Article Text

Abstract
Building on the gains of the National Health Mission, India’s Reproductive, Maternal, Newborn, Child and Adolescent Health (RMNCH+A) Strategy, launched in 2013, was a milestone in the country’s health planning. The strategy recognised the interdependence of RMNCH+A Interventions across the life stages and adopted a comprehensive approach to address inequitable distribution of healthcare services for the vulnerable population groups and in poor-performing geographies of the country. Based on innovative approaches and management reforms, like selection of poor-performing districts, prioritisation of high-impact RMNCH+A healthcare interventions, engagement of development partners and institutionalising a concurrent monitoring system the strategy strived to improve efficiency and effectiveness within the public healthcare delivery system of the country. 184 High Priority Districts were identified across the country on a defined set of indicators for implementation of critical RMNCH+A Interventions and a dedicated institutional framework comprising National and State RMNCH+A Units and District Level Monitors supported by the development partners was established to provide technical support to the state and district health departments. Health facilities based on case load and available services across the High Priority Districts were prioritised for strengthening and were monitored by an RMNCH+A Supportive Supervision mechanism to track progress and generate evidence to facilitate actions for strengthening ongoing interventions. The strategy helped develop an integrated systems-based approach to address public health challenges through a comprehensive framework, defined priorities and robust partnerships with the partner agencies. However, lack of a robust monitoring and evaluation framework and sub-optimal focus on social determinants of health possibly limited its overall impact and ability to sustain improvements. Guided by the learnings and limitations, the Government of India has now designed the ‘Aspirational Districts Program’ to holistically address health challenges in poor-performing districts within the overall sociocultural domain to ensure inclusive and sustained improvements.
- healthcare service delivery
- RMNCH+A
- supportive supervision
- development partners
- high priority districts
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
Based on an inclusive and comprehensive approach, India’s Reproductive, Maternal, Newborn, Child and Adolescent Health (RMNCH+A) Strategy aims to improve outcomes across 184 poor-performing districts of the country.
Recognising the interdependence of RMNCH+A Interventions across the life stages, the strategy prioritised districts for implementation of evidence-based, high-impact interventions by galvanising support from development partners and establishment of a concurrent monitoring mechanism for measuring improvements across healthcare facilities in the High Priority Districts.
Variable responsiveness of health systems across the states, over-reliance on partner agencies, lack of a dedicated monitoring and evaluation framework and an inability to address social determinants of health might have limited the impact of the strategy.
Learnings and limitations of the strategy have paved the way forward for designing holistic implementation frameworks by engaging all relevant stakeholders and adopting a systems-based approach towards improving healthcare service delivery.
Introduction
Access to adequate, acceptable and quality healthcare services is important towards achieving ‘Universal Health Coverage’.1 India has faced the burden of inadequate and poor-quality health services for a prolonged period that has led to high mortality and morbidity and unmeasurable adverse health outcomes among the vulnerable population groups.2 According to an estimate (2013), with a large annual birth cohort of about 26 million live births and 158 million children in the age group of 0–5 years, India accounts for the largest number of deaths in under-five years age group—nearly 1.5 million annually, of which around 0.8 million newborns die within 28 days of birth.3
To reduce inequity in healthcare services and improve reproductive, maternal, newborn and child health outcomes, India’s Ministry of Health and Family Welfare (MOHFW) launched the ‘National Rural Health Mission’ (2005) and the ‘National Urban Health Mission’ (2008). These were later merged into the ‘National Health Mission’ with an overarching objective to strengthen the public healthcare infrastructure and quality of health services and secure an enhanced financial support for overall health system strengthening (HSS). Owing to these efforts and investments in the public healthcare sector, the country has made steady progress towards curbing the deaths among mothers and children. The ‘Maternal Mortality Ratio’ improved by a 5.2% average annual rate of reduction from 600 per 100 000 live births (1990) to 200 per 100 000 live births (2010). ‘Under-Five Mortality Rate’ in India declined at a much faster pace as compared with the global average and registered a 3% average annual rate of reduction from 114 deaths per 1000 live births (1990) to 61 deaths per 1000 live births (2011), against the global average of 87 and 57, respectively.4–6
Conceptualisation of India’s ‘Reproductive, Maternal, Newborn, Child and Adolescent Health Strategy’
Despite the ongoing efforts and progress achieved, the country’s healthcare system reflected a critical imbalance characterised by high out-of-pocket expenditure stemming out from the deficiencies in the public sector’s capacity to deliver basic healthcare. The areas and population groups having the greatest need for quality healthcare services could not get an appropriate share from the existing public health services.7–9 Hence, the situation demanded a comprehensive vision for public healthcare services, encompassing both preventive and curative aspects for a broader range of beneficiaries and health conditions, and necessitating leveraging of new resources.10 Building on these aspects, MOHFW in consultation with stakeholders developed India’s ‘Reproductive, Maternal, Newborn, Child and Adolescent Health Strategy’ or ‘RMNCH+A Strategy’. The strategy was launched during the ‘National Summit on Call to Action for Child Survival and Development’ in February 2013,11 and guided by the central tenets of universal care, entitlement and accountability, it laid a renewed emphasis on high-impact health interventions and addressed strengthening of healthcare services especially in the poor-performing geographies of the country.12
Approach adopted in the Reproductive, Maternal, Newborn, Child and Adolescent Health Strategy
India’s RMNCH+A Strategy was unique as it recognised the fact that maternal and child health cannot be improved in isolation and need to be effectively weaved with adolescent, family planning and nutrition-based interventions. The ‘Plus’ within the strategy focused on continuum of care with linkages between the interventions targeted at various stages of life-cycle from newborn to the reproductive age, with focus on adolescence as a distinct life stage. It laid focus on linkages between home and community-based services to facility-based care, and between referrals and counter-referrals between and among the health facilities at the primary, secondary and tertiary levels.12
The ‘RMNCH+A Strategy’ was based on innovative approaches and management reforms, like selection of poor-performing areas and high-impact healthcare interventions, enhancing responsibility of development partners and establishing a concurrent monitoring system within the healthcare delivery system to improve its efficiency and effectiveness as described in the following section.
Selection of ‘High Priority Districts’
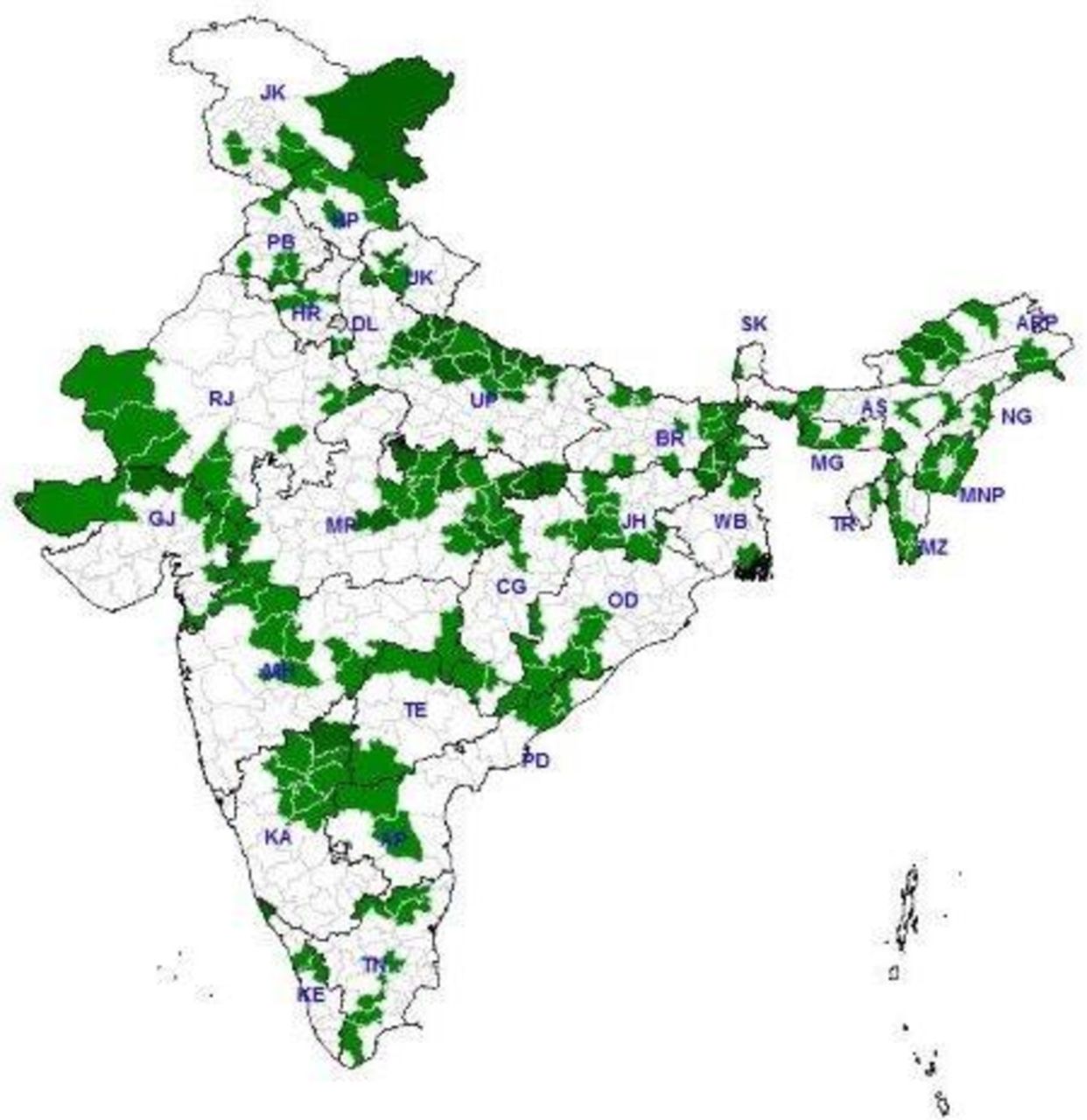
India is a union of 29 states and seven union territories (UT) comprising 718 districts with a vast and variable geographical expanse. The country is characterised by wide interstate and intrastate disparities in terms of distribution, availability, utilisation of public healthcare services and the health status of its citizens contributing towards poor health outcomes.13 14 Under the ‘RMNCH+A Strategy’, underperforming districts named as ‘High Priority Districts’ were identified to facilitate focused planning and implementation. To achieve this, state/UT-wise ranking of districts was done based on defined sets of mortality and outcome indicators selected from the most recent evaluation survey findings for the respective states/UTs. Likewise, ‘Annual Health Survey’ (2012–2013) was considered for nine states, while ‘District Level Household Survey-3’ (2007–2008) was considered for the remaining states/UTs (table 1). Within each state, 25% poorest performing districts were selected based on the performance of selected health indicators. Additionally, the tribal predominant districts and those affected by insurgent and rebel groups were also selected. Likewise, 184 ‘High Priority Districts’ were taken up across the country for focused efforts under the strategy. The number of targeted beneficiaries in these ‘High Priority Districts’ comprised nearly 8.3 million pregnant women and 7.6 million infants annually, accounting for almost 25% of the annual cohort of pregnant women and infants in India.15 Moreover, the strategy also embarked on differential planning with 30% additional resource allocation per capita by the state governments for each ‘High Priority District’ under the National Health Mission (figure 1).
Indicators used for identification of High Priority Districts

High Priority Districts (India).
Prioritisation of high-impact Reproductive, Maternal, Newborn, Child and Adolescent Health Interventions
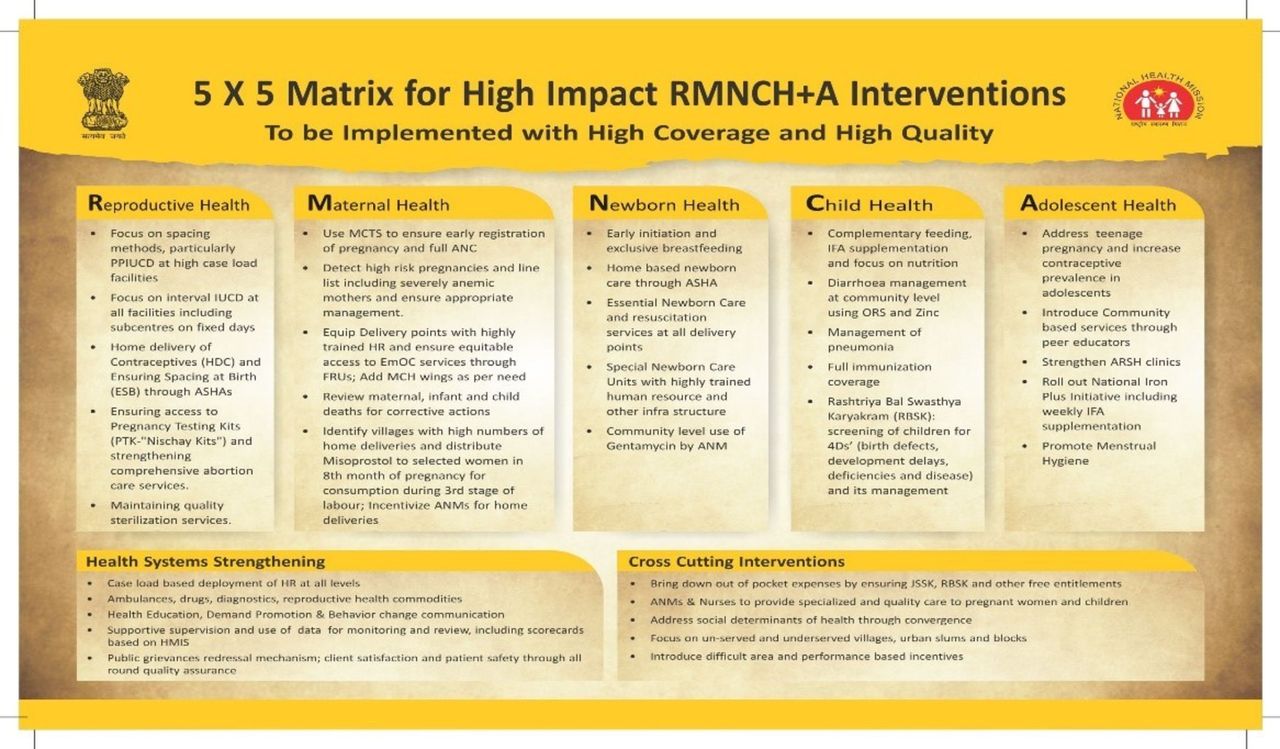
The ‘RMNCH+A Strategy’ focused on promotion, adoption and context-specific adaptation of evidence-based, high-impact interventions across different life-cycle stages including newborn, childhood, adolescence and the reproductive age groups. These interventions were selected based on the available scientific evidence documenting their efficacy and impact on reducing maternal and child, mortality and morbidity. The interventions were summarised in the form of ‘RMNCH+A 5×5 Matrix’ specifying five critical interventions in each of the five thematic areas, viz reproductive health, maternal health, newborn health, child health and adolescent health. Additionally, emphasis was also given on five cross-cutting and five HSS interventions focusing on infrastructure, human resources, supply chain management and referral transport measures (figure 2).16
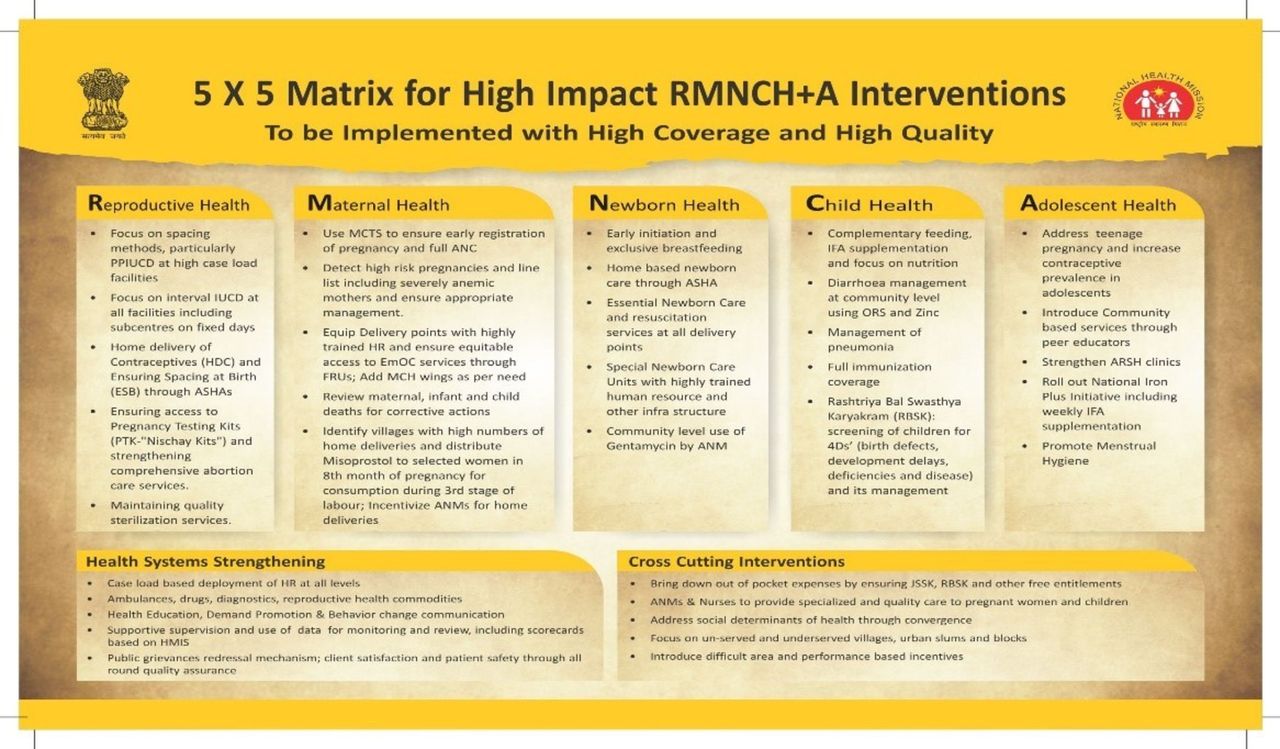
The Reproductive, Maternal, Newborn, Child and Adolescent Health (RMNCH+A) 5*5 Matrix.
Involving the development partners
The ‘RMNCH+A Strategy’ gave high reliance to partnerships and targeted to leverage and harmonise the technical assistance across the RMNCH+A spectrum. Concerted efforts were undertaken to galvanise the state governments and development partners working at the national and subnational levels through a series of steps as follows:15
Periodic consultations were organised by the national ministry for establishing strategic dialogue with the development partners. The partners were nominated in technical advisory and resource groups constituted for development and dissemination of training material and operational guidelines for RMNCH+A Interventions.
At the national level, a ‘National RMNCH+A Unit’ was constituted with support from the US Agency for International Development supported Maternal and Child Health Integrated Program (MCHIP) and ‘Vriddhi’ (Scaling up RMNCH+A Interventions) Projects and was anchored within the MOHFW. It coordinated technical assistance from the national and state-level partners, conducted periodic visits to the health facilities to measure progress and recommend actions, and monitored implementation of RMNCH+A Interventions in the states/UTs and ‘High Priority Districts’.
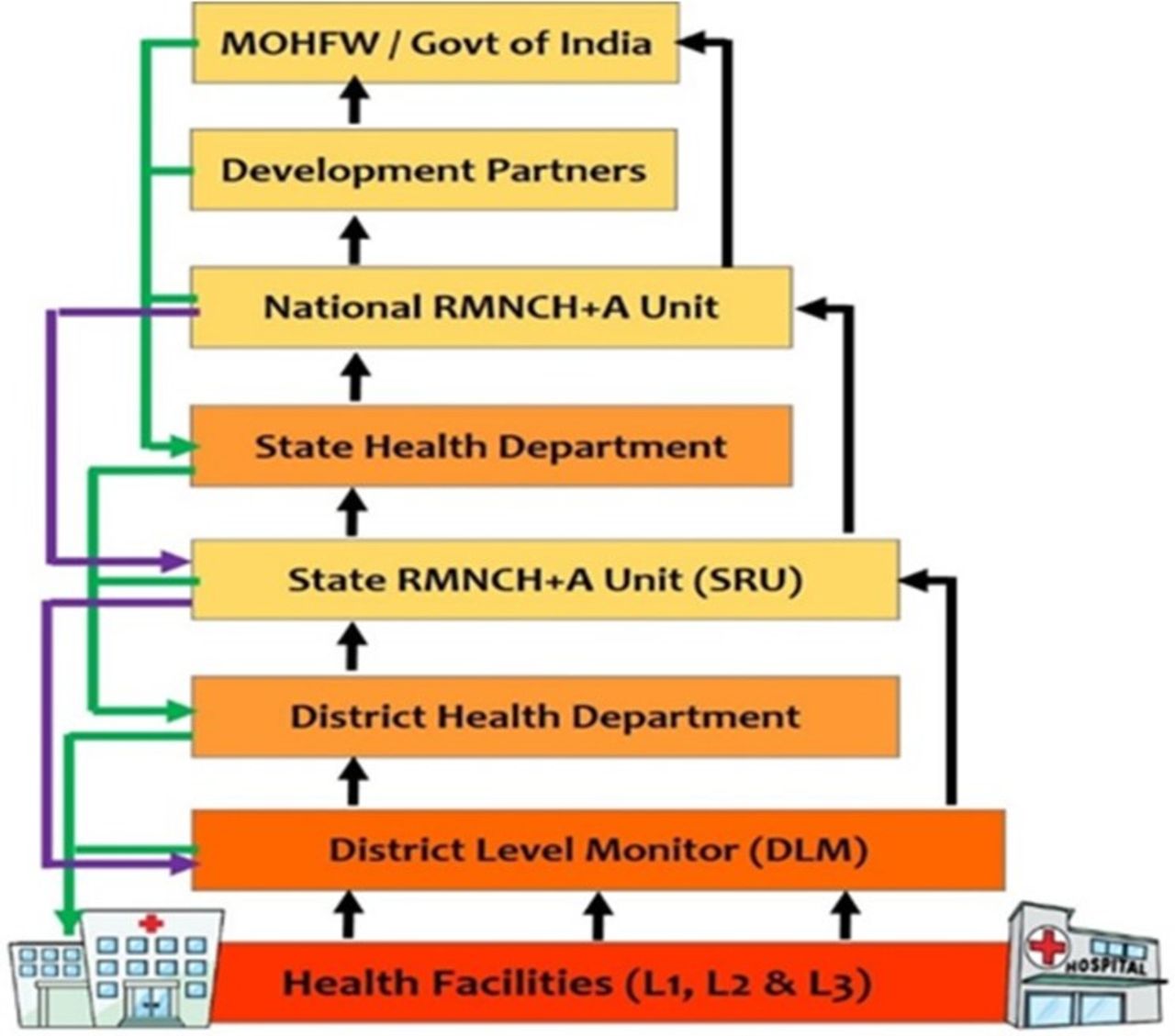
In the states, partners providing significant level of technical support were nominated as ‘State Lead Partner’ for the respective states. These lead partners were entrusted with the role to constitute and administer ‘State RMNCH+A Units’ within the state health departments to coordinate with other partner agencies working in the states, extend support to government health officials and staff in rolling out high-impact RMNCH+A Interventions and monitor implementation and progress under the overall guidance of the ‘National RMNCH+A Unit’ (figure 3).
In the ‘High Priority Districts’, one ‘District Level Monitor’ was recruited by the lead partner to work under the guidance of respective ‘State RMNCH+A Units’ and support district health departments in planning and monitoring implementation of RMNCH+A Interventions.

Reproductive, Maternal, Newborn, Child and Adolescent Health (RMNCH+A) State Lead Partners.
Gap assessment at public health facilities
Public health facilities in India are categorised into three levels, viz L1, L2 and L3 based on the availability of antenatal, intranatal and postnatal care service sets (table 2).17 L1 health facilities provide primary care, while L2 and L3 categories catering to the major proportion of beneficiary load provide basic and comprehensive obstetric care services, respectively, and serve as referral facilities. The ‘RMNCH+A Strategy’ envisaged strengthening of all three categories of public health facilities.
Levels of public health facilities and the services available
Before implementation of RMNCH+A high-impact interventions a gap assessment exercise was conducted in ‘High Priority Districts’ by the respective State Lead Partners to measure the functionality status and readiness of public health facilities to deliver high-impact RMNCH+A Interventions. This entailed collection of information regarding geographical mapping of different categories of health facilities, availability of health infrastructure and human resource, and analysis of existing gaps in terms of availability, accessibility, utilisation and quality of RMNCH+A services. The findings of the assessment were used to guide facility-level action planning and implementation.
Institutionalisation of ‘Reproductive, Maternal, Newborn, Child and Adolescent Health Supportive Supervision’
Various national-level reviews conducted from time to time identified absence of supportive supervision as a critical bottleneck in improving the performance of health staff and quality of healthcare services. The key challenges underlying this gap included inadequate number of supervisors within the system, lack of skills and training, and unavailability of policy and clear guidelines for supportive supervision and concurrent monitoring.12 The RMNCH+A Strategy recognised the need to strengthen supportive supervision of service providers to bring integration of primary care services, improve quality and enhance skills and application. Under the strategy, a supportive supervision model was institutionalised as an external concurrent monitoring mechanism to track progress and generate evidence to facilitate actions for strengthening high-impact RMNCH+A Interventions. Guided by the MOHFW, the RMNCH+A Supportive Supervision model was led by the partner agencies and integrated all five thematic areas for focused support and on-job facilitation.18–21
Preparations for the institutionalisation of the RMNCH+A Supportive Supervision were initiated soon after the launch of RMNCH+A Strategy and involved development of standardised tools comprising a uniform supportive supervision checklist (online supplementary file 1) for use across all High Priority Districts, computer-based (Microsoft Excel) tool for uniform compilation of observations made across the health facilities, training package for the supervisors and standard operating procedures regarding data collection, compilation, sharing at various levels, actions taken and follow-up.
Supplemental material
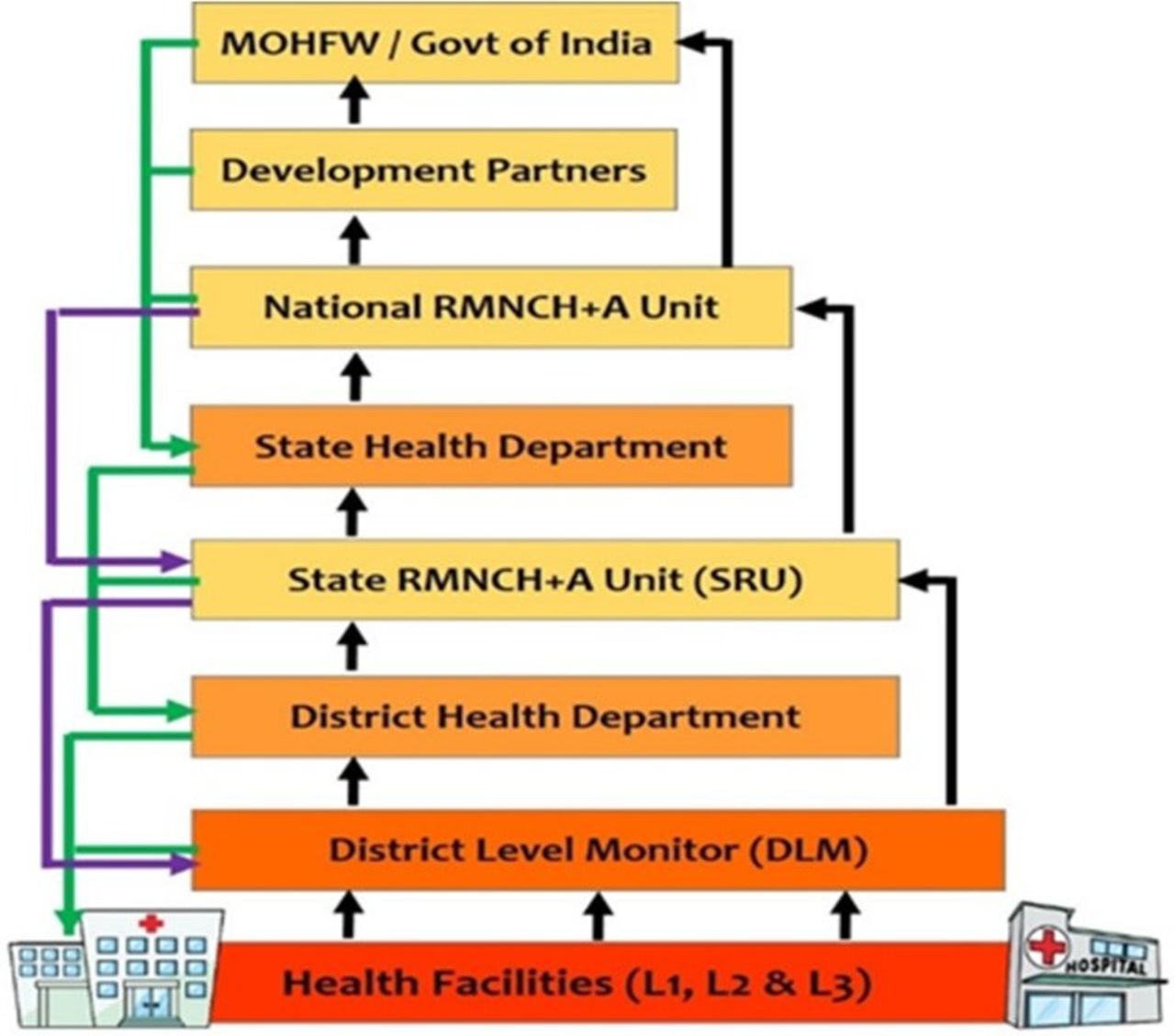
The RMNCH+A Supportive Supervision mechanism was rolled out from January 2015 in all 184 High Priority Districts and involved periodic visits to the health facilities by the ‘District Level Monitors’ to assess availability and quality of services using the standardised checklist and provide on-job mentoring to the concerned health facility staff. The checklist helped data collection on 141 critical RMNCH+A parameters through on-site assessment, direct observation, record review and interaction with the facility-level staff during the supportive supervision visits. The supervisor teams also sometimes comprised state and district government officials and additional representatives from partner agencies. The observations made during the visit were first shared with the facility-level staff followed by facilitation in preparation of facility-level action plans. The visits also entailed sensitisation and mentoring of the staff about national guidelines for adoption of correct practices and key observations and the action points were shared during the review meetings at district, state and the national level to initiate required corrective actions (figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Reproductive, Maternal, Newborn, Child and Adolescent Health (RMNCH+A) Supportive Supervision: feedback and feedforward mechanism. MOHFW, Ministry of Health and Family Welfare.
Progress made
Data from RMNCH+A Supportive Supervision visits conducted over a 2-year period between January 2015 and December 2016 were compiled at the National RMNCH+A Unit to assess the improvement in terms of availability of equipment and supplies and healthcare services at the public health facilities. During this period, health facilities were prioritised for strengthening based on the delivery load, services offered, available infrastructure and in discussion with the district health department. These prioritised facilities were visited more frequently to follow and facilitate the corrective actions. Therefore, during analysis, the data pertaining to the health facilities which were visited for three times or more were disaggregated, and observations made at the time of first visit and the last visit to these facilities were compared to measure progress.
Overall, 17 893 supportive supervision visits were conducted at 6678 health facilities in different categories during the 2-year period in the High Priority Districts (table 3).
Health facility level-wise distribution of supportive supervision visits
Out of these facilities, 2348 (35% of total facilities visited) were prioritised for strengthening including 556 facilities in L1 category, 1354 in L2 category and 438 facilities in L3 category. During the supportive supervision visits by the District Level Monitors and other representatives to the selected health facilities, on-site support was provided to the concerned staff in terms of reorientation, capacity building and to identify gaps and measures to correct them. During each visit, the standard checklist was used to capture the concurrent status with respect to the availability of equipment, amenities and ongoing practices. The information was collected through direct observation (eg, availability and functionality of supplies and equipment, implementation of key practices), review of records since last visit (eg, labour room records and filled partographs) and discussion with the staff (eg, family planning and service delivery at the community level). This information was computerised into an Excel-based data sheet. These compiled data were analysed on periodic basis to reveal progress and gaps to guide focused actions during the subsequent visits. Thematic area-wise key outcomes over a 2-year period are summarised in tables 4–6 (online supplementary file 2).
Supplemental material
Progress achieved in maternal health-related parameters
Progress achieved in newborn and child health-related parameters
Progress achieved in reproductive health-related parameters
Learnings
The RMNCH+A Strategy has been a unique example of adopting a comprehensive and holistic approach towards addressing the major causes of morbidity and adverse outcomes among the vulnerable population groups and geographies having inadequate health services across the entire country.
Recognising the inclusiveness and interdependence of RMNCH+A components, prioritisation of poor-performing districts, targeted implementation of evidence-based high-impact RMNCH+A Interventions, active and coordinated engagement of partner agencies and focused support to high case load health facilities in the High Priority Districts through the RMNCH+A Supportive Supervision mechanism are some novel systems that were established through the strategy, thereby contributing towards a system-based approach to improve health outcomes. The progress and issues were tracked using selected key performance and actionable indicators instead of broad parameters, which helped in facilitating specific and focused action plans.
Moreover, for the first time in the country’s healthcare spectrum, the RMNCH+A Strategy generated shared objectives and established partnerships through active engagement of all stakeholders within and beyond the government structures at the national and state levels. Specifically, the engagement of development partners helped leverage human and technical resource for strengthening healthcare service delivery. An institutional framework administered by the development partners and comprising National and State RMNCH+A Units and District Level Monitors ensured a dedicated team and efforts to support need-based facility-level planning, supervision and mentorship of health staff, and guided the health department take corrective actions.
The RMNCH+A Supportive Supervision exercise led by the development partners and backed up by national guidelines and standardised tools emerged as a unique model to identify gaps in real time and facilitate gap-oriented planning and implementation at the facility level. The findings of the mechanism showed improvements in terms of basic infrastructure, availability of essential drugs, equipment and other supplies, and the service delivery-related processes followed at the public health facilities in High Priority Districts. This perhaps also translated into improved knowledge and quality of care at the health facilities.
The analysis of information captured during the supportive supervision visits shows improvement in terms of the availability of medicines and supplies, the practices followed by the service providers and the upkeep of facility-level records. From the findings it is evident that mentoring support, review mechanisms and development of facility specific action plans translated to improved leadership and governance resulting in improved service delivery. Overall, the RMNCH+A Strategy and the approaches adopted therein contributed in strengthening the WHO HSS building blocks towards an efficient and responsive public healthcare delivery system.22
Building on the gains and to further intensify efforts, the list of High Priority Districts was revised in 2017 based on the findings of National Family Health Survey (Round 4; 2015–2016). Likewise, 209 districts were identified as high priority based on composite index derived from status of six indicators, viz proportion of pregnant women who had four or more antenatal check-ups, proportion of safe deliveries, fully immunised children, prevalence of undernutrition, births in third order or more and use of modern family planning methods.
Limitations
The RMNCH+A Strategy is an initiative of the National Health Ministry and it specifically focused on actions across the RMNCH+A spectrum and the progress achieved. Although the strategy did help in establishing structures and processes, the desired outcomes have been variable as demonstrated by the findings from the supportive supervision mechanism which reveal thematic area-wise as well as geographic variations.
While the differential improvements as evidenced by the Supportive Supervision mechanism might be due to variability in capacity and responsiveness of health systems across the states of the country, over-reliance on development partners might be a contributing factor. This is because while the role of national ministry of health and partner agencies was defined well the expectations of state governments and district administration were not very specific. While the efforts of the partners did result in improved ownership and accountability within the government system, sustainability might be a challenge after withdrawal of partner support. Possibly the results might have been better if the state National Health Mission (NHMs) and district health authorities were in leadership capacities with partner agencies functioning as catalysts.
Also, though the strategy recognised adolescents as an important stakeholder, efforts to improve adolescent outcomes need further strengthening. The RMNCH+A Supportive Supervision mechanism which formed the fulcrum of the entire strategy did not adequately address adolescent health parameters possibly resulting in suboptimal improvements.
In addition, besides the RMNCH+A Supportive Supervision mechanism, the strategy lacked a defined monitoring and evaluation framework. As process evaluation was not undertaken, many of the learnings from implementation in widely variable geographies could not be highlighted. Due to lack of substantial evidence, integration of potential learnings at the policy level is also questionable.
Moreover, it is now well established that social determinants of health play a defining role in improving health outcomes, the strategy could have possibly expanded its scope to address the social determinants resulting in far more impressive gains across the High Priority Districts.
Conclusion
India’s RMNCH+A Strategy has been a historical milestone in the country’s healthcare planning. The strategy succeeded in establishing an institutional framework and a mechanism of facility-level, need-based planning through concerted and coordinated efforts. A recent review of data suggested that 48 of the 184 High Priority Districts have improved and hence are no longer included in the list of these districts.23 However, despite the improvements and the mechanisms established, gaps in the design and subsequent implementation make it difficult to gauge the impact of the strategy thereby limiting translation of learnings into long-term policy and planning. It is, therefore, imperative to identify the weaknesses, opportunities and the learnings gained from this strategy through assessments and data reviews in the coming years to guide future programmes better.
In addition, realising the importance of social determinants in fostering overall improvement in January 2018, the Government of India launched the ‘Transformation of Aspirational Districts’ initiative in 117 districts across the country. The initiative focuses on five themes, viz health and nutrition, education, agriculture and water resources, financial inclusion and skill development, and basic infrastructure and operational and implementation components. Within the health portfolio the initiative builds on the RMNCH+A framework to improve outcomes in the identified aspirational districts in a more holistic and comprehensive manner. More in line with the United Nations’ Sustainable Development Goals, the initiative targets to improve India’s ranking in Human Development Index, raising living standards and ensuring inclusive growth of all sectors.24
Acknowledgments
The authors thank the Ministry of Health and Family Welfare, Government of India, for leading the RMNCH+A Supportive Supervision mechanism and BMGF, DFID, NIPI, UNFPA, Unicef, USAID and Tata Trusts for their support and involvement in the initiative. The authors also acknowledge Arvind Kumar, Ashok Negi and Surajit Dey for supporting the development of the data compilation tool and data analysis.
Footnotes
Handling editor Soumyadeep Bhaumik
Contributors GT contributed towards designing the Supportive Supervision intervention, tested the implementation of the mechanism, drafted, reviewed and finalised the manuscript. He advised data analysis and coordinated the inputs from all the authors. VSS conceptualised the Supportive Supervision data analysis tool, coordinated its development and undertook data analysis and interpretation. JSM facilitated the intervention on ground, supported the development of the resource package for the intervention and drafting of the introduction and discussion sections. AJ facilitated the intervention on ground and supported the drafting of the methodology and results sections. PB cleaned, managed and analysed the data and coordinated with the various stakeholders involved in the implementation of the mechanism. MJ drafted and edited the manuscript and undertook data analysis and interpretation. SG reviewed and edited the manuscript and supported the development of the technical package for the intervention. AK conceptualised the scope of the strategy and the Supportive Supervision intervention and contributed to critically reviewing the manuscript. RK was associated with the conceptualisation of the RMNCH+A strategy and approach, providedoversight and guidance during implementation and reviewed the manuscript. RG contributed to design and development of the intervention, provided inputs into the data management and analysis sections and also critically reviewed the manuscript.
Funding This work was made possible by the support of the American people through the US Agency for International Development (USAID) and its VRIDDHI–Scaling Up RMNCH+A Interventions Project, implemented by IPE Global under the terms of Cooperative Agreement No AID-386-A-14-00001.
Disclaimer The contents of this paper are the responsibility of IPE Global and do not necessarily reflect the views of USAID.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The authors state that the current article describes a programmatic intervention: the RMNCH+A Strategy across the 184 High Priority Districts (HPD) of the country after approval from the Ministry of Health and Family Welfare, Government of India. As this strategy was limited to improving service delivery mechanisms and was a national government-led initiative no ethical clearance was sought before implementation of the intervention.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data generated or analysed during this study are included in this published article (and its supplementary information files: online supplementary file 1–RMNCH+A Supportive Supervision Checklist and online supplementary file 2–Supportive Supervision data set).