Article Text

Abstract
HIV rapid diagnostic tests (RDTs) are instrumental in scaling-up HIV testing services (HTS) in low-income and middle-income countries (LMICs). HIV misdiagnosis is a growing concern in the era of expanded and decentralised access to HTS. External quality assurance (EQA) programme including proficiency testing (PT) for HIV RDTs is a priority to guarantee the accuracy and reliability of the patients’ result. Here we are sharing Haiti’s 11 years’ experience in implementing HIV RDTs EQA programme to help address some of the challenges faced by other LMICs. HTS is expanding beyond laboratory walls and HIV RDTs are increasingly performed by non-laboratory personnel and closer to the community. EQA programmes for HIV RDTs in Haiti have faced significant challenges. In expanded HTS settings, non-laboratory personnel (nurses, aid-nurses) involved in HIV RDT are usually undertrained and participate poorly in PT programs. In more than half of the lab enrolled in the PT programme in Haiti, the panels are always tested by the most experienced technician, defying the purpose of the program which is to evaluate the performance of the technician performing the test daily. EQA programme in Haiti and other LMICs are usually not tailored to address community HIV testing challenges. With decreased funding and absence of government financial commitment to HIV RDTs EQA programmes, more innovative and cost-efficient strategies are sought to ensure the quality of HIV diagnosis in LMICs. Qualified human resources, continuous training, supervision and community-tailored PT programmes remain key components for the success of HIV RDT quality management.
- human immunodeficiency virus
- rapid diagnostic tests
- external quality assessment
- proficiency testing
- HIV testing services
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0
Statistics from Altmetric.com
- human immunodeficiency virus
- rapid diagnostic tests
- external quality assessment
- proficiency testing
- HIV testing services
Summary box
HIV rapid diagnostic tests are instrumental in scaling-up HIV testing services in low-income and middle-income countries.
HIV misdiagnosis is a growing concern in Haiti in the era of expanded and decentralised access to HIV testing services.
Quality assurance programme such as proficiency testing for HIV Rapid diagnostic tests is a priority in resource-limited settings to guarantee the accuracy and reliability of the patients’ result, to assess the performance of laboratories performing HIV rapid testing and the competence of the analytical personnel.
Challenges for proficiency testing programme for HIV diagnostic tests in Haiti included panels being tested by the same laboratory technicians every time, non- lab professionals participating poorly in the programme and lack of focus on ensuring the quality of HIV tests performed at community level.
The adoption of a national laboratory policy, trained and skilled human resources, organised and regular laboratory supervision can help address the challenges to improve the quality of HIV rapid testing in Haiti.
Background
With the introduction and scale-up of ‘Test and Treat’ approach for care and treatment in most countries affected by the HIV epidemics, a stronger focus on the quality of HIV testing services (HTS) is of paramount importance.1 HTS is the gate to care and treatment services and quality management programmes to ensure the accuracy of every HIV test result is critical. HIV rapid diagnostic tests (RDTs) have been instrumental in scaling-up HTS in low-income and middle-income countries (LMICs).2 3 The WHO prequalified HIV RDTs show great performance with high sensitivity and specificity, and all countries using RDTs for HIV diagnosis should use combination of RDT’s (HIV algorithm) to add another layer of reliability and confidence on the final results.2
Haiti adopted a testing algorithm based on two sequential rapid tests: Abbott Determine HIV1/2 (Abbott Laboratories, Abbott Park, Illinois, USA) for use as a screening test and one Uni-Gold HIV-1/2 (Trinity Biotech, Wicklow, Ireland) for use as a confirmatory test (figure 1).4 As recommended by WHO, all positive cases are retested prior to starting antiretroviral therapy (ART) using the same algorithm with a second specimen and ideally by a new laboratory technician to verify their HIV-positive status.5

Rapid HIV testing algorithm used in Haiti. LNSP, National Public Health Laboratory; DBS, Dried Blood Spot.
Despite the great performance of most HIV RDTs, the literature is rich with reports on poor quality of HIV testing. Limitations of the assay itself, operator-related errors, inappropriate storage of reagents, inadequate training and lack of supportive supervision among other factors have been cited to lead to poor HIV diagnosis.2 6 Haiti is not immune to the issue of HIV misdiagnosis. The HIV sentinel sero-surveillance report on pregnant women in 2012 showed significant discrepancies between results from participating sites and the National Public Health Laboratory (French acronym LNSP); about 72% of the sites enrolled on this study had discrepant results.7 This report sounded the alarm on the need to reinforce the quality assurance of HIV RDTs.
The laboratory network in Haiti has a pyramidal-tiered structure. LNSP is at the top of the pyramid and serves as a reference laboratory, overseeing and coordinating the activities at the three levels of services. Three regional laboratories are located at teaching hospitals where a comprehensive range of laboratory services are provided and seven laboratories located at departmental hospitals constitute the third and second tier, respectively.8 About 240 primary level, peripheral public healthcare facilities/laboratories form the bottom of the pyramid, where basic laboratory tests are performed. Each tier has specific testing menu, but HIV RDTs are performed at all tiers. LNSP was inaugurated in 2006, and HIV RDT quality assurance was one of the first activities that defined this new organisation.
HIV quality assurance involves multiple phases and processes to ensure that the end result (the patient HIV serological status) is accurate. One key activity for HIV RDT quality assurance process is the external quality assessment (EQA). WHO defines EQA as a system for objectively checking the performance of a testing site (including the testers and the system used for testing) using an external agency.9 EQA components include proficiency testing (PT), retesting and on-site evaluation. Since Haiti adopted the 2015 WHO recommendation to retest all HIV-positive individuals before enrolment on ART, retesting is no longer recommended as part of an EQA scheme.10
PT is defined as interlaboratory comparisons that are organised regularly to assess the performance of analytical laboratories and the competence of the analytical personnel.11 PT is a key indicator for health system, to be reported annually for all US presidents’ Emergency Plan for AIDS Relief (PEPFAR) supported countries.12 On-site evaluation is critical to address PT poor performance, to directly observe and obtain a realistic picture of laboratory practices under routine conditions and provide on the jobs training and technical assistance to improve the quality of the testing.10 EQA is implemented in multiple LMICs as part of their HIV quality management programme with variable level of challenges and success. Here we present the lessons learnt, challenges and opportunities from 11 years of HIV EQA implementation in Haiti.
The HIV EQA/PT programme in Haiti
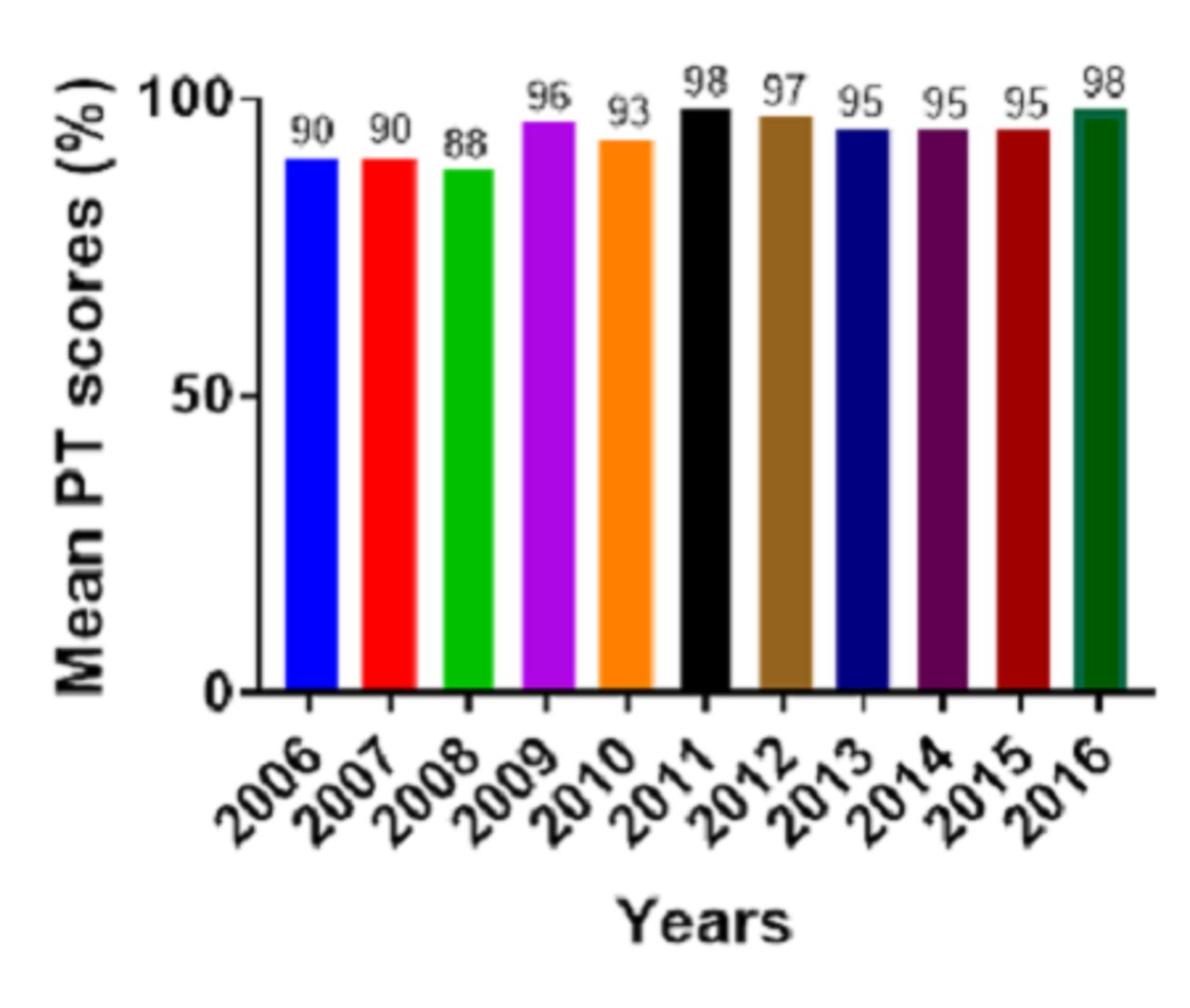
Sponsored by PEPFAR, the PT programme started in 2006 with 76 laboratories enrolled. In 2016, 208 laboratories (163% increase) participated in the biannual HIV PT programme in 2016 (table 1). Dried tube specimens (DTS) were prepared at LNSP from discarded and deidentified units of blood collected from the national blood transfusion centre according to the method described by Parekh et al.13 Six DTS were sent twice a year to laboratories across the countries for testing and the results are sent back to LNSP for data analysis and feedback.4 14 For each shipment of the PT panels, participants were given written standard operating procedures to process and test the DTS PT panels and were asked to report their results to LNSP by an established due date. Departmental technologists, which are laboratory technologist hired by LNSP and based at each of the 10 geographic departments in the country, are responsible to distribute the PT panels and collect the results. Laboratories with PT scores <80% were targeted for on-site technical assistance. Participation response rates across laboratories ranged from 86% to 98% (table 1). Decline in participation rates was due mainly to two major natural disasters (2008 Atlantic hurricane season and 2010 earthquake) and major administrative changes at LNSP in 2016 as previously reported.4 The results of the HIV PT programme from 2006 to 2017 showed an average score >90%, which tends to indicate a good performance for HIV RDTs at the sites (figure 2). However, one question capturing the challenges and limitations of the PT programme is how much of the quality of routine HIV RDT in the field is captured by the laboratories’ PT scores?
Participation in Haiti’s national HIV external quality assessment programme from 2006 to 2016
{kind=link}
{kind=link}
Average proficiency testing (PT) score for laboratories participating in Haiti’s national HIV external quality assessment programme from 2006 to 2016.
Challenges for HIV EQA in Haiti
PT panels being tested by the same laboratory technicians every time
In Haiti, one set of six DTS is sent to every participating laboratory for testing, and sites scoring 100% receive certificates of performance. In most laboratories in Haiti, HIV RDTs are performed by multiple technicians, usually rotating services, and not all of them are formally trained or certified to perform the test. Multiple reports have demonstrated that non-trained technicians perform poorly on HIV PT programme and are more prone to HIV misdiagnosis.15–18 In addition, the PT panels are usually tested by the most experienced technician in the lab or the lab chief every time, defying the purpose of EQA which is to evaluate the performance of the technician performing the test daily. We randomly selected two laboratories from each of the 10 geographical departments from the last five years of the programme and looked at the frequency at which the same technician performed the PT panels over time. We found that in 53% of the laboratories, the same technician was testing the PT panels every year. As stated by Moodley et al.: ‘Reliability of HIV rapid tests is user dependent’19 and so should be the PT programme in assessing individual technician performance. Learning from this experience, starting in 2014, LNSP has strengthened the process to ensure that PT panels are tested by all laboratory personnel performing HIV RDTs in PEPFAR supported sites. During trainings and sites supervision, LNSP reiterated the importance for every laboratory technician performing HIV RDTs to actively participate in the PT programme. However, one major challenge is the availability of panels in sufficient quantity to assess all lab personnel performing HIV RDTs. To address this challenge, LNSP assigned several laboratories to each departmental technologist during each PT round to supervise the PT testing and ensure that different technicians perform the test at each round.
PT testing for non-lab professionals in expanded HTS
HIV RDTs are quick, easy-to-use, reliable on-site antibody testing. These characteristics of HIV RDTs led to task-shifting from more specialised to less specialised health workers, including non-laboratory personnel such as lay counsellors and nurses.14 18 20–22 In Haiti, HIV RDTs are performed not only by laboratory technicians but also by nurses and aid-nurses who also conduct the HIV pre-counselling and post-test counselling. One of the major benefits of that strategy is the reduction in patients’ waiting time.22 In 2016, 12 major hospitals had their HIV RDT performed at 40 HIV testing points outside the laboratory, and these tests are usually performed by nurses and aid-nurses. These 40 expanded HTS services represented 27% of the sites participating in the National PT programme and tested around 145 000 patients, which represented 11% of the total HTS for 2016.23 These non-lab professionals who perform HIV RDTs are usually not trained or have received limited on-the-job training from trained laboratory technicians. In addition, most of them do participate in the national HIV PT programme and send the PT panels to the laboratory for testing when they receive them. The suboptimal accuracy level of HIV RDTs when used by non-laboratory personnel20 highlights the need for ongoing training, supervision and quality assurance for all level of personnel involved in HTS.
EQA and PT in the context of community testing for HIV
WHO recommends making HTS available through a wide range of approaches, both in facilities and in the community.24 Multiple studies have demonstrated that bringing HTS directly to communities resulted in substantial increase of HIV testing uptake and case detection rate.25–27 HIV RDTs have played an instrumental role in decentralising and increasing access to HTS through community-based services. In most LMICs, in addition to laboratory personnel, lay providers and community nurses are key actors to HTS decentralisation. In rolling out of HIV RDTs in the community, quality assurance programmes to ensure the quality of community HIV rapid testing should also be implemented.17 Ensuring the quality of HIV RDTs may be more challenging in community settings and the sensitivity and specificity of HIV point-of care testing may be affected by user training and competency and the testing environments.28–30 Other challenges to implement community HIV testing in Haiti are structural barriers: it can be difficult to create a private, confidential, clean and comfortable area for testing away from the community crowd. Given the difficulties to find adequate space for testing in the community, the quality controls are often neglected. Because of these structural barriers, LNSP recommend to screen patients using only HIV Determine test, and to refer HIV Determine reactive patients to the closest laboratory to repeat the testing using the national algorithm. Unfortunately, many patients with a reactive HIV Determine test never showed up to repeat their test which is a lost opportunity for the care and treatment programme. National EQA and PT programme should be tailored to address community HIV testing challenges. In Zambia, PT was conducted during the 2014–2016 community-randomised trial, investigating the impact of a combination HIV prevention package on HIV incidence; the results of the PT showed a performance score of 94% for community HIV-care providers and follow-up sites supervisions lead to the detection of 120 HIV RDTs discrepant results compared with the laboratory-based HIV test method used.28 Haiti has no guidelines yet for monitoring the quality and accuracy of HIV RDTs in community settings. Non-laboratory personnel should also be a target for the Haitian HIV PT programme, they should be trained on HIV RDTs, participate in the testing of the PT panels and be regularly supervised in the field.
Opportunities to improve HIV rapid test quality management system in Haiti
National laboratory policy
The 2008 Maputo declaration on strengthening of laboratory systems called for a national laboratory policy that is linked to the development and implementation of a national strategic plan to define and regulate laboratory activities in LMICs.31 The government of Haiti has not yet approved a national laboratory policy within their national health development plan. The Haitian national laboratory policy document has been developed and once approved will clearly state the government's vision and commitment to strengthen governance and leadership in the laboratory sector. The laboratory policy will also set the legal and regulatory framework for laboratory licensing, certification and accreditation to improve national quality management system, which is a critical step for HIV RDT quality improvement. Once the laboratory policy is approved and implemented, laboratory technicians will be required to be trained prior to perform HIV RDT and be certified annually which can add another layer to the quality assurance process.
Human resources
There is a lack of skilled laboratory professionals at every level of the Haitian laboratory network. In June 2016, the Haitian Ministry of Health and Population (French acronym MSPP) published a list of only five authorised laboratory schools in Haiti.32 In 2010, a new curriculum for laboratory science was developed to upgrade the national laboratory schools’ system from a 2-year training programme to 4 years leading to a bachelor’s degree; however, resource limitations have hampered the full implementation of the new curriculum. In 2011, the Merieux Foundation, in collaboration with LNSP and the Catholic University of Lyon, France, implemented a postgraduate programme for in-service laboratory technicians to upgrade their training to a bachelor degree level; from 2011 to 2016, 112 laboratory technicians benefited from this programme.33 These new graduated technicians are playing key roles as laboratory chiefs, quality managers and laboratory specialists to help improve the laboratory quality management system in Haiti.
Site assessment and supervision
Because of the challenges and limitations of traditional ways of implementing quality assurance activities, WHO recommends innovative approaches to ensure high-quality testing.9 The creation of a quality corps network of trained volunteers (community-based quality champions) has been proposed to support quality assurance programmes.9 34 Haiti has implemented a slightly different approach since 2006, with mixed results. MSPP has recruited and extensively trained laboratory technicians to serve as quality officers in all 10 geographic departments of the country. These quality officers, called ‘Departmental Technologists’, have the responsibility to assess and audit the laboratories in their department using standardised tools developed by LNSP. They are also responsible to train laboratory technicians on different diagnostic techniques, and they actively participate in distributing PT panels to sites, collecting PT results, returning feedbacks and in providing corrective actions when necessary. In addition, every PEPFAR implementing partners is required to hire a laboratory specialist to supervise testing activities within their laboratory network. These laboratory specialists not only help in the implementation of quality assurance programmes, but they also assist with supply chain management by collecting and forwarding supplies and reagent consumption reports to the central supply chain management system. While in theory the combination of departmental technologists and laboratory specialists was expected to lead to significant improvements in the quality of laboratory testing, logistic difficulties and decrease in funding have challenged the extent of involvement of these specialists in the community to drive the required changes in quality assurance of HIV testing.
PEPFAR and Global Heath Security Agenda
The Haitian national laboratory network has grown and improved significantly with the support of PEPFAR. Hospital laboratories were either built or renovated, and the number of facilities with access to automated chemistry, haematology and tuberculosis (GeneXpert) testing tripled after the 2010 earthquake.8 The Global Heath Security Agenda (GHSA) offers another opportunity to strengthen the Haitian laboratory system to support infectious diseases surveillance and outbreaks response. The same way PEPFAR help strengthen laboratory capacity beyond HIV diagnostics, GHSA can allow capacity building that can benefit multiple laboratory activities for stronger care and treatment programmes; but the financial commitment of the Haitian government remains crucial to sustain the gains and help face the challenges. Haiti joined GHSA in 2015, a roadmap development process has been initiated with the Pan-American Health Organization support in collaboration with other ministries, local and global partners, to identify and strengthen sustainable programmes, policies and capacities to prevent, detect and respond to human and animal infectious disease threats.
Conclusion
Accurate laboratory diagnosis is essential to the prevention and treatment of disease. Traditional programmes to assess quality of laboratory testing must consider the changes in programme management that aim to provide healthcare services closer to the community. EQA programmes for HIV RDTs must not only target all laboratory technicians involved in testing regardless of the setting but also acknowledge the increasing role of community nurses, field agents and other lay providers in providing HTS. HTS is expanding beyond laboratory walls and HIV EQA programmes must find innovative strategies to tailor the trainings, assessments, supervision and PT panels to reflect the reality of the field. In a context of limited resources, the Haitian Ministry of Health and its partners are to work collaboratively to design efficient and sustainable strategies to expand EQA and continuously improve the quality of laboratory diagnosis in Haiti.
References
Footnotes
Handling editor Stephanie M Topp
Contributors FJL conceived the paper and led the drafting of the manuscript; MLE, RA, JB, JB, MS and JWD reviewed and provided critical input on each draft of the manuscript.
Funding This research has been supported by the President’s Emergency Plan for AIDS Relief (PEPFAR) through USAID Haiti under the terms of EQUIP- AID-OAA-A-15-00070.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The datasets used and analysed during the current study are available from the corresponding author upon request.