Article Text

Abstract
Introduction Making oral contraceptives (OC) available over the counter (OTC) could reduce barriers to use. To inform WHO guidelines on self-care interventions, we conducted a systematic review of OTC availability of OCs.
Methods We reviewed data on both effectiveness and values and preferences surrounding OTC availability of OCs. For the effectiveness review, peer-reviewed articles were included if they compared either full OTC availability or pharmacist-prescribing (behind-the-counter availability) to prescription-only availability of OCs and measured an outcome of interest. For the values and preferences review, we included peer-reviewed articles that presented primary data (qualitative or quantitative) examining people’s preferences regarding OTC access to OCs. We searched PubMed, CINAHL, LILACS and EMBASE through November 2018 and extracted data in duplicate.
Results The effectiveness review included four studies with 5197 total participants. Two studies from the 2000s compared women who obtained OCs OTC in Mexico to women who obtained OCs from providers in either Mexico or the USA. OTC users had higher OC continuation rates over 9 months of follow-up (adjusted HR: 1.58, 95 % CI 1.11 to 2.26). One study found OTC users were more likely to report at least one WHO category 3 contraindication (13.4% vs 8.6%, p=0.006), but not category 4 contraindications; the other study found no differences in contraindicated use. One study found lower side effects among OTC users and high patient satisfaction with both OTC and prescription access. Two cross-sectional studies from the 1970s in Colombia and Mexico found no major differences in OC continuation, but some indication of slightly higher side effects with OTC access. In 23 values and preference studies, women generally favoured OTC availability. Providers showed more modest support, with pharmacists expressing greater support than physicians. Support was generally higher for progestogen-only pills compared with combination OCs.
Conclusion A small evidence base suggests women who obtain OCs OTC may have higher continuation rates and limited contraindicated use. Patients and providers generally support OTC availability. OTC availability may increase access to this effective contraceptive option and reduce unintended pregnancies.
Systematic review (PROSPERO) registration number CRD42019119406.
- systematic review
- oral contraceptives
- over-the-counter
- pharmacy access
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Making oral contraceptives (OC) available over the counter (OTC) may increase access.
What are the new findings?
A systematic review of the literature identified four studies using comparative designs to examine the effect of OTC availability of OCs and 23 studies examining values and preferences of patients and providers, mostly from the USA and Mexico.
The more recent and rigorous studies suggested OTC users had higher rates of OC continuation over time; there was some indication that OTC users had lower rates of side effects but slightly higher rates of use of OCs despite contraindications.
Values and preferences suggested general support for OTC availability or pharmacy access, with more support among women and pharmacists than among physicians.
What do the new findings imply?
Making OCs available OTC, perhaps with progestogen-only pills that have fewer contraindications to use, may be an approach to increasing access to and use of this effective contraceptive option.
Introduction
Ensuring access to contraceptive methods, including for vulnerable populations and young people, is essential for the well-being and autonomy of women and girls. Oral contraceptives (OC), both combined oral contraceptives (COC) and progestogen-only pills (POP), are widely used effective methods of birth control. However, access to OCs varies globally—in some countries, OCs are available over the counter (OTC), while other countries restrict access to OCs either by requiring eligibility screening by trained pharmacy staff before dispensation (pharmacy access, or behind-the-counter availability), or by requiring a healthcare provider’s prescription. A 2015 review of OC access across 147 countries found that 35 countries had OCs legally available OTC, 11 countries had OCs available without a prescription but only after eligibility screening by trained pharmacy staff, 56 countries had OCs available informally without a prescription and 45 countries required a prescription to obtain OCs.1 Given the persistently high proportion of unintended pregnancies globally—44% according to some estimates2—making OCs available OTC in more settings has the potential to reduce barriers to access, thereby increasing use of this effective contraceptive option and reducing unintended pregnancies.
While different regulatory criteria are needed in different countries to make a specific medication available OTC or with eligibility screening by pharmacy staff, the WHO is responsible to provide overall guidance to critical questions of whether interventions should be recommended or not. We conducted this systematic review in the context of developing WHO normative guidance on self-care interventions for sexual and reproductive health and rights. We included both a review of effectiveness data and a review of data on values and preferences.
Methods
Effectiveness review: PICO question and inclusion criteria
We sought to answer the following question: should contraceptive pill/oral contraceptives be made available over the counter without a prescription?
Our effectiveness review followed the PICO question format:
Population
Individuals using contraceptive pill/oral contraceptives.
Intervention
Availability of contraceptive pill/oral contraceptives OTC (without a prescription) or behind the counter (pharmacy access, including dispensing from trained pharmacy personnel and pharmacist prescribing of hormonal birth control).
Comparison
Availability of contraceptive pill/oral contraceptives by prescription only.
Outcomes
Uptake of OCs (initial use).
Continuation of OCs (or, conversely, discontinuation).
Adherence to OCs (correct use).
Comprehension of instructions (product label).
Health impacts (unintended pregnancy, side effects, adverse events or use of OCs despite contraindications).
Social harms (eg, coercion, violence (including intimate partner violence, violence from family members or community members, and so on), psychosocial harm, self-harm, and so on), and whether these harms were corrected/had redress available.
Client satisfaction.
To be included in the effectiveness review, a study had to meet the following criteria:
Employ a study design comparing OTC availability of OCs (with or without pharmacist dispensation) to prescription-only availability of OCs.
Measured one or more of the outcomes listed above.
Published in a peer-reviewed journal.
We focused on daily contraceptive pill/oral contraceptives for routine pregnancy prevention and did not include studies examining pills specifically for emergency contraception.
Where data were available, we stratified all analyses by the following subcategories:
Behind-the-counter (pharmacy access) versus OTC availability without a prescription.
COCs versus POPs.
Point of access (eg, stores, pharmacies, and so on).
Prior use of contraception.
Age: adolescent girls and young women (aged 10–14, 15–19 and 15–24) and adult women (aged 25+).
Vulnerabilities (ie, poverty, disability, religion).
High-income versus low/middle-income countries.
Literacy/educational level.
Study inclusion was not restricted by location of the intervention or language of the article. We planned to translate articles in languages other than English if identified. The complete protocol was registered and is available in PROSPERO (CRD42019119406).
Values and preferences review: inclusion criteria
The same search strategy was used to search and screen for study inclusion in a complementary review of values and preferences related to OTC access to OCs (including pharmacy access). We included studies in the values and preferences review if they presented primary data (qualitative or quantitative) examining people’s preferences regarding OTC access to OCs. We included studies examining the values and preferences of both people who have used or potentially would use OCs themselves as well as providers (including pharmacists) and other stakeholders, such as male partners, policymakers and insurance providers.
Search strategy
The same search strategy was used for both the effectiveness review and the values and preferences review. We searched four electronic databases (PubMed, the Cumulative Index to Nursing and Allied Health Literature (CINAHL), Latin American and Caribbean Health Sciences Literature (LILACS) and Embase) through the search date of 30 November 2018. The following search strategy was developed for PubMed and adapted for entry into all computer databases; a full list of search terms for all databases is available from the authors on request.
(‘Contraceptives, Oral’ [Mesh] OR ‘oral contraceptive pill’ [tiab] OR ‘oral contraceptive pills’ [tiab] OR ‘birth control pill’ [tiab] OR ‘birth control pills’ [tiab] OR ‘oral contraceptives’ [tiab] OR ‘oral contraception’ [tiab] OR ‘hormonal birth control’ [tiab] OR ‘hormonal contraception’ [tiab] OR ‘the pill’ [tiab]) AND (‘Nonprescription Drugs’ [Mesh] OR ‘nonprescription’ [tiab] OR ‘over the counter’ [tiab] OR ‘over-the-counter’ [tiab] OR ‘without a prescription’ [tiab] OR ‘pharmacist-prescribed’ [tiab] OR ‘pharmacy access’ [tiab] OR ‘clinician-prescribed’ [tiab] OR ‘physician-prescribed’ [tiab] OR ‘without prescription’ [tiab] OR ‘community pharmacy services’ [Mesh] OR ‘community center’ [tiab] OR ‘community centre’ [tiab] OR store [tiab] OR online [tiab] OR mobile [tiab] OR telehealth [tiab])
To identify articles that may have been missed through online database searching, we used several complementary approaches. We reviewed the resources section of the OCs OTC working group website,3 which gathers scientific articles and reviews on this topic, and reviewed the citations included in several related recent reviews.1 4 5 Secondary reference searching was also conducted on all studies included in the review. We searched for ongoing trials through ClinicalTrials.gov, the WHO International Clinical Trials Registry Platform, the Pan African Clinical Trials Registry, and the Australian New Zealand Clinical Trials Registry. Finally, selected experts in the field were presented with our list of included articles and asked to share any additional article we had missed.
Titles, abstracts, citation information and descriptor terms of citations identified through the search strategy were initially screened by a member of the study staff. Remaining citations were then screened in duplicate by two reviewers (CEK and PTY) with differences resolved through consensus. Final inclusion was determined after full-text review.
Data extraction and analysis
For each included article, data were extracted independently by two reviewers using standardised data extraction forms. Differences in data extraction were resolved through consensus.
For the effectiveness review, data extraction forms covered the following categories:
Study identification: author(s); type of citation; year of publication, funding source.
Study description: study objectives; location; population characteristics; type of oral contraceptives; description of OTC access; description of any additional intervention components (eg, any education, training, support provided); study design; sample size; follow-up periods and loss to follow-up.
Outcomes: analytical approach; outcome measures; comparison groups; effect sizes; CIs; significance levels; conclusions; limitations.
Risk of bias: assessed for randomised controlled trials with the Cochrane Collaboration’s tool for assessing risk of bias,6 and for non-randomised trials but comparative studies with the Evidence Project risk of bias tool.7
For the values and preferences review, data extraction forms included sections on study location, population, study design and key findings.
We did not conduct meta-analysis due to the small number and heterogeneous nature of included studies. Instead, we report findings based on the coding categories and outcomes.
Patient and public involvement
Several of the authors are current or past OC users. HJ, chair of the advisory group for the WHO Patients for Patients Safety Program, was involved as a community representative starting with the phase of protocol development. He commented on the overall study design and protocol, including patient-relevant outcomes, interpretation of results and writing/editing the document for readability and accuracy. Patients were involved in a global survey of values and preferences and in focus group discussions with vulnerable communities conducted to inform the WHO guideline on self-care interventions8; they thus play a significant role in the overall recommendation informed by this review.
Results
Search results
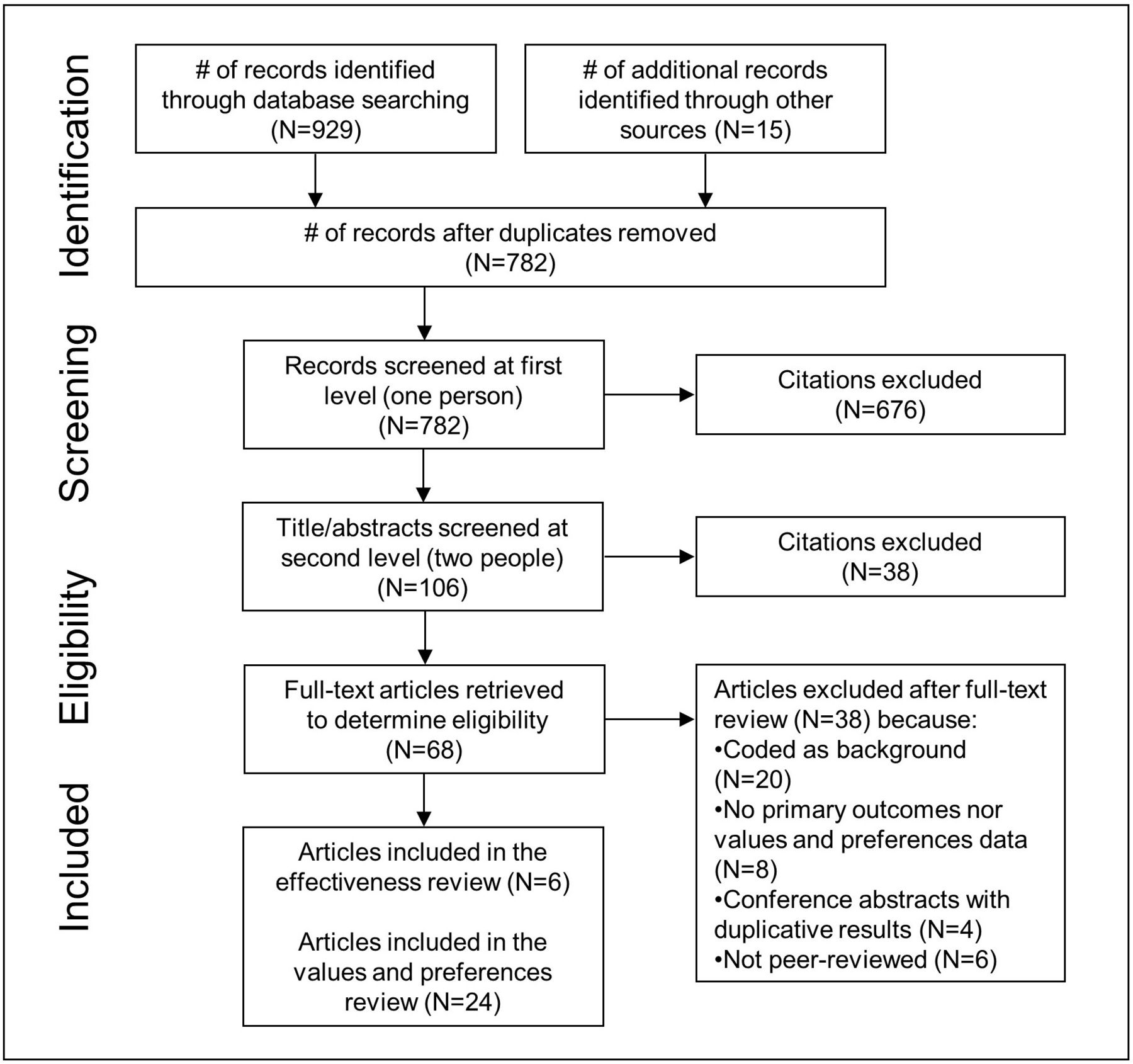
Figure 1 presents a flow chart showing study selection for both the effectiveness and values and preferences reviews. The initial database search yielded 929 records, with 15 records identified through other sources; 782 remained after removing duplicates. After the initial title/abstract review, 68 articles were retained for full-text screening. Ultimately, six articles reporting data from four studies met the inclusion criteria and were included in the effectiveness review.9–14 An additional 24 articles from 23 studies were included in the values and preferences review.13 15–37

{kind=link}
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow chart showing disposition of citations through the search and screening process.
One study was considered for the effectiveness review but ultimately judged to not meet the inclusion criteria.38 In Kuwait, where OCs are available OTC, the study compared women who consulted with a physician and those who did not. We excluded the study because it was not clear whether women received OCs from these physicians or not. However, we note that the study found no difference across groups in OC continuation, duration of first OC use, method failure and reasons for discontinuation.
Effectiveness review
Table 1 shows the characteristics of the four studies included in the effectiveness review.9–14 The first study, the Border Contraceptive Access Study, was a longitudinal cohort study conducted among women living in El Paso, Texas, USA, from 2006 to 2008 with results reported in a number of articles.10 12 13 The study used convenience sampling to enrol 1046°C users who obtained OCs either OTC from a Mexican pharmacy (n=532) or from a family planning clinic in El Paso (n=514). These women were interviewed at baseline and then followed in three additional surveys over 9 months. The second study, an analysis of data from the 2000 Mexican National Health Survey14 by an overlapping group of researchers, was a cross-sectional comparison of women who reported obtaining OCs OTC to women who reported obtaining them from a healthcare provider. The third and fourth studies were significantly older, drawing on data from the 1970s. They presented cross-sectional comparisons of women whose initial contraceptive method was OCs, obtained OTC from a pharmacy/drugstore, from a private provider/clinician or the national family planning programme: one analysed data from the 1979 Mexico National Fertility and Mortality Study among 2063 women9 and the other was a 1974 Fertility and Contraceptive Use survey in Bogotá, Colombia, among 893 women.11 All studies included mainly women using COCs, rather than POPs, although pill formulations likely differed by time.
Descriptions of studies included in the effectiveness review
As all studies were observational, table 2 shows the risk of bias assessments using the Evidence Project tool. The Border Contraceptive Access and Mexican National Health Survey studies found that women who obtained their OCs OTC were different in at least some sociodemographic characteristics than those who obtained them from clinics; however, both studies employed analyses that adjusted for confounders to address this discrepancy.10 12–14 The Mexico National Fertility and Mortality Study and Colombian Fertility and Contraceptive Use Survey said there were only minor sociodemographic differences between groups but did not present actual statistics to support these statements; neither study adjusted for confounders.9 11 The Border Contraceptive Access Study relied on convenience sampling, but was strengthened by its longitudinal design.10 12 13 Conversely, while the other three studies were cross sectional in nature, they were strengthened by their multistage sampling strategies.9 11 14
Evidence Project risk of bias assessment7 for studies included in the effectiveness review
The included studies reported on three of the PICO outcomes: continuation of OCs, health impacts (specifically, use of OCs despite contraindications and side effects) and client satisfaction. For the other PICO outcomes, we found no studies. Results from each study are presented in table 3 and described below.
Outcomes of studies included in the effectiveness review
Continuation of OCs
The Border Contraceptive Access Study reported the proportion of women who continued OC use over the 9-month study period.12 Overall, 25.1% of clinic users discontinued by the end of the study period compared with 20.8% of OTC users (p=0.12). In an unadjusted Cox proportional hazards model, OTC users were more likely to continue OC use than clinic users (unadjusted HR: 1.48, 95% CI 1.07 to 2.04); this estimate changed only slightly in the adjusted model and remained statistically significant (adjusted HR: 1.58, 95% CI 1.11 to 2.26).
The two studies from the 1970s also examined continuation. The Mexico National Fertility and Mortality Study presented continuation rates at 12 months per 100 women who accepted OCs as their first contraceptive method.9 No difference by OC source was found: 59% of private physician or clinic users, 57% of government family planning programme users and 60% of OTC users remained on OCs after 12 months. The Colombian Fertility and Contraceptive Use Survey presented first contraceptive method continuation rates for women who chose OCs at 12 and 24 months.11 Though a validation survey found that the continuation rates were overestimated by approximately 10%–15%, the study found that at both 12 and 24 months, OC continuation was approximately 5% higher for clinic users than OTC users.
Use of OCs despite contraindications
The two studies from the 2000s reported on the use of OCs despite contraindications.
The Border Contraceptive Access Study reported use of OCs despite contraindications using the WHO Medical Eligibility Criteria (MEC) (third edition) relative (category 3) and absolute (category 4) contraindications.10 At the baseline survey, at least one category 3 or 4 contraindication was reported by 21.4% of OTC users and 13.8% of clinic users (p=0.002). OTC users were more likely to have any category 3 contraindication (13.4% vs 8.6%, p=0.006), but there was no difference in category 4 contraindications (7.4% vs 5.3%, p=0.162). The study also provided a list of specific contraindications. For most contraindications there was no significant difference for OTC and clinic users; however, OTC users were significantly more likely than clinic users to have category 3 hypertension (140–159/90–99) (8.4% vs 4.5%, p=0.036) or to both smoke (<15 cigarettes per day) and be 35 years or older (6.4% vs 3.1%, p=0.017).
The 2000 Mexican National Health Survey analysis reported use of OCs despite category 3 contraindications using the WHO MEC Criteria from 1996 based on hypertension and smoking at or over age 35.14 Overall, the study found no significant differences in contraindications between OC users who obtained their pills OTC versus those who obtained them at a clinic (table 3). This finding held true when comparing OTC to clinic users on contraindications related to hypertension (≥160/100) (1.7% vs 1.8%), smoking and age 35 or older (9.4% vs 7.5%), and both contraindications combined (4.5% vs 3.6%).
Side effects
Two studies reported on side effects related to OC use. The Border Contraceptive Access Study found that, at baseline, 22.3% (104/466) of OTC users reported side effects compared with 30.4% (144/474) of clinic users (p<0.01).12 The Colombian Fertility and Contraceptive Use Survey found that 51% of OTC users and 44.4% of clinic users reported any side effect from initial OC use.11 Neither group reported the most important complications of OC use (thrombophlebitis and thromboembolism), and similar proportions reported the most common side effect (headache). OTC users were more likely to mention nervousness, skin problems, pain and bleeding problems, while clinic users were more likely to complain of weight changes, varices and other side effects (not specified).
Satisfaction
One study—the Border Contraceptive Access Study—reported client satisfaction but did not present exact results. They stated, ‘three quarters of clinic users and more than 70% of pharmacy users said they were very satisfied with their source (results not shown). Only about 4% of each group said they were either somewhat or very unsatisfied with their source.’13
Values and preferences review
We identified 24 articles from 23 studies that met the inclusion criteria for the values and preferences review. Of these, 13 articles focused on the perspectives of female OC users, potential users, or women in general,13 15 16 18 19 21–24 29–31 37 9 focused on the perspectives of healthcare providers (particularly physicians) and pharmacists17 25 26 28 32–36 38,39 and 1 focused on the general public;27 one article included both women and healthcare providers.20 Almost all studies were conducted in the USA, except for one each in Canada,32 France17 and Ireland15; one publication from the Border Contraceptive Access Study included in the values and preferences review included women residing in El Paso, Texas, who accessed OCs in both the USA and Mexico.13 Studies used both quantitative and qualitative methodologies.
Studies covered both OTC and pharmacy access. While most studies of women asked about hypothetical values and preferences around OTC availability, a few studies reported the perspectives of women who had actually used OTC or pharmacy access services.13 20 Most studies distinguished between pharmacy access and OTC availability, although a few were less clear about which approach they were studying, using terms such as ‘access to oral contraceptives without a prescription,’ which we assumed to be OTC availability. Using our best assessment of which model studies were examining, we present data for the values and preferences studies separated by true OTC access (table 4) and pharmacy access (table 5), and present results accordingly below. Two studies examined perspectives on both OTC and pharmacy access, so are presented in both tables 4 and 5. One cross-sectional survey among young women aged 14–17 in the USA found slightly higher support for dispensation in pharmacies compared with full OTC availability (79% vs 73%), but slightly higher potential use of full OTC availability compared with pharmacy access (61% vs 57%).30 Another cross-sectional survey among healthcare providers in the USA found much higher rates of support for pharmacy access (74%) compared with full OTC access (28%), although this study combined the pill, patch and ring together in one question about hormonal contraceptives.35
Study descriptions and key findings of studies included in the values and preferences review examining OTC access
Study descriptions and key findings of studies included in the values and preferences review examining pharmacy access
OTC access
Across studies using both quantitative and qualitative methods, women generally expressed high interest in hypothetical OTC availability of OCs. In quantitative studies, support for OTC availability of OCs ranged from a third of female students in two US colleges/universities19 31 to 89% of current OC users aged 18–50 in Ireland.15 However, most quantitative surveys of potential OC users found that a majority of participants supported OTC availability.15 18 21 24 30 Slightly lower but still sizeable proportions of women said they would obtain OCs OTC if available.23 24 30 Ease of access, convenience, privacy and time saved from clinician visits for prescriptions were the main benefits women anticipated from OTC availability.13 16 18 30 However, across studies, participants noted concerns about cost, continued use of other preventive screening options (eg, for Pap smears, pelvic exams, clinical breast exams and sexually transmitted infections) and the safety of such access, particularly for young people, first-time pill users and women with medical conditions.13 16 18 19 23 30 31
Healthcare professionals from France and the USA, particularly medical doctors, voiced moderate to low support for OTC availability of OCs, often citing safety concerns, OC efficacy, concerns about correct OC use or missed examinations for medical contraindications.17 28 35 Providers generally supported making POPs available OTC more than they supported making COCs available OTC.26
Pharmacy access
Among potential or current OC users, most women were in favour of pharmacy access, and substantial proportions said they would obtain OCs through pharmacy access if it were available.29 30 37 Some women currently not using any contraception said they would begin using a hormonal contraceptive if pharmacy access were available.29 One study found that women (and pharmacists) were satisfied with pharmacist-led OC use and expressed willingness to continue seeing pharmacist prescribers.20 While young women appreciated their traditional healthcare providers, they liked the increased access and convenience of obtaining OCs directly from a pharmacy.37
In studies among healthcare providers, pharmacists were generally very supportive of pharmacy access to OCs, while physicians tended to be more moderately supportive.20 25 28 32–36 Increased access to care, preventing unintended pregnancies and convenience for patients were the most frequently identified potential benefits.25 33–35 Safety, time constraints, lack of private space in the pharmacy, increased liability and reimbursement were identified as potential barriers.25 28 33 36 There was also concern from pharmacists about physician’s resistance to making OCs available at pharmacies28 and concern from physicians about pharmacist’s refusal to provide services.34
Finally, in a study of digital comments on online media articles about pharmacy access to OCs in the USA, commentators were generally positive and cited benefits including increasing access to healthcare, reducing unintended pregnancies and supporting individual autonomy, but noted these must be balanced with potential safety and logistical concerns.27
Discussion
In this systematic review, we identified four studies using comparative designs to examine the impact of OTC availability of OCs. Two studies conducted in the 2000s examined women who obtained OCs OTC in Mexico and compared them with women who obtained OCs from providers in either Mexico or the USA. The other two studies were significantly older (from the 1970s) and compared first contraceptive method users who either obtained OCs OTC from a pharmacy or drugstore or through a provider or family planning programme; the OC formulations in these studies were likely different, and women 45 years ago potentially differ from women today in terms of desired fertility, decision-making around contraceptive methods and perception/tolerance of and tendency to report side effects. While the more recent studies suggested OTC users had higher rates of OC continuation over time and fewer side effects, there was some indication that OTC users had slightly higher rates of use of OCs despite contraindications. Contraindications are an important concern; however, research has indicated that women can self-screen for contraindications fairly well using a simple checklist.40 41 Despite the strengths of the studies included in the review, the small evidence base provides limited guidance for countries considering OTC availability of OCs.
We identified a much larger evidence base on the values and preferences of potential users, providers and the public. However, this evidence was also limited, since almost all studies were conducted in the USA. Women were generally in favour of OTC availability; healthcare providers were as well, with pharmacists expressing higher support than physicians for pharmacy access. Among both women and providers, support was generally higher for dispensation in pharmacies compared with full OTC availability, and for OTC access to POPs rather than COCs. Given the near-universal use of COCs at the times and locations where the studies included in the main review were conducted, we had no comparative effectiveness data on POPs. This is unfortunate, as POPs have been suggested as a good option for initial OTC availability, given that they have fewer contraindications to use.
An additional concern about OTC availability is that the concomitant reduced visits to clinicians may also translate to a reduction in routine preventive screening (including for Pap smears, pelvic exams, clinical breast exams and screening for sexually transmitted infections). This was not one of our prespecified PICO outcomes since such exams are not required to receive OCs per the WHO’s Selected Practice Recommendations for Contraceptive Use.42 However, the Border Contraceptive Access Study did report on preventive screening; while women who obtained their OCs from a clinic reported slightly higher rates of some screenings, both groups (OTC and clinic users) had high overall rates of reported screenings with relatively minimal differences between groups.43 One values and preferences study also found that US women said they would continue to get screened if OCs were made available OTC,23 although clinicians were afraid they would not.35 These findings offer some indication that OTC access for OCs may not necessarily result in reduced use of other preventive services.
OTC availability is only one way to increase access to OCs. A previous systematic review found that increasing the number of OC pill packs dispensed or prescribed increased OC continuation, although it also resulted in increased pill wastage.44 There are also internet-based platforms for ordering OCs, which comply with clinician prescriptions or pharmacist screening, but conduct all screenings online.45 A modelling study found that making out-of-pocket pill pack costs low or free would increase OC use.46 Finally, increased insurance coverage for OCs should also reduce access barriers to OC use, regardless of access point. Although moving OCs to OTC status should lead to fewer clinician visits for women, thus decreasing costs related to travel, time and other medical expenses associated with those visits, OTC access could potentially increase the cost of OCs if insurance does not cover OTC purchases, or if women are unaware that they can use insurance in OTC purchases. Insurance considerations should be explicitly considered in policy discussions of OTC availability, as insurance coverage will be particularly important for some of the most vulnerable groups, such as low-income women and girls.
Our review has several strengths, including our broad search strategy and our inclusion of both effectiveness and values and preferences studies. However, conclusions from our review are limited by the small evidence base in this area. We identified four observational studies in our main effectiveness review, from the same global region, and there may have been residual confounding in comparing OTC and clinic OC users despite some analyses being adjusted. Although there were more studies in the values and preferences review, they were also geographically limited, and many relied on participants’ responses to hypothetical questions about OTC availability. While it is challenging to conduct randomised trials of what is fundamentally a policy intervention, researchers should be encouraged to take advantage of natural experiments such as the Border Contraceptive Access Study or to study changes to policies such as those recently allowing pharmacy access to OCs in the US states of Oregon and California. Further, many countries already allow OTC availability of OCs, so policy decisions can also take into consideration the wide range of country experience in this area.
Despite the limitations of the evidence base, this review provides important information to guide policy decisions around OTC availability of OCs. This evidence has been used to inform the development of WHO recommendations for self-care interventions for sexual and reproductive health and rights in relation to OTC availability of OCs. The benefits and harms of OTC availability of OCs and the values and preferences of patients and providers found in the present review, along with a separate survey of community values and preferences and consideration of resource use, human rights and feasibility, will shape the recommendation. Additional research into outcomes critical to decision-makers where little comparative data currently exist should be done to address the gaps identified.
Acknowledgments
We thank Laura Ferguson and Nandi Siegfried for their comments on the review protocol. We also thank Johns Hopkins research assistants Rui (Renee) Ling, Kaitlyn Atkins, Priyanka Mysore, Molly Petersen and Anita Dam for help with screening the initial database search results, conducting hand searching and secondary reference searching, and duplicate data extraction. Finally, we thank Daniel Grossman and Sara Yeatman for their timely and thorough responses to questions about their studies, and the excellent comments from the anonymous reviewers who really helped improve the manuscript.
References
Footnotes
Handling editor Soumyadeep Bhaumik
Contributors MN conceptualised the study. CEK and PTY designed the protocol with input from JK, MLG, LG, HJ and MLN. PTY ran the search and oversaw screening, data extraction and assessment of bias. CEK drafted the manuscript, while all authors reviewed the draft and provided critical feedback. All authors had full access to all of the data (including statistical reports and tables) in the study and can take responsibility for the integrity of the data and the accuracy of the data analysis. All authors read and approved the final manuscript. The corresponding author, as guarantor, accepts full responsibility for the finished article, has access to any data and controlled the decision to publish.
Funding This study received financial support from the UNDP-UNFPA-Unicef-WHO-World Bank Special Programme of Research, Development and Research Training in Human Reproduction (HRP) and the Children's Investment Fund Foundation (CIFF). HRP was involved in the study design.
Disclaimer The funders played no part in the decision to submit the article for publication, nor in the collection, analysis and interpretation of data.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data come from published journal articles. Extracted data are available on request to the corresponding author.