Article Text

Abstract
Background Universal health coverage (UHC) is difficult to achieve in settings short of medicines, health workers and health facilities. These characteristics define the majority of the small island developing states (SIDS), where population size negates the benefits of economies of scale. One option to alleviate this constraint is to import health services, rather than focus on domestic production. This paper provides empirical analysis of the potential impact of this option.
Methods Analysis was based on publicly accessible data for 14 SIDS, covering health-related travel and health indicators for the period 2003–2013, together with in-depth review of medical travel schemes for the two highest importing SIDS—the Maldives and Tuvalu.
Findings Medical travel from SIDS is accelerating. The SIDS studied generally lacked health infrastructure and technologies, and the majority of them had lower than the recommended number of physicians in a country, which limits their capacity for achieving UHC. Tuvalu and the Maldives were the highest importers of healthcare and notably have public schemes that facilitate medical travel and help lower the out-of-pocket expenditure on medical travel. Although different in approach, design and performance, the medical travel schemes in Tuvalu and the Maldives are both examples of measures used to increase access to health services that cannot feasibly be provided in SIDS.
Interpretation Our findings suggest that importing health services (through schemes to facilitate medical travel) is a potential mechanism to help achieve universal healthcare for SIDS but requires due diligence over cost, equity and quality control.
- health policy
- health systems
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known about this topic?
Much analysis of the medical travel market has identified that medical travel is growing, although at a slower pace than originally projected.
A systematic review of medical travel literature observed that the effects on the originating (importing) countries’ health system were mainly perceived as negative. These include patients returning with complications, rising costs and lack of regulation in the industry.
However, findings across the different studies suggested that the impact on a country’s health system depends on the context and capacity.
What are the new findings?
The multicountry analysis presented here is the first of medical travel among small island developing states (SIDS), and the findings confirm that the import of health services among SIDS has occurred at a slower pace than the projected rise of the global medical travel industry.
The non-linear growth of medical travel among SIDS gives evidence that the industry is volatile to external shocks, which is a factor that needs to be taken into consideration by SIDS considering import as a mechanism to increase access to health services.
While existing literature notes the scarcity of institutionalised arrangements for medical travel, our findings highlight the success of three government-funded schemes among SIDS. The Tuvalu Medical Treatment Scheme spent 44.5% of its health budget on overseas treatment in 2013, while the Maldivian government spent $11.6 million on subsidised medical travel in 2012 and highly specialised treatment worth $1.53 million per annum was funded by the Seychelles government.
Key questions
Recommendations for policy
In settings with small health systems and extreme resource constraints, state- led strategic importing of health services using regional integration could be a potential mechanism to help achieve universal health coverage in SIDS. However, appropriate due diligence over cost, equity and quality control needs to be taken to minimise the perceived negative consequences from this trade.
Introduction
Universal health coverage (UHC) refers to a healthcare system that provides coverage of quality healthcare and financial protection to all citizens of a country.1 It has become the globally accepted concept for advocating access to, and affordability of, healthcare and is recognised in the Sustainable Development Goals.2 For countries to achieve UHC, a set of prerequisites are needed, such as political will and stakeholder support for predominantly public sector funding.3 The WHO also proposes four essential attributes for achieving UHC: an efficient and well-run health system; an affordable and equitable system for financing; access to essential medicines and technologies; and a sufficiently trained and motivated health workforce.3
Shortages of medicines, health workers and health facilities are major impediments to moving towards UHC and are characteristics that typify most small island developing states (SIDS). Thirty-nine countries are defined as SIDS, characterised by their narrow economic base, high production costs, shortage of skilled labour and heavy dependence on trade and foreign aid.4 5 The majority of SIDS receive high levels of overseas development assistance, and bilateral and multilateral trade has been one strategy that SIDS have used to overcome domestic shortages.6 While there are benefits to trade, there is a clear need for caution when liberalising trade, including healthcare. Walls et al7 highlight that trade negotiations themselves, and the ongoing management of trade agreements once signed, can become a burden on the governments of smaller and poorer states. Yet, there is a dearth of systematic cataloguing and analysis of trade policy initiatives and their impact on health systems, leaving an incomplete picture of their nature and effects.8 This is especially true when it comes to SIDS, and this is the gap that this paper seeks to fill through the comparative analysis of the experience of a large group of SIDS.
Cross-country comparison of health system performance, if undertaken appropriately, can provide a powerful method for identifying strengths and weaknesses of reforms relevant to similar settings.9 This paper presents a cross-country comparison focused on medical travel to understand the pattern of consumption of health services abroad by SIDS, mapping the linkages between the import of health services and the health indicators relevant to achieving UHC. On this basis, we analyse how import of services through public medical travel schemes affects access to quality health services and UHC for SIDS.
Methods
Study design
Quantitative analysis was conducted on sets of longitudinal secondary data on health-related travel and health indicators covering the period 2003–2013. A review of policy documents was used to understand, where possible, the reasons for the observed trends and patterns identified by the quantitative analysis. The study covered all SIDS that are member states of the UN and that reported health-related travel data to the International Monetary Fund (IMF), which are presented in table 1.
Characteristics of small island developing states (SIDS)
We developed a framework for analysis based on the WHO building blocks framework (2007),10 reflecting the four core dimensions of UHC (table 2). Two health indicators per dimension were selected, based primarily on data availability. To understand the relationship between each dimension of UHC and the import of health services, each pair of indicators was then mapped onto the outcome variable ‘health-related travel expenditure (HRT)’, for the period 2003–2013.
Indicators addressing key health system attributes for universal healthcare
Sources of data
Data for the study were obtained from three sources: the IMF, the World Bank (WB) and the WHO. Data addressing the main outcome variable, ‘Health-related travel expenditure $’ were obtained from the IMF databank online. From the annually published balance of payments (BOP) data by the IMF, the item ‘Health-related travel expenditures (personal) in current USD’ was acquired for the years 2003–2013 for all the SIDS that reported these data. In the BOP, the item is presented under ‘Current Account/Goods and Services/Services/Travel/Personal/Health related, Debit, US Dollars’ for expenditures. According to the BOP manual, the travel component covers the goods and services acquired from an economy by travellers during visits of less than 1 year in that economy.11 Four broad approaches are used by Member States to measure travel expenditure, and the table in online supplementary annex 1 summarises the sources and methodologies used by the selected SIDS to report health-related travel data to the IMF. The WB data bank provided country-level indicators for the years 2003–2013 on health expenditure public (as a proportion of total health expenditure (THE)) (2003–2013), and out-of-pocket expenditure (OOP) health expenditure (as a proportion of THE) (2003–2013), while statistics from WHO (2015) were used to obtain indicators on health infrastructures and health technologies, health personnel and service coverage indicators. The two highest importers having the steepest rises in per capita HRT during the study period were selected, and policy documents relating to these two countries by three international donor agencies (WHO, WB and IMF) were reviewed (table 3 summarises the documents reviewed for each country).
Supplementary file 1
Sources of data for qualitative analysis
Data management and analysis
The unit of analysis is the country. HRT per capita was derived by dividing HRT by the total population for each year. Median, IQR and percentages were used to describe data. Bubble charts that can show the relation between three different sets of variables were used to map the linkages between health indicators and health-related travel. Where indicator data were available for a certain year(s), the HRT data in the bubble represent the same year(s) as the indicators on the x and y axes. In this analysis, the x and y axes present the related indicators, and the data points represent the location of the country with regard to the indicators on the axes. The size of the bubble represents the amount spent on medical travel against the backdrop of each system needed for UHC. For instance, countries scoring high on skilled birth Attendents (SBA) and antenatal care (ANC) indicators show a strong, efficient and well-run domestic health system, while the size of the bubble would be an implication of the deficiencies in that system.
Role of the funding source
The funding source did not have any involvement in the design, collection, analysis and interpretation of the data presented in the paper or in the decision to submit the paper for publication. However, the salary of the corresponding author was covered by the funding source. The corresponding author confirms that she had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Results
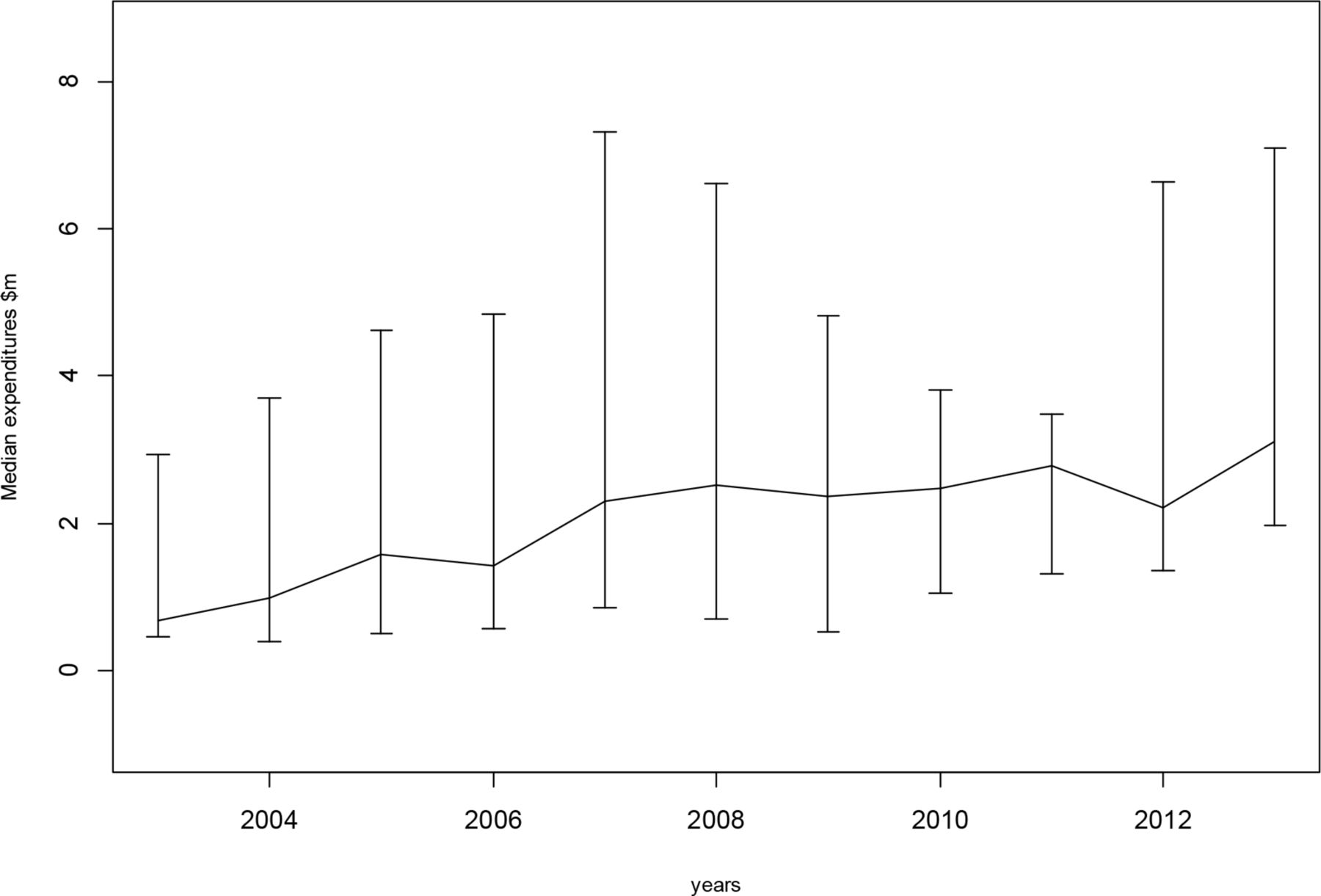
Fourteen of the 39 SIDS reported health-related travel data to the IMF. As shown in figure 1, a rising trend was observed in health-related travel expenses over the 10-year period across the 14 countries. Median expenditures across the countries rose 4.5 times between 2003 and 2013, from $0.68 to $3.11 million, while a few SIDS were found to have extremely high per capita expenditure (figure 2).

Trend of expenditure on health-related travel among 14 SIDS, 2003–2013. SIDS, small island developing states.

Per capita health-related travel expenditures among 14 small island developing states, 2003–2013.
Although expenditure on health-related travel by the SIDS increased over time, it was not linear for any country. Notable fluctuations in medical travel were observed for many countries, particularly from 2009 to 2012, which may reflect issues of data quality or reporting. By 2013, Tuvalu, the Maldives and the Seychelles were observed to be the top importers of health services among the SIDS. While it is beyond the scope of this paper to explore the individual travel growth patterns of SIDS, we examined the relationship between health-related travel and health systems of these countries.
Table 4 indicates that all SIDS perform well on the service coverage indicators that were used to represent a well-running health system, except for Guinea Bissau, which had very low access to skilled birth attendance. In health financing, WPRO SIDS generally perform better than other regions with high public expenditure and very low OOP. Tuvalu had almost 100% of its health expenditures borne by the government. Health infrastructures and technologies range on average 1–10 hospitals per 100 000 populations and 0–13 CTs per one million populations respectively. Access to health workforce were lowest in Guinea Bissau (0.7 and 5.9) and Cape Verde (3.1 and 5.6), while it was highest in Bahamas (28.2 and 41.4).
Performance of SIDS across systems required for UHC
Figures 3–6 show HRTs among SIDS mapped across the health systems indicators identified for UHC dimensions in our framework.

Health-related travel against health service coverage indicators, 2007– 2014.

Average expenditure on health-related travel per capita versus health financing structure, 2003–2013.

Average health-related travel per capita versus health workforce, 2005–2013.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
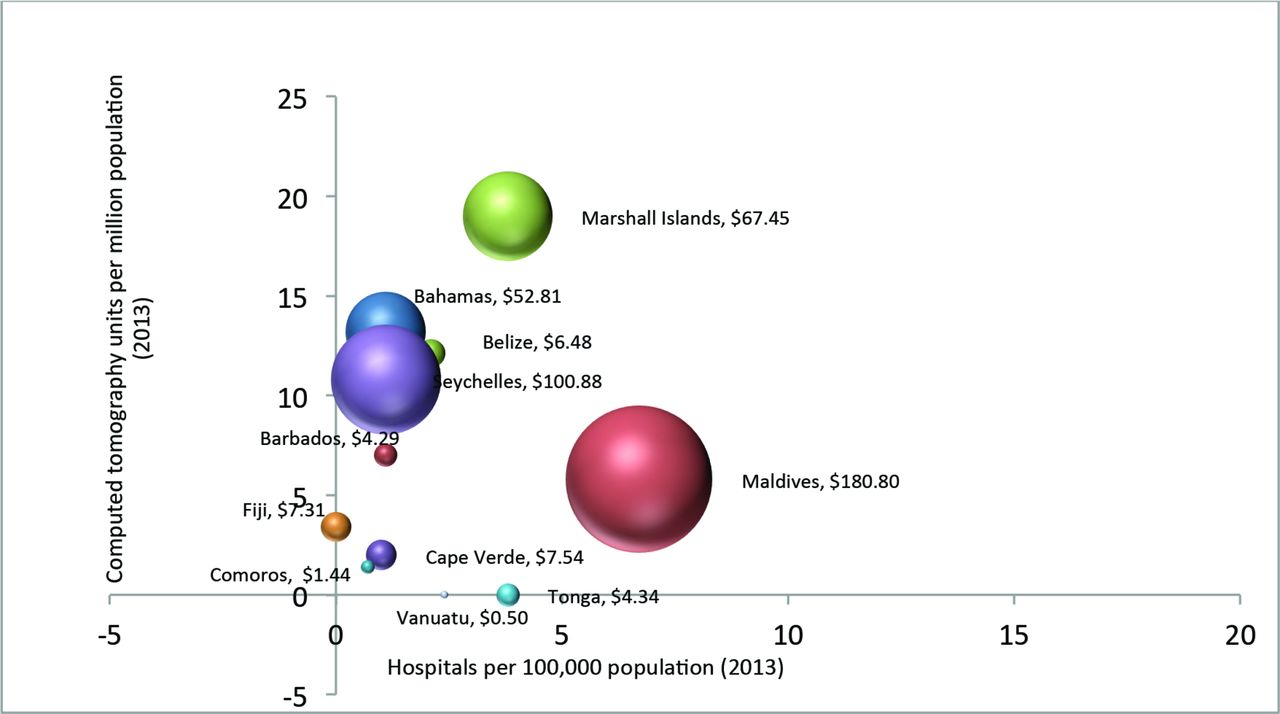
Expenditure on health-related travel per capita versus density of health infrastructure and technologies, 2013.
Mapped across the health service coverage indicators, all SIDS were seen to perform well on coverage. The Maldives and Tuvalu, represented by the largest two bubbles, are observed to perform better on service indicators than the lowest importers of health services (Comoros and Vanuatu). Outliers Guinea Bissau and Vanuatu, which had lower levels of service coverage compared with other SIDS, also experienced low levels of import of health services.
A more linear pattern was observed between the public health expenditure and OOP health expenditure. Two large bubbles (the Maldives and Bahamas) were found at high levels of OOP spending. The largest bubble representing Tuvalu had very high levels of public health spending and very low OOP spending. Among the lowest importers of health services, Vanuatu had a very low OOP and high public expenditure on health, while Comoros’s health financing indicators were very low on both indicators.
Health-related travel mapped across the health workforce indicators showed that the largest bubbles were located at higher levels of nursing and midwifery personnel and around 10–15 physicians per 1000 population. The Bahamas and the Marshall Islands had very contrasting levels of health workforce but experienced similar levels of HRT. The majority of the bubbles were located where health workforce was lower than 13.9 physicians and 28.6 nursing personnel per 10 000 population, which are the global averages for the two indicators. Thus, these countries have lower than the recommended WB ratio of 23 doctors, nurses and midwives per 100 000.
Based on the two indicators used to represent health infrastructures and medical technology, all SIDS faced shortages in health infrastructure and technologies that may reflect the small populations these countries serve. Both large and small bubbles were located where hospitals per 100 000 population were less than 10 and access to technologies were less than 20 units per 1 million population. These were however above the global medians of 1.1 hospital per 100 000 population and 3.8 units per 1 million population.
Table 5 provides a description of medical travel schemes in the two SIDS, Tuvalu and the Maldives, which the quantitative analysis demonstrated had the highest and most fluctuating trends during the study period. It shows that through medical travel, both the Maldives and Tuvalu appear to have increased access to health services unavailable within each country previously, which may have been spent from out-of-pocket. With the government directly approaching foreign health providers, the Maldives compared with Tuvalu is found to be providing a more comprehensive set of services to a greater number of patients at a smaller per capita health budget. However, the multilateral approach by Tuvalu has the ability to reduce the burden of OOP as it covers the full cost of travel episode and offers services of foreign specialists through the scheme.
Description of public schemes for medical travel in Tuvalu and Maldives
Discussion
Based on analysis of 14 SIDS, there appears to be a gradual but fluctuating trend of medical travel. Analysis of medical travel vis-à-vis core health system dimensions required to achieve UHC identified major shortages in the areas of health infrastructure and technology. At the same time, coverage of (more limited) services that the countries are able to provide is exceptionally high. While Tuvalu and the Maldives were found to be the top importers of healthcare, and experienced the most significant growth in medical travel, this appears to be due to the public funding available to facilitate this. Although their approach, design and performance were slightly different, the two public schemes in Tuvalu and the Maldives suggest how an increase in access to health services may be achieved through medical travel. This study suggests that strategic importing of health services could be a promising mechanism to help SIDS achieve UHC.
Much analysis in medical travel literature has identified that it is growing, although at a slower pace than originally projected, with specific regional and heterogeneous patterns, and that it is a diverse industry.8 12–14 The analysis presented here is the first of medical travel among SIDS, and findings confirm this heterogeneous pattern.15 Analysis of data from 140 economies in the travel and tourism competitiveness report of 2011 indicates that the industry has witnessed contractions since 2009 due to the global economic crisis, volatile oil prices, climatic disturbances, multiple security incidents and pandemics16 may explain the non-linear growth of medical travel across SIDS.
The SIDS analysed here generally lacked health infrastructure and technologies that will affect their capacity to achieve UHC. However, this is not inherent in all SIDS. Countries such as Belize ($0.1 million), Barbados ($2.4 million), Cape Verde ($0.01 million), Tonga ($0.006 million) and Tuvalu ($0.004 million) have innovatively earned an income from health-related travel as well. According to the BOP manual, income covers two types of transactions between residents and non-residents; compensation of employees paid to non-resident workers and investment income receipts and payments on external financial assets and liabilities. Reports of income generated directly by medical tourism in SIDS is very rare except for few cases such as by the island state of Penang in Malaysia, which contributes more than 50% of the country’s medical tourism market with seven of its hospitals actively involved in medical tourism.17 The growth of medical tourism in Barbados serving the Carribean, Mexican and the British patients have also been highlighted, although monetary benefits have not been mentioned.18 These bidirectional flows of trade in health services deserve greater investigation to understand better the factors that allow SIDS to act as exporters of services.
The three largest ‘bubbles’, representing high levels of per capita medical travel spending, by Tuvalu ($156.9), the Maldives ($113.2) and the Seychelles ($100.8) had public funds available for medical travel, which implies that medical travel is facilitated by the availability of government subsidy. The Tuvalu Medical Treatment Scheme (TMTS) signed between Tuvalu and overseas hospitals in the region spent 44.5% of its health budget on overseas treatment in 2013,19 while the Maldives under its scheme ‘Aasandha’ spent $11.6 million on subsidised travel in Indian and Sri Lankan hospitals in 201220 and treatments worth $1.53 million per annum are funded by the Seychelles government.21 Evidence has shown that public financing for health has the potential to reduce inequities, and an investigation of equity measures with regard to public financing of overseas treatment in the Maldives has been reported elsewhere. Investments in highly technological specialist care in very small populations, and geographical formations of these island nations may not be economically feasible. Yet, the cost-effectiveness of public financing for health-related travel needs to be explored and compared with alternatives such as the establishment of services locally.
The examples of Tuvalu and the Maldives demonstrate that access to health services that were not feasible to be established in these countries can be provided through the import of health services. Analysis of claims data from the National Social Protection Agency of the Maldives showed that the number of beneficiaries subsidised for treatment abroad increased by 199% and average expenditure per beneficiary increased 49.7% during 2010 and 2013.22 The TMTS, introduced in 2005, has increased its expenditure from approximately $0.3 million to $1.5 million in 2013, and a preliminary analysis of the expected reforms of the scheme suggests that a per-patient saving of $A 15 000 can be achieved by the government of Tuvalu by referring cardiac cases to India.19 These public schemes were different in approach, design and coverage. With a direct government to foreign provider approach, the Maldives appears to be providing a more comprehensive set of services to a greater number of patients at a smaller per capita health budget, while the multilateral approach by Tuvalu is likely to have contributed to reducing the burden of OOP maintained at an average of 0.1% over the past decade. The lack of a private sector in the Tuvaluan health system and predominant public funding of health services also contribute to this. Both the schemes have attracted critique from international organisations such as the IMF and WB, and policy documents of Tuvalu and the Maldives have highlighted the opportunity cost of these schemes. These costs include: lost incentive to improve or expand access to the domestic health system, lost continuums of care, maldistribution and skill mix imbalances of health workers23 and cost of complications that has to be borne by domestic health systems.24 In the Maldives, the cost of the scheme itself is very high, whereby the median expenditure per beneficiary has increased from $605 in 2010 to $739 in 2013.25 The Maldives health policy notes by the WB questioned the fiscal sustainability of the scheme in the long run calling for negotiated close-ended package rates with foreign providers and for targeted subsidies for highly complex treatments only.20 The health master plan of the Maldives 2016–2025 has also cautioned the tendency of overutilisation of services due to the perception that the current scheme is ‘unlimited’, which has resulted in inefficient use of resources especially in the absence of a gate-keeping system.26 The IMF in its latest country report of Tuvalu noted the potential overspending of the TMTS programme and advised the authorities to improve the cost-effectiveness of its policy. The strategic health plan of Tuvalu 2009–2018 further noted that the TMTS put a significant drain on public resources threatening its ability to maintain other health services in the country.27 28 Hence, maintaining a balance in the ratio of expenditure on preventive and curative healthcare is vital if import of health services is implemented as a solution to achieve UHC.
This study relies on international indicators that have limitations in methodology and application in different countries. A review of literature that used indicators as a measurement of health system performance showed that there were differences in the adoption of indicators by developing and developed countries29 and the composition of SIDS in this study included high-income, upper-middle-income, low-and-middle-income and low-income countries, which may limit the generalisability of study findings. We address the issue of data in online supplementary annex 1, which details data sources used by the SIDS to report to the IMF. Data on the volume of travel may have given better insight on trends in medical travel. The IMF member states have also used combination of methods to report travel data, which may result in underestimation or over-estimation of travel data in these countries. However, this study has used panel data of travel expenditures of 10 years and, where possible, panel data of indicators too, to minimise such overestimations and underestimations reflected in 1 or 2 years of data.
Conclusion
The trend in health-related travel among SIDS has over the last 10 years followed the global trend—rising yet heterogeneous. The pattern also demonstrated a volatility to global events, a factor that needs to be taken into consideration by SIDS considering import as a mechanism to increase access to health services.
SIDS generally lacked the health technologies needed to achieve UHC. The two island states with the highest per capita expenditures on the import of health services had publicly funded schemes to manage the process. Assessment of the Tuvaluan and Maldivian public schemes to subsidise medical travel have demonstrated that access to specialised, technology-driven health services can be increased through import of health services. Our findings suggest that import of health services is a potential mechanism to help achieve UHC but highlight the need for due diligence over cost, equity and quality control.
References
Footnotes
Handling editor Seye Abimbola
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All the data used in this study are publicly available.