Article Text

Abstract
Background Egypt is experiencing a hepatocellular cancer (HCC) epidemic due to widespread hepatitis C virus (HCV) transmission. The use of sofosbuvir-related therapies producing improved treatment success has permitted an updated, nationwide, HCV treatment programme with expanded coverage. This study simulated the multidecade impacts of the new treatment programme on hepatitis and HCC.
Methods A Markov model of HCV infection and treatment analysed the HCV-related HCC epidemic between 2009 and 2050, using parameters based on peer-reviewed studies and expert opinion. Comparing the ‘new’ and ‘old’ scenarios, and with the old treatment programme being replaced or not by the new programme in 2015, the annual number, prevalence and incidence of HCC were simulated for representative Egypt populations including HCV-infected patients aged 15–59 years in 2008, healthy people aged 5–59 years in 2008 and 5-year-old children cohorts entering the population each year beginning in 2009. Averted HCC cases were calculated, and sensitivity analyses were performed.
Results Compared with the old scenario, the estimated number, prevalence and incidence of future HCC cases in the new scenario would peak earlier and at lower levels in 2025 (~29 000), 2023 (~28/100 000) and 2022 (~14/100 000), respectively. The new treatment programme is estimated to avert ~956 000 HCC cases between 2015 and 2050.
Discussion By reducing cancer cases and shortening the peak epidemic period, the new programme should substantially diminish the HCC epidemic across Egypt. Our timeline forecast for Egypt’s HCC epidemic, and evaluation of various disease and programme components, should be useful to other countries that are developing policies to address HCV-related liver cancer prevention.
- Liver cancer
- hepatocellular cancer
- hepatitis C
- HCV
- disease burden
- simulation
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known?
Egypt’s new, nationwide, hepatitis C virus (HCV) treatment programme was designed to help mitigate the future disease burden from liver cancer in that country.
The old programme, which used traditional pegylated interferon and ribavirin therapy and only targeted limited numbers of patients at certain fibrosis stages, was replaced in 2015 by a series of superior sofosbuvir-related therapies and greater patient treatment capacity.
What are the new findings?
Simulation results show how the new HCV treatment programme should lessen the magnitude of Egypt’s expanding, decades-long, liver cancer epidemic by clearing infections and reducing disease progression.
These findings demonstrate how fewer hepatitis C infections result in lowered liver cancer incidence and a shorter peak epidemic period.
The forecasted benefits of the programme will be diminished if the capacity of the treatment programme is lower, or if the incidence of acute hepatitis C is higher, than expected.
What do the new findings imply?
Public health interventions to reduce liver cancer should be enhanced by maintaining or increasing the treatment programme capacity.
Our results also highlight the value of improved surveillance and increased analyses of HCV transmission across Egypt, as well as use of high-efficacy sofosbuvir-related hepatitis C therapies.
By developing simulation models that use accurate and detailed treatment success rates for different HCV patient groups, interventions could become more focused.
Introduction
Primary liver cancer ranks among the highest incidence cancers and is the second leading cause of cancer deaths (9%) globally.1 Hepatitis C virus (HCV) infection induces cirrhosis and thereby increases hepatocellular carcinoma (HCC) risk. Worldwide, HCV infection is estimated to cause about one-quarter of HCC cases.2 Egypt is experiencing an HCC epidemic largely due to HCV infection3 with the world’s highest infection prevalence (~10%) in 2008, and a 2015 HCV seroprevalence of 6.3%.4 HCV transmission is still ongoing in Egypt, with new cases estimated at 2.4 per 1000 person-years.5 Accordingly, liver cancer incidence and mortality continue to rise in Egypt: HCC liver incidence cancer increased from 18.8 to 26.5 per 100 000 between 1999 and 2007 among males, and from 5.2 to 7.0 per 100 000 among females.6 The shift from hepatitis B virus to HCV as an underlying cause of HCC is going on among Egyptian patients.7
Recognising that treating patients with HCV can both prevent HCV transmission and decrease cancer risk,8 the Egyptian government embarked on a national HCV treatment programme beginning in 2006 by providing subsidised therapy to certain groups of patients with HCV across the country. The programme provided pegylated interferon and ribavirin (Peg-IFN+RBV) as the standard therapy.9 However, this therapy only leads to a limited sustained virological response (≤60%) for patients with HCV genotype 4,10 which represents 90% of HCV-infected Egyptians.11 Poor administration, as well as the contraindications and side effects of PEG-IFN/RBV therapy, also limited programme effectiveness.12 With this programme ongoing, the HCV-related liver cancer burden was predicted to increase by 10%–15% between 2013 and 2030,13 prompting the Egyptian Ministry of Health and Population (MOHP) to update the HCV treatment programme. This involved combining daclatasvir/sofosbuvir and ribavirin (DAC/SOF±RBV) as the first new standard therapy—which has developed into a series of sofosbuvir-based therapies and generic sofosbuvir-based therapies—and expanding programme coverage to more patients with HCV experiencing a greater range of disease stages.14 Sofosbuvir is a newly developed direct-acting antiviral agent and has been characterised as having higher treatment efficacy, easy oral administration, shortened course, higher genetic barrier to resistance and less adverse effects compared with Peg-IFN+RBV therapy.15 16 Sofosbuvir-based therapy has shown treatment efficacy ranging from 71% to 95% in Egypt hepatitis C patients.17 18
The promise that this new treatment programme holds, with more effective therapy and better capacity, is encouraging, as it could greatly decrease the future burden of HCV-related HCC. However, the long-term impacts of this new treatment programme on the Egypt HCC epidemic have not been adequately quantified, and such insights are needed to inform policymakers and guide future research and prevention. The treatment regimen used in the MOHP treatment programme has been rapidly developing, and generic drugs for sofosbuvir are becoming widely used across the country.19 This changing market landscape, together with the fact that very few of the therapies using generic drugs have been tested for their clinical efficacy, adds additional uncertainty to future patterns of HCV infection and the HCV-related HCC epidemic in Egypt. The sole published study that attempted forecasts of the future epidemic of HCV-related HCC under HCV treatment used limited and now outdated treatment data.13 Therefore, we conducted the present simulation study to produce updated, more realistic results, which quantify likely impacts of the new HCV treatment programme using a series of sofosbuvir-based therapies on Egypt’s future HCC epidemic pattern. We also carried out sensitivity analysis for key parameters of our simulation to test the robustness of our results.
Methods
Model description
We developed a Markov simulation model for HCV-to-HCC progression in MATLAB (V.2017b), from published data on the natural history of HCV infection that was parameterised based on the best available evidence from the Egyptian population (figure 1).7 20 These model parameters were used for both the old and new scenario models. In the old scenario, the old treatment programme was based on PegIFN+RBV and was simulated unchanged through 2050. For the new scenario model, the old treatment programme was maintained until 2015, and then modelled through 2050 under the new treatment scenario that uses sofosbuvir-related therapies and greater population coverage. As compared with the old PegIFN+RBV therapies, which only treat patients with liver fibrosis scores in stages F1–F3, sofosbuvir-related therapies also treat patients in stages F0 and F4 (cirrhosis), as well as with cirrhosis (dashed line, figure 1).21 For these simulations, we assumed that all patient therapy was completed within 1 year.20 Successfully treated people followed the same age-specific and sex-specific mortality pattern of the general population and had a one-time HCV reinfection prevalence of 13%.22 Reinfected patients were treated again in our simulation.5 A proportion of patients had treatment failure, were not treated again and followed the normal HCV-to-HCC transition pattern. The background age group-specific death rates were based on either government census data or the rate of death from cirrhosis or HCC, whichever was greater. Liver transplant for patients with cirrhosis was not considered in the model due to its limited use in Egypt.23 The time horizon of the simulation ended in 2050 considering the changing treatment setting for HCV infection, and the possibility that the incidence of acute HCV infection might change.

Markov model of HCV–HCC disease process. The process of how initially healthy people become chronically infected with HCV, go through fibrosis stages (F0–F3) to cirrhosis (F4), and eventually to HCC. Untreated patients can be successfully treated and then might become reinfected, or they could be the patients for whom the treatment fails (F). Dashed line indicates the newly included patients with HCV who are qualified for treatment in the new treatment programme. HCC, hepatocellular carcinoma; HCV, hepatitis C virus.
Model population and data sources
The Egyptian Demographic and Health Survey 2008 (EDHS 2008) contained the most recent HCV prevalence estimate at a national level. That survey, which tested people 15–59 years old for presence of HCV genetic material and specific antibodies, represented the HCV patient case data for stage-specific infection in 2008. Our simulation added newly infected patients beginning in 2009. We considered three population subgroups as representative of Egypt: HCV-infected people aged 15–59 years in 2008, healthy people aged 5–59 years in 2008 and 5-year-old children cohorts that entered the population each year beginning in 2009. Simulation was carried out on these base cohorts, with no overlap among cohorts or population subgroups.
Population and demographic data for 2008, as well as the projected number of children aged 0–4 years for 2009–2050, were obtained from the United Nations Population Department.24 Apart from the age-specific and sex-specific HCV prevalence from the EDHS survey,25 we applied a constant incidence estimate of acute HCV infection at 2.4 per 1000 person-year,5 in addition to age-specific and sex-specific mortality rates of Egypt’s general population from WHO.26 The age-specific and sex-specific fibrosis progression rates, together with mortality rates of patients with cirrhosis and HCC, were calculated from several other previous studies.13 27 We obtained information on the capacities (number and eligibility of patients treated) of treatment programmes and the success rate of past HCV therapy (PegIFN+RBV) from multiple sources.20 21 28 Because several clinical studies are still ongoing that are evaluating the success rate of the sofosbuvir-based therapies among Egyptian patients with HCV genotype 4, we based our overall success rate of 95% for sofosbuvir-related therapies on published reports among Egyptian populations and expert advice.17 18 29–31 Details of the data used in parameterising the simulation are included in the online supplementary tables.
Supplementary file 1
Main outcome measures
Beginning with the EDHS 2008 data, we estimated from 2009 to 2050 the future patterns of HCC due to HCV infection within the three population subgroups to produce the number of new cases, the annual prevalence and the annual incidence. Two scenarios were simulated: one where the past treatment programme using PEG-IFN/RBV was maintained, and a second in which the new treatment programme with sofosbuvir therapies was initiated in 2015. The new programme differs from the old one in three ways: (A) the patient inclusion criteria were expanded from people with liver fibrosis scores of F1–F3 to F0–F4 patients; (B) the target number of patients treated annually was increased from 55 000 to 350 000; and (C) the new sofosbuvir-related therapies was used to improve overall HCV treatment success from ~62% to ~95%, with 95% based on evidence for DAC/SOF±RBV therapy and expert opinion.18 21 23 30 31 The proportion of patients with hepatitis C treated was estimated for each year based on the preceding year’s number of patients with HCV across all subgroups. The number, prevalence and incidence of cirrhosis and HCC in each year and for both scenarios were simulated. The forecasted number of averted HCC cases during 2009–2050 under the new programme, that is, the total old treatment scenario simulated patients with HCC minus that for the new scenario, was calculated as a measure of the new programme impact.
Sensitivity analysis
The success rate uncertainty of sofosbuvir-based therapies was estimated by varying the base case incidence of acute hepatitis C by ±25%. We performed one-way deterministic sensitivity analysis (DSA) and probabilistic sensitivity analysis (PSA) to evaluate the uncertainty in parameter estimates used during simulations. Parameters evaluated included those for acute hepatitis C incidence, self-clearance of acute HCV infection, rate of reinfection after successful HCV treatment, the number of patients treated annually by the new programme and the success rate of sofosbuvir-related therapies. The forecasted number of averted HCC cases by the new programme was calculated in each simulation as indicator of new programme impact. In one-way DSA, changes in the number of averted cases were estimated by varying ±50% of the range for the number of treated patients annually and for acute hepatitis C incidence, varying between 92.5% and 97.5% for treatment success rate and ±25% of their ranges for all other parameters. Tornado plots were used to present the DSA results. In PSA, 1000 Monte Carlo simulations were performed to allow for the parameters to vary simultaneously based on their different distributions. Scatterplots were used to present the distributions of averted HCC cases in relation to three key parameters of the new treatment programme and hepatitis C epidemic, namely the treatment success rate of sofosbuvir-related therapies, the number of patients treated each year by the new programme and the incidence of acute HCV infection. The distribution and related distribution parameters used in PSA are presented in the online supplementary tables.
Results
HCV incidence at different fibrosis stages
The simulated number of incident HCV cases at different fibrosis stages decreased sharply with the implementation of the new treatment programme (figure 2B) compared with the old scenario with the old programme (figure 2A), except for F0 cases where there were more cases in the new scenario (figure 2B). This forecasted decline for F1–F3 cases under new scenario continued until around 2024, and then stabilised at a low level with a trend of slow increase.
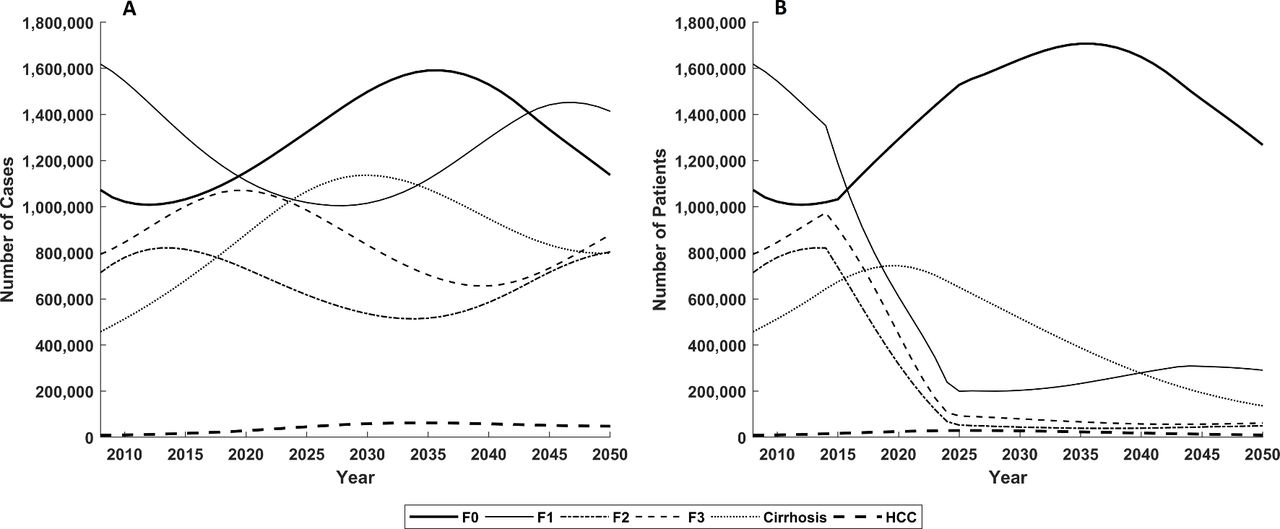
Change in number of HCV-infected patients in different stages in both scenarios. The change in number of patients with HCV in all stages in the future decades, under the old scenario (A) where the old programme is maintained and under the new scenario (B) where the new programme was initiated in 2015. HCC, hepatocellular carcinoma; HCV, hepatitis C virus.
HCC epidemic forecasts
Using scenarios in which different treatment programmes were adopted and with various success rates, the forecasted number, prevalence and incidence of cirrhosis and HCC cases in Egypt were projected each year (figure 3). Under the old scenario, the estimated peak number of new HCC cases (~61 000) would occur in 2034, followed by a slight decrease towards 2050 (figure 3B). The prevalence (figure 3D) and incidence (figure 3F) of newly incident HCC cases peaked around 2032 (~54/100 000) and 2030 (~26/100 000), respectively, and both decreased through 2050. In the new scenario with the implementation of the new programme, the general trajectories of HCC case number, incidence and prevalence were similar, except at much lower levels following implementation of the new programme in 2015, and with their peaks occurring earlier than in the old scenario. Simulation results for cirrhosis cases (figure 3A, figure 3C, figure 3E) followed a similar pattern as for HCC cases. Comparing the results for the old and new scenarios, the new scenario treatment programme averted ~956 000 HCC cases and ~18 million cirrhosis cases during 2015–2050.

Projected case number, prevalence and incidence of cirrhosis and HCC in both scenarios. The simulated number of cirrhosis cases (A) and HCC cases (B), the prevalence of cirrhosis (C) and HCC (D), as well as the incidence of cirrhosis (E) and HCC (F). For the new scenario with the new treatment programme using sofosbuvir-related therapies, high (97.5%) and low (92.5%) overall treatment success rates were assumed in order to evaluate uncertainty in the efficacy of this treatment protocol.
One-way DSA
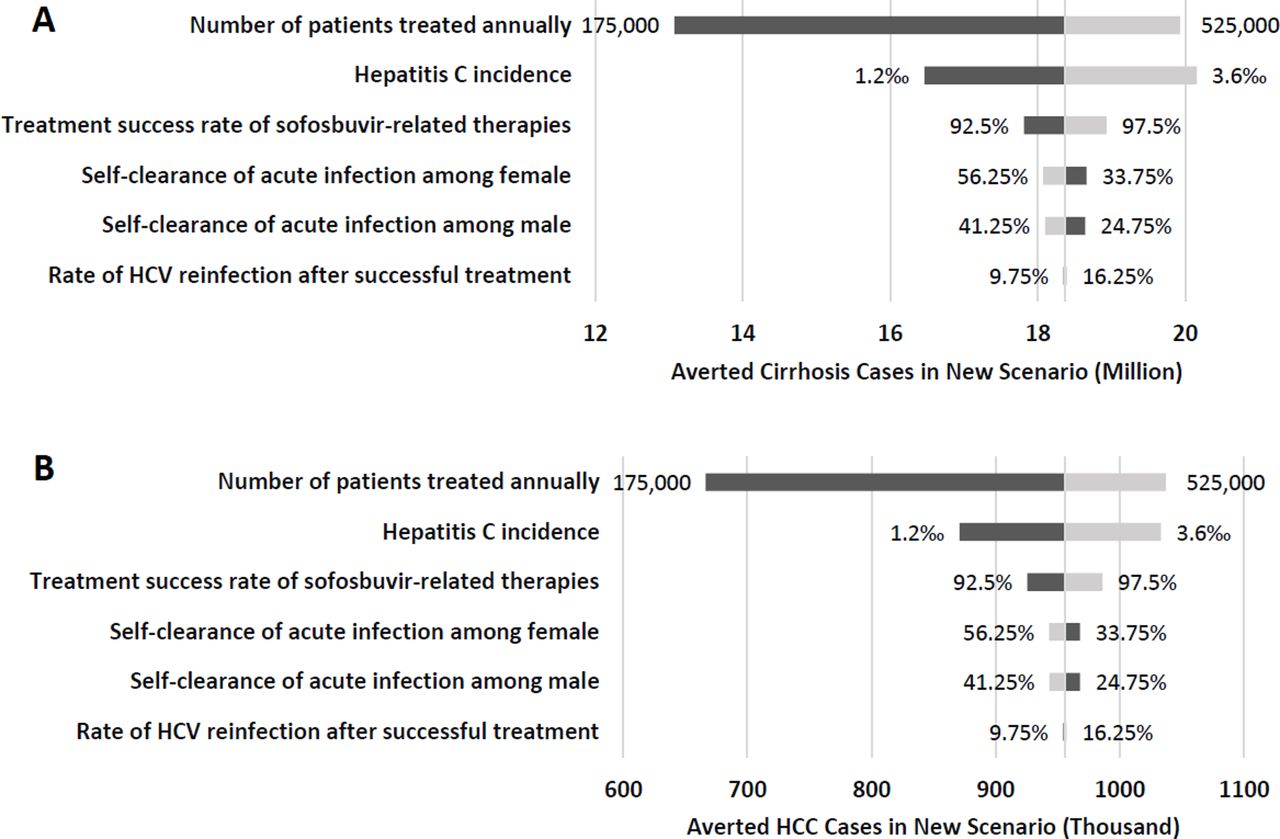
The robustness of the simulation results was evaluated by calculating the number of cirrhosis cases averted and the number of HCC cases averted while varying each of the key parameters within their tested range (figure 4). The number of patients treated annually had the greatest influence on the number of averted cancer cases, followed by incidence of acute HCV infection, and less effect from the success rate of sofosbuvir-related therapies. Self-clearance rates of acute HCV infection had relatively little impact, with that for males being slightly more influential than that for females. The impact patterns of parameter variabilities on averted cirrhosis cases were similar. The influence of sofosbuvir-related treatment success on trends of cirrhosis and HCC was also made evident (figure 3) by varying parameter values between 92.5% and 97.5%. This produced high–low differences ranging ~2 600 HCC cases, a prevalence range of ~2.5 HCC cases per 100 000 people and an incidence range of ~1.1 HCC per 100 000 per year (figure 3B, figure 3D, figure 3F).

Influence on the impact of new treatment programme from single programme parameters. Changes in the forecasted number of averted cases of cirrhosis (A) and of HCC (B) that would occur as the result of differences in key input parameters under the old and new treatment scenarios. The number of averted cases refers to the difference in future cases under the scenario where the old treatment programme was maintained and that in the scenario with the new treatment programme being implemented, that is, the number of cases avoided by the implement of the new programme. Light grey bars indicate the direction and magnitude of change of the number of averted cases when given the input parameter as its maximum tested value, whereas the dark grey bars indicate the direction and magnitude of change of the number of averted cases when given the input parameter as its minimum tested value. HCC, hepatocellular carcinoma; HCV, hepatitis C virus.
Probabilistic sensitivity analysis
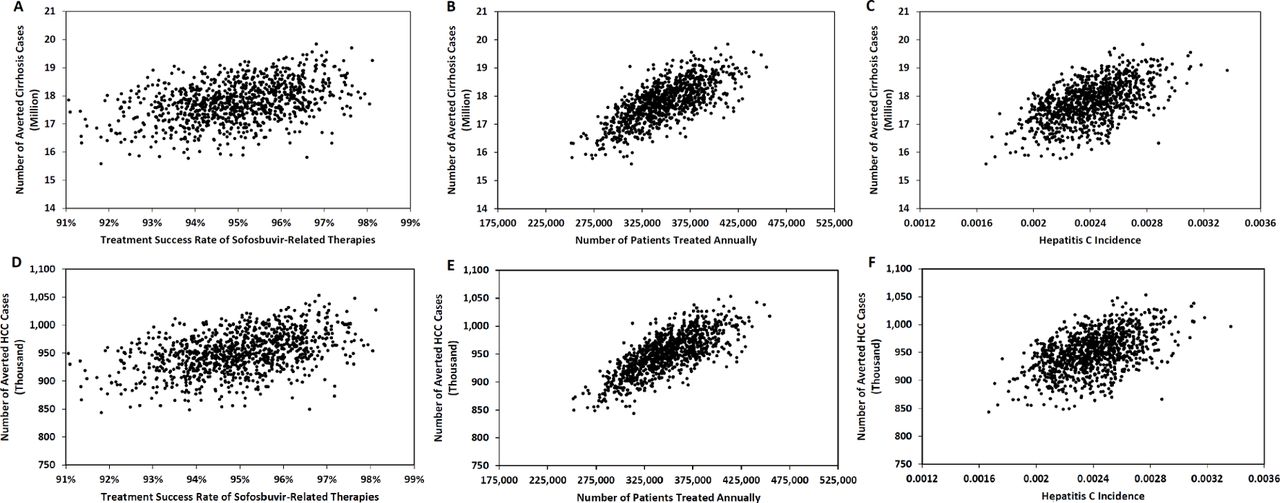
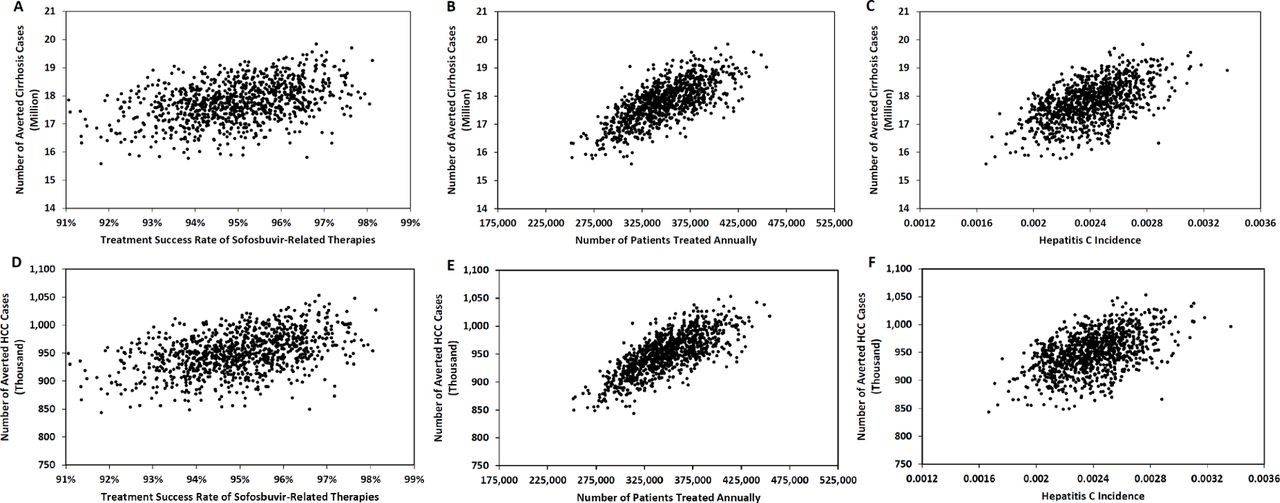
Using 1000 PSA simulations, the numbers of cirrhosis and HCC cases averted under the new programme varied in relation to treatment success, number of patients treated and incidence of acute hepatitis C (figure 5). Overall, these simulations generated a range of averted cirrhosis case numbers between ~15 and ~20 million (figure 5A, figure 5B, figure 5C), and a range of averted HCC case numbers between ~800 thousand and ~1050 thousand (figure 5D, figure 5E, figure 5F). There was a strong positive relationship between the number of patients treated annually by the new programme and averted HCC case numbers (figure 5E). The positive relationship between hepatitis C incidence and averted HCC case number was weaker (figure 5F), and even weaker for the treatment success rate of sofosbuvir-related therapies and number of averted cases with higher level of uncertainty, as reflected in the more scattered distribution pattern (figure 5D). The relationship between averted cirrhosis case number and the three parameters were similar, except with slightly less uncertainty (figure 5A, figure 5B, figure 5C).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Influence on the impact of new treatment programme from multiple program parameters. Changes in the forecasted number of averted cases of cirrhosis (A–C) and of HCC (D–F) in relation to the variation of key input parameters under the old and new treatment scenarios were presented through 1000 PSA simulation results. HCC, hepatocellular carcinoma; PSA, probabilistic sensitivity analysis.
Discussion
The simulation results from this study indicate that the new HCV treatment programme will avert ~956 000 HCC cases and ~18 million cirrhosis cases between 2015 and 2050. Using a Markov modelling approach, which forecasted the future epidemic of HCV-related liver cancer in Egypt, we demonstrated how a new treatment programme is likely to have considerably greater impact than the older programme would have, with more effective sofosbuvir-related therapies and an expanded population being treated. We analysed the evolution of the HCC epidemic from the present to the year 2050, and by comparing the number, incidence and prevalence of HCC cases in Egypt under the two treatment scenarios, we demonstrated that the new treatment programme, if carried out as planned, should substantially reduce the HCV-related HCC epidemic across Egypt by curing patients at an earlier stage and diminishing the number of patients at advanced fibrosis stages.
Today’s HCV epidemic in Egypt is the result of a mass schistosomiasis treatment campaign during the 1950s to 1980s, when improperly sterilised needles were reused.32 Largely due to Egypt’s improved infection control practices in clinical settings,9 decreased HCV seroprevalence among Egyptian blood donors has been observed,33 indicating a lower transmission rate of HCV infection. Nevertheless, HCV-related HCC cases are continuing to rise due to the long delay between infection and appearance of liver cancer. The peak of HCV-related HCC cases around year 2032 forecasted in our model corresponds to results of another study addressing the future disease burden of HCV under the old treatment methods, with predicted HCC cases reaching a plateau during 2020–2030.13 Our more detailed simulation demonstrated that those patients with HCC who comprised this peak mostly consisted of existing HCV infections in 2008, with the latter increase being represented mainly by patients with cancer from the patients with HCV developed from healthy population later in the century, demonstrating the potential future disease burden resulting from both a current high prevalence of HCV and an anticipated future population increase.
Under the new treatment programme, the peak of HCC cases was still predicted, although at reduced and more concentrated levels. The magnitude of this trend depended on the capacity of the new treatment programme, or number of patients with HCV treated each year, with flatter epidemic curves at lower levels as number of treated patients increased. DSA and PSA results showed how changes under the new treatment programme could alter future epidemic patterns. Our analyses also revealed how the effectiveness of the new treatment programme could be compromised by unmet treatment capacity targets or inferior bioequivalence of generic sofosbuvir drugs. In addition, results showed that the forecasted epidemic pattern would change if the true incidence of acute hepatitis C in Egypt were different than current estimates. Specifically, the higher peaks of simulated HCV infection would produce a more severe HCC epidemic, even under the new treatment programme.
The actual treatment capacity (number of patients treated each year) of the new programme is the most important factor that influenced the forecast results and will be influenced by several factors, such as the cost of sofosbuvir-related therapies and the capacity to detect HCV-infected patients who, at early stages, might have few symptoms. When the new programme began (between 2014 and 2015), the producer of sofosbuvir (Sovaldi), Gilead, offered the drug to Egypt at 99% discount,34 which enabled rapid expansion and scale-up of the number of people reached. The recent introduction of generics is also correlated with, and might further accelerate, the decrease in the price sofosbuvir-related therapies,35 which may lead to even better patient access through the new treatment programme. One possible challenge to achieving the targeted high treatment capacity of the new programme involves building and maintaining a competent infrastructure and administration system, which has been the focus of attention since the beginning of the new programme era; relevant efforts have brought about improved patient access and compliance.5 As to successfully identifying patients with hepatitis C patients through population screening programme and timely diagnosis, a nationwide screening programme for HCV infection has been launched at hospitals, universities, and mobile clinics in Egypt but has yet to gather momentum.36 37
There is some uncertainty regarding the incidence of acute hepatitis C in Egypt. The true HCV infection incidence across Egypt is difficult to access, because it relies on national HCV infection surveillance that is not publicly available and whose quality is unknown. Estimates of national-level HCV incidence based on back-calculated HCV antibody prevalence in cross-sectional studies7 may only apply to certain age cohorts who have been through the schistosomiasis treatment era.38 We relied on the few cohort studies from local areas that have been carried out,39 producing results that may not be representative of Egypt as a whole.25 One recent report calculated a whole population incidence of 2.0‰ derived from the Egyptian government’s claim that there are 150 000 newly infected HCV patients each year.29 We used an incidence of 2.4‰ per person-year based on an expert review.5 However, this number might still be an underestimation considering that the cancer incidence we calculated seemed to be relatively low: our HCC estimate was much smaller than a liver cancer incidence level (33.6/100 000) in 2011 calculated from a national population-based cancer registry programme, which was the first and only time liver cancer incidence was calculated on a national level for Egypt.40 This discrepancy might be due to an underestimation of hepatitis C incidence, an overestimation of the treatment success rate of the old programme, or that the model did not include people who were older than 59 years old in 2008. Although values of the parameters related to the old programme came from clinical studies and government reports,21 23 it is difficult to evaluate their accuracy due to lack of disease registries and incomplete surveillance.
The overall success rate of the new sofosbuvir-based and generic sofosbuvir-based therapies was another important parameter influencing the impact of the new treatment programme. As demonstrated by sensitivity analysis, the overall treatment success rate of sofosbuvir-related therapies across all-stage hepatitis patients had a positive association with the number of averted HCC cases. Yet estimations for such efficacy can be difficult considering that Egypt’s recommended national treatment programme has been changing recently between different sofosbuvir-based therapies. With little clinical evidence about efficacy on Egypt’s genotype 4 patients, several generics drugs for sofosbuvir have been used in Egypt, yet their bioequivalency is not fully documented, and other generics may enter the treatment setting in the near future.19 21 23 Moreover, patients’ adherence to hepatitis C treatment may also have an impact on the overall treatment success rate of sofosbuvir-related therapies, which would be an important topic in future studies.
Despite the realism and complexity of our model and forecasts, some limitations and assumptions should be kept in mind. First, we did not evaluate changing HCV transmission. Because the new programme is treating many hepatitis patients, HCV transmission should decrease somewhat, thereby further enhancing the treatment programme. Second, we did not distinguish between compensated and decompensated patients with cirrhosis, who might experience different disease progression rates and response to treatments. Epidemiological data that support the differentiation between these two groups among the Egyptian population was limited, and although this differentiation is often important for disease burden analysis, this was not the primary concern of the present study. Finally, we assumed that patients for whom treatment failed would not have another chance to be treated, which might not be the case as the overall hepatitis burden declines.
Our report represents the first study to define and quantify the impacts of the new hepatitis C treatment programme on the epidemic of HCC in Egypt. In so doing, we have quantified several influential parameters that will affect the future HCC epidemic. Our simulations provided updated forecasts well into the future that are consistent with the best understanding and available data, rather than providing highly precise predictions requiring more variables that are not now obtainable. We produced a timeline for how the new hepatitis C treatment programme will decrease the HCV-related HCC epidemic in the coming decades, as well as the impact from two important programme components, namely the number of patients treated annually and the treatment success rate.
Conclusion
Our analysis provides a framework for population-level, public health policy decisions and identifies needs for improved disease registry, surveillance and research. Overall, our simulation results suggest promising benefits to Egypt in controlling its HCC epidemic if the new HCV infection treatment programme with sofosbuvir is maintained or expanded. We highlighted the value of enhanced studies on HCV transmission across Egypt and of expanding simulations using accurate and detailed treatment success rates for different HCV patient groups.
Acknowledgments
We would like to thank Dr Ahmed Cordie, who provided updated information on the ongoing clinical studies in Cairo. Dr David Hutton from the Department of Health Management and Policy at the University of Michigan School of Public Health provided useful suggestions for the modelling approach in MATLAB. We would also like to thank other doctors and staff at Gharbiah Cancer Society and Cairo who helped the data collection and the access to relevant background information, as well as other support they provided to this study.
References
Footnotes
Handling editor Seye Abimbola
Contributors WM, ASS, WAA and MLW contributed to the conception and design of the study. AH, MR and IAS monitored the field surveillance and integrity of the data. WM and AH. MR and IAS were involved in data acquisition and management. TBED contributed to the understanding of current pattern of hepatitis C treatment in Egypt. WM and MLW were responsible for statistical analysis, interpretation and the report draft. All authors contributed to revisions and the final version.
Funding This study was funded by University of Michigan Office of Global Health. This study also received funds from Cancer Epidemiology Education in Special Populations (CEESP) Program of the National Cancer Institute (Grant R25 CA112383).
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Model files and data available on request.