Article Text

Statistics from Altmetric.com
Summary box
One key recommendation of the Lancet Commission on High-Quality Health Systems in the Sustainable Development Goal Era published in September 2018 is the redesign of childbirth services.
The plea for the childbirth service redesign is underpinned by the assumption that the centralisation of childbirth services to hospitals will result in (1) more efficient delivery care, (2) more skillful maternity providers and (3) more timely emergency care interventions including blood transfusion and caesarean section.
We call for research to develop and test context-specific redesign strategies for improved childbirth care based on the two continuums of care: from pregnancy, through to childbirth and postnatal care, and from community to specialised referral care.
Strategies need to take into account specific aspects of access, safety and quality of care in the respective setting in order for safe and respectful childbirth care to reach all women.
Introduction
A strategy of childbirth in facilities close to home has been in place for almost two decades,1 but given numerous reports of low quality of care,2 3 the recent review of the strategy is timely.2 4 The Lancet Commission on High-Quality Health Systems in the Sustainable Development Goal Era suggests that childbirth services should be centralised to hospitals under the premise that larger volumes will result in (1) more efficient delivery care, (2) more skillful maternity providers and (3) more timely emergency care interventions including blood transfusion and caesarean section.
There is no doubt that the present strategy of childbirth care is not fulfilling expectations: maternal mortality is not reducing at the expected pace of 5% per year, but only 2.4% in low-income and middle-income countries5—except in a few settings such as Cambodia, where dedicated midwives offer childbirth care in health centres, and maternal mortality has reduced with an annual decline of 7.4% from 1020 (1990) to 161 (2015) deaths per 100 000.5 6 Neonatal mortality also remains high, at above 25 per 1000 live births in sub-Saharan Africa and Eastern and South-Eastern Asia.7
There are many good reasons for the proposed shift towards centralising childbirth care to hospital, and this is the most common model in high resource settings. Complications can arise suddenly, even after a normal pregnancy and an uncomplicated first stage of labour, so it is best to deliver in a facility where such complications can be managed. However, the low complication rate after normal pregnancy is an argument to offer childbirth care beyond the hospital walls, as, for example, in the Netherlands where neonatal mortality rates are no higher than in other European countries.8
We propose a debate, in the hope that the proposed shift is not misunderstood as a magic bullet, but rather a nuanced and adapted approach. Given the realities of poverty and systems constraints, strategies should be (1) based on evidence, (2) respect the needs of mothers, families and the community and (3) anchored in, and supportive of, the local health system: strategies need to be context specific.
The roots, the shapes and the pitfalls of the present system of childbirth care
It is important to first review the history of maternal health strategies and what the present model intended to fix. The first global childbirth strategy was born in the early 1990s and proposed a four-pillar approach of family planning, antenatal care, clean and safe (home) delivery for uncomplicated childbirth and hospital delivery in the case of complications.9 This strategy was revised in the late 1990s in view of high and stagnant maternal mortality rates, doubts about the effectiveness of care given by traditional birth attendants and new evidence based on historical review suggesting that proficient, trained midwives are of key importance.10 Many of the risk factors used to identify high-risk pregnancies had low predictive values for complications, such as maternal height to predict obstructed labour or high parity for haemorrhage.11 On the World Health Day in 1998, the new strategy was summarised with the slogan ‘every pregnancy faces risk’12 and the policy of childbirth care by a skilled attendant near to people’s homes was subsequently followed. This strategy has without doubt contributed to the recent large increases in facility delivery.13
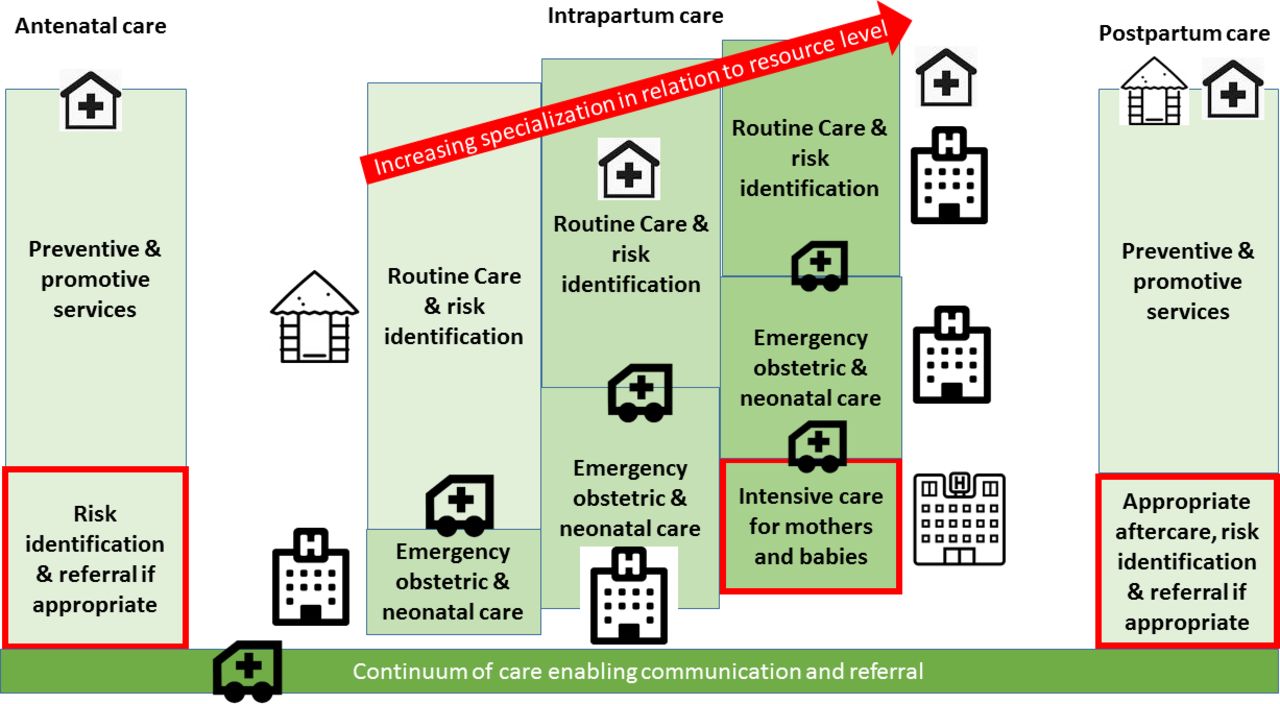
One side-effect of this policy shift was the neglect of the identification of high-risk pregnancies through antenatal care and referral to higher level care.14 The fact that some mothers and babies face substantially greater risks, as with twins, premature birth or previous caesarean section,15 is a central aspect of all childbirth care systems in high-income countries. In these settings, risk detection and referral is continuous throughout the antepartum and intrapartum period with access to highly specialised childbirth care, as well as neonatal intensive care, for situations where mothers have complications or risk factors such as such as multiple pregnancy, previous caesarean section or pre-eclampsia or eclampsia (figure 1). In low perinatal mortality settings, we see continuous developments to more specialised care, improved triaging to allow low-risk pregnancies to have safe midwifery-led care, backed by functioning emergency referral. This triaging and referral is largely absent in low-resource settings, and the lack of the identification of pregnancies which are at very high risk might be one reason for the slow decline in maternal and perinatal mortality.14 16
{kind=link}
Framework of maternal and newborn care.
Kruk and colleagues4 argue that women and families are ready to travel large distances for childbirth care in rural, low-income settings. The argument is supported by several studies reporting bypassing of primary facilities.17 18 We would like to add a note of caution as not all of these studies excluded women with complications in pregnancy and who were referred. Nevertheless our own study reported a promising trend of increased care seeking in hospitals in rural Southern Tanzania: uptake of hospital delivery increased from 29% in 2007 to 40% in 2013, for women with a birth in the year prior to the survey. Yet in 2013, rates of childbirth in hospitals were just 25% for those living over 25 km away.19 We believe that it is important to recognise that some women will face insurmountable barriers to overcome distance, particularly poor and multiparous women.20 Moreover, seasonal differences in accessibility of facilities also need to be taken into consideration.21 In Germany, it is suggested that a hospital offering childbirth care should be within 20 to 30 min travel time.22 In sub-Saharan Africa, about 90% of the population lives within 2 hours of travel to a hospital, the present benchmark, but only 50% within 30 min.23 If we are serious about leaving no one behind, major investments are needed, both to assist poor rural women to overcome the distance to hospitals and to build more hospitals to reduce travel time.
Another aspect which is not yet sufficiently integrated into the policy shift is how such a model will relate to the aim of integration along the continuum of care through pregnancy to childbirth and the first few months of life. The hospital-based models in high-income countries use very different systems; rarely do they, however, provide continuity of healthcare care spanning from antepartum, intrapartum to postnatal care with a single provider being a primary contact person. More innovation and research are needed to identify such continuity-of-care models and approaches that allow community participation as highlighted in the latest antenatal care guidelines of WHO.24 Traditional community health workers will rarely be linkable to hospitals which are far from home villages.
Cost effectiveness including both a societal and health systems perspective will need to be considered comparing hospital-based care to decentralised primary care-based or mixed systems. Hospital care is often not the cheapest as the availability of technology and equipment make the overuse of interventions more likely. Rates of caesarean sections are likely to rise, both necessary and unnecessary, further contributing to rising costs as well as mortality and morbidity.25 26 Midwifery-led childbirth care units as an annex to hospitals or closer to people’s homes but efficiently connected to hospitals could be a solution.27
We use a case study from the field to illustrate why several points along the continuum of care need improvement and that a radical shift will neither be the only solution nor will it alone result in better care (Box 1):
Case story
An 8-month pregnant woman had a high fever, headache, abdominal pain and was bleeding. Her mother and her husband took her to a dispensary. At the dispensary, the nurse told the family that the facility did not have medicine and equipment to help the patient and referred the mother to a health centre. At the health centre, the woman was checked by a nurse, who suspected the woman had a stillbirth. At this time, the nurse did not tell the mother or the family of the result of her assessment, instead she referred the patient to the district hospital. On the way, the woman continued bleeding and to complain about headache. When they reached the district hospital, the woman was assessed again and she was told that the baby had died and that her blood pressure was very high. At this point, the woman became unconscious and a doctor suggested that the patient needed a caesarean section. One day after the surgery, the woman died.
First, the case illustrates the road to death with several missed opportunities—a concept which is well known in the maternal health community. Asking colleagues what should have been done differently, the most common response at present is: ‘If the health centre had done a caesarean section, then the woman would have been saved’—mirroring the present advocacy work that health centres should provide comprehensive emergency obstetric care.2 Proponents of the policy shift towards hospital care would argue that if the woman had gone immediately to seek care in the district hospital she would have been saved.
While it is true that we do not know where the tipping point was, the case study suggests that high blood pressure was missed during antenatal care. Further, neither the mother, the family nor the nurse at the dispensary were aware that her conditions could only be handled at a hospital, and not at a health centre. Lastly, the mother needed to be stabilised and a caesarean section to deliver a dead baby is contraindicated, suggesting quality deficits in the hospital. As proposed by Kruk and colleagues, major improvements in knowledge and skills of maternity providers and the introduction of critical care are indispensable, regardless of which system is favoured.4
A proposed innovation and research agenda
We call for research to develop and test new context-specific strategies taking into account access, safety and quality of care in order for safe and respectful childbirth care to reach all women. Antenatal and postnatal care as well as the links between the different components is key for quality childbirth care. Screening, detecting and managing risks in pregnancy and childbirth must remain part of the strategy. The aim is here not to predict complication, but to prevent or prevent worsening of complications. This includes recommendation of the most appropriate place for childbirth taking individual risk factors and context-specific factors into consideration. Such a system will need to be supported by a greater attention to preservice training to allow sufficient numbers of high-quality health providers.
In sum, we call for context-specific redesign strategies for improved childbirth care based on the two continuums of care: from pregnancy, through to childbirth and postnatal care, and from community to specialised referral care. Comprehensiveness, balance and context should be the key points to consider.
References
Footnotes
Handling editor Seye Abimbola
Contributors CH and JS jointly developed the comment, the arguments and wrote the comment together.
Competing interests None declared.
Patient consent for publication Next of kin consent obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No additional data are available.