sample sizes allowed for saturation to be reached to adequately capture the range of cultural beliefs and perceptions on nutrition and child health-seeking practices across the study sites. Interviews were conducted in French, Swahili or Lingala. Interviews with community members took place in a private space in or near the home; interviews with healthcare providers usually took place at a health centre. For all study participants, interview topics included knowledge and practices around care for sick or malnourished children under 5, and nutrition/illness counselling and treatment provided/received. Verbal informed consent was obtained from all participants, who were also provided with a copy of the consent form. For participants aged 18 years and below, additional parental assent is not required in the DRC; women are considered ‘adults’ by age 15 if they are currently the parent of a child.
Data were analysed iteratively and collaboratively between local and remotely based members of the research team, both virtually and via in-person workshops. Interviews were translated into French and transcribed verbatim; words with no agreed French translation were retained in the original language and checked with data collectors for definitions. Preliminary analyses of interviews and FGDs identified dominant themes to develop a coding structure, using thematic content analysis with elements of grounded theory, namely the constant comparative method and inductive theoretical analysis.10 The final codebook included 35 codes grouped around the following categories: community perceptions of child health, nutrition and illness; care-seeking and child feeding behaviours; and roles in provision of services for child health and nutrition. Thematic analysis of transcripts was done using NVivo V.1119 to apply codes and compare across categories to explore respondents’ knowledge, perceptions and practices about child health; as well as roles of different actors in care seeking and care provision. Preliminary findings were discussed in stakeholder workshops in Kinshasa and Kisangani in November and December 2017.
Patient and public involvement
This research aimed to understand the provision of care for childhood illness from the perspective of families and communities. Patients (children under 5) were not involved, however their families and communities gave permission for the research and helped establish the list of interviewees. Findings are currently being used to improve child health services in these communities.
Results
In Tshopo Province, the main health workers present at community level are CHWs (relais communautaires in French) and traditional healers. Relais communautaires are volunteers from a village or street who facilitate the connection between community members and the health system. There are two types of relais: relais promotionnels, who provide counselling for child illness, and relais sites who classify and treat child illness. Traditional healers are the other main cadre present within the community. These are community members who receive training through an apprenticeship or are taught through family lineage to offer botanical, spiritual and physical therapies, often while holding parallel roles such as farmer or pastor at the local church. Sick children in Tshopo Province were most likely to be treated with home care first (using either herbal medicines or Western biomedicines bought from vendors). If the illness persisted, parents consulted traditional healers or more rarely CHWs to diagnose the illness, give appropriate care or provide referral to the formal health system (both healers and CHWs referred sick children to health centres). Major differences were not observed across sites in terms of recourse to traditional or modern medicine or the types of treatments dispensed.
Child illnesses belong to one of two spheres: traditional/local or modern/biomedical
According to families interviewed in this study, child illnesses could have a variety of natural, spiritual or social causes; however, all illnesses fell into one of two categories: traditional/local or modern/biomedical. Modern or biomedical illnesses, frequently referred to as ‘white man’s diseases,’ were defined as those requiring care at the health centre or using biomedicine, including tablets and medicines purchased from shops and pharmacies. Traditional illnesses required treatment with traditional medicine (see table 1 for a list of local illnesses most often mentioned by respondents). Both types of illnesses could have organic and/or spiritual aetiologies. A full description of the reported symptoms, associated illnesses, and traditional and biomedical treatments reported by participants has been published elsewhere.18
Selected local illnesses mentioned by participants
Children’s symptoms, such as cough, could often be assimilated to conditions belonging to either category, such as pneumonia or Fota itoko (a febrile syndrome, usually attributed to the breastfeeding mother’s consumption of inappropriate foods). Families commonly mentioned local illnesses around breastfeeding including Fota itoko; Kunde, a disease of the mother’s genitals and breasts transmissible to the child during breastfeeding; and Sanga, a condition when a breastfeeding mother becomes pregnant and the breastfed infant becomes malnourished, has diarrhoea or is not able to walk until the mother gives birth. Other local illnesses were characterised by respiratory troubles in young children, including Kafeke, which presents as respiratory difficulties associated with cough and fever, and ‘chest disease’ (Maladie de la poitrine), compression in the child’s chest with localised swelling, causing a failure to gain weight. Another local illness of note is Lonyama, which leads to convulsions and loss of consciousness.
Families evoked biomedical or ‘white man’s’ diseases far less commonly. Pneumonia, for example, was spontaneously mentioned by only one mother. A majority of mothers, fathers and grandmothers did mention malaria, usually when prompted or when describing their child’s diagnosis at the health centre. However, families’ understanding of this illness was often incomplete or did not overlap with its biomedical description, as with a mother of five from Ubundu who said her daughter had malaria at birth, or a father of four from Yaleko who said:
We don’t know the difference between malaria and fever. If we notice the child is sick, we say we’ll use our traditional products.
In addition, families sometimes assimilated local illnesses to modern/biomedical ones, saying the same disease could have different names:
Here we say Lonyama but at the hospital they say malaria. (Grandmother, Yaleko)
Some respondents said Fota itoko was their name for measles or malaria, but more often these were understood as separate diseases. Yet the signs and symptoms of modern and traditional illnesses can overlap, as with fast breathing, a sign of both pneumonia and Kafeke (named for a fish with fast-moving gills):
In this case [when the child has a cough and fast breathing], we recognise that the hospital isn’t competent to treat this kind of problem, so we turn directly to traditional medicine. (Father of one child, Bengamisa)
As explained by a different father, Kafeke must be treated using traditional means:
Find the head of the kafeke [fish], burn it, then take the traditional salt and mix with the powder from the burnt fish. You tattoo [scarify] the chest and apply this medicine. If it’s really this disease, after a few minutes the child will start to breathe well again. (Father of two children, Yaleko)
This assimilation of symptoms could have implications for the recognition of danger signs, including fast breathing (as above) and convulsions. In one episode witnessed by an interviewer at a health centre, a convulsing child was grabbed by her mother and raced to the pit latrines, whose smell was supposed to revive the child. This practice was also described by a CHW in one of the FGDs:
For Lonyama … that is, severe malarial convulsions … you take leaves to make a liquid then put drops in the child’s eyes … Then you take him to the toilet and put his face in the hole. When he breathes the toilet air, he revives, then after that they bring the child to the hospital. (CHW, Yakusu)
Care-seeking pathways for sick children pass through traditional healers, not CHWs
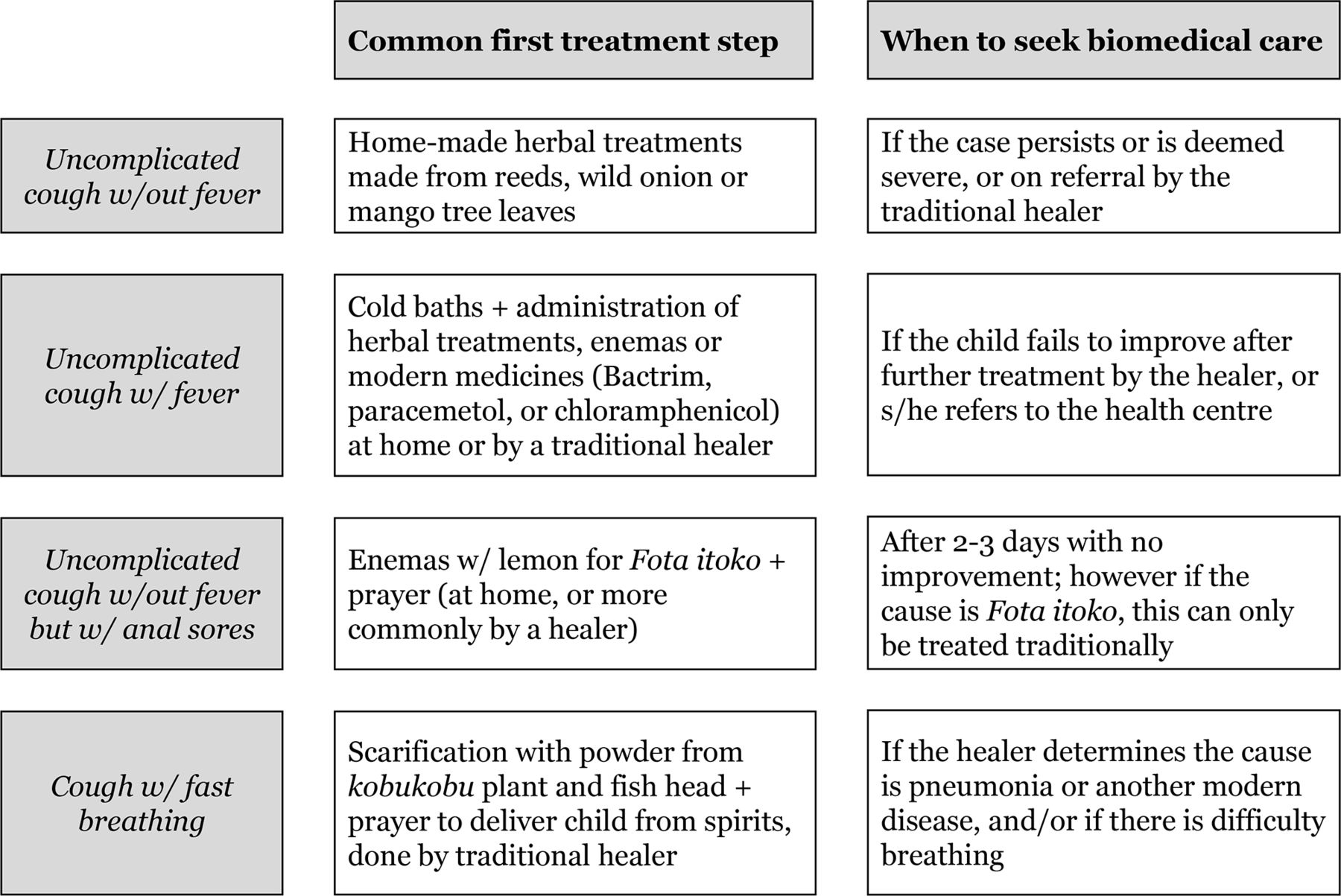
Across the four study sites, families seeking care for sick children usually first tried home care before consulting traditional healers and/or CHWs. When families first observed a child’s symptoms, for example, fever or cough, they applied home remedies such as cold baths, medicines made from wild plants, therapeutic enemas, or modern medicines such as paracetamol, Bactrim or chloramphenicol (both antibiotics) bought from a local vendor or shop (see figure 1 for treatment pathways for a child with cough).
{kind=link}
Treatment pathways for children with cough.
If the illness did not resolve or became more severe, families often had recourse to traditional healers, who diagnosed the illness and provided a variety of plant-based treatments (oral medicines, baths, enemas or pomades) and spiritual treatments (prayer, scarification). Several traditional healers said they sometimes provided modern medicines such as paracetamol and antimalarials to sick children. Children could also be prayed over in ceremonies to ‘chase the demons,’ either at home or at the church. Traditional healers made their own determination on whether they were competent to treat the illness in question. If not, they referred families to the formal health system.
Sometimes, families determined on their own that their child was suffering from a ‘white man’s’ disease:
If it’s a disease that has to do with traditional medicine, I go to the healer. If it’s a modern disease, I go to the closest medical facility … I know [which type of disease it is] by looking at the child. (Mother of a 1-month-old daughter, Bengamisa)
Relatively few families reported consulting CHWs, who were present in all four study sites. CHWs appeared ill equipped to care for sick children, however, since they did not receive adequate training, supervision or appropriate job aids from the Congolese health system (though they received some training and supplies to treat malaria from external partners). Nor were they reliably provided with the required medicines and supplies:
We don’t have medicines. We only advise them to go to the hospital. (CHW, Bengamisa)
Across interviews and FGDs, referral to the health centre appeared to be a major component (perhaps the major component) of CHWs’ activity. While families were aware of CHWs, they seldom recounted using their services. Furthermore, families also rarely appeared to receive the counselling meant to be the main activity of Relais promotionnels: few mothers said they had received home counselling from these workers, or even knew they were entitled to this service.
Families demonstrated a pronounced medical ‘syncretism’ in approaches to treating child illness, beginning with home treatments based in both traditional and modern medicine. As mentioned, families initially gave children both traditional and modern medicine at home, based on the type of symptom the child presented. When the child did not improve, or seemed to be severely ill, families sought care from traditional and biomedical sources one after the other or at the same time:
If the child is sick, prepare him so that we can go directly to the hospital, do the traditional treatment and then we’ll take him to the church. (Grandmother, Yakusu)
Community members recognised the legitimacy of all these forms of treatment, though they sometimes had differing opinions about which diseases traditional healers should treat and which required treatment with biomedicine. Each of the diseases included under iCCM (malaria, diarrhoea, pneumonia and malnutrition) were mentioned as treatable using either modern or traditional medicine. On the other hand, local illnesses were only treatable using traditional medicine.
The traditional medicine sphere encompasses biomedicine, but not vice versa
Services provided by traditional healers were more comprehensive than services provided by CHWs, as the traditional medicine sphere recognised and encompassed care for ‘modern’ diseases, but biomedicine did not recognise or treat traditional/local illnesses. Traditional medicine thus was a logical first step in care seeking, as the healer could diagnose all types of illnesses and identify whether possession by spirits or some ‘natural’ cause was at fault. All traditional healers recognised biomedical illnesses such as malaria, and many referred children to the health centre when they were unable to treat them themselves:
If it’s a disease that can be treated traditionally, I take care of it. If it’s modern, I say, ‘it’s not for me, it’s for modern medicine.’ (Traditional healer, Bengamisa)
Especially malaria and diarrhea, and those that are missing water or blood in their bodies—we send [those cases] to the hospital. (Traditional healer, Yakusu)
In many cases, traditional healers advised parents to pursue traditional and modern medicine at the same time:
If I see a malnourished [child], I tell [families] to follow all paths—the path of the hospital, and the traditional one. (Traditional healer, Bengamisa)
When you mix [traditional treatment] with modern, the child will get well. (Traditional healer, Bengamisa)
At least one of the healers interviewed said he was trained in both traditional and modern care:
They come because first of all, I’m a nurse, I give modern medical care … I didn’t finish my degree—I can’t know everything, given my limited studies. But they come for me to treat them. (Traditional healer, Yaleko)
When asked directly about modern diseases (specifically those included under iCCM), however, most traditional healers tended to say that ‘only the hospital’ (meaning any type of health facility) could help:
Interviewer: What is your advice for families … whose children have diarrhea?
Traditional healer, Yasuku: … It’s just to go to the hospital.
Interviewer: For malaria?
Traditional healer: It’s simply to go to the hospital.
Interviewer: For pneumonia?
Traditional healer: Simply to go see the doctor at the hospital.
Families find healers far more accessible than the formal health system
Compared with the formal health system, traditional healers were far more accessible to families due to proximity and lower cost. While care for children under 5 is nominally free in Tshopo Province, this was not found to be the case in the study sites. As one biomedical healthcare provider said, ‘Here we almost have free care [emphasis added]’; another said medical care ‘appears to be free but isn’t as free as indigenous products.’ Financial barriers often made it difficult or impossible for families to seek care at health centres, even when they would have wished it:
They ask for a lot of money at the hospital. (Mother of five children, Bengamisa)
Last month we didn’t have enough money in hand to go to the hospital. Since the money wasn’t there yet, we said first we’ll buy traditional medicines. (Father of four children, Yaleko)
In contrast, traditional healers were seen as much more affordable and flexible about payment. Families were usually not required to pay the traditional healer up front, and could sometimes pay in kind, a system which one traditional healer framed as more ethical than payment arrangements at facilities:
The [hospital worker] says ‘if I get no money then I’m staying home.’ But maybe I only have … a chicken or a duck, so I leave with that and I beg my brother [the hospital worker] to treat the child … and he says, ‘Since I’m not getting anything I’m staying at home.’ That’s how the sickness gets to weaken the child and he or she can die. (Traditional healer, Ubundu)
Families also had trouble seeking modern treatment due to lack of time, necessity of working in the fields and distance to medical facilities. Healthcare workers recognised that distance to the health facility was a common barrier:
The foremost difficulty [for families] is the distance between the village and the health center. (CHW, Bengamisa)
In contrast, traditional healers received patients and dispensed treatment at their own homes or the home of the sick child. While some healers said they received sick children at specific times (eg, after church), most said parents and families could come at any time:
Interviewer: If there’s a problem, are there set hours to come see you?
Traditional healer, Yaleko: I don’t set hours.
Being located in the community, traditional healers can also provide prolonged care as necessary:
If they get sick, they come stay here for the treatment. If you have demons, the treatment can take four days … (Traditional healer, Yaleko)
Lack of trust and collaboration between traditional and biomedical healers
CHWs and other biomedical providers usually spoke of traditional healers in the context of receiving children whose condition had deteriorated or not improved under their care. Most said they counselled parents to avoid traditional medicine:
Mama, papa … for your child to be in good health, no matter what type of disease, don’t bring your child for traditional medicine. Go over there [to the health center], it’s the doctor’s job. (CHW, Bengamisa)
In FGDs, CHWs sometimes expressed outright disdain for traditional medicine:
We don’t accord much consideration to traditional medicine. (CHW, Yaleko)
More commonly, CHWs seemed to understand that the traditional healer was less expensive and more accessible to the majority of families compared with care at facilities. Many seemed quite knowledgeable about specific traditional treatments and their modes of preparation and application. However, generally speaking, CHWs tended to advise families away from traditional medicine.
Traditional healers, on the other hand, did refer patients to the formal health system, as described above. However, they appeared wary of the state in other ways. For example, a certification process for traditional healers exists in the DRC yet was seen as onerous, inviting official scrutiny and requiring financial outlays. As one healer said:
We’re afraid of the agents of the state … I don’t have any state documents … They make us pay. Right now, I’m afraid of you [the interviewer] because you arrived today [to question me]. (Traditional healer, Bengamisa)
Traditional healers interviewed for this study appeared to be either unaware of this process or to prefer to avoid it. And while the latest national community health strategy (2019–2022) describes links between healers and community-level committees, such connections were not (yet) in evidence in the communities examined in this study.20
Discussion
In the communities of Tshopo Province examined in this study, families of sick children more frequently consulted traditional healers compared with CHWs or facility-based health workers as a first step in care seeking after home care. Families and communities distinguished between local and ‘white man’s’ diseases, as did traditional healers. However, representatives of the biomedical health system (CHWs and facility-based providers) only recognised, diagnosed and treated biomedical (‘white man’s’) diseases. As such, traditional healers’ understanding of child health and illness corresponded more closely to that of families, and they were able to provide a broader spectrum of care than biomedical providers. Healers were also more geographically and financially accessible to families compared with facility-based providers, though they commonly referred families to the formal health system if they felt they were unable to treat an illness. CHWs in Tshopo Province were well intentioned, however they could not provide free, accessible care and counselling, since they were inadequately trained, supplied and supported by the health system. Their main activity appeared to be referral to the health centre, which many said themselves that families tried to avoid for reasons of distance and cost. (Indeed care seeking from CHWs represents a small proportion of overall care seeking for childhood illness.21) Traditional healers thus emerged as the ‘real’ CHWs, in that they operated within the community, dealt with the full range of health complaints and referred families to the formal health system, fulfilling our working definition as ‘any health worker carrying out functions related to health care delivery; trained in some way in the context of the intervention, and having no formal professional or paraprofessional certificate or degree in tertiary education.’
Our findings accord with previous studies in the DRC, for example, in Ituri and North Kivu provinces, where spiritual and social aetiologies were described as being far more relevant to ordinary people’s understandings of illness than biomedical ones.22–24 Sabuni23 recounts the popular saying, ‘Congolese people do not die from microbes,’ and enumerates seven types of local illness aetiologies: natural; physical/environmental; social; breaking taboos; heredity; witchcraft, sorcery and ‘poisoning’; and punishment from ancestors.23 Few of these causes (even ‘natural’, ‘environmental’ and ‘hereditary’) correspond to biomedical notions of the causes of disease. Describing one illness whose cause has to do with witchcraft, the Congolese author writes, ‘It is very difficult to explain to a Cartesian mind.’ (Interestingly, Sabuni also mentions the ‘pit latrine’ cure, this time for abscesses, as a memory from his youth.) At the national level in the DRC, a traditional medicine programme has existed since 2001, however collaboration with the formal health sector has been stymied by lack of trust between traditional and biomedical healers, the unstructured nature of traditional healers’ profession and its infiltration by ‘charlatans,’ according to the 2016 strategy itself.25 Nonetheless, recent updates to the health sector framework, and a 2017 law on the organisation of public health in the DRC containing a specific article on traditional medicine, indicate that increasing attention is being given to the integration of traditional medicine into the formal health sector.
Our findings on the juxtaposition between ‘white man’s medicine’ and traditional medicine are also reminiscent of the distinction between doktor kot (‘book doctors’) and doktor sla (‘plant doctors’) reported in Meghalaya, north-east India.10 In India, alternative medicines, such as Ayurveda, are officially recognised by the state; their claims to legitimacy rest on specifically local, rather than universalist schema. However, practitioners still suffer from a ‘subaltern’ status, since their patients tend to be poorer rural people whose illnesses ‘were not only untreatable by biomedicine, but not even recognised by biomedicine.’10 Similarly, in Ethiopia, disempowered groups like women and rural people were more likely to consult traditional healers than biomedical practitioners, compared with men and urban people, when seeking care for epilepsy (an illness commonly interpreted as having spiritual or social causes).26
Globally, CHW programmes have recently undergone a resurgence, with CHWs lauded as an accessible, culturally competent cadre and a key component of the movement to achieve UHC.27 As a result, CHW programmes have been introduced or reinvigorated in many low/middle-income countries, with an emphasis on ‘community embeddedness,’ a tenet by which CHWs are trusted by community members, who feel a sense of ownership over the programme. According to a recent systematic review of reviews on CHWs,28 14 reviews highlighted aspects of community embeddedness as a factor of success resulting in higher CHW retention, motivation, performance, accountability and support, ultimately leading to higher acceptability and uptake of their work. CHWs trusted by their communities are also a more effective link to the health system and are better able to reach remote and underserved populations, although they can become implicated in tensions within the community and between the community and the health system. (Notably, in places where the government is not trusted by citizens, CHWs associated with Ministry of Health (MOH) may be less accepted by communities.)
In our study, traditional healers were more ‘embedded’ in their communities than were CHWs, and they were also arguably more effective along recognised dimensions of high-quality, accessible healthcare. While we are not aware of any studies showing traditional healers in the DRC provide evidence-based care with their clients having positive health outcomes, other contextual indicators of quality are present. Indeed, following one exploration of iCCM care in contexts of livelihood insecurity,29 our study would suggest that traditional healers in Tshopo Province rated highly in terms of availability (there are enough healers to serve the community, and they do not suffer from stock-outs), accessibility (healers are located near villagers’ homes), affordability (healers cost less and offer flexible payment schemes), adequacy (healers receive at times adapted to caregiver needs, and their services meet community expectations) and acceptability (healers provide care in congruence with community norms and understandings of disease, and treat the full spectrum of illnesses, while also providing psychospiritual support).
Yet recent discussions of ‘community health systems,’ defined as the ‘set of local actors, relationships, and processes engaged in producing, advocating for, and supporting health in communities and households outside of, but existing in relationship to, formal health structures,’ have rarely specifically invoked the role of traditional healers.4 This is despite the fact that traditional healers’ unique contribution is a therapeutic activity extending beyond the patient’s body to address their social and emotional equilibrium within the web of community relationships and values.30 31 Analyses of why traditional healers have remained peripheral to discussions of community health systems and CHWs must factor in MOH’s lack of ‘ownership’ over non-state actors, but also the role of colonialism in undermining the legitimacy of traditional health systems and the ‘ethnocentric and medicocentric tendencies of the Western hegemonic mentality’ that remain a feature of public health debates.6 All the more so, as the right of indigenous people to their systems of medicine is enshrined in the 2008 UN statement on the rights of indigenous peoples.32
An honest accounting of community health systems that incorporates the role of traditional healers is overdue. Traditional healers do not always help patients, can administer biomedical and possibly herbal drugs in harmful ways, create delays accessing other options and invoke gender-related blame and shame, among other harms. However, biomedical providers may also provide low-quality care (in terms of treatment efficacy, and along dimensions of respect and dignity),33 34 delay treatment (as in slow referrals in emergency obstetric cases)35 and, of course, are often expensive and geographically inaccessible. At the end of the day, traditional healers are meeting people where they live and providing socially appropriate care that aligns with community identity, strengthens social relationships, fosters hope and avoids bankrupting families. In the best case, they are also providing useful front-line care for certain illnesses and appropriate referral for others.
Our findings lend credence to previous work suggesting that further engagement with traditional healers could improve communities’ interface with the formal health system,36 and that training them on specific diseases could reduce delays in seeking biomedical care,31 for example, as part of a certification programme. As Krah et al9 note, the opportunities for integration are numerous, including a huge existing infrastructure (large number of healers, providing easy access to care, who do cross-referrals) and healers’ willingness to collaborate. One case study from Guatemala suggested that trusting interpersonal relationships between healers and biomedical staff are a key factor to successful partnerships,37 and indeed the issue of trust is frequently evoked and should be a topic of further research.6 9 37–39 Further research should also explore the risks of engaging with traditional healers, such as potential delays in care seeking and diversion of patients to ineffective treatment pathways.40 41 More fundamentally, policymakers at global and national levels must consider and weigh the benefits of engaging with and investing in traditional healers, alongside strengthening the formal health system to make it more accessible along the axes discussed above.
This study is based on a robust qualitative data set, with interviews with a wide range of community members, as well as different types of healers working in traditional and biomedicine, yet has some limitations. First, it is based on data that were collected for the purpose of strengthening the integration of nutrition interventions into iCCM, not for analysing the interface between traditional and biomedicine within communities. However, interview and FGD guides included questions about traditional medicine, care seeking and related topics, and we felt the data were rich enough to support this use of it. Second, our study deals with highly culturally specific issues using data collected in multiple languages; thus we worked in close collaboration with DRC-based data collectors and cross-checked definitions of illnesses and other untranslatable terms. Third, study participants may have sought to dissimulate their use of traditional medicine or reflect positively on the DRC health system (social desirability bias). We addressed this by triangulating between different types of respondents and checking with data collectors about the types of responses likely to be deemed favourable. Finally, our study would have benefit from more rigorous investigations of patients’ treatment pathways between traditional and modern medicine. Further studies should explore the interface between these two systems from the patient’s perspective.
Abstract translation
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.Acknowledgments
We gratefully acknowledge the participation of communities in Tshopo in this study, as well as the Bukavu-based research team who contributed strongly to preliminary analysis of findings. We also thank Shannon McMahon for her contributions to conceptualising an early version of this manuscript, and Malia Boggs and Nefra Faltas for their comments on a later draft.
References
Footnotes
Handling editor Seye Abimbola
Contributors JAK and MP designed and oversaw the initial study, with the assistance of JA and EM in the DRC. Additional data analysis was performed by LG with SLD. The manuscript was conceived and written by SLD with SS, with additional inputs from KS, JA and EM. All authors participated in revising the manuscript and approved the final version.
Funding This article is made possible by the generous support of the American people through the US Agency for International Development (USAID) under the terms of the Cooperative Agreement AID-OAA-A-14-00028.
Disclaimer The contents are the responsibility of the Maternal and Child Survival Program and the authors and do not necessarily reflect the views of USAID or the US Government.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Approval for this study was granted by the Institutional Review Boards at John Snow (IRB No 16-045) and the Kinshasa School of Public Health (DRC) (ESP/CE/001/2017).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No data are available.