Article Text

Abstract
Introduction High discontinuation rates of contraceptive methods have been documented in sub-Saharan Africa. However, little is known about gaps within individual episodes of method use, despite their implications for unintended pregnancies. The objective of this mixed methods study was to examine the prevalence of, and explore the factors contributing to, delays in repeat appointments for pills and injectables in Senegal.
Methods First, we constructed a longitudinal data set of women’s contraceptive consultations using routine records from 67 facilities in Senegal. Consultations for pills and injectables were classified as on time, delayed or with unknown delay status based on time since previous appointment. We described the prevalence of delayed appointments and used backward stepwise regression to build a mixed-effects model to investigate risk factors for delay. Second, we conducted workshops with family planning (FP) providers, and indepth interviews and focus group discussions with women of reproductive age, to explore factors contributing to delays.
Results Almost one-third (30%) of appointments for pills and injectables were delayed, resulting in risk of pregnancy. Previous delay, pill use, lower educational level, higher parity, third and subsequent visits, and Islamic faith were independently predictive of delays (p<0.04 for all). Although women’s ‘forgetfulness’ was initially mentioned as the main reason for delays by women and providers, examining the routines around appointment attendance revealed broader contextual barriers to timely refills—particularly widespread covert use, illiteracy, financial cost of FP services and limited availability of FP services.
Conclusion Delays in obtaining repeat pills and injections are common among contraceptive users in Senegal, exposing women to unintended pregnancies. Strategies to reduce such delays should move beyond a narrow focus on individual women to consider contraceptive behaviour within the broader socioeconomic and health systems context. In particular, effective interventions addressing low acceptability of contraception and appointment reminder strategies in high illiteracy contexts are needed.
- family planning
- contraception
- adherence
- discontinuation
- delay
- Senegal
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known?
High contraceptive discontinuation contributes to high unmet need in sub-Saharan Africa, and short-term gaps in method use have been documented in Malawi and South Africa.
What are the new findings?
Delays in obtaining repeat pills and injections are common in Senegal, exposing contraceptive users to pregnancy.
Widespread covert use, illiteracy, cost and availability of family planning services limit women’s ability to attend the facility on time.
What do the new findings imply?
Women who are most likely to have delayed appointments could be identified in health facilities and provided with additional support.
In the short term, innovative appointment reminder strategies should be tailored to contexts of high illiteracy and covert use.
Introduction
Pills and injectables are two of the most popular contraceptive methods in sub-Saharan Africa: more than half of contraceptive users relied on these two methods in 29 of 43 countries with Demographic and Health Survey (DHS) data.1 Among the advantages explaining their popularity, they are less invasive than longer acting methods and reversible without assistance from a health provider—a particular benefit in contexts where desired fertility is high and contraception is primarily used for spacing births, such as West Africa.2 3
However, one important constraint of pills and injectables is the need for regular refills to effectively protect against unwanted pregnancy. Women using progesterone-only injectables need a reinjection within 13 weeks,4 5 although they are not at risk of pregnancy until several weeks later.6 For pill users, the effectiveness period depends on how many pill packs—each covering one 28-day cycle—are provided, varying with setting and duration of use.
Senegal has experienced a rapid increase in modern contraceptive use in recent years, from 12% among married women in 2010–2011 to 23% in 2016.7 8 More than half of modern contraceptive users rely on injectables (35%) and pills (20%).8 The rates of unintended pregnancies are high in Senegal, with up to one-third of births estimated to be unplanned or unwanted.7 9 The extent to which the recent increase in contraceptive use will be translated into a reduction in unintended pregnancies depends in part on continuity of method use, including the extent of interruptions in use. Gaps in contraceptive coverage are particularly a concern for short-acting methods requiring regular refills by women, leading to more opportunities for lapses in adherence.
To date, much of the evidence on continuity of use relates to women discontinuing contraception altogether or switching to another method. High rates of discontinuation for method-related reasons (such as side effects) have been found for pills and injectables in low-income and middle-income countries,10 including Senegal where one-third of women discontinue their method within a year and unmet need is high after discontinuing.11 12 Much less evidence is available on gaps in continuity within the same episode of method use. Temporary discontinuation has been documented among inner-city adolescents in the USA and new contraceptive users in South Africa, with gaps lasting 7–8 months on average.13 14 Shorter term interruptions have also been demonstrated in the USA, where around half of women had delays in refilling prescriptions in the first 3 months after initiation.15
Few large-scale data sources of contraceptive appointments or refills are available in low-income countries. Calendar data—based on women’s self-reported contraceptive use month by month for the preceding 3–5 years, widely available in DHS—are poorly suited for analysing gaps in contraceptive use, since women may forget or not report them. Prospectively recorded data of the timing of contraceptive refills are needed to examine gaps in continuity, yet few longitudinal studies of contraceptive consultations have been conducted. In Malawi, only 51% of injectable users received their first reinjection within 13 weeks,16 and 16%–25% of women returned more than 2 weeks late for injections in South Africa,17 suggesting that delayed refills for short-acting methods may also be widespread in other sub-Saharan settings.
Moreover, reasons for any gaps in continuity are poorly understood. Women seeking to refill short-acting methods face a number of financial, geographical and other barriers to accessing contraception in sub-Saharan Africa,18 19 at every appointment. In South Africa, the most common reason for attending appointments late was conflicting work or family priorities, followed by forgetting and lacking transport or money.17 Qualitative evidence in particular is needed to further understand the reasons behind ‘missed appointments’ in other countries, including Senegal.
The recent rise in contraceptive use in Senegal is underscored by a large increase in the number of injectable and pill users. Existing barriers to family planning (FP) access in Senegal20 21 suggest that gaps in contraceptive continuity may be common there. Ethnographic data have also shown that despite global and national commitments, FP programmes in Senegal have sometimes failed to address the socioeconomic challenges faced by women in their everyday reproductive lives.22 Mixed methods studies are useful in gaining a fuller understanding of individual and contextual factors influencing contraceptive behaviour.23–25 The objective of this study is to examine the prevalence of, and explore the reasons for, delays in appointments for pills and injectables in Senegal, using a mixed quantitative and qualitative approach.
Methods
Study setting and design
Senegal counts 3.5 million women of reproductive age.26 The public health system follows a pyramid model, with the 14 regional medical offices overseeing the health centre and health posts in subregional districts.27 The vast majority of modern contraceptive users in Senegal obtain their methods from public facilities, including 77% in health centres and posts.8 FP providers in these facilities record each consecutive visit on the same consultation card for individual women. In addition, women are given an appointment reminder card with the next scheduled appointment date. FP products are sold at subsidised cost in public facilities, and women may also be charged for auxiliary products (such as syringes for injections).
This study used information collected for the evaluation of a supply chain intervention, the Informed Push Model, rolled out nationally in a staggered scale-up between 2012 and 2015. Under the Informed Push Model, third-party private logisticians were contracted to undertake stock inventories and distribute contraceptives to all public health centres and health posts in Senegal, with the aim of reducing contraceptive stockouts.28
As part of this evaluation, we collected qualitative and quantitative information to better understand barriers to contraceptive use in Senegal. Preliminary analysis of facility records suggested that women often missed their follow-up contraception appointments, and regular attendance also emerged as a concern for FP providers in qualitative workshops. Based on these concurrent observations, we incorporated the topic of appointment attendance in the interview and focus group guides to enable a mixed methods study of barriers to regular attendance.
Quantitative methods
Data source
In total, data on FP consultations were collected from 72 public facilities in 9 regions. Data were collected in July and August 2016 by surveyor teams including at least one medical doctor and midwife. Public health centres and health posts were selected randomly using a stratified sampling design (regions sampled by simple random sample from zones, districts sampled by simple random sample from regions). In each selected district, the district health centre was included, as well as three randomly selected health posts.
Information on facility characteristics and the number of FP providers was collected from facility managers using a questionnaire designed for this study. Data were extracted from routine, standardised FP consultation cards for all women attending an FP consultation in April, May or June 2016. These consultation cards record information on sociodemographic characteristics, method chosen at first appointment, and the date and units received at each consecutive appointment for the same woman at the facility. A standardised FP record management system is promoted by district reproductive health coordinators, whereby consultation cards are organised according to the date of next scheduled appointment (eg, third month after injection), facilitating the identification of our study sample. Data on months with recorded stockouts for contraceptive products were also extracted from stock cards, and monthly number of consultations was extracted from FP registers.
All information from routine records was captured in facilities using handheld scanners and subsequently entered into a database. Extensive data quality checks were performed during data collection and entry, including comparing data entered with scanned records for approximately 5% of all consultation cards.
Data preparation and definition of delay
We constructed a longitudinal data set of FP consultations linked by women using routine consultation cards. Consultations in which women received an injection or pill pack(s), with known current and subsequent visit dates, were included in the analysis and classified into three categories: (1) those with a subsequent consultation whose timing did not expose women to pregnancy (‘on time’), (2) those with a delayed subsequent consultation exposing women to pregnancy (‘delayed’), and (3) those with a subsequent consultation of unknown delay status (table 1). For pills, consultations were considered on time if they occurred before the woman’s pill supply was exhausted, and delayed thereafter. Consultations with delays longer than 3 weeks were considered of unknown delay status, since women may have obtained contraceptive pills elsewhere.
Classification of timeliness of consultation by method
Although repeat depot medroxyprogesterone acetate (DMPA) injections (including the two injectables distributed in Senegal, Depo Provera and Sayana Press) ‘can be given up to four weeks late without requiring additional contraceptive protection, this does not mean that the regular DMPA injection interval can be extended by four weeks’.6 Injectable consultations were considered on time if they occurred before the end of the 13-week effectiveness period, or within the 4-week grace period with no delay at the previous injection. They were considered delayed if they occurred after the 4-week grace period, or within the 4-week grace period if the previous consultation was also delayed. The delay status was considered unknown if the visit occurred more than 11 weeks after the end of the effectiveness period, since women may have received an injection elsewhere.
Statistical analysis
The analysis sample included consultations in the 3 years prior to data collection (July 2013–June 2016) to describe the current situation regarding delayed appointments. The characteristics of facilities and women included in the sample were described, as well as the delay status of consultations overall, and for each method separately. We used three-level mixed-effects logistic regression models (consultations nested among women nested among facilities) to identify women and facility characteristics associated with delayed consultations, excluding consultations with unknown delay status. Variables associated with a delayed consultation in bivariate models with a p value ≤0.25 were included in the full multivariable model. We used Spearman correlations to examine multicollinearity in the full model. Manual backward stepwise elimination based on Wald tests was used to reduce the full model to a more parsimonious final model, using records with complete data for the variables included in the full model. Variable elimination stopped when all predictors had a p value ≤0.1. The final model presented includes all records with complete data for included variables. Forward stepwise regression was performed as a sensitivity analysis.
Qualitative methods
Data source
The qualitative data source used in this study consists of 2 participatory workshops with 12 FP providers (nurses and midwives) conducted in July 2016, as well as 8 focus groups and 112 indepth interviews with women of reproductive age conducted between September and December 2016, in 11 of the 14 regions of Senegal. Sampling was purposive to represent urban and rural areas, distance to nearest facility, and different cultural and socioeconomic contexts. Some women participating in focus groups or interviews may also be included in the quantitative analysis; however, participants were anonymised and unidentifiable between study arms. Interview and focus group guides were informed by a desk review of peer-reviewed and grey literature (in French and English) on FP in Senegal, and by exploratory work conducted through preliminary discussions with FP stakeholders and visits of FP facilities. Interview guides were designed to allow unexpected issues to emerge.
Analysis
Verbatim transcripts of interviews, workshops and focus groups conducted in Wolof were translated into French and independently coded by the study researchers along key themes. Deductive codes were derived from the interview guide, and inductive codes were developed through analysis of the selected transcripts. Codes were further developed using qualitative software and agreed on collectively between research assistants and supervisors. For the scope of this paper, we focused on documenting the routines surrounding FP appointments to better understand contextual reasons for delayed attendance, through a thematic analysis of workshop, interview and focus group transcripts.
Results
Quantitative findings
Description of sample of women and consultations
In total, 6800 women attended an FP consultation in April, May or June 2016 in the facilities sampled. The reasons for excluding women and consultations are described in figure 1. The sample used for analysis included 4005 women with 14 806 consultations (59% of 25 222 total consultations among these women) between July 2013 and June 2016 during which they received pills or injectables.

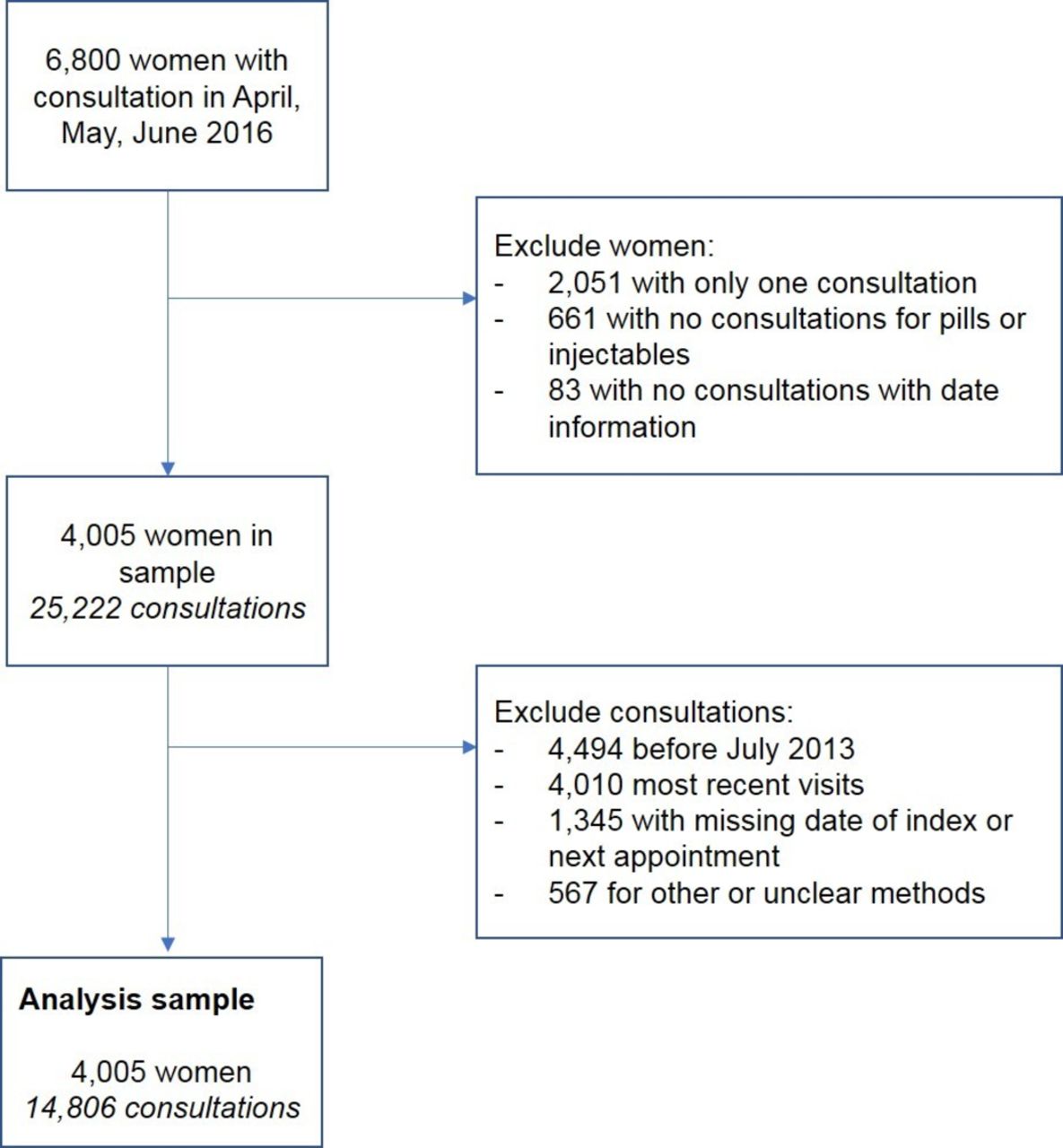{kind=link}
Selection of women and consultations in the sample for analysis.
The vast majority of contraceptive users were currently married (88%) and Muslim (90%), and most women had at least two children (73%; table 2). Almost half of women (45%) had not received any formal education. Between 5% and 11% of women had missing information on sociodemographic variables. Facility characteristics of the 16 health centres and 51 health posts attended by women in the sample are described in table 3.
Description of women in the sample (N=4005)
Description of facilities in the sample (N=67)
Prevalence of delays
A similar proportion of appointments for pills and injectables were ‘on time’ (36% and 35%, respectively) (table 4). A further 30% of appointments for injectables were within the 4-week grace period with no delay at the previous visit, meaning in total two-thirds of appointments for injectables were ‘on time’, with no exposure to pregnancy. However, 27% of appointments for injectables were delayed with the effect of exposing women to pregnancy, either because they occurred after the 4-week grace period (5%) or because of consecutive delays at the current and previous visits (22%). Delays were more common for pill appointments (44%) than injectables (27%). Around 8% of injectable visits had an unknown delay status, compared with 20% for pills. Overall, the timing of 30% of all visits for pills and injectables exposed women to pregnancy, while 60% were on time.
Timeliness of subsequent visit for pill and injectable consultations (N=12 247 consultations)
Predictors of delayed consultations
We examined risk factors for delays among consultations with known delay status. In bivariate analyses age, parity, ethnicity, religion, marital status, education, visit number, method received, previous delay, facility type, stockout level and region were associated with delayed consultation (p≤0.25; table 5). There was no association between delayed appointments and women’s occupation, facility location, number of FP providers or FP consultation volume.
Predictors of delayed appointment for pills and injectables among women attending family planning (FP) consultations in Senegal
In the final model, previous delay, pill use, lower educational level, higher parity, third visits and Islamic faith were predictive of a delayed consultation (p<0.04 for all). The strongest predictor was having experienced a delay at a previous consultation (OR=7.54, 95% CI 6.53 to 8.72). Consultations for pills were 4.6 times more likely to be delayed than those for injectables, while Christian women had 0.78 times the odds of delay as compared with Muslim women. Women with at least secondary education had 13% lower odds of delay than women with no education. Although after adjusting for all other predictors the odds of delay peaked at the third visit and declined thereafter, this is probably an artefact of adjusting for previous delay. A better representation of the association between delays and visit number is given without adjusting for previous delay, showing that the second visit is least likely to be delayed, while the odds of delay remain higher from the third visit onward (see note in table 5). More of the variance in delays was explained by between-women variability (intraclass correlation=0.093) than between-facility variability (0.007).
The forward stepwise approach identified the same predictors in the final model.
Locating missed appointments in the routines surrounding FP consultation attendance: insights from qualitative data
In interviews and focus group discussions, we focused on documenting the routines surrounding missed appointments to explore factors contributing to delays.
Knowing when to return for a follow-up consultation
Women ‘just being forgetful’ was initially mentioned by community members and providers as a reason for delays to FP appointments; however, looking more closely at the routines surrounding missed appointments revealed broader barriers to regular attendance. The ‘forgetfulness’ narrative makes the assumptions that women know (and later forget) when they need to return for a follow-up consultation. In contrast, it appeared that not all women were aware of when their next appointment was, as illustrated in the exchange below.
“Facilitator: Do you know the date of your next appointment?
Woman: Yes.
Facilitator: When is it?
Woman: In 2 weeks.
Interviewer: Does she [FP provider] have your appointment reminder card?
Woman: Yes.
Facilitator: At what time is your appointment?
[…]
Woman: I don’t know, I will go there [to the facility] and she will tell me.
Facilitator: So, you don’t know.
Woman: No, I forgot.” (Woman, focus group discussion)
Most contraceptive users reported having an appointment reminder card filled in by the FP provider (although the next scheduled appointment dates recorded in consultation cards were sometimes wrong; providers sometimes rounded up to 3 months—rather than 12 weeks—when giving three pill packs). However, illiteracy made some women unable to use them, particularly in rural areas, making them reliant on others to know their next appointment date, as illustrated by this woman’s explanation:
I do not know but I know there is still time. Since I do not know how to read I show the card to the literate so they can tell me. S. knows how to read, each time she’s the one who tells me my appointment [date] . (Woman, interview)
Furthermore, women using contraception without their relatives’ knowledge often preferred not to keep their appointment reminder card at home, thereby foregoing reminders altogether. Some providers developed practices to support women, for example keeping appointment reminder cards at the facility (as reported in the first exchange), or requesting outreach workers to remind them in person. Therefore, women did not always know their next appointment date due to being unable to use their appointment reminders.
Socioeconomic barriers to timely appointments
Another assumption of the ‘forgetfulness’ narrative is that women have the agency to return to the facility at the required time. In contrast, our findings highlight that even when women knew their next appointment date, they were sometimes unable to attend the facility on time.
Although our data show increasing acceptance of FP for spacing births in Senegal, a substantial number of women nonetheless used contraception without their husband’s or mother-in-law’s knowledge. Covert use appeared to be widespread, occurring in all regions where data were collected, especially (but not exclusively) in more remote rural areas.
[…] they do not want family planning. […] Sometimes when you do vaccination outreach activities in hard-to-reach areas, you use this opportunity to offer family planning services. […] In the villages, it’s difficult. (Nurse in charge of health post; workshop with FP providers)
As a consequence, women reported waiting until their husband travelled to go to a facility, seeking FP services in a distant facility to avoid being identified or pretending to be sick as an excuse to go to a facility. Covert use thereby constrained when women were able to attend consultations, affecting the timeliness of refills. It also influenced contraceptive method choice, with many covert users preferring injectables due to their ‘invisible’ nature. Although some providers encouraged women to switch to a longer acting method in order to space their appointments more, in some villages there were concerns that such methods would be discovered by husbands.
If you see that others get Depo Provera injections, it’s because the injection does not leave any trace on the body. When it comes to Jadelle [implant], the men are informed now. They check. […] Some women use it [injection] so that their husbands don’t know. (Nurse in charge of health post; workshop with FP providers)
Beneath the logistics of missed appointments therefore lies the broader issue of acceptability of contraceptive use. Although the stigma against FP does not always prevent women from using contraception altogether, it constrains them to use injectables requiring regular refills and prevents them from obtaining reinjections on time, thereby exposing them to discontinuity in contraceptive use and to pregnancy.
The cost of attending FP services was also mentioned as an important obstacle to timely appointments, as illustrated in the following focus group exchange:
“Facilitator: And you F, do you go to your appointments?
Woman 6: No.
Facilitator: Why don’t you go?
Woman 6: I don’t have any money.
Facilitator: And you B, do you go?
Woman 2: It might be that within 2 days I’ll go.
[…]
Facilitator: What are you waiting for?
Woman 2: Because of the money, because if you go there […] you are asked to buy a ticket [consultation fee]." (Women, focus group discussion)
The total cost of services could represent substantial amounts: women reported having to pay up to CFA2000 (US$3.65 equivalent) for one consultation. Within this context, contraception appointments were sometimes intentionally delayed by women in response to low cash flow, especially during periods of increased household spending such as the religious holiday of the Tabaski (Eid al-Adha).
Health system barriers to timely appointments
Restricted opening hours of FP services were mentioned as a factor affecting missed appointments, related to long distances women have to travel to reach their nearest facility; this appeared to be especially problematic in rural areas during the harvest season when women worked in the fields during the day. FP services were not always available during health post opening hours. For example, midwives’ administrative and clinical workload was linked to their regular absence from facilities, while women reported sometimes arriving at a facility to be asked to return on the facility’s ‘family planning day’, on a different day of the week. Furthermore, dépositaires (storeroom managers) managing medical commodities are usually paid by village health committees to be present part-time in health posts (eg, only in the mornings). These health systems barriers imply that women attending facilities may sometimes not be seen by a provider or receive their chosen product.
Discussion
Our findings indicate that delays to women obtaining repeat pills and injections are common in Senegal, with the timing of almost one-third of all appointments exposing them to the risk of pregnancy. A quarter of injectable appointments were delayed, corresponding to one delayed appointment per year on average among the vast majority of short-acting method users. Women with previous delays, less education, more children, at least two visits and who used the pill were more likely to experience delays. In contrast to the prevailing narrative of women’s ‘forgetfulness’, broader contextual barriers to regular attendance emerged as the main reasons for missed appointments: women were not always able to use appointment reminders, and when they knew their next appointment date they sometimes had to delay attendance to avoid revealing contraceptive use or in times of financial scarcity. The time-limited availability of FP services was an additional obstacle to timely contraceptive refills.
Similar to our findings, 16%–25% of injectable appointments occurred after the grace period in South Africa,17 while half of first reinjections were delayed in Malawi (this figure does not take into account the grace period).16 The 36% of women obtaining pill packs on time in our study was slightly higher than the 28% reported in Malawi.16 For injectable users, delays resulting in pregnancy risk were most commonly due to repeated delays within the grace period at consecutive appointments, highlighting a potential need for better information among injectable users. These delays probably contribute to the high prevalence of unintended pregnancies in Senegal,7 29 with important health implications in a country where abortion is heavily criminalised and unsafe abortion is common.9 30
Around 9% of appointments had an unknown delay status, meaning they occurred so late after the scheduled appointment date that women may have obtained contraception elsewhere. The higher proportion of unknown delays for pills is consistent with the fact that they can be purchased in pharmacies, which are not licensed to administer injectables (16% of pill users nationally obtained their last pack in a pharmacy).8 Many of these long ‘delays’ are due to women wanting to get pregnant; indeed, contraceptives are primarily used to space—rather than limit—births in Senegal,8 and desire for pregnancy is a primary reason for discontinuation in high-fertility countries.10 These interruptions are not problematic from a public health perspective, as they do not indicate an unmet need for contraception. Some delays may also reflect temporary discontinuation (‘taking a break’ from contraceptives) as a result of side effects, as has been described in South Africa and the USA.13 14
Covert use was found to be widespread in Senegal, echoing findings in urban Mali31 and Burkina Faso, where half of contraceptive users were estimated to use covertly in 2010,32 as well as elsewhere in sub-Saharan Africa.23–25 32–34 Covert use appears to be an important barrier to contraceptive continuity among FP users in our study, by depriving them of appointment reminders and constraining when they are able to attend the facility, similar to Ghana and Ethiopia where covert use was a risk factor for discontinuation.23 24 Acceptability remains an important barrier to contraceptive use in Senegal, despite information and advocacy efforts. A large proportion of women with unmet need do not intend to use FP in the future,20 and opposition to contraceptive use is the primary reported reason for non-use among women and men.35 36 The slightly lower odds of delay among non-Muslim (predominantly Christian) women may reflect lower acceptability of contraception among the Muslim Senegalese population, or better access to FP among Christian women, who tend to be from wealthier households, larger urban centres and monogamous households.37 Government, local and international efforts have long involved religious leaders in FP promotion in Senegal, including through local ‘champion’ imams and pamphlets highlighting Quranic verses interpretable as permitting contraception (such as women’s need to rest between pregnancies), in opposition to prevailing more conservative interpretations.38 However, such efforts were piecemeal and not sustained, and some imams continue to be vocally opposed to FP.38
Similar to findings in South Africa,17 having had a previous delay is a risk factor for future delays; women who delay appointments (intentionally or not) have a higher chance of facing similar circumstances at subsequent appointments. In our study, using the pill was predictive of delays. This difference is due to pill users becoming exposed to pregnancy shortly after their last pill, while injectable users are not immediately at risk of pregnancy; indeed, the proportion of appointments strictly on time was identical for both methods (36% and 35%). Low education was identified as a contributing factor to delays in qualitative and quantitative findings; this was not the case in Malawi16 or South Africa.17 Illiteracy limits the usefulness of appointment reminder cards for the 45% of women in the study without any formal education; nationally, 60% of women above 15 are estimated to be illiterate.39 However, women with primary education—who are likely literate—also experienced more delays, indicating that the protective effect of higher education is probably due to associated financial, geographical or autonomy benefits, rather than a causal effect of literacy only.
The cost of FP services was an important barrier to timely contraceptive refills. Although since 2003 the price of pill packs and injections has been set at CFA100 and CFA20040 (US$0.18 and US$0.36, respectively), FP consultation fees have not been harmonised and varied around CFA500 (US$0.91). This fee includes the cost of auxiliary products and appointment reminder cards in some, but not all, districts, with variable costs across Senegal. Overall, women reported paying up to CFA2000 (US$3.64) for one FP appointment, a substantial barrier in a country where 38% of the population lives on less than US$1.90 per day41 and where women may not always have financial decision-making power. Despite funding increases since the 2012 London Summit, the national budget for FP remains low at US$13 per woman per year.42 Unlike other countries, FP services are not provided for free, although they are included under Senegal’s Universal Health Coverage package via community health insurance schemes. However, population coverage of these schemes is low in rural areas and the informal sector, and it is unclear whether they include auxiliary products.43 Health facilities conduct regular outreach activities (stratégies avancées), although services are only provided for free when support is available from partner non-governmental organisations (NGOs).
The use of routine FP consultation cards and qualitative data was a major strength of our study, enabling us to examine appointment behaviour among 4000 women in 9 regions and explore factors contributing to delays with women and providers in 11 regions. These data sources provided complementary perspectives, identifying different risk factors: for example, operating hours and covert use were not recorded in consultation cards but were identified as barriers in qualitative findings, highlighting the importance of using mixed methods to fully understand ‘missed’ appointments. High-quality routine data are better suited to examining gaps in continuity than self-reported contraceptive calendar data, which would likely underestimate the prevalence of delays; however, routine data have limitations for our analysis.
First, our identification of women attending a consultation in April–June 2016 may have been incomplete. Although most sampled facilities appeared to implement standardised filing systems, the extent to which these were rigorously implemented is unknown, and some women may have been missed. Overall, we believe the ascertainment of current users was near-complete in most facilities. Second, there was no specific prompt for providers to record contraceptive method beyond the first visit. However, many providers recorded it nonetheless, and only 2% of consultations were excluded due to the method received being unclear. Extensive data quality checks and correspondence with midwives in Senegal ensured the data were entered and interpreted correctly. Records did not include other important information, such as parity after the first visit, or refills obtained from other facilities or retailers, although these are captured indirectly in our category of ‘unknown delay status’. As with many routine data sources, the proportion of missing data was important (5%–10%) for women’s sociodemographic characteristics, potentially biasing our identification of risk factors, although we have no reason to believe that women with missing data are systematically different from others.
Our findings point to several recommendations for improving FP service delivery. More accessible FP service hours are needed, particularly in rural areas (as identified in Ghana).23 Providers should consider giving women more than the routine two to three pill packs after several months’ use without side effects to minimise the frequency of consultations, although the additional cost would likely be prohibitive for some women. Providers should be retrained on giving women the correct time to next appointment, particularly not rounding up the months for pills, and highlighting the pregnancy risk associated with repeat delays for injectables. Furthermore, standardised policies to screen contraceptive users for risk factors (including previous delay, illiteracy and covert use) should be developed to help identify women at higher risk of delay and most likely to benefit from interventions to improve attendance. Innovative strategies are needed for appointment reminders in settings of high illiteracy and covert use to improve contraceptive continuity. Existing strategies for contacting women missing appointments, using mobile phones or community health volunteers (bajenu gox), should be expanded with women’s consent and while respecting the imperative of confidentiality. In light of high covert use, facilities need to ensure privacy and confidentiality for all women.
Nonetheless, beyond a narrow focus on individual women, comprehensive strategies addressing contextual barriers to regular attendance are needed. In particular, effective, innovative interventions should be developed to increase the acceptability of contraceptive use among men and community members generally, building on existing campaigns.20 38 Cost studies are needed to understand how much women spend for FP services, transport and opportunity costs in Senegal and elsewhere. FP service costs should be harmonised nationally and auxiliary products included under the consultation fee across all districts. Subsidies should be considered to remove financial barriers for short-acting methods, for example by ensuring free community health insurance for women least able to pay or making FP services free. Systematic support should be gathered from NGOs to ensure outreach activities in remote areas provide free services. Lastly, our findings echo the need to reinforce provision of postabortion care and educate providers and women on the legality of such care.30
Conclusion
Our study found that pill and injectable users in Senegal often experience delays in their FP appointments, with the timing of one-third of appointments exposing them to pregnancy. Such gaps in continuity imply that recent increases in contraceptive use may not translate into commensurate reductions in unwanted pregnancies. Understanding factors contributing to short-term gaps in contraceptive use can also help shed light on causes of discontinuation. The results from this study indicate that women in Senegal do not always know their next appointment date and are not always able to attend the facility on time, highlighting the importance of addressing contextual barriers. In particular, innovative interventions are needed to increase acceptability of contraceptive use, remind illiterate women of their appointments, and reduce or eliminate the cost of FP services.
Acknowledgments
The authors gratefully acknowledge the study teams and participants in Senegal. The research in this publication was supported by funding from MSD, through its MSD for Mothers programme. MSD had no role in the design, collection, analysis and interpretation of data, in writing of the manuscript, or in the decision to submit the manuscript for publication. The content of this publication is solely the responsibility of the authors and does not represent the official views of MSD. MSD for Mothers is an initiative of Merck & Co, Kenilworth, New Jersey, USA.
References
Footnotes
Handling editor Seye Abimbola
Contributors FLC designed and conducted the quantitative analysis, with support from JAC. DD designed the qualitative analysis and conducted the analysis with SF. CAL was the principal investigator of the Informed Push Model evaluation, and contributed to all aspects of the study design and conduct, with input from AF, FLC, DD and SF. AF and FLC managed the quantitative data collection, and DD and SF managed the qualitative data collection. FLC wrote the first draft of the manuscript. All authors provided input on the manuscript and approved the final version.
Funding Funding for the evaluation of the Informed Push Model was provided by MSD for Mothers.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Ethical approval for the evaluation of the Informed Push Model was granted by the ethics committee of the Senegalese Ministry of Health and Social Action, and of the London School of Hygiene & Tropical Medicine, UK, which also granted ethical approval for this secondary analysis.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The full data set is available from the corresponding author at francesca.cavallaro@lshtm.ac.uk.