Article Text

Abstract
Background Multimorbidity, the presence of two or more non-communicable diseases (NCD), is a costly and complex challenge for health systems globally. Patients with NCDs incur high levels of out-of-pocket expenditure (OOPE), often on medicines, but the literature on the association between OOPE on medicines and multimorbidity has not been examined systematically.
Methods A systematic review was conducted via searching medical and economics databases including Ovid Medline, EMBASE, EconLit, Cochrane Library and the WHO Global Health Library from year 2000 to 2016. Study quality was assessed using Newcastle-Ottawa Scale. PROSPERO: CRD42016053538.
Findings 14 articles met inclusion criteria. Findings indicated that multimorbidity was associated with higher OOPE on medicines. When number of NCDs increased from 0 to 1, 2 and ≥3, annual OOPE on medicines increased by an average of 2.7 times, 5.2 times and 10.1 times, respectively. When number of NCDs increased from 0 to 1, 2, ≥2 and ≥3, individuals spent a median of 0.36% (IQR 0.15%–0.51%), 1.15% (IQR 0.62%–1.64%), 1.41% (IQR 0.86%–2.15%), 2.42% (IQR 2.05%–2.64%) and 2.63% (IQR 1.56%–4.13%) of mean annual household net adjusted disposable income per capita, respectively, on annual OOPE on medicines. More multimorbidities were associated with higher OOPE on medicines as a proportion of total healthcare expenditures by patients. Some evidence suggested that the elderly and low-income groups were most vulnerable to higher OOPE on medicines. With the same number of NCDs, certain combinations of NCDs yielded higher medicine OOPE. Non-adherence to medicines was a coping strategy for OOPE on medicines.
Conclusion Multimorbidity of NCDs is increasingly costly to healthcare systems and OOPE on medicines can severely compromise financial protection and universal health coverage. It is crucial to recognise the need for better equity and financial protection, and policymakers should consider health system financial options, cost sharing policies and service patterns for those with NCD multimorbidities.
- public health
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known about this topic?
Patients with multimorbidity are disproportionately financially burdened due to complex health needs and high healthcare utilisation.
Medicines constitute the largest proportion of out-of-pocket expenditure (OOPE) for patients with multimorbidity.
Current health systems fail to provide sufficient financial protection for OOPE on medicines.
What are the new findings?
There was an association between level of multimorbidity in patients and out-of-pocket expenditure (OOPE) on medicines. More multimorbidities were associated with higher OOPE on medicines as a proportion of total healthcare expenditures by patients.
Even with the same number of non-communicable diseases (NCD), certain specific combinations of chronic conditions yielded higher OOPE on medicines.
The elderly were more vulnerable to higher OOPE on medicines, while some evidence suggested medicine OOPE accounted for a greater proportion of income for low-income groups.
In patients with multimorbidity, non-adherence was a coping strategy for OOPE on medicines, with adverse health consequences.
Recommendations for policy
It is crucial to recognise the need for better equity and financial protection, and policymakers should consider health system financial options, cost sharing policies and service patterns for those with NCD multimorbidities.
Policymakers should move from a single-disease framework to one that takes into account multimorbidity, when allocating funds and when designing policies aimed at financial protection.
Targeted government funding and support programmes should take into account multimorbidity status of individuals, particularly for the elderly and low-income groups who are most vulnerable to OOP hardships.
Policy measures could include exemptions from certain costs for the elderly and low socioeconomic status groups, lower caps on copayments and subsidies for vital drugs.
Prescription drug cost sharing benefit plans must be designed to provide enhanced and broadened coverage for multimorbidities, particularly for certain NCD combinations.
A crucial clinical implication relates to the need for better clinical prescription guidelines to prevent prescription of unessential medicines and generic drugs for chronic illness which may cause unwarranted expenditures on medicines by patients.
Introduction
Non-communicable diseases (NCD) are the leading cause of morbidity and mortality globally.1 The United Nations and the World Health Organization(WHO) have established coordinated responses to address NCDs worldwide.2 3 A particular challenge with NCDs is multimorbidity, the presence of two or more NCDs.4 Patients with multimorbidity are disproportionately burdened with illness, and economically, due to complex needs and high healthcare utilisation.5 A study of six low-middle income countries (LMIC) found that the highest contribution to out-of-pocket expenditure (OOPE) in patients with multimorbidity was on medicine.6 Using nationally representative data, a study in the USA found that elderly patients with three or more NCDs used five or more prescription drugs, revealing that medicines contributed to high healthcare expenditure by patients.7
Given the scale of the healthcare and financial burden of NCDs, understanding the financial burden on patients with multimorbidity, particularly on medicines, is crucial when developing strategies towards universal health coverage (UHC), which aims to provide access to health services, including medicines, without financial hardship, and in order to ensure equity in financial protection.8 A review on the global impact on NCDs on impoverishment revealed that OOP medical expenditures drive households into financial catastrophe and impoverishments.5 In many LMICs, health systems fail to protect individuals from OOPE on medicines due to inequitable financing, where insurance schemes or benefits packages do not cover all essential medicines, or patients have to incur substantial copayments.6 9 A study in rural India found medicines accounted for 49% of total aggregate OOPE for illnesses.10 Patients in developed countries also incur large OOPE for medicines. A 2003 survey of Medicare beneficiaries in the USA aged above 65 years showed that more than one-quarter had no prescription coverage, and almost half of low-income seniors in selected states lacked coverage for medicines.7 Inadequate insurance that covers inpatient and outpatient services but not costs of medicines is likely to worsen access to medicines.11
This review contributes to the existing literature by investigating evidence on the relationship between multimorbidities and OOPE on medicines. To date, existing reviews have only examined the overall economic burden of NCDs in countries, but not OOPE incurred by individuals.5 12 13 Other studies have investigated total OOPE on healthcare overall, but not on medicines alone specifically.14 15 To address this knowledge gap, we conducted a systematic review of published studies and synthesised current literature on OOPE on medicines by patients with NCD multimorbidities.
Methodology
We followed the methods detailed in a peer-reviewed systematic review protocol that is registered with PROSPERO (registration CRD 42016053538). We systematically searched electronic databases (Ovid Medline, Cochrane Library, EconLIT, EMBASE, WHO Global Health Library) in January 2017 for articles published from 1 January 2000 to 31 December 2016. We only included studies from year 2000 onwards to concentrate on recent relevant studies. Bibliographies of included articles were searched for additional articles that met inclusion criteria.
Search strategy involved keywords and Medical Subject Headings. Search strategies were tailored to each database. Online supplementary appendix pp 1–4 describes detailed search strategies for each database. In summary, keywords used for identifying NCD multimorbidity included ‘Chronic disease’, ‘Chronic condition’, ‘Chronic illness’, ‘Multimorbid’, ‘Multimorbidity’ and ‘Non-communicable’; keywords for identifying medicines were ‘Prescription drug’, ‘Medicine’, ‘Drug’, ‘Pharmaceutical’ and ‘Polypharmacy’; and keywords for identifying outcome measure of OOPE were ‘Out-of-pocket’, ‘Financial’, ‘Utilisation’, ‘Health expenditures’, ‘Health care cost’ and ‘Drug cost’.
Supplementary file 1
Inclusion and exclusion criteria
Table 1 shows our detailed inclusion and exclusion criteria.
Inclusion and exclusion criteria for reviewed studies
Study selection
Two independent reviewers reviewed titles and abstracts. Subsequently, article full texts were screened for eligibility. Any disagreements were resolved through consultation with a third reviewer.
Data extraction
Information extracted from articles included reference information, population and study settings, study design and data sources, key findings on relationship between OOPE for medicines and multimorbidity, and other secondary outcomes including medicine utilisation for multimorbidity, coping strategies for OOPE on medicines and OOPE for other healthcare services.
Currency of OOPE
For comparability, all OOPE on medicines was converted to 2015 US$. This was done by using Purchasing Power Parity Indices to convert costs from one country to another (in this case, the USA), and subsequently the overall US Consumer Price Index (CPI) was used to convert historical costs to 2015 US$.16 17 If the year of OOPE was not specified in the article, we calculated OOPE based on the year of data collection (eg, survey year). OOPE was reported to the nearest dollar.
Calculations of OOPE as a proportion of mean annual national average wages
All selected articles had results on OOPE on medicines, but a few did not clearly specify absolute amounts (eg, OOPE reported as percentage of income). Hence, we contacted authors of the latter subset of articles. As a result, we had absolute amounts of OOPE on medicines (for different numbers of multimorbidities) for 11 of our 14 included studies. One of these 11 of 14 studies reported absolute OOPE on medicines for last outpatient visit, and the remaining 10 of 14 studies reported absolute annual OOPE on medicines.
We obtained annual national average wages (2015) (calculated by OECD: average wages are obtained by dividing the national-accounts-based total wage bill by the average number of employees in the total economy, which is then multiplied by the ratio of the average usual weekly hours per full-time employee to the average usual weekly hours for all employees) from the OECD,18 and mean annual household net disposable income per capita from OECD.19 Subsequently, using the 10 studies that reported annual OOPE on medicines, we calculated OOPE on medicines as a proportion of annual national average wages, and OOPE on medicines as a proportion of mean annual household net adjusted disposable income per capita, to allow comparability between settings and years.
Quality evaluation
The Newcastle-Ottawa Scale (NOS) is a well-established quality assessment tool for observational studies,20 21 which we used to evaluate the quality of studies included in this review. We modified the tool to suit our specific purposes by designing questions directly addressing OOPE and NCDs (online supplementary appendix pp 5–6). We assessed quality of articles in three categories—population selection, comparability and outcome measures. Under population selection, we assessed if population studied was nationally representative, how NCDs were measured (eg, self-reported) and how multimorbidities were classified (eg, 0 NCD, 1 NCD, 2–3 NCDs, 4–6 NCDs). For comparability, we assessed if studies might have incurred bias as a result of study design and analysis. For outcome measures, we assessed if measurement of OOPE for medicines was reliable (eg, self-reported or verified with administrative data).
We measured six items in the NOS quality assessment tool: four items for population selection, one item for comparability, one item for outcome. A maximum of 1 point can be awarded for each item. The NOS scale can have a maximum of 6 points total. A score was computed by adding the number of points. Studies were categorised into high (4–6 points), moderate (3 points) and satisfactory (0–2 points) quality.
Statistical methods
Due to considerable heterogeneity of studies for OOPE on medicines, meta-analysis of OOPE on medicines was precluded. We discussed our findings narratively and presented median and IQR of absolute OOPE on medicines calculated from our included studies, stratified by number of NCDs.
In addition, for each study that provided absolute mean annual OOPE on medicines for different numbers of NCDs, we calculated the ratios of absolute mean annual OOPE on medicines across groups with different numbers of NCDs, relative to the group with the fewest NCDs, for comparability within studies. For example, for an article that reported absolute mean annual OOPE for 0 NCD, 1–2 NCDs and ≥3 NCDs, we calculated the ratio of absolute mean annual OOPE on medicines for ≥3 NCDs to absolute mean OOPE on medicines to 0 NCD, as well as the ratio of absolute mean annual OOPE on medicines for 1–2 NCDs to absolute mean annual OOPE on medicines for 0 NCD.
Results
A total of 7340 records were identified from database searches. After removing duplicates, there were 6667 records, which were screened based on titles and abstracts. Of these, 209 full-text articles were assessed for eligibility. Figure 1 shows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow chart. Fourteen primary articles met the eligibility criteria and were included in this review.22–35
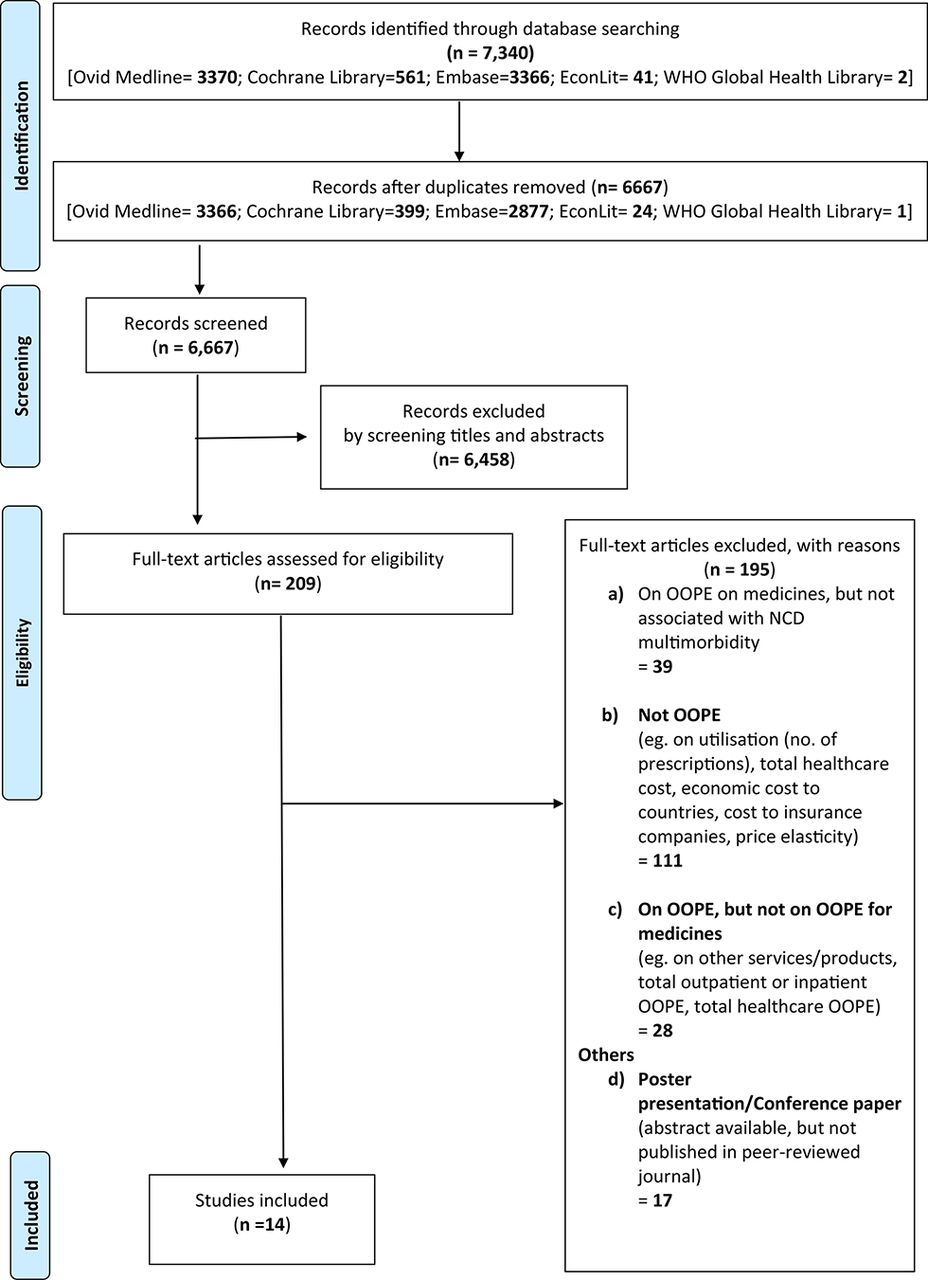
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow chart. NCD, non-communicable disease; OOPE, out-of-pocket expenditure.
Characteristics of included articles
Characteristics of the 14 selected studies are summarised in table 2.22–35 Eight of 14 articles were published between 2011 and 2016, three between 2006 and 2010, and three between 2000 and 2005. Six studies were conducted in the USA, two in Canada, one in Australia, four in South Korea and one in India. All articles were observational. Three articles studied populations of all ages, four studied elderly populations ≥65 years and seven studied those aged between 18 and 64 years.
Characteristics of selected articles (n=14)
Thirteen of 14 articles studied multimorbidity based on number of NCDs, while the remaining one article studied specific combinations of NCDs. In general, articles studied OOPE on medicines for zero, one, two and three or more NCDs. The majority (11 of 14 papers) of studies referred to NCDs as ‘chronic conditions’ or ‘medical conditions’. Two studies defined NCDs as conditions that had lasted, or were expected to last, 12 or more months and resulted in functional limitations, and/or a need for ongoing medical care. One study defined them as chronic conditions that lasted or expected to last 3 or more months. Four of 14 articles did not specify the list of NCDs studied; for the remaining 10 papers, five papers included a full list of self-reported NCDs that were studied, while five papers stated the most prevalent self-reported NCDs. The most common NCDs studied were diabetes, hypertension, stroke, arthritis and respiratory disease.
Quality of included articles
Online supplementary appendix p 7 shows the scoring for quality assessment, where studies were categorised into high (4–6 points), moderate (3 points) or satisfactory (0–2 points) quality. Median and mean quality scores for eligible studies were 3.5 and 3.4, respectively, with 50% of articles categorised as high quality. All papers, except the three papers classified as satisfactory quality, were nationally representative. Eleven of 14 papers (80%) only measured NCDs with self-reporting. Six of 14 papers did not compare results with a reference group without NCDs (ie, they examined OOPE for different numbers of multimorbidities (eg, 2 NCDs, 3–5 NCDs, and so on) but did not compare with patients with 0 NCD).
Out-of-pocket expenditure on medicines
Table 3 summarises key results on OOPE on medicines by numbers of multimorbidities.
Primary outcomes
Absolute OOPE on medicines
Ten of 14 articles provided absolute amounts of annual OOPE on medicines. In all 10 studies, a greater number of NCDs were associated with a larger absolute annual OOPE on medicines, and hence, as a proportion of annual national average wages, and proportion of mean annual household net adjusted disposable income per capita.
Figure 2 shows the associations between numbers of multimorbidities, and OOPE on medicines as a proportion of annual national average wages, and proportion of mean annual household net adjusted disposable income per capita.

{kind=link}
{kind=link}
OOPE on medicines as a proportion of annual national average wages, and mean annual household net disposable income per capita, by numbers of multimorbidities, for studies with absolute annual OOPE on medicines 1Population aged <65 2 Population aged ≥65 ACS Acute Coronary Syndrome ACS+Acute Coronary Syndrome with asthma and osteoarthritis Diabetes+ Diabetes with gastro-oesophageal reflux disease and depression. NCD, non-communicable disease ; OOPE, out-of-pocket expenditure.
When number of NCDs increased from 0 to 1, 2 and ≥3, annual OOPE on medicines increased by an average of 2.7 times, 5.2 times and 10.1 times, respectively. When number of NCDs increased from 0 to 1, 2, ≥2 and ≥3, individuals spent a median of 0.36% (IQR 0.15%–0.51%), 1.15% (IQR 0.62%–1.64%), 1.41% (IQR 0.86%–2.15%), 2.42% (IQR 2.05%–2.64%) and 2.63% (IQR 1.56%–4.13%) of mean annual household net adjusted disposable income per capita, respectively, on annual OOPE on medicines.
The magnitude of OOPE increment as number of NCDs increased varied among studies. In Crystal et al’s study,22 a high-quality paper from the USA on a nationally representative survey on Medicare beneficiaries aged 65 years and above, annual OOPE on medicines was 2.5 times (US$254), 3.7 times (US$379), 5.6 times (US$581) and 7.7 times higher (US$791) for those with 1, 2, 3–5 and >5 NCDs, respectively, compared with those with no NCDs (US$103). Jung et al’s study,35 a moderate-quality paper from Korea on a nationally representative population aged 20 and above, reported that absolute amounts of annual OOPE on medicines, compared with those with 1 NCD (US$82), were 1.9 times (US$156) and 3.2 times higher (US$260) for those with 2 and ≥3 NCDs, respectively.
One study, by Kemp et al 28 from Australia, ranked in the satisfactory-quality category, which conducted a nationally representative survey of households and individuals across Australian states and territories, examined multimorbidity by specific disease clusters, in addition to examining number of NCDs. With the same number of NCDs, certain combinations of NCDs had higher OOPE on medicines than others. The article compared patients with diabetes only (one NCD) with those with three NCDs (diabetes with depression and gastro-oesophageal reflux disease), and compared patients with acute coronary syndrome (ACS) (one NCD) with those with three NCDs (ACS with asthma and osteoarthritis). Those with ACS (either alone or in conjunction with others) experienced greater OOPE compared with patients with diabetes (either alone or in conjunction with others).
OOPE on medicines as proportion of total healthcare expenditure by patients
Four papers studied the share of OOPE on medicines in total healthcare expenditure by individuals and households. In general, patients with more multimorbidities experienced higher OOPE on medicines, as a proportion of total OOPE on healthcare and medical services by patients. Paez et al 27 studied elderly subjects aged more than 65 years in the USA and reported that annual OOPE on medicines as a proportion of total healthcare expenditures by patients increased from 31.5% (zero NCD) to 50.5%, and to 63.5%, for one and two NCDs, respectively.
Impact of age on OOPE on medicines
Three articles by Hwang et al,23 Paez et al 27 and Campbell et al 29 (two high-quality category and one satisfactory-quality category, respectively) investigated differences in OOPE on medicines among elderly and the young. All three studies consistently showed absolute annual OOPE on medicines for subjects aged older than 65 years was higher than those aged less than 65 years, at every multimorbidity level. In Hwang et al’s study23 for subjects aged less than 65 years, annual OOPE on medicines was US$62, US$166, US$345 and US$669 for zero, one, two, and three or more NCDs, respectively, whereas for those aged above 65 years, annual OOPE on medicines was higher at US$171, US$354, US$661 and US$1006 for zero, one, two, and three or more NCDs, respectively.
Increased financial burden of lower income groups
Ruger and Kim’s study,26 a paper ranked as high quality, using the Korean National Health and Nutrition survey, found that patients from lower income quintiles suffered greater OOPE burden ratios (ratio of average OOPE to individual’s share of household income). The authors reported that OOPE burden ratios for subjects of the lowest income quintile were 6.0, 22.6, 27.4 and 37.7 for patients with zero, one, two, and three or more NCDs, respectively. OOPE burden ratios for subjects from the highest income quintile experienced lower burdens of 1.4, 3.3 and 4.9 for zero, one and two NCDs, respectively, and even dropped to 3.9 for those with ≥3 NCDs.
Secondary outcomes
Online supplementary appendix pp 8–11 summarises secondary outcomes. Five papers studied the association of multimorbidity with medicine utilisation. Consumption of medicines increased with multimorbidity. In Hennessy et al’s study,34 as the proportion of household income spent on OOPE on medicines increased from 0 to 0%–5% to >5%, mean number of medications used increased from 4.0 to 3.9 to 6.9, respectively. Two papers, both ranked as satisfactory quality, studied coping strategies for OOPE on medicines. Non-adherence to medicines was the coping strategy for high OOPE incurred by patients. Campbell et al 29 found 37.7% of respondents who reported financial barriers to medications stopped taking their prescribed medications. Hennessy et al 34 found that 5.2% of individuals spending less than 5% of their income on OOPE on medicines, and 21.5% of individuals spending more than 5% of their income on OOPE on medicines, reported non-adherence.
Online supplementary appendix pp 12–13 displays which primary and secondary outcomes were reported by each of the 14 papers.
Discussion
Summary and interpretation of findings
A greater number of multimorbidities were associated with higher OOPE on medicines. This finding could be explained by polypharmacy worsening with more NCDs, which gives rise to higher OOPE on medicines. The problem of polypharmacy may be a result of single-disease guidelines applied to multimorbid patients, even though such guidelines were designed based on frameworks that excluded patients with multimorbidities.4 6 Some evidence from our results suggested that with the same number of NCDs, specific combination of NCDs yielded higher OOPE on medicines. This is likely due to certain NCDs requiring more medicines or more expensive medicines than others. A greater number of multimorbidities were also associated with higher OOPE on medicines as a proportion of total healthcare expenditures by patients, which may have implications that multimorbid patients with higher OOPE on medicines had to allocate less resources to other medical services.
We also found that absolute OOPE on medicines for the elderly was higher than the young, at every multimorbidity level, indicating that being older is associated with being more vulnerable to higher OOPE on medicines, consistent with other studies showing that the elderly tend to suffer from higher medicine utilisation and healthcare expenditures.36 Some evidence from our study also suggested that OOPE on medicines accounted for a substantially greater proportion of income for low-income groups. Our results are consistent with findings from other systematic reviews on high susceptibility of household impoverishment from poor management of NCDs in low-income group.5
Non-adherence to medicines was found as a common coping strategy for OOPE on medicines and polypharmacy, a finding consistent with other papers, which will have adverse consequences on patient outcomes.37
Strengths and limitations
Our paper is the first systematic review examining OOPE on medicines for multiple chronic conditions. We conducted an extensive search via medical and economic databases, including grey literature, through the use of precise search terms and application of stringent inclusion criteria.
A limitation was OOPE on medicines not being studied specifically with multimorbidity (eg, in association with Charlson Comorbidity Index, an indication of NCD severity, but not number of NCDs). Hence, there is a need to address these gaps in future studies by examining OOPE specifically, and how OOPE is associated with different numbers and types of NCDs. Another limitation was that most eligible articles examined numbers of NCDs without reporting the exact chronic conditions. Future studies should examine specific NCDs with a view to understanding which NCDs may yield higher OOPE on medicines.28 The number of NCDs and OOPE were mostly self-reported and may be subject to greater under-reporting of NCDs in persons from lower socioeconomic background.
Regarding quality assessment of included articles, the NOS is an established and well-used quality assessment tool for non-randomised studies. The NOS has potential limitations as questions over the validity of the scale have been raised,38 and we adjusted the NOS to meet our analysis, specifically altering the grading categories to match NCD measurement rather than a specific exposure, and remove questions relating to follow-up. Nonetheless, with a descriptive analysis, the NOS is very useful in providing comparison between studies reported, and our adjustments to the NOS are in line with assessing the key biases potentially present (including selection, measurement and representativeness).
Policy implications
Individuals suffering from multimorbidities may have greater OOPE on medicines due to their complex treatment needs. Despite increasing prevalence of multimorbidity, current health policies and clinical practices rely on a single-disease specific approach. This may suggest to policymakers to move from a single-disease framework to one that takes into account multimorbidity, when allocating funds and when designing policies aimed at financial protection. Low socioeconomic status groups whose high rate of NCDs and low incomes result in more price-sensitive behaviour, as well as being more sensitive to the ill effects of high cost sharing, may need priority attention.5 In addition to NCD multimorbidity, vulnerable groups may experience a double burden from NCDs and infectious diseases, which may drive patients into further impoverishment.39 Targeted government funding and support programmes should take into account multimorbidity status of individuals, particularly for the elderly and low-income groups who are most vulnerable to OOP hardships.
In considering a policy response to the financial burden and impoverishment from OOPE on medicines for multimorbidity, there may be a need for policy interventions to account for the underestimation of the problem in standard measures, owing to the impact of coping strategies (eg, non-adherence). For example, vulnerable and marginalised groups may not even seek healthcare and hence will not be prescribed medicines, resulting in the under-representation of the true extent of multimorbidity and potential implications for OOPE on medicines.40 Policy measures could include exemptions from certain costs for the elderly and low socioeconomic status groups, lower caps on copayments and subsidies for vital drugs. Prescription drug cost sharing benefit plans must be designed to provide enhanced and broadened coverage for multimorbidities, particularly for certain NCD combinations.
There are also important clinical implications of OOPE in patients with multimorbidity. The literature shows a trend that multimorbidity in family practice is now the norm rather than the exception.41 Clinicians need to consider the financial burden incurred by patients with multimorbidity due to polypharmacy, and the risks of non-adherence and foregoing medicines as coping strategies. Another crucial clinical implication relates to the need for better clinical prescription guidelines to minimise prescription of unnecessary medicines for chronic illness which may cause unwarranted expenditures on medicines by patients.6 42
Conclusion
Multimorbidity of NCDs is increasingly costly to healthcare systems and OOPE on medicines can severely compromise financial protection and UHC. The evidence reviewed here shows the relationship between multimorbidity and OOPE on medicines. It is crucial to recognise the need for better equity and financial protection, and policymakers must examine health system financial options, cost sharing policies and service patterns for those with NCD multimorbidities.
Acknowledgments
Thanks to Dr Deirdre Hennessy and Dr Anna Kemp for providing additional study information.
References
Footnotes
Handling editor Seye Abimbola
Contributors JTL, CM, and GS contributed to the conception and design of this research. GS performed the literature search and extracted data from individual studies. GS and TH conducted the data analysis and interpreted the data. GS wrote the first draft of the paper. All authors revised the first and subsequent drafts. All authors contributed to the interpretation of the findings and revised the manuscript for important intellectual content.
Funding GS is funded by the President’s Graduate Fellowship, National University of Singapore. JTL is funded by the Ministry of Education (MOE) Tier 1 Grant, Singapore. CM is funded by NIHR Research Professorship.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.