Article Text

Abstract
Introduction The continuum of care has recently received attention in maternal, newborn and child health. It can be an effective policy framework to ensure that every woman and child receives timely and appropriate services throughout the continuum. However, a commonly used measurement does not evaluate if a pair of woman and child complies with the continuum of care. This study assessed the continuum of care based on two measurements: continuous visits to health facilities (measurement 1) and receiving key components of services (measurement 2). It also explored individual-level and area-level factors associated with the continuum of care achievement and then investigated how the continuum of care differed across areas.
Methods In this cross-sectional study in Ghana in 2013, the continuum of care achievement and other characteristics of 1401 pairs of randomly selected women and children were collected. Multilevel logistic regression was used to estimate the factors associated with the continuum of care and its divergence across 22 areas.
Results Throughout the pregnancy, delivery and post-delivery stages, 7.9% of women and children achieved the continuum of care through continuous visits to health facilities (measurement 1). Meanwhile, 10.3% achieved the continuum of care by receiving all key components of maternal, newborn and child health services (measurement 2). Only 1.8% of them achieved it under both measurements. Women and children from wealthier households were more likely to achieve the continuum of care under both measurements. Women’s education and complications were associated with higher continuum of care services-based achievement. Variance of a random intercept was larger in the continuum of care services-based model than the visit-based model.
Conclusions Most women and children failed to achieve the continuum of care in maternal, newborn and child health. Those who consistently visited health facilities did not necessarily receive key components of services.
- maternal health
- child health
- health services research
- cross-sectional survey
- community-based survey
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Women and children do not necessarily receive all recommended care along the continuum of care from pregnancy to post-delivery.
What are the new findings?
From pregnancy to post-delivery, 10% of the pairs of women and children received all recommended components of services, and 2% of them received them in addition to meeting the recommended number of visits to health facilities in Ghana.
Geographical disparity existed in the coverage of the continuum of care in Ghana.
What do the new findings imply?
Health administrators should ensure that women and children receive all the key components of services on their visit to health facilities.
Continuum of care should be measured at the individual level and compared subnationally to reduce inequality in provision of care across subnational areas.
Introduction
Saving lives from maternal and neonatal complications remains a major health challenge in low-income and middle-income countries. In these countries, the maternal mortality ratio was 20 times higher and the neonatal mortality rate was 7 times higher than those in high-income countries in 2015.1 2 Many such deaths are preventable by receiving appropriate care for maternal, newborn and child health (MNCH).3–6 This also contributes to their long-term health outcomes.7
The coverage of MNCH services is typically measured as the number of antenatal care (ANC) visits, delivery attended by a skilled birth attendant (SBA) and the number of postnatal care (PNC) visits. The coverage has been improving in low-income and middle-income countries, and it is regarded as one of the major contributions to the reduction of maternal, newborn and child mortalities.8 However, targeting the coverage of each MNCH service separately does not necessarily ensure that every woman and her child receives a series of MNCH services continuously from the pregnancy to post-delivery stages.9
The continuum of care (CoC) has recently received attention in MNCH; its intention is to guarantee that every woman and child receives care whenever they need. CoC can be an effective policy framework to improve the coverage of MNCH services for women and children.10–14 It is broadly divided into two dimensions: time and space. CoC at the time dimension refers to a situation where a woman and her child receive MNCH services from prepregnancy to childhood. CoC at the space dimension addresses coordination among family level, community-level and facility-level MNCH care and referral to advanced-level care if needed.10 CoC at the space dimension is an important concept for those who need specific care for their complications, danger signs and diseases. In contrast, CoC at the time dimension is a policy goal that every woman and child should achieve. Thus, it can be an indicator that measures the coverage of MNCH services.
CoC at the time dimension addresses the importance of linkages among the packages of MNCH service delivery at different reproductive stages.3 10 12 Among such packages, routine ANC, delivery attended by SBA and PNC are primary means of ensuring CoC. Women and children can potentially receive timely and necessary MNCH care through these packages and reduce risks of maternal and infant mortality and morbidity. However, only 8% of women and children in Ghana received all of ANC four times or more, delivered attended by SBA and PNC three times.15 In Pakistan, 27% of women and children received all of ANC four times or more, delivered attended by SBA and PNC at least once within 6 weeks of delivery in 2012–2013.16 In nine South Asian and sub-Saharan African countries, 17% of women and children received all of ANC four times or more, delivered attended by SBA and the first PNC within 24 hours of delivery.17 These CoC coverage are lower than composite coverage index, the weighted average of individual MNCH indicators.18 19 That is, improvement in individual MNCH indicators does not necessarily translate into a situation that no one is left behind from receiving all essential MNCH services.
Achieving CoC in MNCH at the time dimension may be measured differently. It can be measured as the components of services that mothers and children receive at ANC, delivery attended by SBA and PNC. In low-income and middle-income countries, some of the key components are not provided in ANC.20–24 This lack of key components in service delivery is also referred to as the quality gap in CoC in MNCH.24 25 Similar problems exist in delivery5 24 26 and PNC.27 28 Under the quality gap, even if women and children visit health facilities with their own intentions, they may not receive some components of services due to the lack of services available at health facilities. Thus, CoC could be more affected by services provided by a health facility when it is measured as receiving key components of services, rather than simply counting the number of visits. Such health facility factors may explain part of availability of MNCH services and efficiency in managing health workers and services at health facilities.29 In addition to such supply-side factors, CoC can be influenced by factors related to women and their households. According to an analysis in Cambodia among women who received ANC and delivered attended by SBA, women from wealthier households tended to receive PNC more.30 A study in Ghana showed that marital status, education, means of transportation to a health facility, women’s autonomy in decision making and wealth level were associated with achieving CoC.15
Ghana is one of the sub-Saharan African countries to improve MNCH-related health outcomes, although there is much to be done to meet the global target of such outcomes.19 31–33 The maternal mortality ratio and infant mortality rate in Ghana were estimated at 380 per 100 000 live births in 2013 and 49 per 1000 live births, respectively, in 2012.34 Improved coverage of ANC, delivery attended by SBA and PNC have been regarded as keys to improving MNCH-related health outcomes.35–38 The ANC coverage of four times or more visits was 87.3%, delivery attended by SBA was 73.7% and first postnatal check-up for mothers within 48 hours was 81.1%, according to the Demographic and Health Survey (DHS) 2014.31 However, such coverage differed across 10 regions of Ghana. For example, the coverage of delivery attended by SBA ranged from 36.4% in the lowest region to 92.1% in the highest region.31 Room for improvement exists in MNCH service delivery in Ghana.
The objectives of this study were threefold. First, this study compared CoC achievement in MNCH at the time dimension based on two measurements: CoC measured by counting visits and CoC measured by key components of services that were received. Second, this study compared the factors affecting CoC based on the two different CoC measurements. Finally, this study examined to what extent CoC achievement was different across areas, using the two measurements described above.
Methods
Study design and area
Under a cross-sectional design, this study measured MNCH service-seeking behaviours of women and their children at the pregnancy, delivery and post-delivery stages in Ghana. It also measured their background characteristics and complications using face-to-face interviews with women in health demographic surveillance sites under three Health Research Centres (HRC) in Ghana, namely Dodowa,39 Kintampo40 and Navrongo.41 The total population of this survey area was 456 492 in 2012 and the estimated number of live births per year was 13 695, assuming that the crude birth rate was 30 out of 1000 people.
This study was conducted as part of the formative research of the Ghana EMBRACE (Ensure Mothers and Babies Regular Access to Care) Implementation Research.42 This research is aimed at evaluating the impact and implementation process of a set of MNCH interventions that enhance CoC under the EMBRACE Model, as proposed by the Government of Japan.43 44 It was funded by the Japan International Cooperation Agency (JICA) and the JICA Research Institute.
Participants and selection criteria
The targeted women in this study were aged between 15 and 49 years who experienced their latest pregnancy as a live birth or stillbirth between January 2011 and April 2013. Inclusion criteria were women who lived in study site on the date of the data collection. If the women delivered twice or more during the above period, the latest pregnancy data were used.
A total of 1500 women were selected based on the two-stage random sampling method. The primary sampling unit involved communities under a zone or subdistrict (area), depending on HRC. The study site has 22 areas in three HRCs. Women were randomly selected under probability proportional to the sample size. The sample size was calculated based on the assumption that the expected coverage of key MNCH services throughout pregnancy, delivery and post-delivery was 15%. A sample size of 1275 provided an estimate with 2% confidence limits at a 0.05 significance level. Assuming 15% of women with incomplete information, a total of 1500 women was proposed.
Measurements
Two outcome variables were used to assess CoC achievement in MNCH. The first measurement is the proportion of women and children who received MNCH services at the pregnancy, delivery and post-delivery stages. Under this measurement, a pair (woman and child) achieved the CoC when the woman received ANC four times or more, delivered at a health facility and received both maternal and child PNC within 48 hours and around 2 and 6 weeks post-delivery. According to our observations in the study site, women and children visited health facilities and received such MNCH services while few received them at the community level. Thus, coverage under the first measurement is referred to as ‘visit-based CoC'. The second measurement is the proportion of women and children who received the key components of MNCH services during ANC and PNC, and during and post-delivery based on women’s self-reports. Coverage under the second measurement is referred to as ‘services-based CoC'.
The components of MNCH services were measured in this study as follows. As services received during ANC, three components of the services were measured: received immunisation for tetanus toxoid, received intermittent preventive treatment, and received an HIV test. For delivery, two components of the services were measured: exercised skin-to-skin care immediately after delivery and initiated breast feeding within an hour of delivery. For PNC, three components of the services were measured: learnt about post-delivery complications among women and children, learnt about nutrition, anaemia and breast feeding, and received immunisation. These components of services were selected based on the guidelines and policy documents for ANC, delivery care and PNC,3 45–47 related literature48–54 and comments from health administrators at the study site. The services measured as listed above were limited to those that could be determined through women’s self-reports.
This study collected the socioeconomic characteristics of women and their households that were likely to affect their MNCH service-seeking behaviour based on previous research.55–58 These characteristics included the women’s ages, educational attainment, marital status, religion, number of pregnancies, age and educational attainment of their partners and number of children aged under 5 years in the household. Socioeconomic status was also estimated using factor analysis based on the following variables: availability of electric power, availability of a clean toilet, type of roof material of the house, ownership of refrigerator, availability of clean water, ownership of TV, ownership of radio, ownership of mobile phone and ownership of transportation (car and motorbike).
Factors during the latest pregnancy of women were also measured. These factors included intended pregnancy, birth preparedness, health insurance, support from household members and complications and danger signs.
Data collection
This study collected data using a structured questionnaire that was written in English. Interviewers who could speak at least one local language in a survey area were hired and received training in July 2013 on the objectives, design and ethical consideration of this study, as well as the contents of the questionnaire. Pretesting was undertaken in each HRC in July 2013, and the contents of the questionnaire were confirmed. Face-to-face interviews with women were undertaken from July to September 2013 in local languages that women could listen to and speak. The data items used to construct the socioeconomic status were extracted from the health demographic surveillance database at each HRC.
Data analysis
First of all, women whose information was partly missing or they were found not to meet the inclusion criteria were excluded from analysis. Then, descriptive analysis was performed to present the background characteristics of women and children in the sample and the coverage of CoC. Paired t-test was performed to compare the coverage in MNCH services using the definitions of visit-based CoC and services-based CoC. A multilevel logistic regression with a random intercept at the area level was performed to identify the factors associated with the achievement of CoC and the variance of the achievement across areas. In the regression, both of visit-based CoC and services-based CoC were dichotomised so that this study could evaluate factors associated with making all necessary visits to health facilities (visit-based CoC) and received all necessary components of MNCH services (services-based CoC) as defined in the ’Measurements' section. As explanatory variables, socioeconomic characteristics (the women’s ages, educational attainment, marital status, religion, number of pregnancies, age and educational attainment of their partners and number of children aged under 5 years in the household) and factors during the latest pregnancy of women (intended pregnancy, birth preparedness, health insurance, support from household members and complications and danger signs) were included in the model. Variance inflation factor was used to check the multicollinearity, although no variable exceeded 4 as a threshold. To evaluate to what extent differences in the level of CoC were caused by specific factors at the area level, this study used different sets of explanatory variables in the regression model. In addition to the full model (socioeconomic characteristics and factors relating to the latest pregnancy as explanatory variables), the null model (excluding all explanatory variables) and the model excluding factors relating to the latest pregnancy were tested. Then, intraclass correlation coefficient (ICC) was used to compare the proportion of variance caused by the random intercept at the area level among different models.
Ethical consideration
All respondents voluntarily participated and were given details of the study before the survey. Written informed consent was obtained, and confidentiality was assured for all participants.
Results
Characteristics of women and their households
Table 1 shows the socioeconomic characteristics of women and their households. Of 1500 participants recruited, 99 women were excluded as their background information was partly missing or they were found not to meet the inclusion criteria. A sample of 1401 women was used in this study. Most women (84.6%) were aged between 20 and 39 years. Only 9.0% of women were aged 19 years or under and 6.4% of women were aged 40 years or above. While 38.3% of women did not complete primary education, 23.3% and 28.6% of women completed primary and lower secondary education, respectively.
Characteristics of women and households (n=1401)
Table 1 also shows factors during the latest pregnancies of women. While 79.7% of women received non-financial support from their household members during and after deliveries, only 34.9% had prepared funds in advance for delivery. About half of the women (53.8%) experienced complications during pregnancy, delivery or post-delivery within 6 weeks of delivery and 17.6% of children had complications within 6 weeks of delivery.
CoC achievement
Table 2 presents CoC achievement in MNCH. Only 111 women (7.9%) achieved visit-based CoC; 145 women (10.3%) achieved services-based CoC.
CoC achievement in MNCH based on different measurements (n=1401)
Coverage of MNCH services components
The coverage of the key components in the MNCH services was substantially different from the coverage of the ANC, delivery attended by SBA or PNC. According to figure 1(A), 86.2% of women received ANC four times or more, and almost all women (98.5%) visited the ANC at least once. Among the key components of the services, the coverage of the HIV test was lowest (62.8%).
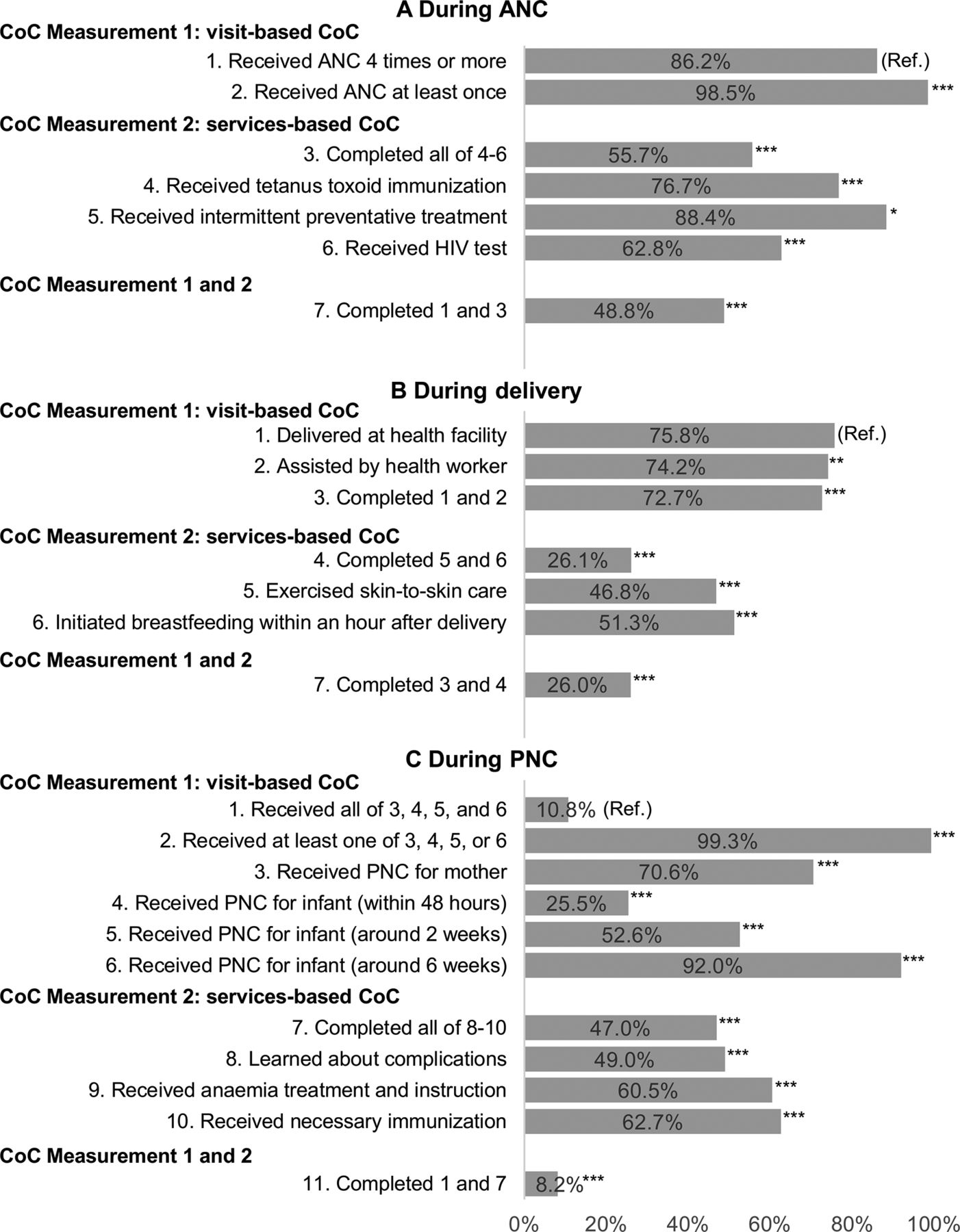
MNCH services received. (A) During ANC. (B) During delivery. (C) During PNC. Paired t-test was conducted for testing the difference in proportions between the reference variable and each of the other variables in each figure. *Significant at 5% level; **significant at 1% level; ***significant at 0.1% level. ANC, antenatal care; CoC, continuum of care; MNCH, maternal, newborn and child health; PNC, postnatal care; Ref., reference variable.
Figure 1(B) presents the differences between delivery assisted by SBA and the coverage of key components of services at delivery. The percentages of women who exercised skin-to-skin care and initiated breast feeding within an hour of delivery were 46.8% and 51.3%, respectively. Such coverage was substantially lower than the rate of delivery at a health facility (75.8%).
Figure 1(C) presents the coverage of PNC. Of all women, 25.5% received PNC for their children within 48 hours of delivery, while 92.0% received PNC around 6 weeks post-delivery. Women who learnt about complications, received treatment for anaemia and instruction on nutrition and received necessary immunisations were 49.0%, 60.5% and 62.7%, respectively.
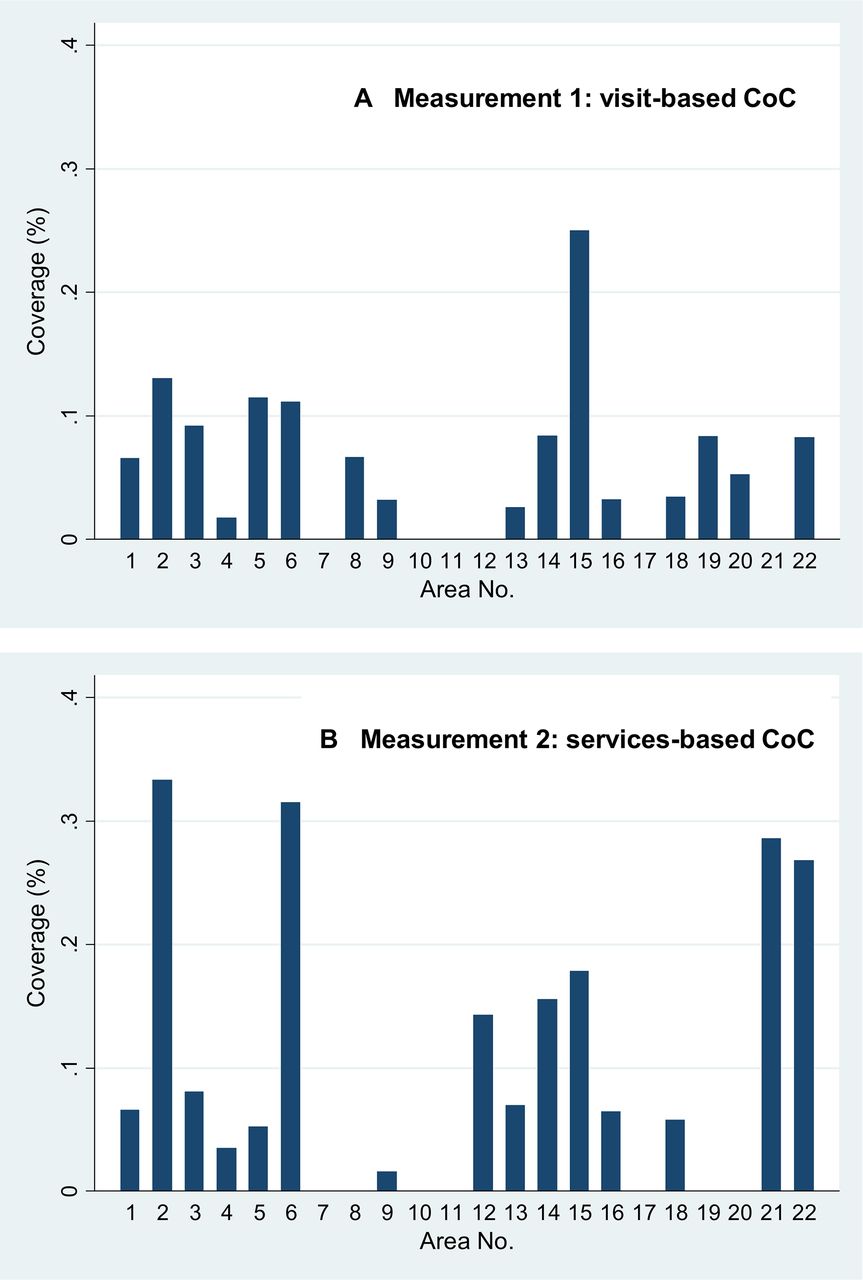
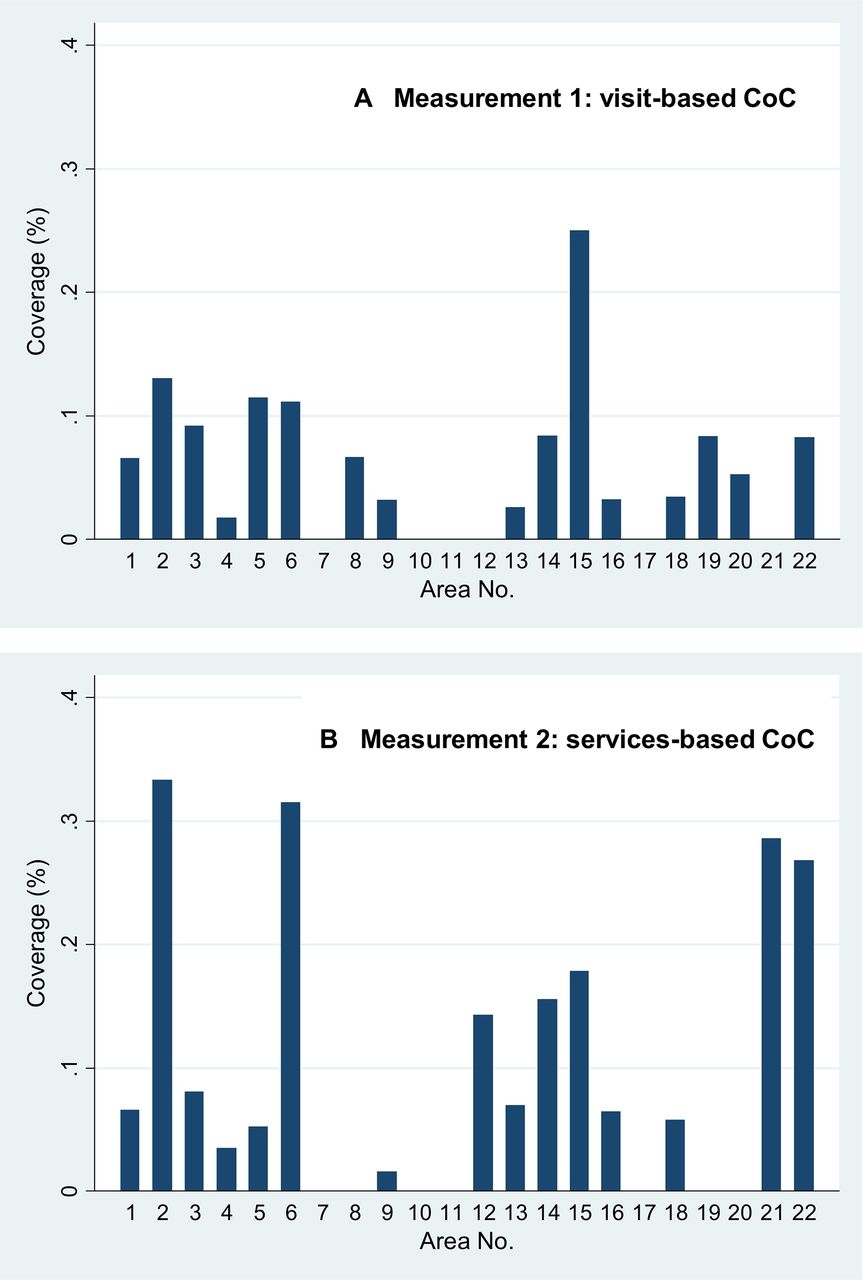
CoC achievement across areas
Figure 2 presents CoC achievement by area. According to figure 2(A ), only one area out of 22 (area no. 15) exceeded 20% regarding CoC visit-based achievement. Six areas did not have women who achieved CoC (area no. 7, 10, 11, 12, 17 and 21). Figure 2(B) shows that seven areas had no women who achieved CoC based on services received (area no. 7, 8, 10, 11, 17, 19 and 20), while four areas had a coverage of approximately 30% (area no. 2, 6, 21 and 22).
{kind=link}
{kind=link}
Continuum of care (CoC) acheivement by measurement and area. (A) The percentage of women who achieved visit-based CoC exceeded 20% in one area out of 22 (area no. 15). Six areas did not have women who achieved visit-based CoC (area no. 7, 10, 11, 12, 17 and 21). (B) The percentage of women who achieved services-based CoC was approximately 30% in four areas (area no. 2, 6, 21 and 22). Seven areas had no women who achieved services-based CoC (area no. 7, 8, 10, 11, 17, 19 and 20).
Multilevel logistic regression analysis of the factors associated with the CoC achievement
Table 3 presents the result of the multilevel logistic regression analysis with a random intercept at the area level regarding the factors associated with CoC achievement. According to model (3), religion, marital status and socioeconomic status were associated with better visit-based CoC achievement. Women who practised traditional religions or others were more likely to achieve CoC (adjusted OR (AOR) 2.71, 95% CI 1.37 to 5.35), as compared with Christians. Women cohabitating with their partners without formal marriage were less likely to achieve CoC (AOR 0.49, 95% CI 0.25 to 0.97), as compared with married women. Wealthier women were more likely to achieve CoC (AOR 1.50, 95% CI 1.09 to 2.07).
Multilevel logistic regression analysis of factors associated with the CoC achievement (n=1401)
According to model (6), services-based CoC achievement was explained by educational attainment, religion, socioeconomic status, financial preparedness and complications among women. Completed upper secondary education or above was positively associated with CoC achievement (AOR 2.47, 95% CI 1.19 to 5.14), as compared with women without formal education. Women who practised traditional religions or others were more likely to achieve CoC (AOR 2.64, 95% CI 1.40 to 5.00), as compared with Christians. Wealthier women were more likely to achieve CoC (AOR 1.41, 95% CI 1.05 to 1.89). Women who prepared money for delivery were more likely to achieve CoC (AOR 1.48, 95% CI 1.03 to 2.26). Women who experienced any complications during pregnancy, delivery or post-delivery were less likely to achieve CoC (AOR 0.59, 95% CI 0.44 to 0.92). Models (2) and (4) show that AOR and its level of significance for socioeconomic characteristics variables were not largely affected when excluding variables about factors during the latest pregnancy.
Table 3 also presents the proportion of variances caused by differences in CoC achievement across areas. According to the ICC in model (1), the null model, 13.3% of the variance regarding CoC visit-based achievement was explained by a random intercept, that is, areas in the place of living. After controlling for various factors related to women and their households, 3.5% of variations were explained by a random intercept according to model (3).
The variation in CoC achievement was larger when it was measured as services received. The ICC was 22.0% in the null model (model (4)) and 8.5% with explanatory variables (model (6)). The ICC of model (6) that estimated CoC services-based achievement received was more than twice as large as the ICC of model (3) for CoC visit-based achievement.
Discussion
This study provides us with new insights on CoC achievement in MNCH at the time dimension in three HRCs in Ghana. First, most mothers and children did not receive MNCH services comprehensively during the pregnancy, delivery and post-delivery stages; visit-based and services-based achievement of CoC was low. Second, different factors were associated with CoC based on its two measurements. Women practising traditional religions and those with a formal marital status tended more towards making routine visits at facilities to achieve CoC. Women’s education, financial preparedness and pregnancy complications among mothers were associated with services-based CoC. Women in wealthier households were more likely to achieve both visit-based and services-based CoC. Third, across-area differences were larger in services-based CoC than visit-based CoC, after controlling for various factors related to women and their households.
In this study, a small percentage of women and children achieved CoC based on both measurements by visits and services received. The coverage of CoC was extensively lower than the coverage reported in the studies in Pakistan (27%) and nine South Asian and sub-Saharan African countries (17%) based on DHS.16 17 This can be explained as follows. First, CoC was interrupted by low coverage of PNC within 48 hours despite relatively high coverage of ANC and delivery attended by SBA. The coverage of PNC reported in this study was extensively lower than the widely cited PNC coverage based on DHS 2014 in Ghana (81%).31 This is due to differences in measurement of PNC. The DHS measured PNC only once after delivery, and it regarded women who delivered at health facilities as having received PNC. However, delivery at a health facility does not guarantee that they received PNC as recommended.27 28 59
Second, health facilities where women and children visited may not provide key components of MNCH services. In this study, the coverage of the key components of services in each of the pregnancy, delivery and post-delivery stages was largely lower than the coverage of ANC, delivery attended by SBA and PNC. This supports the view of an existing quality gap in the supply of MNCH services.24 25
Different factors were associated with the coverage of both visit-based and services-based CoC. Notably, services-based CoC was affected by non-economic characteristics of women in addition to socioeconomic status. Such differences could be interpreted as follows. Providing the key components of services constitutes a portion of quality at a health facility.24 27 Women could make a choice of which health facility to visit for MNCH services if they have access to two or more health facilities. In this case, they can achieve services-based CoC due to their proactive choice of better MNCH services. Educated women may be more capable of comparing the quality of MNCH services among candidate facilities.35 60
Socioeconomic status and religions were associated with better CoC achievement for both visits and services received. Poor socioeconomic status broadly explains the limited affordability of services, as is consistent with previous literature.55 61–63 Women and children from poorer households had a lesser tendency to visit even the most easily accessed health facility. Mixed evidence exists in the effect of religion on MNCH service use.55 The effect of the same religion may be different across societies. In the study site, women had been advised to be at home after delivery. This can be interpreted as a factor that influenced the low coverage of PNC. However, it seems that women practising specific traditional beliefs were free from such traditions.
Across areas, variations in services-based CoC achievement were wider compared with visit-based CoC achievement. This implies that achieving visit-based CoC did not necessarily translate into services-based CoC and vice versa. In the multilevel models in table 3, a random intercept might capture area-specific factors, after controlling for various factors specific to women and their households. Such area-specific factors may include differences in MNCH service provision. This is consistent with evidence found on the importance of the quality of MNCH service provision in its coverage in the previous literature.29 64 65
This study highlighted the importance of monitoring CoC at the subnational level. According to the findings, the achievement of CoC was low on average and divergent across areas. Given the past progress of the coverage of ANC, delivery attended by SBA and PNC, a national MNCH policy should now address CoC by measuring to what extent women and children continuously receive services.
The measurements of visit-based and services-based CoC should be addressed in the national MNCH guideline in a country. This study counted PNC in the visit-based CoC as within 48 hours, 2 weeks and 6 weeks following the guideline in Ghana. The key components of services were selected from the guideline as well. In addition, the services-based CoC may be defined based on prioritisation in the national MNCH policy and data availability. For example, in Ghana, an MNCH policy document addresses the importance of CoC and prioritises key components of services to be provided during pregnancy, delivery, neonatal and childhood periods, although it does not define how to measure the achievement of CoC.66 Thus, the measurements of CoC can be different across countries as the measurements should serve the progress of MNCH services in line with the national MNCH guideline.
To solve divergence in CoC at the subnational levels, health administrators in a country can identify areas where CoC is low using the two measurements of CoC proposed in this study. Then, by comparing the two measurements, they may infer what factors broadly affected the low level of CoC. If the visit-based CoC is relatively low in an area, then the availability of health facilities and factors related to women and their households, including socioeconomic and cultural factors, may be further investigated. In an area where the services-based CoC was relatively low, the provisions of services in health facilities may be constrained by supply-side factors. These factors include an excess in the number of clients and tasks relative to the number of health workers, the capacity and knowledge of health workers and insufficient equipment and supplies.
Limitations
This study has the following limitations. First, visits and received key components of services were measured based on women’s answers obtained 6 weeks post-delivery or later. Despite potential recall bias, the authors believe that this is the best method to obtain information about MNCH service-seeking behaviours and the services received throughout different MNCH stages, including from women who did not visit health facilities or visited different health facilities during each visit. Second, geographic barriers to accessing a health facility, such as distance from a woman’s residence to a health facility were not explicitly accounted for in this study, although differences in areas of residence were controlled under multilevel modelling. Third, some components of the MNCH services were excluded in this survey; this study measured only key components that could be ascertained through interviews with the women. Fourth, this study was implemented in three HRCs in Ghana and not nationally representative. The results of this study reflected the situations of CoC in the broader part of Ghana but not the whole country of Ghana.
Conclusions
In conclusion, this study highlights that most of women and children failed to achieve both visit-based and services-based CoC throughout the pregnancy, delivery and post-delivery stages. They did not necessarily achieve services-based CoC even if they achieved visit-based CoC. To ensure that every woman and child consistently receives the necessary care, both visit-based and services-based CoC should be enhanced. Particularly, MNCH services provision should be standardised so that women and children receive key components of services regardless of their area of living and a health facility that they visit.
Acknowledgments
The authors would like to thank the Ministry of Foreign Affairs in Japan and the Ministry of Health in Ghana. The authors also express their gratitude to the Ghana Health Service and the District Health Management Teams of the Shai-Osudoku, Ningo-Prampram, Kintampo North, Kintampo South, Kassena Nankana East and Kassena Nankana West for the support they provided to this study. The Ghana EMBRACE Implementation Research Project was conducted by the Government of the Republic of Ghana, Japan International Cooperation Agency (JICA) Human Development Department and JICA Research Institute with a coordinating support from the System Science Consultancy.
References
Footnotes
Handling editor Valery Ridde
Contributors AS conceived the research questions, designed the study, analysed the data and drafted the manuscript. FY and SO were involved in designing the study, conducting the fieldwork and revising the manuscript. EM, CTN and YE were involved in designing the study and conducting the fieldwork. KK and KN were involved in designing the study and revising the manuscript. EKA, AH and MJ monitored the study progress and were involved in revising the manuscript. All authors read and approved the final manuscript.
Funding This paper was funded by the Japan International Cooperation Agency (JICA) Human Development Department, and JICA Research Institute (https://www.jica.go.jp/english/index.html and https://www.jica.go.jp/jica-ri/).
Competing interests None declared.
Patient consent Not required.
Ethics approval Ethical approval was obtained from the Research Ethics Committee of the Graduate School of Medicine, the University of Tokyo, The Ethical Review Committee of the Ghana Health Service, Institutional Review Boards of Dodowa Health Research Centre, Kintampo Health Research Centre and Navrongo Health Research Centre.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement There are no additional data available for this article.
Collaborators The Ghana EMBRACE Implementation Research Project Team. Yoshiharu Yoneyama; Ebenezer Appiah-Denkyira; Masamine Jimba; Abraham Hodgson; Gloria Quansah Asare; Evelyn Ansah; Junko Yasuoka; Keiko Nanishi; Akira Shibanuma; Kimiyo Kikuchi; Sumiyo Okawa; Margaret Gyapong; Sheila Addei; Vida Kukula; Doris Sarpong; Clement Narh; Seth Owusu-Agyei; Kwaku Poku-Asante; Charlotte Tawiah; Yeetey Enuameh; Kwame Adjei; Emmanuel Mahama; Abraham Oduro; John Williams; Cornelius Debpuur; Francis Yeji; Evelyn Sakeah; Peter Wontuo; Akiko Hagiwara; Sakiko Shiratori; Yusuke Kamiya.