Article Text

Abstract
Introduction Male circumcision (MC) confers partial protection to men against HIV and, in research settings, some sexually transmitted infections (STIs). It is also associated with protection from some STIs among female partners. However, real-world data on changes in STI transmission associated with large-scale public African medical male circumcision (MMC) conducted for HIV prevention are lacking and would improve estimates of the health impact of MMC.
Methods The HIV Incidence Provincial Surveillance System is a community-based surveillance platform for HIV prevalence, incidence and intervention coverage trends in KwaZulu-Natal province, South Africa. HIPPS collected cross-sectional self-reported data on circumcision status (from men), partner circumcision status for past three partners (from women) and demographic characteristics and behavioural risk factors; and tested participants for HIV, herpes simplex virus type 2 (HSV-2), syphilis, hepatitis B, Neisseriagonorrhoeae, Chlamydiatrachomatis, Trichomonasvaginalis and Mycoplasmagenitalium. Bivariable and multivariable analyses were performed on associations between own (men) or partner’s (women) circumcision status and each STI. Multivariable analyses adjusted for age, demographic characteristics and behavioural risk factors, and incorporated false discovery rate (FDR) correction.
Results Among men, MMC had a protective association with HSV-2 (OR 0.66, 95% CI 0.50 to 0.86), hepatitis B (OR 0.53, 95% CI 0.30 to 0.95), HIV (OR 0.50, 95% CI 0.38 to 0.65) and M.genitalium (OR 0.53, 95% CI 0.32 to 0.88). Among women, partner circumcision had a protective association with HSV-2 (OR 0.71, 95% CI 0.53 to 0.95) and HIV (OR 0.66, 95% CI 0.49 to 0.90). Associations with HIV and HSV-2 remained significant for men and all women after FDR correction.
Conclusion These real-world data, supporting protective associations between MMC conducted for HIV prevention and STIs in men and women, can help clarify the full impact of MMC and support a role in broader sexual health programming.
- HIV
- prevention strategies
- community-based survey
- cross-sectional survey
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Medical male circumcision (MMC) provides men with partial protection against acquiring HIV and some sexually transmitted infections (STI) such as human papillomavirus (HPV), chancroid, Trichomonas vaginalis, Mycoplasma genitalium, genital ulcer disease and syphilis through heterosexual sex.
In observational studies and research settings, MMC is also associated with protection from some STIs for female partners, including herpes simplex virus type 2 (HSV-2), chlamydia and syphilis; and cervical cancer and dysplasia (resulting from oncogenic HPV).
What are the new findings?
This study provides the first real-world data on the association of MMC with STIs in men and women in a programmatic voluntary MMC (VMMC) scale-up setting: KwaZulu-Natal, South Africa, where STI prevalences are high.
For men, MMC was protective against HSV-2, M. genitalium, hepatitis B (a novel finding) and HIV. For women, partner circumcision was protective against HSV-2 and HIV.
What do the new findings imply?
These data validate the expectation that the VMMC programme is providing substantial ancillary protection against STIs responsible for large population health burdens.
These findings suggest that VMMC can play an important role in broader sexual health programming, in addition to its foundational purpose of HIV prevention.
Introduction
Medical male circumcision (MMC) confers approximately 60% protection to men against HIV infection,1–3 and partial protection against some sexually transmitted infections (STI)4–6 via heterosexual transmission. A recent systematic review also demonstrated protective associations between male circumcision (MC) and multiple STIs and their complications in female partners,7 particularly syphilis, chlamydia, cervical cancer and dysplasia, and herpes simplex virus type 2 (HSV-2). These associations in women may result from a mix of ‘indirect’ protection—circumcised men are less likely to be infected—and ‘direct’ protection—infected men may be less infectious if medically circumcised. Biological mechanisms are poorly understood. Voluntary MMC (VMMC) programmes for HIV prevention in sub-Saharan Africa performed nearly 19 million MMCs between 2008 and 2017 and annual achievements continue rising.8 Given the health burden exacted by STIs, estimated at over 12 million disability-adjusted life years annually in 2015,9 the protective association with MC therefore has important potential public health implications beyond HIV prevention.
However, while population studies have demonstrated the real-world effectiveness of VMMC in preventing HIV in men10 and women,11 12 data for STIs come from research settings or predate VMMC scale-up. VMMC is a broadly targeted service package, consciously undertaken by men for HIV prevention, that includes complete foreskin removal and HIV testing and counselling, STI screening and referral, and condom provision.13 Thus, its impact on STIs may not be identical to that of traditional or religious circumcision as an isolated procedure, in sexually isolated subpopulations, or with a different purpose—the typical contexts of pre-VMMC observational studies. A better understanding of effects of the modern VMMC programme on STIs, particularly in high-prevalence settings, would better define its potential role in sexual health.
KwaZulu-Natal (KZN) province in South Africa is an informative setting for exploring these associations. It has a high HIV prevalence (27% among 15–49 year-olds in the 2017 South African National HIV Prevalence, Incidence and Behaviour Survey (SABSSM)),14 and a high STI prevalence, shown in studies of sexually active young women.15 16 Most recently, a 2016–2017 population-based study among women aged 15–24 years found prevalences of 28.7% for HSV-2, 11% for chlamydia, 2% for gonorrhoea, 5% for trichomonas, 0.4% for active syphilis and 42% for bacterial vaginosis.17 Prevalences in men were similar but lower for all STIs. Additionally, hepatitis B had prevalences of 7.5% among HIV-negative infants and 13% among HIV-positive infants in 2011 samples from HIV-exposed KZN infants,18 reflecting likely higher prevalences in their mothers, despite national introduction of infant vaccination in April 1995.19
KZN is also a national VMMC priority area. Substantial scale-up in the study area began in 2010.20 The 2012 SABSSM found self-reported 23.2% MC coverage among adult KZN males.21 Though uncommon in the study area, traditional circumcision is also practised.22 Some variants involve full foreskin removal and appear to confer protection, where others do neither;23 conversely, instrument sharing may promote HIV transmission.24 In our sample, traditionally circumcised men were fewer than 4% of male participants and had HIV prevalence similar to that of uncircumcised men.25
Here we aimed to provide the first real-world data on associations of VMMC with STIs in men and women. We analysed baseline data from a large population-based household survey to assess whether these anticipated ancillary benefits are observed in this high-transmission intensity setting.
Methods
Study design, recruitment and enrolment
The HIV Incidence Provincial Surveillance System (HIPSS) was established as a platform to monitor trends in HIV prevalence, incidence and intervention coverage in Vulindlela and Greater Edendale subdistricts, uMgungundlovu municipality, KZN. The region has a combined population of about 360 000 people and includes rural (Vulindlela) and periurban and informal settlements (Greater Edendale, near Pietermaritzburg). Sixteen primary care centres, three district hospitals and multiple community-based organisations providing HIV prevention and care serve the area. HIPSS has serial cross-sectional and longitudinal components; this analysis used data from the 2014–2015 baseline cross-sectional survey. Recruitment used multistage cluster sampling, with simple random selection at enumeration area level, systematic selection at household level and random selection with replacement of one age-eligible (15–49 years) household member. Of 15 100 households, sized for 84% power to detect a 30% HIV incidence reduction, 11 289 were eligible and consented, from which 9812 individuals consented and enrolled. Participants provided blood and self-collected vulvovaginal (females) or first-pass urine (males) samples. Details are described elsewhere.26
Patient and public involvement
Study design included extensive engagement with local stakeholders including traditional leaders, service providers, local government and others. Participants were provided opportunities to access HIV and STI test results at a local clinic using a unique identifier. Details are described elsewhere.26
Data collection
Survey data included demographic information, partner characteristics and circumcision status. Men were asked, ‘When you do NOT have an erection, would you say your penis is uncircumcised or circumcised?’ Those answering ‘circumcised’ were asked, ‘Who circumcised you?’ with options ‘medical circumcision’, ‘traditional circumcision’ and ‘don’t know’. Women were asked their number of lifetime sexual partners and then for the three most recent, if male, ‘Is he circumcised?’ Options were: ‘circumcised at start of relationship’, ‘not circumcised’, ‘became circumcised during relationship’ and ‘don’t know’. Women were not asked circumcision type.
Key covariables collected included education level, categorised as ‘no schooling/creche/pre-primary’, ‘primary’ (grades 1–7), ‘incomplete secondary’ (grades 8–11/National Technical Certificate (NTC) 1 or 2), ‘completed secondary’ (grade 12/NTC3) and ‘tertiary’ (diploma/degree); household monthly income, categorised; and for women, presence or absence of a 5-year age gap with the male partner being older; age in years; relationship status; and measures of behavioural HIV risk (table 1).
Demographics of HIV Incidence Provincial Surveillance System participants: baseline sample, KwaZulu-Natal, June 2014 to June 2015
Peripheral venous blood samples were tested for HIV antibodies using the fourth-generation HIV enzyme Biomerieux Vironostika Uniform II Antigen/Antibody Microelisa system (BioMérieux, Marcy l’Etoile, France). Positive samples were confirmed with the HIV 1/2 Combi Roche Elecsys (Germany) (Roche Diagnostics, Penzberg, Germany) and HIV-1 Western Blot Bio-Rad assay (Bio-Rad Laboratories, Redmond, WA, USA). Indeterminate results were resolved using ADVIA Centaur HIV Antigen/Antibody Combo (CHIV) assay (Siemens, Tarry Town, USA).
Syphilis antibodies were detected via rapid plasma reagin (RPR) assay (Immutrep RPR, Omega Diagnostics, Alva, UK) with a quantitative titre of 1:8 or higher considered positive. Serum was also tested for HSV-2 antibodies via ELISA (HerpeSelect, Focus Diagnostics, Cypress, CA, USA) and for hepatitis B surface antigen (Siemens Centaur, USA). Neisseria gonorrhoeae, Chlamydia trachomatis, Mycoplasma genitalium and Trichomonas vaginalis were detected via multiplex PCR (RotorGene 3000/6000/RotorGene Q real-time platforms (QIAGEN, Hilden Germany)) in DNA extracted from the swab and urine samples, using N.gonorrhoeae (ATCC 700825), C.trachomatis (ATCC VR-885), T.vaginalis (ATCC 30001) and M.genitalium (ATCC 33530) strains as controls.
Inclusion and data analysis
Men with a known self-reported circumcision status who reported ever having had vaginal or anal sex (and thus were able to report on risk behaviours included in the final model) were included. Those reporting being uncircumcised or traditionally circumcised, or not knowing their circumcision status, were all classified as uncircumcised.
Women who reported being sexually active (defined as for men) and reported a circumcision status for all of their reported partners (not ‘don’t know’) were included. A secondary analysis was conducted on the subgroup reporting only one lifetime sexual partner, to allow adjusting for presence of an age gap with their partner. Women were classified by partner circumcision status:
Main analysis: ‘all partners reported to be circumcised at the start or during the relationship’ versus ‘any partner uncircumcised’.
Subgroup with one lifetime partner: ‘partner circumcised at the start or during the relationship’ versus ‘partner uncircumcised’.
For participants excluded based on self-reported lack of sexual activity, STI prevalence was examined to assess the presence of substantial sexual activity in this subpopulation, suggesting the exclusion of their data had potential to affect findings. For hepatitis B only, participants aged under 20 years were also excluded, to prevent confounding from the national immunisation programme in effect during their infancies.
Missing values were uncommon for most variables and are shown in the tables. In multivariable analyses, for number of partners and income, ‘missing’ was a separate category; for education level and presence of an age gap with the partner, observations’ missing values were excluded. This caused few exclusions.
Analyses used survey weights accounting for unequal selection probabilities and non-response.27 Survey procedures used SAS V.9.4 (SAS Institute). Associations between own or partner’s circumcision status and risk behaviours were explored using the Rao-Scott χ2 test, to identify potential confounders for the relationship between circumcision status and STI outcome. Associations of age with STI infection and circumcision status were also tested to examine the role of age as a confounder.
The association between circumcision status and each STI outcome was then assessed in each group using multivariable logistic regression. For each sex separately, two sets of models were created. Bivariable models controlled only for age. Multivariable models controlled for age, education, income, relationship status, condom use, drinking before sex and number of lifetime partners. For women with only one lifetime partner, models also controlled for existence of a 5-year age gap with an older partner. Because of the complex multidirectional nature of causality between different STIs, and because order of infection is not ascertainable nor the focus of this analysis, STIs were not covariables for each other. Not all variables included in final models were significant at p<0.05, but all had been identified as epidemiologically plausible or possible confounders to measuring the relationship between circumcision status and STI outcome. In addition, an alternate approach was trialled for women with one lifetime partner, in which partner age was treated as a continuous variable. Because this change had minimal impact (not shown), final models treated age as a dichotomous variable as described above.
Exceptions were made for gonorrhoea, syphilis and hepatitis B. Because these STIs were rare among women with only one lifetime partner, only age and partner’s circumcision status were included in final models.
Corrections for multiple comparisons were performed using the false discovery rate proposed by Benjamini and Yekutieli.28
Results
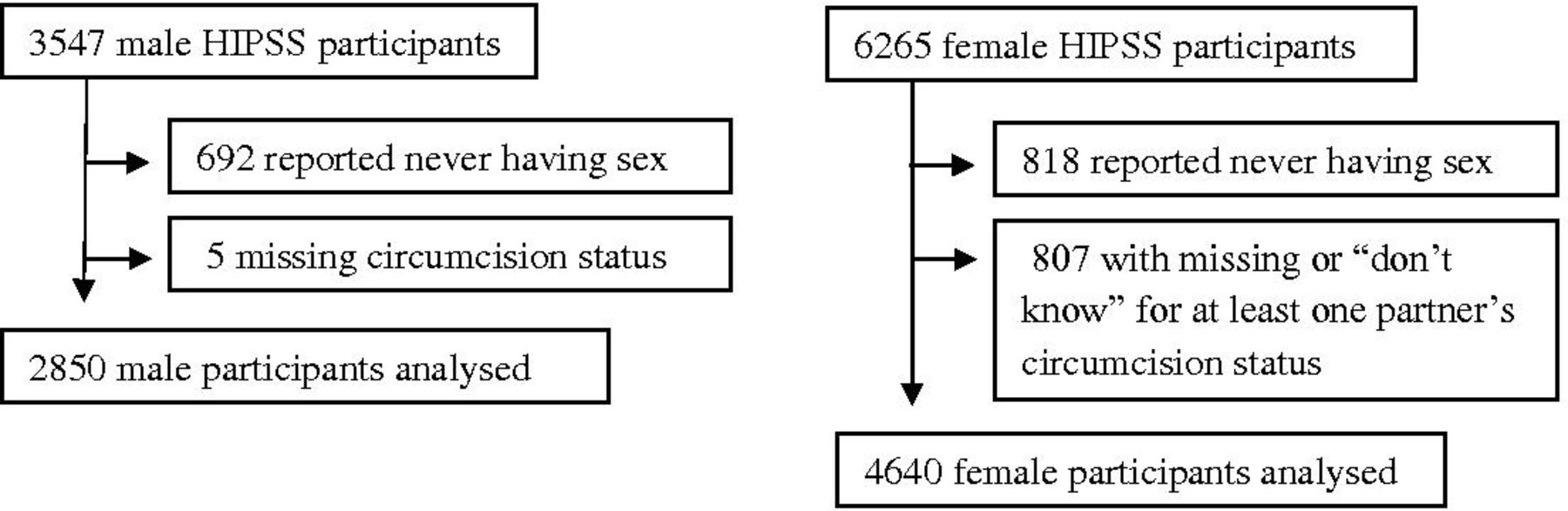
The analysed sample included 4640 women and 2850 men (figure 1). Virtually all exclusions among men were due to reporting never having had sex. Exclusions among women were evenly divided between this and not knowing circumcision status for all partners. The overall individual participation rate for the study was 69% among inhabitants of occupied households and 86.7% of those of enrolled households.25
{kind=link}
Inclusion flow charts for male and female HIV Incidence Provincial Surveillance System (HIPSS) participants in subanalysis of associations between medical male circumcision and sexually transmitted infections.
Both male and female participants were generally young (52.3% and 49.8% under 30 years, respectively), and single, having never married or cohabitated (86.4% and 77.7%, respectively) (table 1). Virtually all (97.7% and 97.5%, respectively) had at least primary educations. Most households reported low incomes, 501–6000 rand (about $42–$504) monthly, and close to 10% reported no income. Compared with women, men were less likely to have had only one partner, and more likely to report sexual debut before 15 years old and sex after drinking. Among men, 29.2% reported being medically circumcised; among women, 35.1% reported their most recent partner was circumcised. Medical circumcision was negatively associated with older age among men (p<0.01; see online supplementary appendix tables 1–3 for associations between circumcision status and covariables).
Supplemental material
Women with one lifetime partner were younger than all women (59.6% vs 49.8% under 30 years, respectively) and more likely to be married (22.0% vs 14.3%), though most were single and never married (72.2% vs 77.7%) (table 1). They were similar to all women in household income, age gap with most recent partner, self-reported partner HIV positivity, never having sex after drinking and reporting a circumcised ‘most recent’ (only) partner (40.0% vs 35.1%, respectively).
With respect to risk behaviours that could act as confounders, circumcised men were at lower behavioural risk than uncircumcised men, with significantly fewer reporting more than two lifetime partners (67.5% vs 74.5%; p<0.01), higher prevalence of having always used condoms with their most recent partner (31.2% vs 21.1%; p<0.01) and lower prevalence of ever having sex after drinking (25.9% vs 33.2%; p=0.01). Women had similar results: those with circumcised partners were less likely to report more than two lifetime partners (41.5% vs 48.5%; p<0.01) and were more likely to have always used condoms with most recent partner (24.2% vs 17.3%; p<0.01), though they had similar likelihood of sex after drinking (95.4% vs 95.6% said ‘never’; p=0.04). These variables were included as predictors in multivariable analyses. With respect to age as a potential confounder, only C.trachomatis and N. gonorrhoeae had negative univariable associations with increasing age (online supplementary appendix tables 4–6).
Tables 2 and 3 show STI prevalences among men and women, respectively, and associations with circumcision status. Complete regression results are found in online supplementary appendix tables 4–6.
Association of medical male circumcision status with sexually transmitted infection outcomes among men (n=2850)
Association of male partner circumcision status with sexually transmitted infection outcomes among women
For men, HSV-2 was the most prevalent STI at 53.2%, followed by HIV at 32.4%; prevalences of other STIs were near or below 5%. In bivariable analysis, circumcision had a protective association with HSV-2, T. vaginalis, M. genitalium, hepatitis B and HIV. There was also a positive association between circumcision and C.trachomatis. Adjustment for age alone weakened this association, but it remained significant. In the final multivariable analysis, the association with circumcision remained protective for all but T. vaginalis, and the positive association with C.trachomatis was further weakened but remained significant.
For women, HSV-2 was also the most prevalent STI at 76.8%, followed by HIV at 49.0%. T. vaginalis was third at 14.2%. Other STIs had prevalences below 10%. STIs were substantially more common in women than in men, except that prevalences were similar for syphilis, M. genitalium and hepatitis B. In bivariable analysis among all women, partner circumcision had a protective association with HSV-2 and HIV, and a positive association with C.trachomatis. Among women, unlike men, adjustment for age alone eliminated the C.trachomatis association. In multivariable analysis, the protective associations remained, and the association with C.trachomatis was again not significant. The same protective associations were seen in women with one lifetime partner, with nearly identical magnitudes.
When findings were corrected for multiple testing, for men and for all women, associations with HIV and HSV-2 remained significant; for women with one lifetime partner, associations were not significant (online supplementary appendix tables 7–9).
Both men and women excluded due to reporting never being sexually active had lower, but still substantial, STI prevalences (eg, HSV-2 at 16.9% and 21.3% among men and women, respectively; and C.trachomatis at 3.2% and 5.8%).
Discussion
For men, MMC had a protective association with HSV-2, M. genitalium, hepatitis B and HIV. For women, partner circumcision had a protective association with HSV-2 and HIV. These findings incorporate adjustment for important confounders including age and risk behaviour. They provide evidence for benefits of VMMC in STI prevention previously documented only in research settings and observational studies predating VMMC programme expansion. For women, findings did not differ between the general population and those with one partner, raising confidence in these results. (For women with one partner, partner circumcision status should be more accurately assessed, and age gap with current partner was controlled for.)
Protective associations with HIV and HSV-2 remained significant for men and for all women after adjusting for multiple comparisons. However, the protective associations for other STIs and the positive associations with chlamydia were not. The study was not powered around the STI outcomes reported here and so it is not surprising that only the most common STIs, for which power to detect differences is greatest, retained significance. However, this finding demonstrates that even in this setting with relatively high STI prevalences, an even larger sample size is needed to determine associations for rarer STIs, and no final claims about how these relate to circumcision can be made without more data. Significant associations referred to in the remainder of this discussion are uncorrected values where not otherwise specified.
HSV-2 causes recurrent painful outbreaks and is responsible for an estimated 10 000 cases of neonatal infection globally each year, most in Africa, conferring 60% case fatality without treatment.29 HSV-2 may also contribute30 to the common obstetric danger of preterm delivery.31 In the high-prevalence environment of our study setting, MC may have potential for substantial impact on HSV-2 and its associated risks.
M. genitalium is a risk factor for HIV acquisition.32 It is associated with urethritis in men33 and with cervicitis, urethritis and pelvic inflammatory disease in women,34 though we found a protective association only in men.
Hepatitis B is typically an acute infection and most cases resolve spontaneously, but it can cause acute liver failure and, in a minority of patients, can progress to chronic infection leading to cirrhosis and liver cancer.35 Our test measures current infection, and the finding of protection for men associated with MMC is intriguing. We are not aware of previous studies examining this association for MMC in the general population. Observational studies have found evidence in both directions for circumcision outside the VMMC context: an increased risk of hepatitis B virus (HBV) associated with traditional or religious circumcision,36 37 presumably due to lack of equipment sterilisation; and protection associated with circumcision in special populations (eg, men who have sex with men).38 However, even after excluding participants born after introduction of infant HBV vaccination, we cannot rule out confounding by vaccination later in life. (Adult vaccination is only recommended for health workers in South Africa, but catch-up vaccination is recommended for children under 5 years and those with HIV.)39 This new evidence for a protective association should be confirmed by including HBV in future studies capturing MMC status. Vaccination remains the most effective mechanism for preventing HBV infection, but VMMC may provide marginal protection in unvaccinated male populations (South Africa’s three-dose coverage has remained between 65% and 74%40) or those whose immunity has waned with age, common in adolescence.41
The protective associations found here for non-HIV STIs in women are more limited than those identified in a recent global systematic review7:HSV-2 and chlamydia and syphilis, as well as cervical cancer and dysplasia (caused by human papillomavirus (HPV), which was not assessed in our sample). However, the protective associations noted in that review were not seen in the subset of articles reporting on female partners of HIV-positive men, expected to have increased susceptibility to and shedding of multiple pathogens facilitated by their HIV infection. The high prevalence of HIV in our study population may therefore account for some of the narrower scope of protection seen here. This cannot be tested, since partner HIV status was not directly measured for female participants.
Potential biological mechanisms underlying protective effects of circumcision on STI transmission are more obvious for some observed associations than for others. HSV-2 has a plausible basis for effect: it is an ulcerative infection which circumcision deprives of a microabrasion-prone portal of entry and a hidden surface for eruption and transmission. Preventing microabrasions may be a plausible basis for protection against hepatitis B in men as well. For urethritic infections like M. genitalium and chlamydia (discussed below), it is less clear how foreskin removal could affect risk. Foreskins provide a warm, moist environment that might increase survival time for pathogens in secretions and increase their chance of gaining access to the urethra. Alternatively, associations might be mediated by coinfection with HIV42 or with other STIs.
The protective association seen for HIV is as expected in men. For women, it is encouraging that HIV prevention benefits from MC which were expected based on modelling43 and observational literature7 were confirmed. Other recent literature supporting this finding includes the 2018 description of an incidence cohort in a VMMC scale-up area of Kenya, in which women with circumcised partners had significantly lower incidence of HIV than those with uncircumcised partners.12
The positive bivariable association between MC and C. trachomatis seen in both men and women was an unexpected finding, which further analyses attributed largely to confounding by age. In women, the association was not significant in the multivariable model; the negative association of C. trachomatis with age may result from increased cervical ectopy in younger age groups, exposing a more vulnerable tissue type to infection.44 In men, age adjustment did not eliminate the association. As above, no candidate for a biological mechanism has been identified.
The previously mentioned systematic review7 found high-consistency evidence for a protective relationship between circumcision and C. trachomatis, but the number of included studies was small, limitations were present (eg, lack of adjustment for some strong predictors) and findings were not unanimous. Another study not included in that review also supports a protective association.45 Another recent systematic review found that evidence on this association was mixed.46 If circumcision does confer protection against individual infection episodes, another possible explanation for our findings is a paradoxical protective effect from repeated infection,47 causing enhanced immunity and ultimately lower prevalence in uncircumcised males. However, this seems inconsistent with the existence of the association with circumcision in even the youngest age groups.
Prevalences of STIs among women were roughly consistent with the recent population-based study conducted by Francis et al17 in the rural district of uMkhanyakude, KZN, northeast of our study area. Because participants in the Francis study were substantially younger, it is unsurprising that they had a lower prevalence of HSV-2, gonorrhoea, trichomonas and syphilis (using the more specific treponemal testing with Veneral Disease Research Laboratory confirmation), and a higher prevalence of chlamydia. However, with the exception of HSV-2, absolute prevalence estimates were within 10% of each other. Prevalences in men were also consistently higher in our sample, presumably for the same reason.
In addition to limited power for STI outcomes, limitations include the potential for misclassification of MC status by both women (including missing data on prior partners) and men (medical vs traditional). However, if non-differential, this would bias associations towards the null. Also, traditional circumcision is probably not equivalent from an STI risk perspective to being uncircumcised, but traditionally circumcised men were a small minority and had the same HIV prevalence as uncircumcised men. It is also possible that classifying partners who became circumcised during the relationship as circumcised introduced self-selection bias (those who were HIV negative being more likely to get circumcised). These limitations will be partially addressed by a planned analysis of cohort data capturing STI incidence. As self-reported sexual history in these data will cover only 1 year, it will presumably be less subject to recall errors and circumcision status changes, and baseline STI data will support ascertainment of order of events in coinfection cases.
In addition, key subpopulations whose HIV risk would not result from heterosexual transmission were not excluded. Our inclusion of them would also be expected to bias associations towards the null since circumcision status would have less impact on their total HIV risk. The substantial prevalence of STIs in participants excluded for lack of sexual activity also suggests some activity or other exposure was present, and associations with MC could be different in this subpopulation. Some risk behaviour questions did not have a ‘no response’ option, potentially leading to under-reporting by respondents who might have preferred not to answer. However, this does not seem likely to differentially affect circumcision and non-circumcision groups. It is also possible that protective associations in men result partly from the STI screening and treatment services included in VMMC, though only infections with signs or symptoms would be identified.13 HPV was not assessed in this data set, but is perhaps the STI through which MC has greatest potential impact by preventing cervical cancer, the most common cancer among African women.48 Finally, the study was probably underpowered to detect associations of MC with rarer STI outcomes like syphilis.
Conclusion
This study provides the first real-world data on changes in STI transmission in southern Africa associated with the VMMC programme. Protective associations with several STIs in men including what we believe is the first general population data on HBV, and with HSV in women, are encouraging in this area with high STI burden. Findings are representative of the sexually active general population and, given the biomedical nature of the mechanism of protection, are likely to apply in other settings. Programmes may benefit from use of this and similar data to better quantify potential impacts of VMMC on sexual health. Further research is needed with larger sample sizes that can confirm findings in rarer STIs, and in longitudinal cohorts that can confirm the attribution of these outcomes to VMMC.
Acknowledgments
The authors gratefully acknowledge the intellectual contributions of David Lewis of the University of Sydney and Robert Kirkcaldy of the US CDC Division of STD Prevention, and the support of the local stakeholders engaged in the planning process.
References
Footnotes
SD and CT are joint first authors.
SD and CT contributed equally.
Handling editor Sanni Yaya
Presented at This work was previously presented orally at the 2017 International AIDS Society Meeting.
Contributors SD drafted the manuscript and participated in the analyses. CT conceived and designed the data collection, conceived the manuscript and participated in drafting and revision. LL performed the statistical analyses and provided intellectual input to the manuscript. BMB provided intellectual input to the analyses and manuscript. KA provided intellectual input to the manuscript. ABMK conceived, designed and oversaw the implementation of data collection, and provided intellectual input to the manuscript.
Funding This publication has been supported by the President’s Emergency Plan for AIDS Relief (PEPFAR) through the Centers for Disease Control and Prevention (CDC) under the terms of operative agreement 3U2GGH000372-02W1. ABMK is supported by the joint South Africa–US Program for Collaborative Biomedical Research from the National Institutes of Health (R01HD083343).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Institutional Review Board at the University of KwaZulu-Natal (BF269/13). The protocol was also approved by the CDC Center for Global Health as research in which CDC personnel were not engaged (2014-080).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data are available upon reasonable request.