Article Text

Abstract
Introduction The rapid ageing of populations around the world is accompanied by increasing prevalence of multimorbidity. This study is one of the first to present the prevalence of multimorbidity that includes HIV in the complex epidemiological setting of South Africa, thus filling a gap in the multimorbidity literature that is dominated by studies in high-income or low-HIV prevalence settings.
Methods Out of the full sample of 5059 people aged 40+, we analysed cross-sectional data on 10 conditions from 3889 people enrolled in the Health and Ageing in Africa: A longitudinal study of an INDEPTH Community in South Africa (HAALSI) Programme. Two definitions of multimorbidity were applied: the presence of more than one condition and the presence of conditions from more than one of the following categories: cardiometabolic conditions, mental disorders, HIV and anaemia. We conducted descriptive and regression analyses to assess the relationship between prevalence of multimorbidity and sociodemographic factors. We examined the frequencies of the most prevalent combinations of conditions and assessed relationships between multimorbidity and physical and psychological functioning.
Results 69.4 per cent (95% CI 68.0 to 70.9) of the respondents had at least two conditions and 53.9% (52.4–55.5) of the sample had at least two categories of conditions. The most common condition groups and multimorbid profiles were combinations of cardiometabolic conditions, cardiometabolic conditions and depression, HIV and anaemia and combinations of mental disorders. The commonly observed positive relationships between multimorbidity and age and decreasing wealth were not observed in this population, namelydue to different epidemiological profiles in the subgroups, with higher prevalence of HIV and anaemia in the poorer and younger groups, and higher prevalence of cardiometabolic conditions in the richer and older groups. Both physical functioning and well-being negatively associated with multimorbidity.
Discussion More coordinated, long-term integrated care management across multiple chronic conditions should be provided in rural South Africa.
- ageing
- multimorbidity
- south africa
- HIV
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
To date, multimorbidity has been studied mostly in high-income countries, with a small number of studies considering non-high-income countries and very few describing multimorbidity in sub-Saharan Africa and regions with high HIV prevalence.
Globally, there is increasing prevalence of multimorbidity among older adults. Compared with persons with a single condition, previous studies have found that multimorbidity is associated with higher mortality rates, health expenditures and frequency of service utilisation, lower self-reported health, physical functioning and well-being.
What are the new findings?
We estimate high prevalence of multimorbidity in this rural South African population. More specifically, we found high prevalence of single and combination of cardiometabolic conditions, even among the poorest households.
This older study population also had a high prevalence of HIV, many of whom are experiencing multimorbidity.
Contrary to existing literature, we did not see large positive relationships between the number of conditions and age and wealth. Certain conditions occur more in the relatively younger ages (ages 40–59), such as HIV, and others more in relatively older age groups (ages 60 and above), such as diabetes and angina.
What do the new findings imply?
There needs to be higher awareness of chronic multimorbidity in rural South Africa, and more coordinated, long-term integrated care management across multiple chronic conditions, as well as attention to HIV in older populations should be provided.
Data on the types of combinations and their frequencies could inform multimorbidity-related treatment guidelines on how care is designed and delivered. Synergies may be generated when certain treatments are bundled together to facilitate better quality of care, reduce the number of visits required and the burden to manage multiple conditions for patients.
Introduction
The ageing of populations has given rise to greater focus on chronic conditions.1 Health systems are commonly designed to address the burden of specific conditions, with less attention given to the impact of multimorbidity—commonly defined as two or more clinical conditions.2 Compared with persons with a single condition, prior studies have found that multimorbidity is associated with higher mortality rates,3 health expenditures and frequency of service utilisation,4–7 use of secondary care compared with primary care,8 9 hospitalisation rates,3 4 7 as well as lower self-reported health,10 physical functioning and well-being.11–13
Most research on multimorbidity to date has focused on high-income countries,12 14 with a small number of studies considering non-high-income countries6 8 15 and very few describing multimorbidity in sub-Saharan Africa and regions with high HIV prevalence. South Africa is already experiencing high prevalence of both cardiometabolic conditions and HIV infection together with the ageing of the population, and it is expected that an increasingly complex profile of multimorbidity will have a pronounced impact on individuals the health system in the near future.16 17 This study aims to enhance the evidence base on multimorbidity by developing a comprehensive portrait of the epidemiology of multimorbidity in a rural South African community. To our knowledge, this is one of the few studies considering multimorbidity in an older sub-Saharan African population with a high HIV prevalence.
Methods
Study design and participants
This study is a cross-sectional analysis of the population-based survey conducted in the Health and Ageing in Africa: a longitudinal study of an INDEPTH Community in South Africa (HAALSI) Programme, at the MRC/Wits Agincourt Health and Demographic Surveillance System site in the Bushbuckridge subdistrict, Mpumalanga Province in South Africa.18 19 Based on predetermined criteria, the study enrolled 5059 randomly selected participants aged 40+, with household-based interviews completed between November 2014 and November 2015.18 The primary survey instrument queried the demographic, health and economic conditions of individual participants. Dried-blood spots (DBS) were collected to test for haemoglobin A1c, HIV antibody and viral load. Tests for cholesterol (Cardiocheck PA Silver version), haemoglobin (Hemocue HB 201 Analyzer) and glucose (Caresense N Monitor) were measured using point of care machines. Blood pressure and anthropometric measurements were also obtained. More details on data collection are described elsewhere.18
Patient and public involvement
MRC/Wits Agincourt Research Unit has been working with the communities of the 32 villages of the study site for many years with a close interaction with the population and their political and traditional representatives. All studies, including HAALSI, were discussed with the Community Advisory Group (CAG) with representatives of all villages before implementation. In this specific study, the study investigators met with the CAG in different occasions to find out what the main issues of adult health were worrying the community and whether the objectives of the study were responding to those worries. The study was based on existing knowledge of health problems of the older population in this community and the discussions with the CAG served as an input to the design of the study.
The recruitment of participants was done after informing the communities (a meeting in each village) about the study. The MRC/Wits Agincourt Research Unit has a Health and Demographic Surveillance System in place which is used as a demographic platform from where to sample for research studies and HAALSI was done in the same manner. Finally, after HAALSI was completed, the main results were communicated back to the community in 2018 with a series of meetings in the communities and with meetings with the local authorities represented in the Community Development Forums.
Selection of conditions and definitions of multimorbidity
The selection of the conditions for this study was driven by the need to be harmonised with the sister studies, such as the Health and Retirement Study in the USA,18 study critical features of HIV/AIDS infection, cardiometabolic disorders and other common diseases in the study area. We selected 10 chronic conditions that were defined based on clear clinical criteria described in box 1, including cardiometabolic conditions (hypertension, dyslipidaemia, diabetes, angina), HIV, mental disorders (depression, post-traumatic stress disorder, alcohol dependence), anaemia and chronic bronchitis. Online supplementary appendix S1 provides further details of definitions of the conditions. We excluded participants who did not have sufficient information to identify their health status for all 10 selected conditions.
Supplemental material
Definitions of the ten chronic conditions
Hypertension was defined as a mean systolic blood pressure of at least 140 mm Hg, mean diastolic blood pressure of at least 90 mm Hg or self-report of current treatment. (While these conditions are often considered as risk factors for cardiovascular diseases, in this study, we take a broader approach and include all conditions that cause morbidity.)
Dyslipidaemia was defined as having elevated total cholesterol (≥6.21 mmol/L), low high-density lipoprotein (1.19 mmol/L), elevated low-density lipoprotein (>4.1 mmol/L), elevated triglycerides (>2.25 mmol/L) or self-report of ever being diagnosed with high cholesterol.1
Diabetes was defined as having glucose ≥126 mg/dL in fasting group (defined as >8 hours), glucose ≥200 mg/dL in non-fasting samples or self-report of current treatment.1
Angina was determined using the Rose Chest Pain Questionnaire.42
HIV status was ascertained either from the collected dried blood spots that showed HIV infection (confirmatory HIV ELISA) or exposure to antiretroviral treatment or self-report of HIV-positive disease status.
Depression was defined based on the Centre for Epidemiological Studies—Depression Scale eight-item questionnaire, using a cut-off of three or more symptoms.43
Post-traumatic stress disorder was defined as having a score of four or more on a seven-symptom screening scale developed by Breslau and colleagues.44
Alcohol dependence was defined using the CAGE questionnaire.45
Anaemia was determined by assessing measured haemoglobin against the recommended cutoffs from the South African National Health and Nutrition Examination Survey.46
Chronic bronchitis was defined based on whether the individual self-reported a usual cough with phlegm every day for at least 3 months per year for at least two successive years.47
Two definitions of multimorbidity were applied: the presence of more than one condition2 and the presence of more than one category of conditions. For the latter, based on conditions with similar pathophysiological risk profile or management plans, we identified four groups of conditions: cardiometabolic conditions, mental disorders, HIV and anaemia.20 This latter definition considers the fact that comorbidities within categories are likely to have different determinants and consequences than comorbidities across categories. To illustrate, consider two patients, one with hypertension and dyslipidaemia and another with hypertension and HIV. Under the first definition, both will be considered having multimorbidity with the same number of conditions, while under the second definition, only the latter will be considered multimorbid. In addition, people with HIV are more likely to also have anaemia.21 We therefore explored the patterns of multimorbidity by excluding anaemia from the definition of multimorbidity and presented the results in the online supplementary appendix S7. Chronic bronchitis was not included in the second definition because of its low prevalence and lack of good fit into the broader clinical categories.
Measures of physical functioning and well-being
Primary measures of functioning included activities of daily living (ADL), positive and negative experience scores and self-rated health. ADL was measured using five questions around daily self-care activities, including difficulty in walking, eating, bathing, getting in/out of bed and using the toilet. Well-being was measured using the positive and negative experience scores calculated using the Gallup World Poll instrument, a commonly applied instrument to assess well-being.22–24 Finally, a five-point response scale was used (very good, good, moderate, bad and very bad) to construct an ordinal variable for self-rated health with the question, ‘In general, how would you rate your health today?’.
Statistical analyses
We performed descriptive analyses of multimorbidity prevalence by key sociodemographic covariates. Multivariable regression analyses were used to assess the relationship between prevalence of multimorbidity or number of conditions/categories of conditions and sociodemographic factors. Covariates included were age, sex, education, country of origin, marital status, household size, employment status and wealth, measured in quintiles based on household asset ownership and created using standard methods.25
We identified unique, mutually exclusive profiles and explored the frequency of patterns of conditions. We estimated the proportions of multimorbidity by sex and age group, and by HIV status and age group. Finally, the relationships between the number of conditions and the number of categories and various functioning variables were assessed using quasi-Poisson and zero-inflated Poisson regressions. More details on the statistical models can be found in the online supplementary appendix S2.
Results
Prevalence, distribution and patterns of multimorbidity
Out of the full sample of 5 059, 3889 (76.9%) had complete data on the 10 conditions of interest and were included in these analyses, 23.1% were excluded, most commonly due to missing measurements for HIV and dyslipidaemia (online supplementary appendix S3). 9.4% were excluded due to missing DBS results for HIV, and it is likely that we are underestimating HIV prevalence due to those with HIV refusing to be tested. For dyslipidaemia, selection bias is of lower concern since missingness was primary due to issues with the measurement tool and unrelated to individual characteristics. The online supplementary appendix S3 provides detailed description of the selection process of the analytic sample and the comparison between included and excluded study samples.
Of the study sample, 54.8% were female, average age was 61.7, majority of whom did not have formal education, are currently married, living in a 3–6 person household and not employed (table 1). Using the first definition of multimorbidity (presence of more than one condition), 69.4% (95% CI 68.0 to 70.9) of the respondents had at least two conditions and 37.7% (36.2–39.2) had at least three conditions. Using the second definition of multimorbidity (the presence of more than one category of conditions), 53.9% (52.4–55.5) of the sample had at least two categories and 17.5% (16.3–18.7) had at least three categories.
Number of conditions and categories of conditions by sociodemographic characteristics
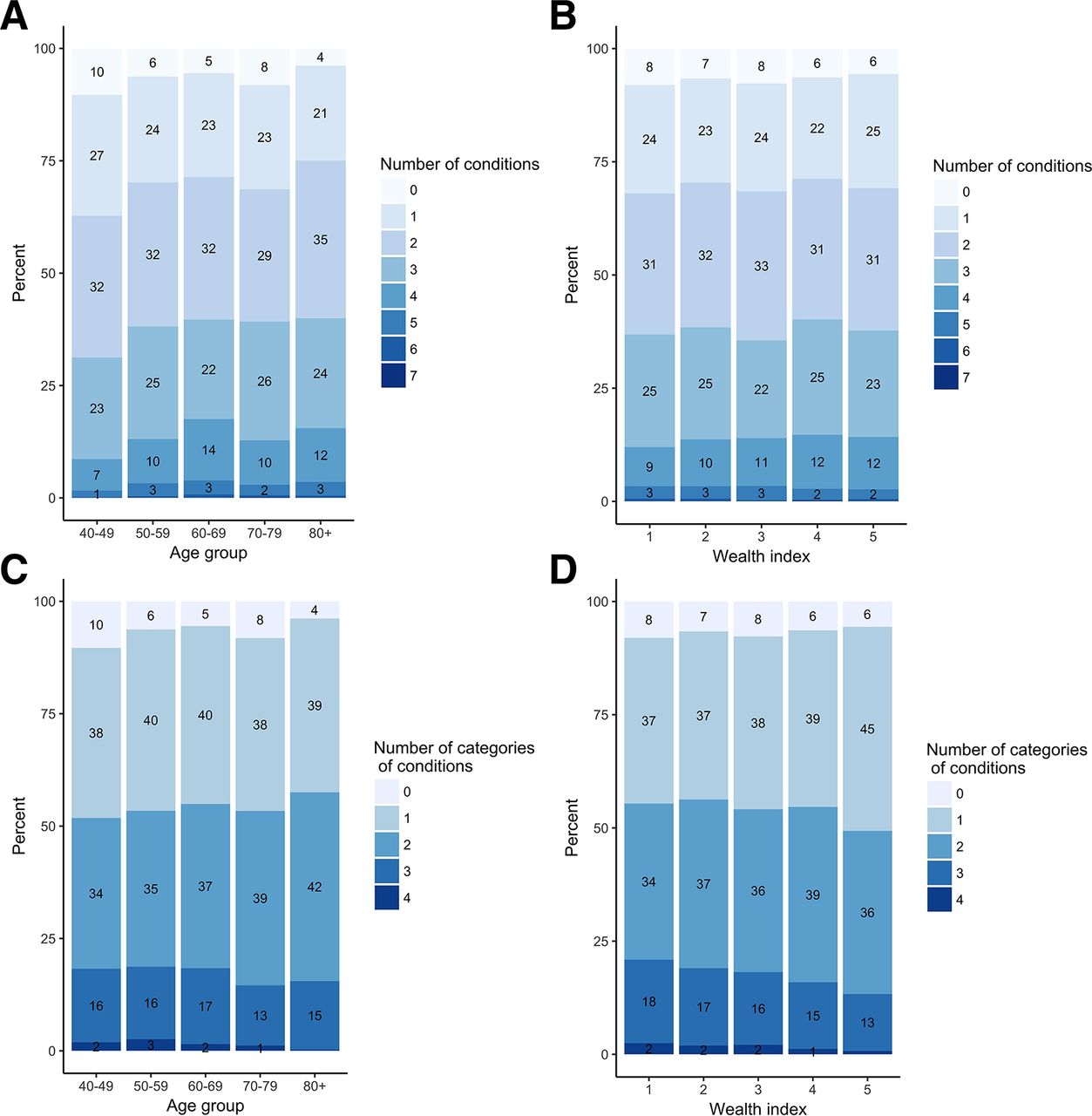
Looking at the relationship between age and the number of conditions, we found statistically higher proportion of people with two or more conditions with increasing age up to age 69, compared with the age group just below it (figure 1A, online supplementary appendix S8). However, when looking at the proportion of people with three or more conditions, we found a relatively weak relationship among people above age 50. When focusing on age and people with four or more conditions, we observed an inverse U-shape, with the highest percentage with four or more conditions occurring at ages 60–69 (17.5%), significantly higher than any other age group except ages 80 and above. Similarly, we observe a relatively weak relationship between the number of conditions and wealth index: the proportions of people with multimorbidity do not significantly increase nor decrease with wealth (figure 1B, online supplementary appendix S8). While the wealthier groups suffered more from cardiometabolic conditions, the poorer groups had higher proportions of anaemia and HIV (online supplementary appendix S4). Only the two richest quintiles had significantly higher number of chronic conditions than the poorest quintile (online supplementary appendix S8). We further assessed the combinations of age and wealth and the relationship with multimorbidity in the online supplementary appendix S4, but the results do not change the descriptions above.

Distribution of number of chronic conditions and categories of condition by age group and wealth quintile. Distribution of numbers of conditions by age group (A and C). Distribution of numbers of conditions by wealth quintile (B and D).
When we applied the second definition of multimorbidity (number of categories of conditions), we observe similar trends but none were statistically significant. We found slightly higher proportion of people with two or more categories and lower proportions of people with three or more categories with higher age (figure 1C). On the other hand, we observed a negative (but non-significant) relationship with wealth, since the richer groups tended to have several cardiometabolic conditions that were considered to be one category (figure 1D).
The figure 2 shows the prevalence of pairwise comorbidities of the 10 conditions. The most common clusters of conditions were the combinations of different cardiometabolic conditions, cardiometabolic conditions and depression, HIV and anaemia and the combinations of different mental disorders. There were 212 mutually exclusive disease profiles (online supplementary appendix S5). The most common profile was having hypertension alone (11.7% of the full sample), followed by hypertension and dyslipidaemia (9.4%), no condition (6.9%) and hypertension and anaemia (6.4%). More than half of the population had multimorbidity, approximately 15.8% (14.7–17.0) of the population had three categories and 1.7% (1.3–2.1) had all four (online supplementary appendix S6).

Prevalence of chronic conditions and their co-occurrence probabilities. The size of the bubble reflects the relative magnitude of prevalence. AlcDep, alcohol dependence; PTSD, post-traumatic stress disorder.
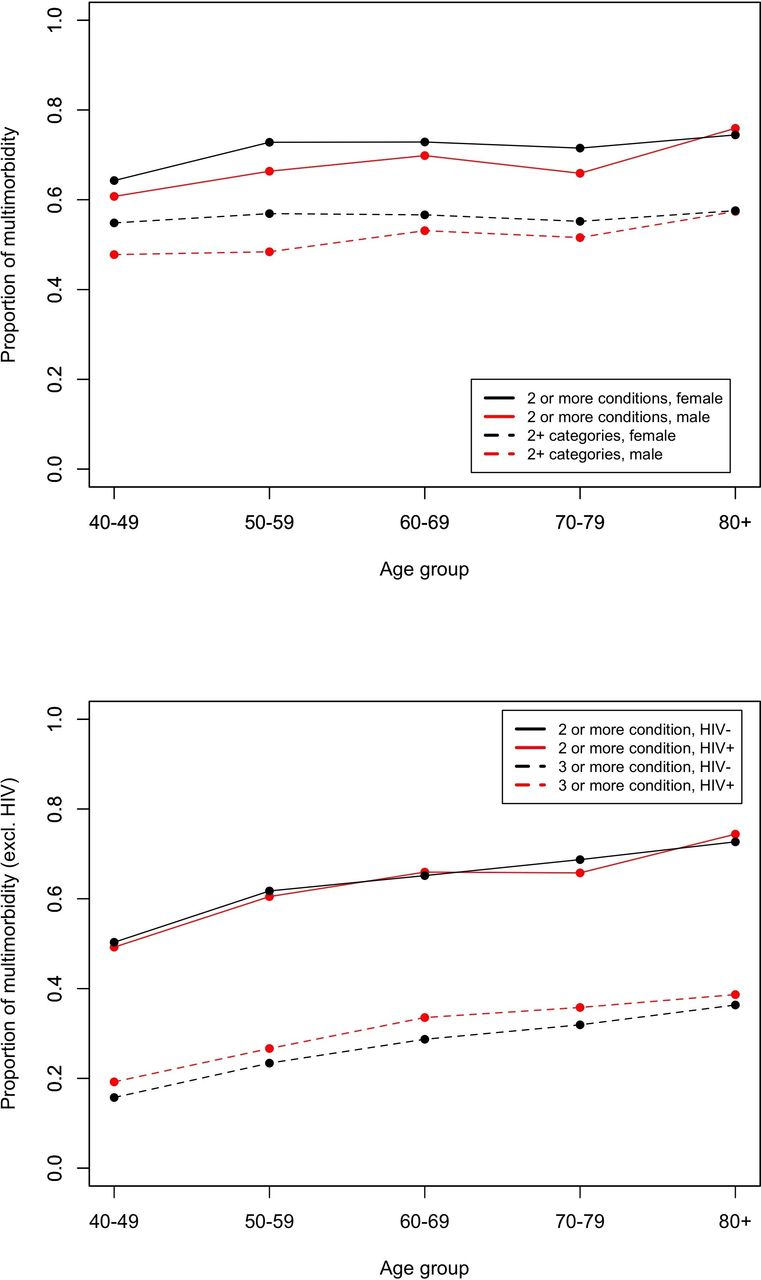
Comparing the proportion of multimorbidity across age, sex and HIV status (figure 3), females have significant higher number of chronic conditions. The gap between the sexes was wider when considering number of categories instead of conditions (figure 3A), with the gap narrowing with age. However, the differences between the two sexes under both definitions were not statistically significant. Comparing the prevalence for each condition, females had significantly higher prevalence of hypertension, depression and angina, whereas males had statistically higher prevalence of alcohol dependence (online supplementary appendix S4). We did not see differences in the probabilities of having multimorbidity between those with and without HIV under the first definition of multimorbidity (and excluding HIV) (figure 3B). When applying the second definition of multimorbidity (and excluding HIV), respondents with HIV had a higher proportion of multimorbidity for all age groups. The difference in the proportion of multimorbidity between people with and without HIV is the greatest, though not statistically significant, in the 60–69 age group, compared with the reference group. The same set of results in which anaemia is excluded from the definition of multimorbidity is presented in the online supplementary appendix S7.
{kind=link}
{kind=link}
{kind=link}
Proportion of people with multimorbidity, defined as having more than one condition or having more than one category of conditions, by age, sex and HIV status. (A) Proportion of people with multimorbidity, defined as having more than one condition or having more than one category of conditions, by age and sex. (B) Proportion of people with multimorbidity, defined as having more than one condition (excluding HIV) or having more than one category of conditions (excluding HIV), by age and HIV status.
Factors associated with multimorbidity
Age, marital status and wealth were positively associated with higher numbers of chronic conditions. In applying the first definition of multimorbidity as the outcome, age, marital status and wealth quintiles were positively associated with having multimorbidity, whereas a larger household size was negatively associated (online supplementary appendix S8). In contrast, under the second definition, only marital status was positively associated with having multimorbidity, while household size was negatively associated.
Relationship between multimorbidity and physical functioning and well-being
Both physical functioning and well-being declined with increasing numbers of conditions and categories (online supplementary appendix S9). As expected, the number of ADL limitations and negative experiences increased with the number of conditions/categories, whereas positive well-being score and self-reported health decreased. Having multimorbidity was associated with having more limitations in ADLs, negative experiences, fewer positive experiences and lower self-rated health.
Discussion
This study investigated the prevalence and patterns of multimorbidity, factors associated with multimorbidity and its association with physical functioning and well-being in an older rural South African population. We estimated high proportion of the study sample with multimorbidity in this rural population, under both definitions used in this study. In addition to high prevalence of cardiometabolic conditions, we found that close to one in four persons had HIV. Commonly found positive relationships between multimorbidity and age and wealth were not found in this study, whereas measures of physical functioning and well-being were negatively associated with multimorbidity.
Only a handful of recent multimorbidity studies have been conducted in sub-Saharan Africa, all of which analysed data from the first wave of the WHO’s Study on global AGEing and adult health.7 26 Our study has the advantage of including a broader range of conditions, such as HIV, anaemia and mental disorders, most of which were objectively measured, thus filling a gap in the multimorbidity literature that is dominated by studies in high-income or low-HIV prevalence settings. Second, we adopted two definitions of multimorbidity to account for potential synergies between similar conditions and additional complexity due to different needs and severity of conditions. Third, we used a population-based survey, unlike other studies that rely only on administrative records from health facilities, which may be vulnerable to selection bias. Finally, this study focused only on people aged 40+ and analysed the relationship between age and multimorbidity using 10-year age intervals. Compared with most studies that included the younger population or applied a wider age range (eg, age groups of 18–49, 50–64 and 65 and above), our analysis in 10-year age increments allowed us to observe unique patterns between age and multimorbidity that were not identified elsewhere.7 15
This study has several key findings. First, the prevalence of multimorbidity in this population was high, consistent with existing literature.6 8 12 14 15 27 We found high prevalence of single and combination of cardiometabolic conditions, even among the poorest quintiles (online supplementary appendix S4).28 Data on the types of combinations and their frequencies could inform multimorbidity-related treatment guidelines on how care is designed and delivered. Synergies may be generated when certain treatments are bundled together to facilitate better quality of care, reduce the number of visits required and the burden to manage multiple conditions for patients.29–31
Second, this population had a high prevalence of HIV, at 23%. A study from a similar setting found significant increases in adult life expectancy due to the scale up of antiretroviral treatment (ART) in recent years,32 which may explain high prevalence even among this older population. Differences in HIV prevalence between age groups (online supplementary appendix S4) may reflect the differences in sexual behaviour and changes in public health strategies across time. With increasing survivorship, we expect to continue to see high prevalence of HIV in our study population over the coming years with an ageing population on ART. In this study, we also found that people living with HIV have high prevalence of multimorbidity. South Africa’s HIV prevention and treatment programmes have expanded rapidly over the years, yet, currently the majority of prevention programmes are largely focused on younger adults with less complicated disease profiles.33 Our findings highlight the importance of providing integrated care, such as campaigns that combine communicable and non-communicable disease screenings into a community-level HIV testing drive that was successfully implemented in rural Uganda.34
Third, contrary to other studies,8 35 we do not see large positive relationships between the number of conditions and age and wealth. One reason is because other studies include much younger age groups (eg, adults aged 18–39 years). Certain conditions occur more in the relatively younger ages (ages 40–59), such as HIV, and others more in relatively older age groups (ages 60 and above), such as diabetes, and angina. Similarly, we observe higher prevalence of HIV in the poorest quintile, compared with higher prevalence of cardiometabolic conditions in the richest quintile. Thus, simply adding the number of conditions leads to a relatively weak relationship between the number of conditions and age and wealth. One possible explanation could be that older people with more conditions are less likely to survive, and hence cannot be observed. Similarly, in contrast to prior studies,36 37 we did not see differences in the probabilities of having multimorbidity between those with and without HIV under the first definition of multimorbidity, likely due to the inclusion of anaemia in the analysis, as these two conditions often co-occur. With regard to the relationship between multimorbidity and wealth, we find that simply adding the number of conditions masks the different epidemiological patterns that occur across wealth quintiles, with the richest quintiles facing more cardiometabolic conditions and the poorest quintiles having higher rates of HIV and anaemia. Finally, our findings are consistent with previous work showing that physical functioning and well-being decrease with multimorbidity.12 38
This study has several limitations. First, restricting to ages 40 years and older may have reduced variability, making it harder to detect associations between factors and outcomes. Second, all conditions were weighted equally in the first definition, by taking a simple count without considering the severity of each. We attempted to address this issue by categorising concordant conditions together. Third, the number and selection of conditions considered must have affected our results. We only included study participants with non-missing disease status of all 10 conditions, though estimated prevalence of HIV and dyslipidaemia, two of the most common missing data, are in the similar ranges as the population estimates of the broader region. Fourth, some conditions were diagnosed using biological criteria whereas some were based on self-reported symptoms and thus may result in an underestimation or overestimation of the population prevalence. For example, in the case of chronic bronchitis, we would expect higher prevalence if spirometry or pulmonary function tests were performed.39 Fifth, the study is cross-sectional in nature, and thus, we cannot prove any causal relationship nor can we explore the onset or timing of symptom manifestations. Finally, measures of physical functioning and well-being were self-reported, which may have introduced the potential for inaccuracies of over-reporting or under-reporting of performances. However, these measures are commonly applied in the literature, and subjective judgments of how people perceive functioning are also of value to our work.
In an ideal setting, multimorbidity would be managed by well-trained providers who would address all needs of the patient and maintain a long-term relationship to ensure coordination and care continuity. Clinical guidelines that stipulate which additional comorbidities providers should anticipate or concurrently managed would be readily available and integrated into routine provider training. However, this ideal scenario is often not present even in resource-rich health systems, let alone in a rural poor community. The Integrated Chronic Disease Management (ICDM) model was recently introduced in South Africa with the aim of ‘ensuring an integrated response of communicable and non-communicable chronic diseases’.40 41 It was also designed to reduce HIV-related stigma by using the same consultation rooms and being seen by the same providers for all. In the context of Agincourt, a person with any symptom or condition arrives at one of the local clinics and is greeted by nurse practitioners who is expected to address all patient needs, follow guidelines to address the chief complaint and diagnose and manage any additional comorbidities. However, real-life barriers, such as long waiting times, staff shortage and poor integration between vertical HIV programmes and general services, negatively affected the implementation of ICDM in Agincourt.41
Our study provides needed information for planning primary healthcare needs and chronic care health services that will increasingly have to treat individuals with multimorbidity. The findings indicate a strong need for coordinated, long-term integrated care management for those with multimorbidity and highlight the importance and urgency of ensuring successful implementation of the ICDM model.
References
Footnotes
Handling editor Seye Abimbola
Contributors FXGO, AW, LM, ST, and JAS contributed to the design of the HAALSI study and coordinated baseline data collection and data preparation. AYC and JAS conceived and designed the study. AYC conducted theanalysis and developed the initial draft of the manuscript. FXGO contributed to early conceptual and technical support in the study design and data interpretation phases. All authors substantively reviewed, revised, and approved the final manuscript.
Funding The HAALSI study, funded by the National Institute on AgingAgeing (P01 AG041710), is nested within the Agincourt Health and Demographic Surveillance System site, supported by the University of the Witwatersrand and Medical Research Council, South Africa, and the Wellcome Trust, UK (grants 058893/Z/99/A; 069683/Z/02/Z; 085477/Z/08/Z; 085477/B/08/Z). ANW is supported by the Fogarty International Centre (NIH) under Award Number K43TW010698. This paper describes the views of the authors and does not necessarily represent the official views of the National Institutes of Health.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study received ethical approvals from the University of the Witwatersrand Human Research Ethics Committee, the Mpumalanga Provincial Research and Ethics Committee, and the Harvard T.H. Chan School of Public Health Office of Human Research Administration.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data may be obtained from a third party and are not publicly available.