Article Text

Abstract
Background Healthcare is under attack in Syria with repeated air strikes on hospitals and ambulances and the largest death toll of health workers in any recorded conflict.1 Ambulances in Syria have been bombed, shot at, stolen, looted and obstructed, significantly impeding their ability to safely evacuate the wounded and provide medical aid.
Methods This article presents the summary of a literature review on attacks against ambulances in Syria from 2011 to 2018, as well as a descriptive secondary data analysis on individual attacks reported by the Syrian Network for Human Rights from January 2016 to December 2017. A peer-reviewed literature search included three databases (PubMed, ProQuest and Embase), and a grey literature search included reports from groups involved in the Syrian health response or human rights monitoring.
Findings From 2016 to 2017, there were 204 individual attacks involving 243 ambulances. Half (49%) were either heavily damaged or put out of service. The main perpetrators were the Syrian regime (60%) and the Russian armed forces (29%). Half (52%) of ambulances were directly targeted. The peer-reviewed literature search yielded 18 articles, from which the following themes were drawn: targeting of ambulances, ‘double-tap’ attacks, delays to care, obstruction and other forms of violence, and long-term consequences.
Interpretation Ambulances have been intentionally and repeatedly targeted throughout the Syrian conflict as part of a war strategy. Real challenges in monitoring and systematically tracking attacks on ambulances exist, but as a result, they are understudied and likely under-reported.
- syria
- ambulance
- violence
- attacks
- health
- medical transport
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0
Statistics from Altmetric.com
Key messages
What is already known?
There have been well-documented and systematic attacks on health facilities and healthcare workers in Syria.
Ambulances are also frequently targeted in conflict settings, but there are few reports characterising the violence against ambulances and prehospital providers.
What are the new findings?
Of the ambulances in Syria which sustained damage from attacks, half of them were specifically targeted and half were severely damaged or put out-of-service. Other forms of violence, including obstructing, looting and stealing ambulances, are likely much more widespread than what is recorded.
What do the new findings imply?
This review highlights the intentional, highly destructive and repetitive targeting of ambulances, which leads to delays and inability to access medical care.
Introduction
Now in its eighth year of conflict, Syria is known as the most dangerous place to work for healthcare providers with attacks on health personnel and health infrastructure disturbingly commonplace. In 2017, Syria had the most cases of violence against healthcare than all other countries with ongoing conflict.2 This ‘weaponisation of healthcare’ turns the essential need for healthcare into a war tactic that aims to destabilise, intimidate and demoralise.1 3 Attacks against healthcare include bombing hospitals, kidnapping health workers, looting health centres and blocking ambulances.
Ambulances have a critical role to play in armed conflicts by evacuating the wounded, providing life-sustaining treatment and transporting patients to hospitals. In Syria, prehospital services provided by ambulances and paramedics have been targeted since the beginning of the conflict.1 The first reported deliberate attack on an ambulance was in September of 2011 when a clearly marked Red Crescent ambulance was ambushed at a government checkpoint in Homs, killing one paramedic and injuring three others.1 4 WHO reported that by 2013, around 78% of ambulances were damaged and 52% of them were not functioning.5
Tracking and recording attacks on healthcare is challenging due to insecure areas, remote locations and non-standardised definitions and reporting methods.2 6–8 Moreover, attacks on ambulances are likely under-reported and understudied. In Syria, many of the groups actively documenting attacks on healthcare (Physicians for Human Rights, Violations Documentation Center in Syria, Syrian American Medical Society, WHO’s Surveillance System of Attacks on Healthcare) either do not systematically track attacks on ambulances or have limited ambulance-specific data.6 Instead, most databases focus on attacks against hospitals and/or personnel.
Ambulances and paramedics are arguably more vulnerable to violence than other healthcare entities. From March 2011 to September 2016, paramedics were the third largest cadre of health workers to be killed (after physicians and nurses).1 Ambulances are mobile and highly visible within the community, subject to curfews and pass through multiple military checkpoints. Their on-scene presence after an attack makes them susceptible to ‘double-tap’ attacks, where a location is bombed twice several minutes apart with an intention to target first responders.
Similar to health facilities, ambulances are protected under International Humanitarian Law and the Geneva Conventions.9 10 While attacking an ambulance is a war crime, blatant disregard for these protections continue in Syria. The UN Security Council passed Resolution 2286 in 2016 which condemns attacks on medical facilities and personnel. Despite the resolution, the International Committee of the Red Cross (ICRC) documented over 1200 incidents in 16 countries of attacks on healthcare in the subsequent 2 years.11 12 Many groups have started advocacy campaigns like Medécins Sans Frontières’s (MSF) Medical Care under Fire, ICRC’s Health Care in Danger and Safeguarding Health in Conflict Coalition to raise awareness and continue placing pressure on international governing bodies. Globally, the number of incidents is rising despite increased attention.
In most complex emergencies, consistent data collection of individual attacks in granular detail is impossible. Syria is unique because unlike most conflict-ridden countries, it had a high-middle-income preconflict infrastructure with widespread prevalence of smart phones and cellular connectivity. The Syrian Network for Human Rights (SNHR) uses this connectivity to track violations against the Syrian people and attacks on healthcare.13 Their methodology involves gathering eyewitness accounts through an extensive network of contacts around the country.14 They attempt to link incidents with several first-hand accounts and often include photo documentation of the damaged ambulance and/or health facility. They are one of the few groups that routinely collect detailed data on attacks on ambulances.
Ambulances play an integral role in the healthcare system in conflict settings, and continuous attacks on ambulances have disastrous impacts on mortality, access to healthcare and morale of a population. This review attempts to characterize the disturbing yet ongoing targeting of ambulances in Syria since the start of the conflict.
Methods
This article presents the summary of an in-depth literature review on attacks against ambulances in Syria from January 2011 to August 2018, as well as a descriptive secondary data analysis on available reports by the SNHR from January 2016 to December 2017.
For this review, we used the ICRC definition of ‘ambulance’: “A locally available means of transport that carries, as safely and comfortably as possible, wounded and acutely sick persons to a place where they can receive the emergency medical and/or surgical care they need; it is also where the condition of these patients is stabilized”.15 The term ‘medical transport’, which according to the ICRC can encompass medical ships or aircraft, was not used given the focus of this paper. However, this also excluded private vehicles, civilian motorbikes and other means of personal transport that may be used.
Secondary data analysis
SNHR publishes monthly reports on ‘Violations against the Health Sector’ and ‘Attacks on Vital Facilities’, which include attacks against ambulances. Secondary data analysis involved a thorough scoping of the primary data that are publicly available from January 2016 to December 2017 on the SNHR website. These reports provide details of individual attacks on ambulances (as well as other structures and personnel) including the date, location, mechanism of attack, perpetrator, damage to the ambulance, the controlling faction in the location of the attack, and whether health workers or civilians were injured or killed. Individual events were extracted from these reports into an Excel spreadsheet and analysed.
Literature review
The literature review consisted of both primary and secondary data collection, including peer-reviewed journal articles, commentaries in peer-reviewed journals and other grey literature sources. We conducted a search on PubMed, ProQuest and Embase databases with the following inclusion and exclusion criteria (see online supplementary file 1).
Supplemental material
Custom date ranges were used to exclude events before 2011 (the start of the Syrian conflict). See online supplementary file 2 for an example of the search strategy used. Due to an overall low number of articles that met our initial search strategy focusing on ambulances, the search was widened to include general healthcare keywords during the abstract review stage. The search was run for all databases in the first week of August 2018.
Supplemental material
All abstracts were screened by two researchers, and discrepancies in the inclusion and exclusion of abstracts were discussed until consensus was reached. Abstracts were collected and organised using citation software Zotero. Full texts were also reviewed by two researchers.
We searched grey literature by browsing websites and published reports by organisations involved in the provision of care in Syria, organisations that report on violations in Syria related to health, and UN agencies. These included the websites for Syrian Civil Defense (White Helmets), Physicians for Human Rights, WHO’s Surveillance System of Attacks on Healthcare, Syrian American Medical Society (SAMS), Human Rights Watch, SNHR, ICRC, Safeguarding Health in Conflict Coalition, Amnesty International, MSF, United Nations Office for the Coordination of Humanitarian Affairs and several others.
Results
Secondary data analysis
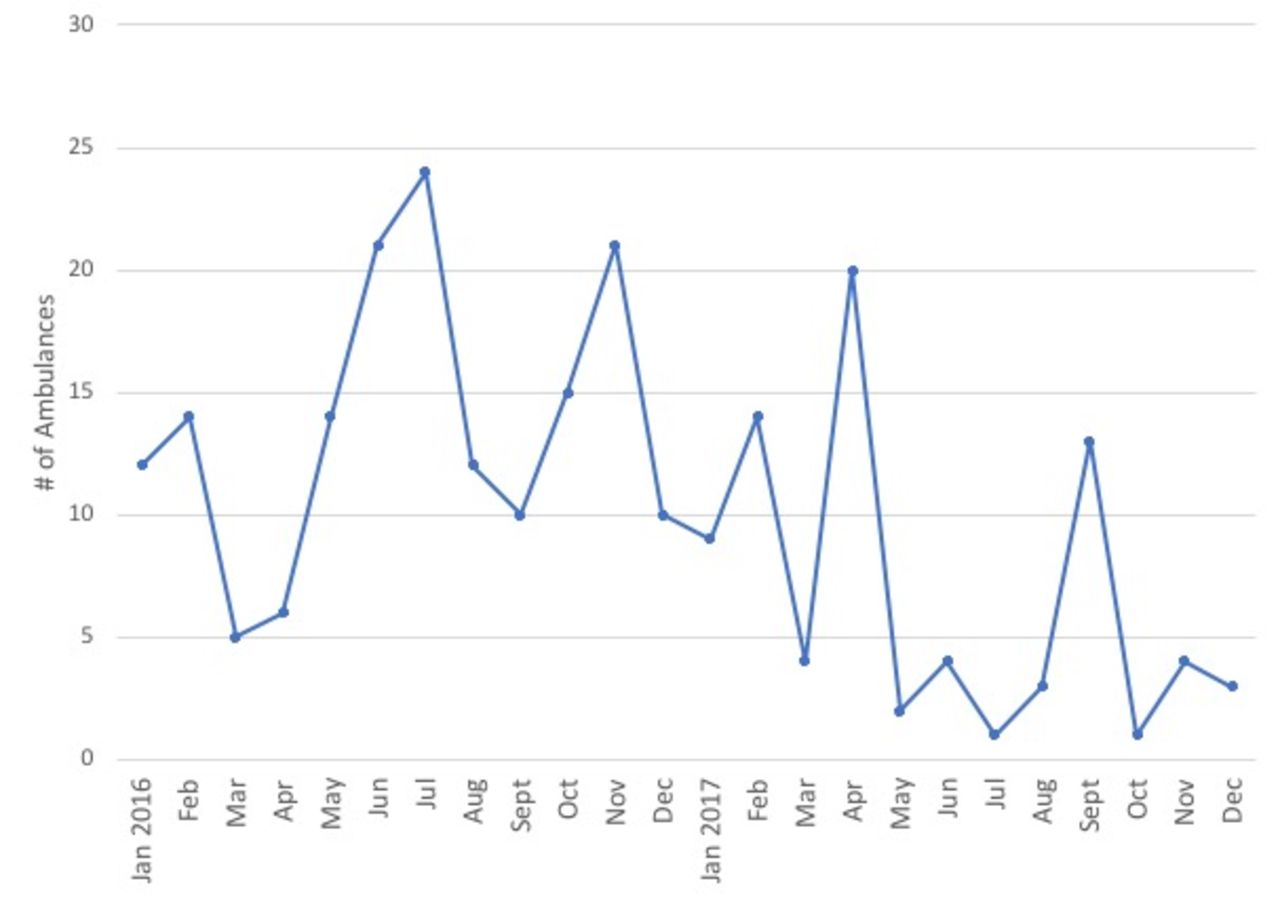
According to the SNHR database, from January 2016 to December 2017, there were 204 attacks involving 243 individual ambulances (see figure 1). Overall, there were fewer attacks involving ambulances in 2017 (62) compared with 2016 (142).

Attacks on ambulances per month according to the Syrian Network for Human Rights.
The majority of attacks on ambulances in 2016–2017 occurred in Aleppo, Idlib and Damascus governorates (figure 2). These are areas which have large armed opposition-controlled factions. The primary aggressor was the Syrian regime with 123/204 (60%) incidents of attacks as recorded by SNHR. The second highest was attributed to Russian forces with 60/204 (29%) attacks (table 1).
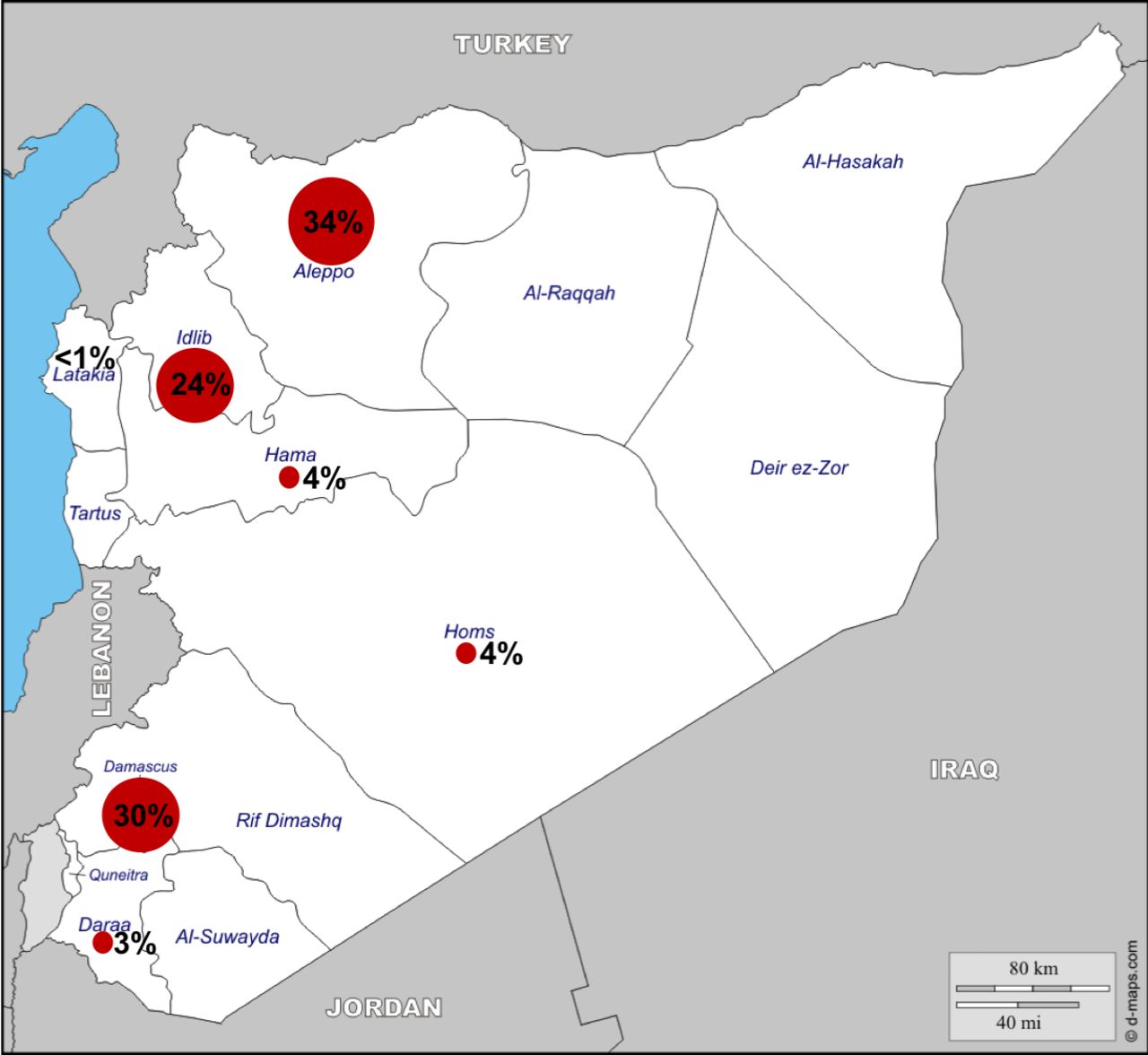
Map of ambulance attacks 2016–2017 (n=204 incidents, Syrian Network for Human Rights data).17 28
Perpetrator of attacks on ambulances (n=number of incidents, Syrian Network for Human Rights data)
The majority of attacks occur in areas controlled by the armed opposition (79%) or the armed opposition and the Fatel Al Sham Front (8%), an Islamic extremist group, with a base in Idlib governorate in 2016. Only 1%–2% of the attacks on ambulances occurred in pro-government areas (table 2).
Controlling group at the location of the attack (n=number of incidents, Syrian Network for Human Rights data)
The most common modality of attacks on ambulances were air-to-surface missiles and shelling in 2016–2017 (table 3). Weaponry commonly employed by the Syrian government and Russian forces include cluster bombs and barrel bombs. Cluster bombs scatter submunitions or bomblets over a wide area that leave unexploded remnants in the ground that become landmines. Barrel bombs are unguided, large drums filled with metal fragments and explosives with a massive blast radius.
Mechanism of ambulance attacks 2016–2017 (n=number of ambulances, Syrian Network for Human Rights data)
When an ambulance was involved in an attack, 49% of them were either heavily damaged or put out-of-service (figure 3). Only 12% of ambulances sustained ‘mild’ damage and were immediately usable. ‘Out-of-service’ implies that the vehicle sustained significant damages and needed major repairs, or it had to be replaced.
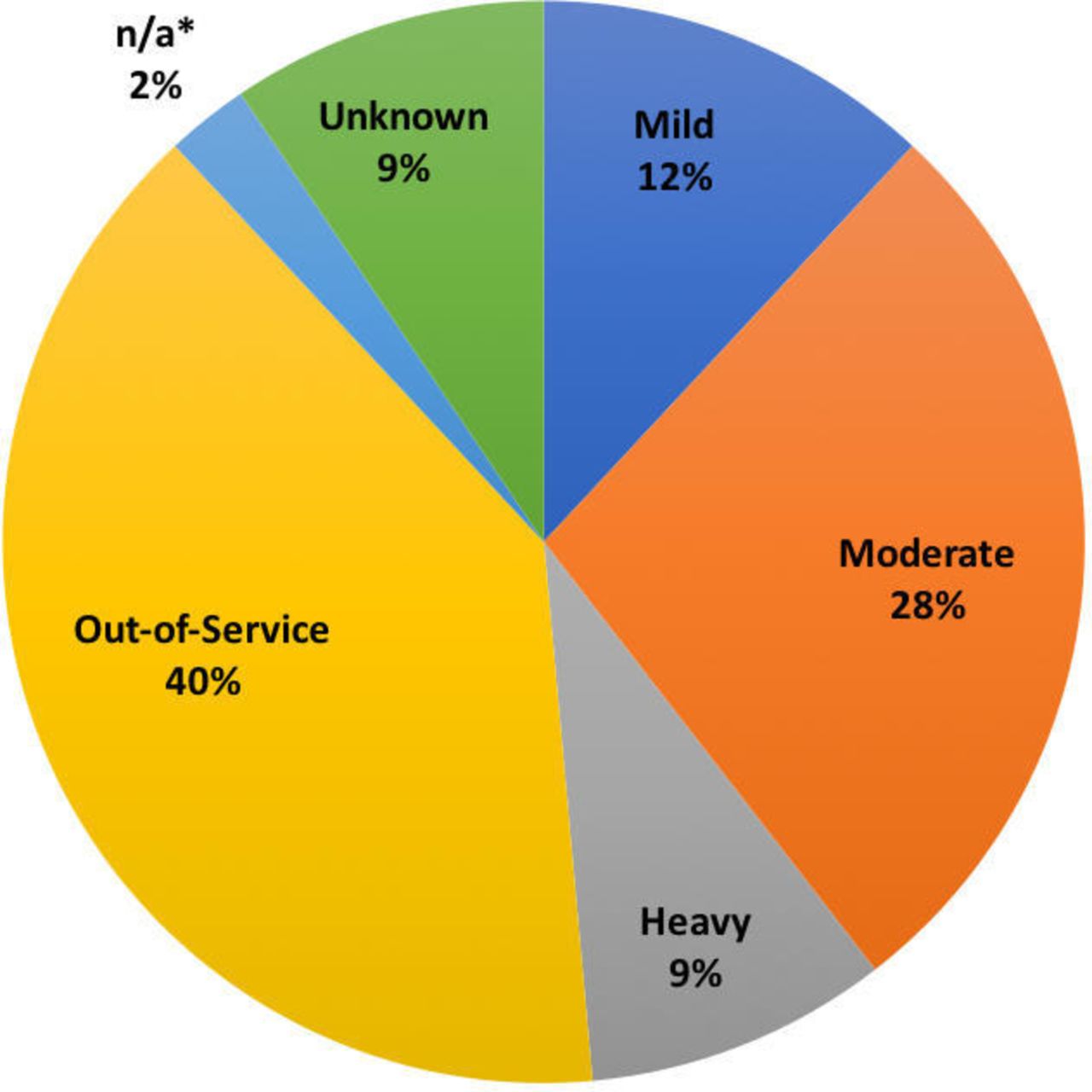
Degree of damage sustained to ambulances 2016–2017 (n=243 in number of ambulances, Syrian Network for Human Rights data). *n/a, not applicable (ambulance stolen).
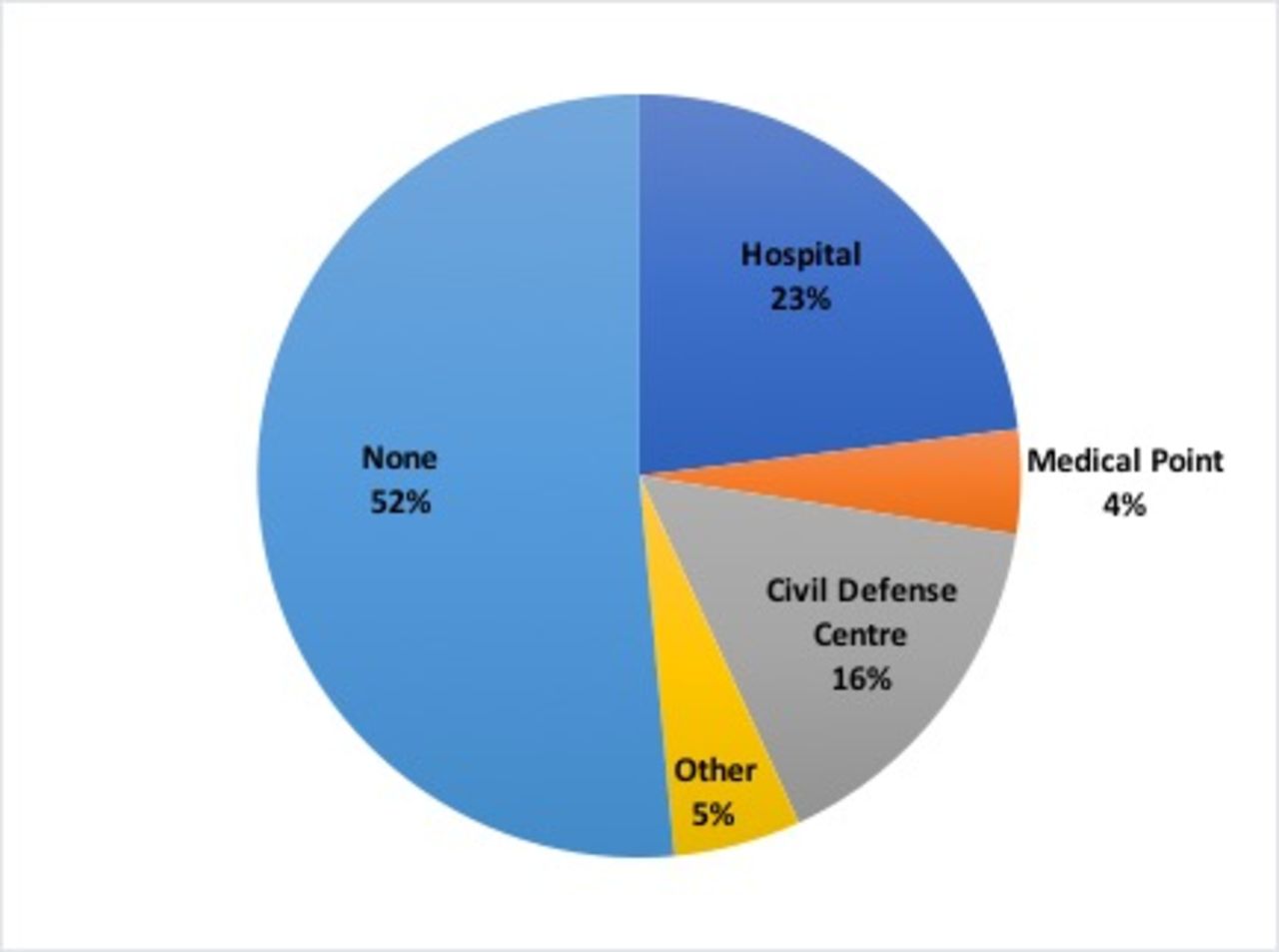
Around half of all attacks involving ambulances included other structures, mostly hospitals and civil defence centres (figure 4). Syrian Civil Defense (White Helmets) are a group of volunteer rescue workers with bases and ambulances stationed throughout the country in primarily opposition-controlled areas. In the SNHR reports, often a specific hospital, medical point or civil defence centre was targeted, and the ambulance was parked nearby. The other structures which were targeted included residential buildings, internally displaced persons and refugee camps, non-governmental organisation buildings and bakeries.
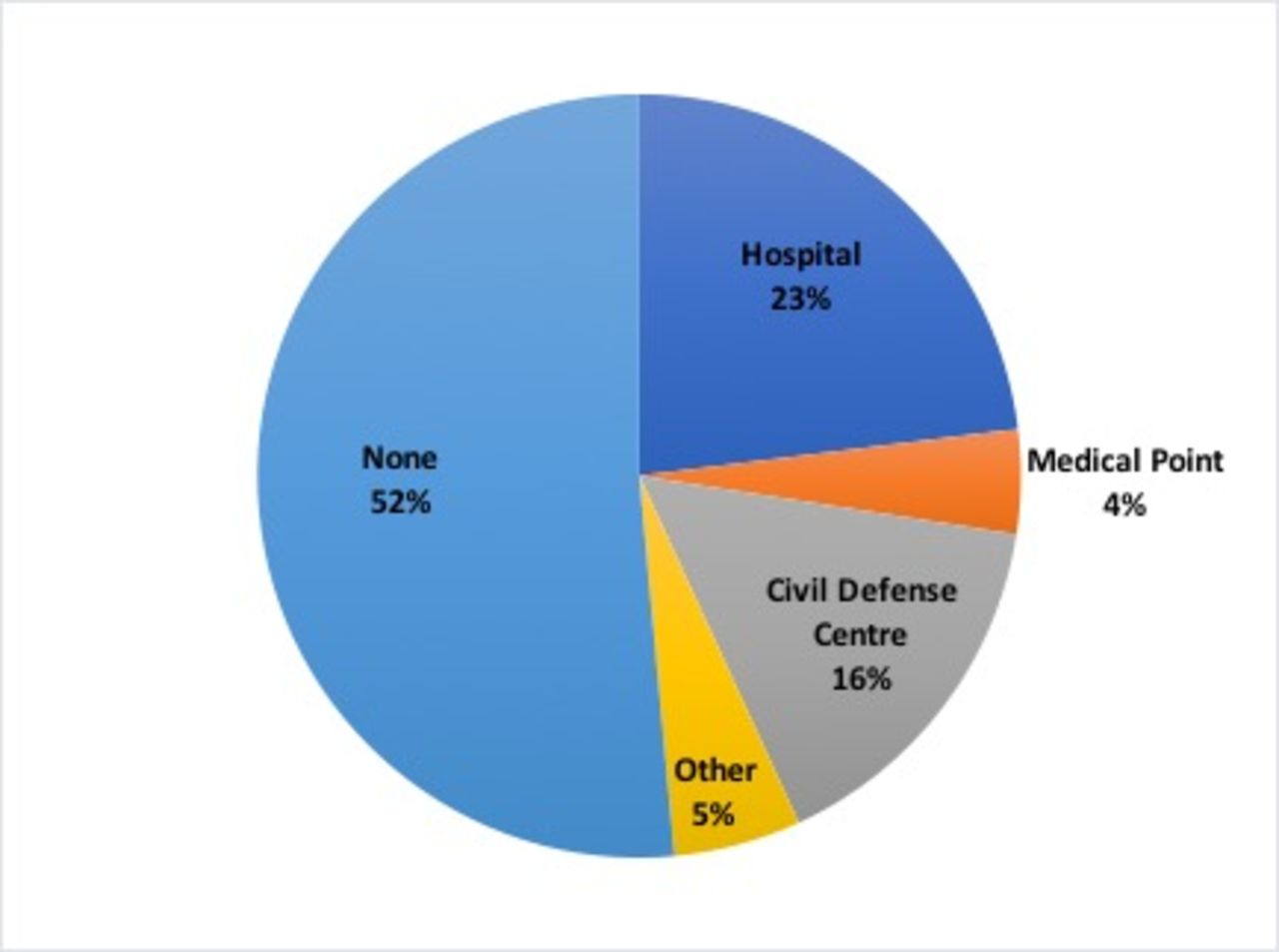
Attacks involving other structures 2016–2017 (n=204 in number of incidents, Syrian Network for Human Rights data).
Literature review
The literature review yielded 991 results which were screened and of which, 18 were included in the review (figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Literature review flowchart.
Themes were drawn from these 18 articles as well as from the grey literature review. The themes included targeting of ambulances, ‘double-tap’ attacks, delays to care or lack of access, obstruction and non-physical forms of violence, and both short-term and long-term consequences of attacks on ambulances (online supplementary file 3).
Supplemental material
Double-tap attacks
One insidious strategy used by the Syrian regime and Russian forces is the ‘double-tap’ attack. ‘Double-tap’ or ‘follow-up’ attacks occur when there is a delayed second strike on the same area. The Syrian Civil Defense (White Helmets) reported experiencing 149 double-tap attacks in 2016 alone.16 One ambulance system manager in Aleppo said, “Once rescue teams reach the area, warplanes hit the same spot for the second time, which leads to higher numbers of wounded and killed, and more ambulances damaged”.17 In 2016, an air strike hit a school and residence building nearby the MSF-supported al-Quds Hospital in East Aleppo. Several minutes after the wounded were transported into the emergency department, the hospital was assaulted by two additional air strikes 5 min apart, killing 55 people and damaging the hospital’s ambulances and infrastructure.18
Delay to care
A downstream consequence of ‘double-tap’ and other forms of attacks are delays to care. First responders are more inclined to wait until an area is deemed secure before entering a building after an air strike. This delay could have grave consequences for the wounded. Members of the Syrian Civil Defense (White Helmets) and other first responders face the difficult decision of weighing their own safety with the time-sensitive nature of life-threatening injuries.
Delays to care also result from a general lack of functional ambulances available to retrieve patients.17
Obstruction of ambulances
An ICRC study in 11 countries between 2012 and 2014 reported 426 acts of violence against ambulances including threats, denying access, delays, robberies and hijacking ambulances.19
Physical destruction of ambulances may be easier to track and visually confirm; however, other forms of violence are common in Syria. These include blocking or obstructing ambulances, restricting movement at night via curfews, and looting or stealing ambulances.7
Short-term and long-term consequences
The short-term and long-term consequences from attacks on ambulances are numerous, although this type of data is not routinely recorded or studied. Taken from many first-hand accounts, there is an overall demoralisation and loss of confidence when an ambulance is delayed or does not arrive. Additionally, the repeated assaults and disregard for medical neutrality have led some humanitarian actors, like MSF, to pull out of certain areas.20 SAMS, a medical relief organisation, noted that with the restrictions placed on ambulances and fear associated with travelling at night, maternal mortality is rising in Syria.21
Discussion
The SNHR data suggests that attacks on ambulances are relatively common but decreasing between 2016 and 2017 (figure 1). Perhaps this can be attributed to increased attention and mounting international pressure to protect medical neutrality in Syria. However, the spikes in attacks during July and November of 2016 may correspond to the sieges in east Aleppo with widespread aerial bombardment campaigns throughout the city.22 It is too soon to tell if the overall number of attacks will continue to down-trend.
While the most common modality for attacks are air-to-surface missiles and shelling, the use of cluster and barrel bombs are significant because of their high degree of indiscriminate and widespread destruction (table 3). They likely contribute to the large number of ambulances that become collateral damage during an attack on a hospital, for example. Cluster bombs were prohibited in 2008 by the Convention on Cluster Munitions.23 The majority of attacks occur in opposition-controlled areas and are perpetrated by the Syrian regime and Russian armed forces (tables 1 and 2). Taken together, this demonstrates the regular and intentional disregard for international treaties on medical neutrality by the government.
In general, the attacks that involve ambulances are highly destructive where half of them are heavily damaged and/or put out-of-service (figure 3). The disturbingly common tactic of ‘double-tap’ attacks may contribute to these high numbers. ICRC affirms that double-tap attacks are a deliberate and direct assault on first responders and paramedics.15
The peer-reviewed and grey literature reviews reveal several themes underlying attacks on ambulances in Syria. These include direct targeting of ambulances, ‘double-tap’ attacks, delays to care and/or lack of access, obstruction and other forms of violence, and short-term and long-term consequences. Violence involving ambulances is relatively common in Syria. In fact, it is often cited by journal and newspaper articles to demonstrate the gravity of the Syrian health crisis and repeated violations of the Geneva Conventions. However, there is currently an overall lack of focus and research on this important topic. Even the most active human rights monitoring groups tracking attacks on healthcare in Syria, Physicians for Human Rights and the Violations Documentation Center, do not include attacks on ambulances.6 24
When ambulances are taken out-of-service, there are significant ramifications in exacerbating delays to care and ability to retrieve the wounded and sick, although these are hard to measure.
Without an ambulance, individuals may turn to personal cars and motorbikes to transport patients, which may place unnecessary risk to civilians.16 Humanitarian organisations also face significant logistic and financial strain to find replacement parts and repair the vehicles during times of active battle.17 Several anecdotal reports from humanitarian organisations suggest that these delays and other forms of violence are ubiquitous and have a significant impact on morbidity and mortality. They are likely under-reported but also under-studied.
Challenges to systematically collecting the full scope of attacks on healthcare include heightened security risks in conflict areas, inherent bias in data collection, inadequate funding and lack of established methodologies.3 25 In 2012, the World Health Assembly passed a resolution (WHA65.20) calling for WHO to take leadership in the collection and dissemination of data on attacks on healthcare.26 The WHO Monitoring Violence against Health Care programme (now part of Surveillance System for Attacks on Health Care) developed a reporting and tracking methodology which was piloted in Syria by the Turkey health cluster in 2015. Anonymous, real-time reporting through an encrypted online portal was recorded with follow-up verification and triangulation of each incident. However, during the pilot phase from November 2015 to December 2016, attacks on hospitals were verified in 60% of incidents reported, while only 26% of incidents involving ambulances were verified.26
Similarly, SAMS trialled an incident-based reporting mobile platform with field data collectors in four governorates Aleppo, Idlib, Homs and Hama in 2016. The SAMS mobile data collection tool found 35 incidences involving attacks on ambulances in 2016 whereas the SNHR data for the same four governorates reported 102 incidents.6 This significant discrepancy speaks to the challenges in accurate data collection in conflict settings.
Reporting bias is an important limitation to incident-based reporting mechanisms. Events involving greater physical destruction of property or associated mortality are more likely to be reported and verified.6 This grossly underestimates smaller-scale attacks and likely misrepresents the true incidence of attacks on healthcare (eg, a type 2 error). Additionally, standardised methodologies for monitoring and reporting is essential to prevent misuse and politically motivated manipulations of data.27
One important limitation of this manuscript is that while the secondary data analysis provides insight into the characterisation of attacks on ambulances in Syria, it only includes one dataset. The SNHR data have some shortcomings, which include variable reporting of attacks over time, lack of clearly defined methodologies and inconsistent definitions. However, SNHR currently has the most comprehensive, publicly available database of attacks on ambulances in Syria.
Conclusion
The intentional, highly destructive and repetitive targeting of ambulances throughout the Syrian conflict has had an immeasurable and devastating impact on the people of Syria and the healthcare system. As the most dangerous place in the world to be a healthcare provider, no cadre of health worker or health facility is immune to the attacks.
Monitoring and tracking attacks on ambulances and prehospital providers in these settings is challenging, but it is important that both non-governmental organisations and WHO continue to strive for collecting high-quality, standardised data. This is the first step to ensuring that these attacks on ambulances globally do not become normalised as ‘usual war-time tactics’.7 The UN Security Council and global humanitarian community must do more to protect the sacred space of medical neutrality in conflict and bring harsher punishments to perpetrators of violence against healthcare in Syria.
Acknowledgments
We would like to thank Les Roberts, Rachel Moresky and John Usseglio for their time and guidance.
Supplementary materials
Press release
Press release
Footnotes
Handling editor Seye Abimbola
Contributors CHW initiated the study and defined the initial research question. CHW and CY-TC developed the detailed methodology and carried out the literature review. CHW drafted the protocol, analysed the data and drafted the manuscript. All authors reviewed any doubtful papers. All authors critically reviewed the draft and approved the final version for publication.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.