Article Text

Abstract
Background Published evidence on the drivers of absenteeism among the health workforce is mainly limited to high-income countries. Uganda suffers the highest rate of health workforce absenteeism in Africa, attracting attention but lacking a definitive ameliorative strategy. This study aimed to explore the underlying reasons for absenteeism in the public and private ‘not-for-profit’ health sector in rural Uganda.
Methods We undertook an empirical qualitative study, located within the critical realist paradigm. We used case study methodology as a sampling strategy, and principles of grounded theory for data collection and analysis. Ninety-five healthcare workers were recruited through focus groups and in-depth interviews. The NVivo V.10 software package was used for data management.
Results Healthcare workers’ absenteeism was explained by complex interrelated influences that could be seen to be both external to, and within, an individual’s motivation. External influences dominated in the public sector, especially health system factors, such as delayed or omitted salaries, weak workforce leadership and low financial allocation for workers’ accommodation. On the other hand, low staffing—particularly in the private sector—created work overload and stress. Also, socially constructed influences existed, such as the gendered nature of child and elderly care responsibilities, social class expectations and reported feigned sickness. Individually motivated absenteeism arose from perceptions of an inadequate salary, entitlement to absence, financial pressures heightening a desire to seek supplemental income, and educational opportunities, often without study leave.
Conclusion Health workforce managers and policy makers need to improve governance efficiencies and to seek learning opportunities across different health providers.
- health workforce
- absenteeism
- public sector
- private sector
- Uganda
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known about this topic?
Sickness and work-related stress are the leading causes of health workforce absenteeism in high-income countries, especially among nurses working in hospital settings, but little is known of the reasons for health workforce absenteeism in low-income and middle-income countries.
What are the new findings?
Weak health workforce governance in the public sector, depicted through inefficient management of workers’ salaries, inadequate infrastructure, low financial allocation for managing primary healthcare services, and insufficient supplies of essential medicines and supplies, is the main underlying reason for workforce absenteeism.
Social-cultural norms accepting of absenteeism and societal expectations pressured healthcare workers to influence their absence motives.
Effective workforce supervision, as depicted in the private non-profit sector, is critical to minimising absenteeism.
Recommendations for policy
There is potential for health sector learning on workforce governance models for mitigating absenteeism.
Urgently, there is need for advocacy and actioning the efficient payment of healthcare workers’ salaries to minimise productivity losses from absenteeism, resulting in staff shortages and the compromised quality of patient care.
Introduction
The prevalence of health workforce absenteeism in Uganda is estimated to range between 37% and 48%.1–3 High absenteeism among Ugandan doctors has been associated with delays in the provision of care and adverse outcomes for mothers and neonates.4 The reduction of health workforce absenteeism from 48% to 20% has been a priority for Uganda’s health sector since 2010, tracked through annual monitoring indicators.5–8 However, there is no corresponding strategy. The absence of a guiding strategy is in part attributable to a limited understanding of the underlying causes of health workforce absenteeism9 10 and the poor implementation of absenteeism policies as articulated in Uganda’s Public Service Standing Orders.11
Among the key drivers of absenteeism in low-income countries is the phenomenon of health workforce dual practice12–14—holding two or more concurrent jobs—as a means of compensating for low salaries in the public sector. In low-income countries, dual practice arises principally from healthcare workers’ perceptions of organisational injustice,13–15 and specifically the perceived inadequacy of working conditions and unfair pay.16–20 Also contributory are scheduled or unscheduled attendance to ‘off station’ duties, such as training workshops and immunisation outreaches,18 19 social activities, including prayers, burials and weddings,21 22 and administrative duties at the decentralised government.18 However, many surveys in these settings commonly report unknown reasons.1 18 23
Typically, several low-income countries define health workforce absenteeism as the proportion of healthcare workers unavailable at a health facility at one or two audit visits conducted by external supervisors such as policy makers19 24 or researchers.1 18 20 Using the audit method, also termed the Public Expenditure Tracking Survey (PETS),20 24 interviewers ask healthcare workers found on duty to list all missing or absent colleagues and to provide reasons why they are absent. The PETS surveys report the same reasons for health workforce absence in low-income countries as those found in the literature.18 19 21–23 25
Although important for understanding the non-availability of the health workforce in low-income countries, the PETS audit method is prone to reporting and social desirability biases. For example, healthcare workers may have an incentive to provide or withhold potentially incriminating information regarding a colleague’s absence. Also, the design inherently lacks validation of findings, which could be improved through accessing workers’ schedules and conducting follow-up interviews with absentees. Consequently, PETS overestimates health workforce absenteeism, reporting rates above 40% in countries where ‘off station’ working is common, such as in Uganda, Bangladesh1 and Tanzania,18 while in countries where out-of-station working is uncommon, such as Laos People’s Democratic Republic (PDR), rates are as low as 17%.20
In contrast, absenteeism data in high-income countries are mainly obtained from healthcare organisation sickness registers,26–28 sickness benefits registers,29–31 insurance records32 and interviews with healthcare managers.33 34 Absenteeism is computed as the work-time lost due to absence,35 36 thereby measuring both non-availability and productivity loss. However, data from these sources assume that absenteeism is due to sickness or work-related stress/injury.37 Moreover, only medically certified absenteeism (typically lasting 3 days or longer) is notifiable in many healthcare organisations,27 38–40 thus failing to detect short-term, often motivated absenteeism.21 41 Yet there is growing evidence in several countries of the Organisation for Economic Co-operation and Development such as Australia, the UK, USA, Canada and the Netherlands that health workforce absenteeism is due to reasons other than sickness.42–46 Nonetheless, the empirical evidence is often limited to nursing professionals working in urban hospital settings10 21 47 and is almost exclusively from high-income countries.21 48
To contribute to the limited evidence, we undertook a qualitative approach to explore the reasons and motives of front-line and supervisory healthcare workers’ engagement in absenteeism in rural Uganda. The rural setting was of relevance because health workforce absenteeism is understood to worsen existing workforce shortages,49–51 potentially widen inequalities in accessing healthcare52–54 and negatively impact on quality and outcomes of care.55
A number of theoretical frameworks have been used to analyse absenteeism across sectors, especially the ‘withdrawal’ or motivational model,56 the work-stress or sickness model,9 57 and the rational choice economic model applied to labour market forces.58 59 The withdrawal model suggests that individual absence such as lateness, absenteeism and turnover manifests in avoidance of dissatisfying work environments and conditions.35 56 Relatedly, the rational choice model suggests that individuals absent voluntarily when they perceive their jobs as secure, such as for tenured compared with contractual workers,58 and if their skills are in high demand, such as for the highly skilled migrant health professionals.60 The two preceding theories have the motivational construct central to explaining a worker’s absence. Contrary, the work-stress and sickness models suggest that individuals absent themselves when job resources are overshadowed by job effort, leading to strain, stress and consequently injury or disability.9 38 57 The empirical findings of this study were evaluated for how well or not they aligned to these prominent individual-focused absenteeism models.
Methods
Study setting and participants
Uganda’s population has more than doubled since 1990 from 16.1 to 36.6 million, reflective of the 10th highest fertility rate globally at 5.8 children per childbearing woman.61 Over half (52%) of its population is aged 14 years or younger,62 signifying a high child dependency on healthcare services. Yet Uganda has a low per capita income; in 2015, its gross domestic product purchasing power parity was US$1850, which was less than half that of neighbouring Kenya.63
However, available evidence suggests that the relative size and specialisation of the health workforce have not markedly grown to match the increasing population health needs. For example, the public healthcare workforce vacancy rate was 31% and 44% in 2015 and 2010, respectively.5 8 Similar to other regions globally, health workforce shortages are most severe in rural settings, where the demand is highest for subsidised public healthcare services52 64–66 (see online supplementary appendix and figure 1 for summary on the organisation of Uganda’s health system).
Supplementary appendix
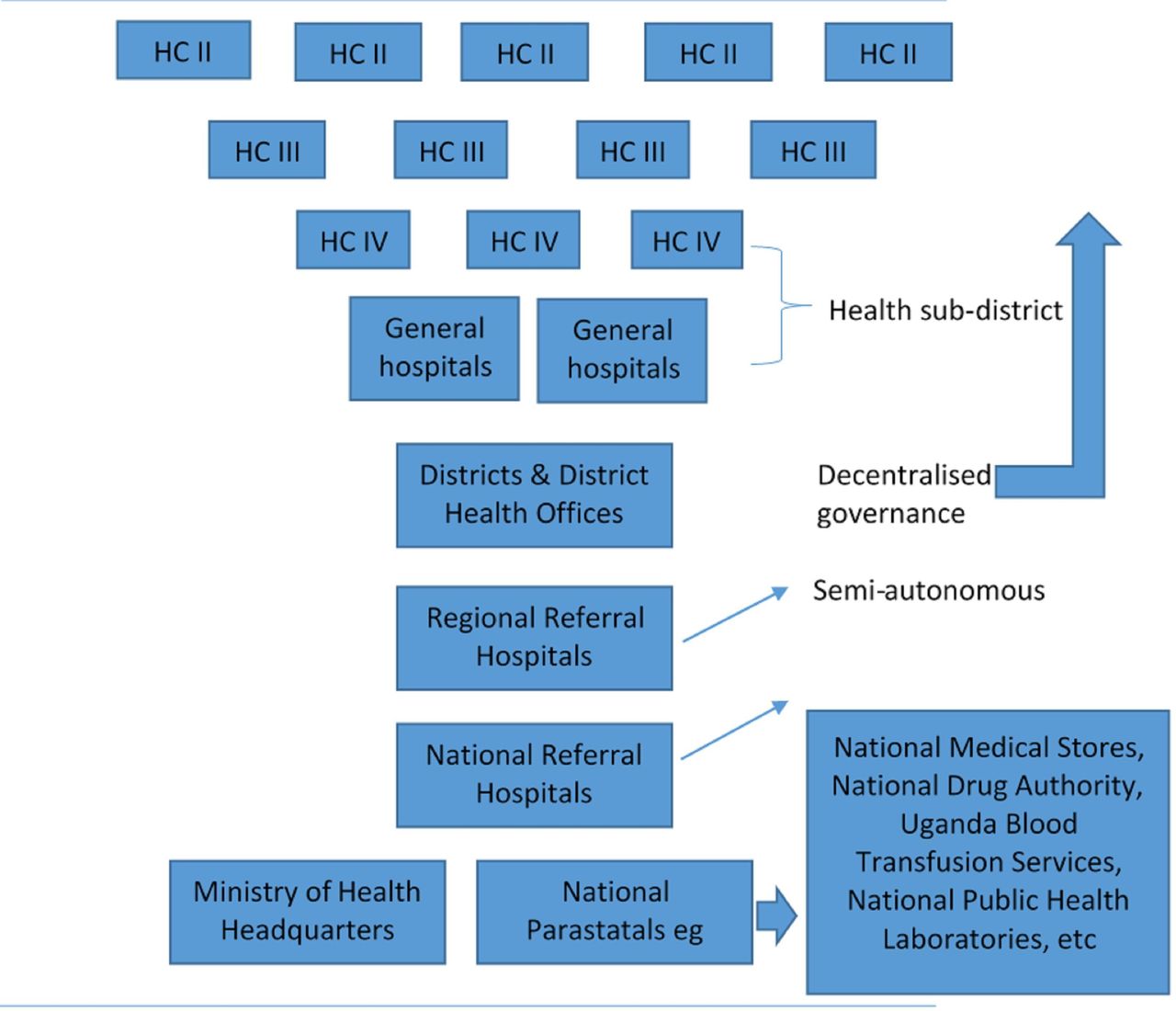
The health infrastructure in Uganda. HC, health centre.
Methodology
A qualitative approach was used, located within critical realism theory, central to which is the notion that knowledge about a social phenomenon such as absenteeism can be accessed with a reasonable degree of certainty.67 68 For example, critical realism theory asserts that knowledge about the existence of contributors to and the underlying mechanisms that generate absenteeism is real and exists independent of a researcher’s interpretation of it.69 Therefore a triangulation of data sources and data collection methods are essential for increasing the validity and reliability of findings within this approach.68 70
Sampling and recruitment
A case study design was used for the sampling strategy.71 72 A case was defined as a rural referral-level health facility. First, sampling at the district level involved listing all the 19 typical rural districts of central Uganda. Subsequently, three neighbouring districts with comparable health system infrastructure (a combination of public and private not-for-profit (PNFP) health facilities at referral level) were identified and purposively selected.
For the identification of cases, the sampling criteria included presence of referral-level health facility; health centre (HC IV) or district hospital, and health facility ownership, public or PNFP. A scoping review of the literature from various service sectors conducted prior to the empirical study (unpublished data, R Tweheyo, 2017) indicated that characteristics such as organisational size, public or private sector employment, and permanent or fixed-term contracts affected employee absenteeism.73 At the individual level, the sampling criteria included a qualified healthcare worker (not nursing assistant) who was not on annual leave during the study period. Maximum variation sampling was used to purposively access participants from five cases (three public and two PNFPs). A total of 95 healthcare workers were recruited using three strategies summarised in tables 1 and 2.
Characteristics of respondents
Data collection strategies
The participants of the ‘scoping focus groups’—focus group discussions used to explore topical issues and modalities for planning individual interviews—were independent of those involved in subsequent interviews. However, about one-third of the participants of the in-depth interviews were invited and participated in the ‘credibility check focus groups’—focus group discussions used for validating the findings of the individual interviews. As such, the credibility check focus groups had a mix of previous in-depth interviewees and new participants.
Data collection, management and analysis
All interviews were audio-recorded. Focus groups were conducted in Luganda, the local dialect, with the aid of one native research assistant, while in-depth interviews were held in English. All focus groups excluded supervisors, deliberately involving only front-line workers to avoid evoking fear of being reported and possible apprehension by health managers. Verbatim transcription was completed in the field to provide contemporaneous coding of emerging themes based on the research questions. Interview topic guides were adapted on the basis of emerging findings, and interviews were conducted until data saturation was achieved. In-depth interview and focus group transcripts were entered into NVivo V.10 QSR International software, indexed by type of case and interview, to allow for both method and data analysis triangulation. Coding queries were run to generate substantive codes, for example, ‘what cadre of healthcare workers report an experience of absenteeism?’ coded as ‘public clinician absence’ and ‘private nurse-midwife absence’. Subsequently, line-by-line data coding was done alongside memoing of contextual and emerging insights from transcripts and field notes.
The constant comparative method of analysis, a principle of classic grounded theory,74 was used to compare incident codes from the first case (public hospital) with the subsequent incident codes from all cases until data saturation was achieved. The public hospital, the two public health centres and the two PNFPs (hospital and HC IV) formed three somewhat distinct categories for comparison. Consequently, these three categories constituted the between-case analysis, while explanators were obtained mostly within cases. Finally, a codebook (coding summary) was printed to ease merging of codes for synthesising into core categories. Exemplar and deviant quotes of participants’ narratives are selected from the memos to illustrate the emergent themes. The main narratives from in-depth interviews were compared with those in focus groups. After synthesis from the analysis, the final stage was to derive overall explanators, achieved through an evaluation to assess fit or misfit of study findings against existing absenteeism theoretical models in various disciplines. These included the work-stress or sickness absence model,9 75 the withdrawal or motivational model (using the theory of planned behaviour),35 76 and the rational choice economic model in relation to the labour market approach.77 78
Ethics approval
All participants provided written informed consent.
Results
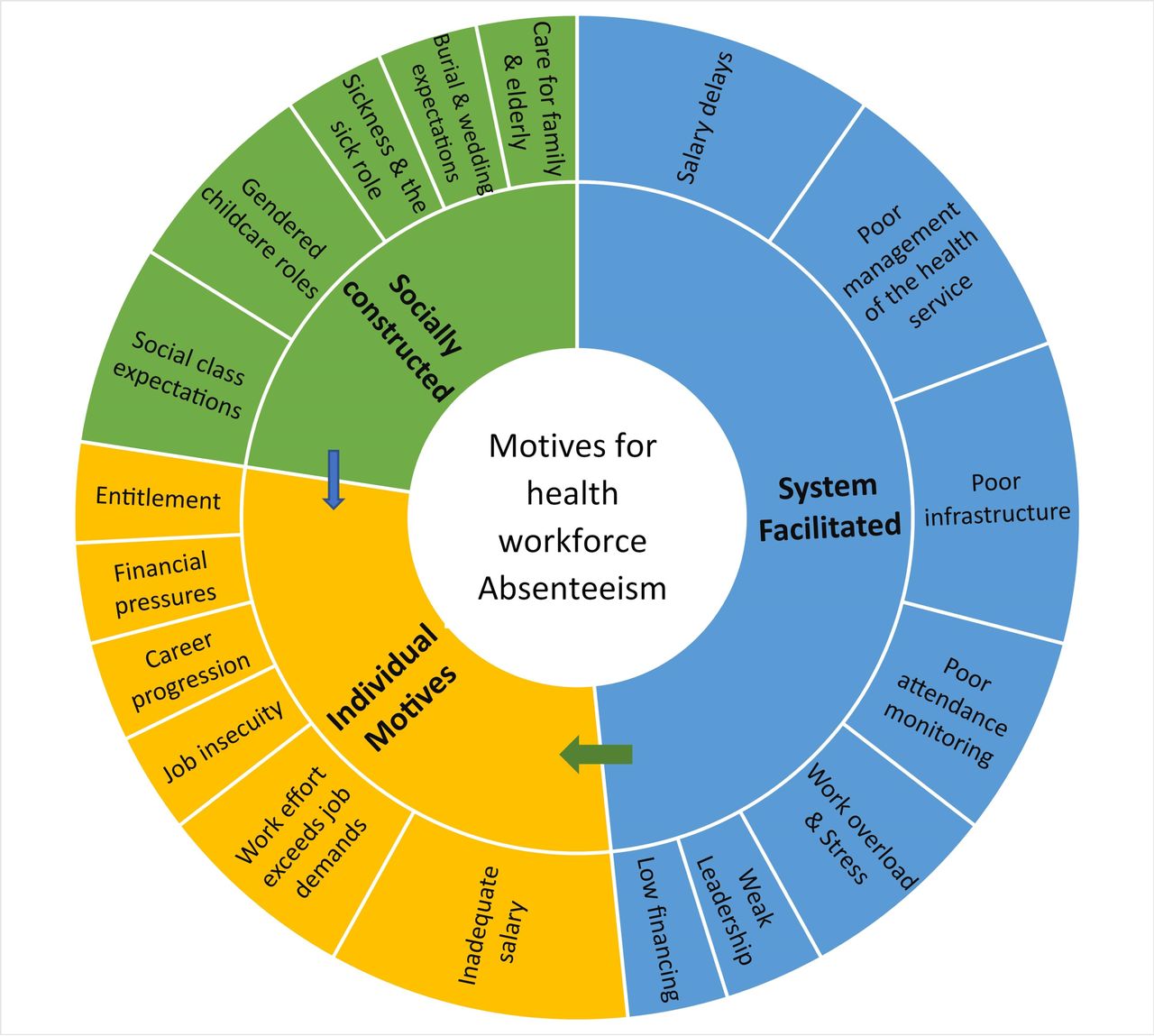
Broadly, two categories of reasons for absenteeism emerged. These included external influences such as health system-facilitated contributors and social-cultural discourses, and internal influences which we consider ‘individually motivated’. Figure 2 summarises all themes found in this study on reasons for health workforce absenteeism in rural Uganda.
{kind=link}
{kind=link}
Reasons for health workforce absenteeism.
External influences
System-facilitated absenteeism
The strongest justifications reported for absenteeism were delays, deductions and sometimes the total omission of workers’ salaries. This challenge was experienced mainly in the public sector, affecting mostly new recruits, but several public sector workers’ salaries were unpredictably affected. Moreover, the public service had a financial policy that dictated that workers lost their salary arrears if they were unpaid beyond the fiscal year, knowledge and experience of which generated frustration and resolve for prolonged absenteeism.
We register a lot of absenteeism, most especially at the beginning of service [start of employment], for everyone, because there is always a delay in payment. They keep on telling us that joining the payroll takes a lot of time, [it] could even take up to a year without being paid, and the arrears, sometimes, they don’t even give them. (P7: public HC IV, non-physician clinician)
…when staff had not yet been paid salary, it was very difficult. Every staff was using that as a complaint, and it was general, should I say countrywide, because even in other districts, that was the main complaint. (P16: public HC IV, laboratory worker)
The biggest cause of absenteeism in [health facility named] is the issue of salary delays. If the salaries are not there, then some workers don’t come for duty. (P20: private HC IV non-physician clinician)
Most participants in supervisory positions reported the low prioritisation of, and financial allocation to, decentralised healthcare services. Specifically, they described inadequate funding for the maintenance of staff accommodation and health unit infrastructure. Also, funding was reportedly inadequate for the provision of amenities such as water, electricity and back-up fuel for electricity, maintenance and running costs for ambulances, compound cleaning, and for supervision visits to lower level health facilities.
This health facility is provided [US$450] each quarter. So, in a month, you have available [US$150] from which you pay cleaners, slash [mow the compound], buy fuel for the generator, buy tyres and service the ambulance, conduct supervisions to all lower level health facilities in the sub-district and attend district meetings. (P18: public HC IV, physician in-charge)
We don’t have electricity, we use a generator. We book patients [for surgery], but the fuel is not enough. We put in [the generator] 20 litres, and we get it [fuel] in [every] three months. But because we pile [overbook] the patients, they are many, so we can use the generator for 6 hours per day for [only] four times in a month and it [the fuel] runs out. (P13: public HC IV, nurse)
Government is failing to put up accommodation structures for their staff, or for most of the staff here. You find one room is being shared by two staff, and the rooms are leaking when it rains. (P16: public HC IV, laboratory worker)
The rooms are too small to accommodate a family, and so you have to get them [family members] where to stay. So, with this, you find yourself absent sometimes, because you have to try balancing family life with work. (P34: public hospital, laboratory worker)
Frequent stock-out of supplies, including medicines listed as ‘essential’, connoting basic medicines for treating common health conditions, was reported in all public health facilities. Likewise, insufficient stocks of laboratory reagents, disinfectants, protective gear such as gloves, and other sundries were common in the public sector. The inefficiency of the local and central health system in procurement of supplies and the low financing to health facilities for operational expenditure tended to demoralise healthcare workers, thus incentivising absenteeism. HC IVs (providing both primary and secondary care) experienced acute funding inadequacies causing higher workforce absenteeism and resulting in the operation of the facilities as outpatient practices. This situation was enabled by weak supervisory structures and low accountability of the health workforce to the health unit and district leadership. Interestingly, participant accounts strongly indicated that the district and health facility leadership were aware of the prevailing absenteeism but refrained from sanctioning it because they acknowledged shared blame for the situation.
That you report somebody who misses work! In reality, it is not there in our profession. The one you are reporting may not even be the worst person in the profession. You see, money for Malaria and other programmes [at central Ministry of Health] was eaten [embezzled]. Now this one has gone to do ‘kyeyo’ [seek supplemental income], and you report? (P14: public HC IV, nurse supervisor)
The health facility in-charges themselves are absconders [frequent absentees]. (P7: public HC IV, non-physician clinician)
Nobody is after you; it is your initiative to start work. Whether you start on time or not, no one is after you, so, you take your time if you want. [Possibly] Because management is not at station [are absent] and people [workers] come from far. (P13: public HC IV, nurse)
Actually, what is making public [health] units exist [function] is because of accepting absenteeism to be there. Otherwise, most people would not apply to be in those units. (P24: PNFP HC IV, physician in-charge)
In contrast, absenteeism was highly sanctioned in the PNFP sector, constituting grounds for dismissal. Also, the presence of several on-site supervisors working within clinical and non-clinical teams made it difficult for many to engage in absenteeism. Although except for extreme salary inefficiencies the working conditions in the PNFP sector were comparable with those in the public, continuous monitoring and supervision of the health workforce in the former proved effective for minimising absenteeism.
…there is no job security here in [health facility named] in regard to being absent. (P20: PNFP HCIV, non-physician clinician)
If you are allocated duty, you are supposed to be there, unless there is something very crucial that you need to attend to. Most of the times, we are supposed to write down on a paper [seek written permission from a colleague] in case an administrator asks about you. So, the level of supervision is very high, because you can hardly see the opportunities to sneak out of the hospital to do something out. (P37: PNFP hospital, laboratory worker)
However, several PNFP sector participants reported taking absence when feeling fatigued or stressed without seeking permission or communicating to colleagues. As a result, colleagues left on duty took similar absence because they too became overworked as a result of covering colleague’s duties. Further, there was not any absentee replacement policy to refer to. Relatedly, the most common reason reported by private sector healthcare workers for their absence was sickness, although many clarified that it was mostly false claims of sickness. Also, the flow of clients in the PNFP sector was high in relation to low staffing as compared with the existing public sector staffing and client flow.
You reach a time when you feel you are fed-up. Nobody appreciates your work; you are disturbing your heart. And in turn, you ask yourself why you are working so hard. Sometimes you lose morale because there is nothing that motivates you, then you say to yourself ‘I got so tired yesterday; let me wake up at 8am’. (P19: PNFPHC IV, non-physician clinician supervisor)
Socially constructed absenteeism
Sickness and caring roles
Many participant nurses were of childbearing age, with an interquartile age range of 20–29 years. It became apparent from the interviews that they were responsible for both elderly and child caring roles.
Both public and PNFP sector participants clearly expressed that their sickness or that of their child or other close relative was a legitimate reason for taking absence with or without seeking permission. This invariably stemmed from the normative organisational expectation that sick individuals should not attend work, and also from the gendered societal prescription of sick caring roles to women, who formed the vast majority of the health workforce at the study sites.
…whenever you inform the in-charge [health facility manager] about your sickness, she makes prior arrangements to have someone to cover you. (P33: public HC IV, midwife)
Take an example of these young ladies [nurses], how do they balance pressure at work and their personal lives! Though they get offs [scheduled off-days], their partners are staying very far, because they don’t have accommodation here. So, if you go to see your partner, you spend some little more days than you would have. (P30: public HC IV, nurse)
Communal ceremony norms
A majority of the participants reported that attendance at weddings and burials was socially mandatory, particularly for the immediate family, extended family and friends. While weddings could be planned and leave days were requested in advance, the same was impractical for burials, which often occurred within 3 days of losing someone.
Most of the times, people at home complain that I don’t attend burials, and I have to find a way of attending without informing my supervisors, so that my image [in the family] does not to get tarnished’. (P21: PNFP HC IV, nurse supervisor)
As with sickness, several healthcare workers clarified that they often requested attendance at burials or weddings as excuses to ease obtaining official leave, although permission seeking occurred mostly in the private sector.
Societal pressure
About a quarter of participants reported that society judged healthcare workers unrealistically as belonging to high social classes, affording both satisfaction of daily needs and luxuries for themselves and their immediate family. This therefore exerted pressure on them to portray the profession as satisfying and deserving of the accorded esteem. As a result, several healthcare workers reported taking their children to more popular schools, and where possible living in decent accommodation. Consequently, they were pressured to seek supplemental income to their primary jobs, which was achieved through engagement in dual practice and resulting in absenteeism.
If you say that you are a doctor, or a health worker, and you send your child to an awkward school, they will say: ‘that person’ [mockery], and yet your pay is [low]. They expect your son to be in ‘Kisubi’, in ‘Gayaza’, in ‘King’s College Buddo’ [top schools], but how much are you earning! (P24: PNFPHC IV, physician in-charge).
Internal influences
Individual reasons and motives
All study participants decried the inadequacy of salaries in relation to their employment expectations and the rising standards of living.
We are paid ‘cartoon’ [very low/uncompetitive] salary…we are in a remote set-up and it is not like an urban setting where people work for [a few] hours and go elsewhere [to perform another job]. Searching for another job is hard in the rural set-up. (P37: PNFP hospital, laboratory worker)
The public and private sector employers were viewed as unwilling to offer higher salaries. Therefore, in response to perceived financial pressures, many participants in clinical roles (physicians, non-physician clinicians, nurses and midwives) had strong resolve for, or were already engaged in, a form of dual practice, ‘holding two or more concurrent jobs’. The majority of those involved in dual practice ran their own clinics, drug shops, maternity care homes or were employed in another facility within the health sector. However, a few were engaged in other industries, notably farming, retail shops and hawking.
I can say that at least 50% of staff have their private units. And if they don’t have private units, three-quarters have units, which they are supervising…and then the other remaining a quarter has at least somewhere where they do private work. (P7: public HC IV, non-physician clinician)
Additionally, official opportunities for attending training seminars, workshops and outreach activities such as community camps for safe medical circumcision supported by non-governmental organisations were highly coveted, since they were regarded as supplemental income sources.
…we have an understanding or put in some lenience since it is something which can boost somebody’s salary. If somebody gets a ‘kyeyo’ [side job], we really have to be flexible and allow that somebody to go away. (P10: public hospital, non-physician clinician)
In reaction to perceived inadequacy of salary and financial pressures, several public sector participants felt that the health system inadequately valued their skill-set and perceived their effort as exceeding the job rewards. Consequently, they felt entitled to absenteeism as a means of countering the limited rewards.
There is need to intellectualise. You need to calculate how much government pays you, then you pay them back their time’s worth. One or two days a week is more than adequate. (P8: public HC IV, physician supervisor)
People now have the mentality that government [employment] is a holiday, hmm [yes]. They come [take government employment] to take a break. (P8: public HC IV, physician supervisor)
Since we are being cheated [by government], like our salaries, there is no way of cheating government apart from using time. (P5: public hospital, non-physician clinician)
Perceived job insecurity
Several non-physician clinicians and healthcare workers such as nursing and laboratory assistants viewed their jobs as insecure, and thus had urgency for career advancement. About one-third of public sector participants and a fifth of PNFP participants were pursuing self-sponsored studies concurrent with their jobs. Moreover, studies were pursued in the absence of prerequisite permissions in order to avoid contractual salary deductions in the public sector and risking dismissal in the PNFP sector.
…most health workers in the maternity [labour ward] are now in school, because government is scrapping off nursing assistants. So, in order to safeguard their positions, they have to go back to school, and yet they are not replaced at the health facility. In the end, what you observe is absenteeism. (P34: public HC IV, laboratory worker)
Discussion
This study aimed to explore the underlying reasons and motives for healthcare workers’ engagement in absenteeism, involving front-line and supervisory workers in the public and PNFP sector of rural Uganda. This aim was against the dearth of published knowledge on reasons for health workforce absenteeism in low-income and middle-income countries. Findings suggest the existence of complex interrelated influences operating within—and external to—an individual healthcare worker, often stemming from the health system, but also related to social-cultural discourses and individual motives. As depicted in figure 2, evidence from this study suggests a strong influence of system and societal factors on individual motives for absenteeism. An individual lens on absenteeism, as posited in the withdrawal,35 56 ‘stress or sickness’9 31 57 and ‘rational’ economic models,58 59 appears insufficient to explain absenteeism in resource-poor settings like Uganda. Salary inadequacy was universal among participants, with perceived entitlement to take absence more often expressed in the public sector by clinicians and managers, unlike the nurses and laboratory personnel who generally regarded absenteeism as immoral and unethical. This finding suggests potentially unchecked abuses of power, which might be fuelled by prevailing healthcare labour market forces where clinician skills are in high demand. As described in similar resource-poor settings, physicians were in more severe shortage relative to the nursing workforce.79 80 Also, high clinician absenteeism relative to non-clinicians is reported in other low-income and middle-income countries such as Argentina, Bangladesh, Indonesia, Laos PDR and Tanzania.1 18 19 23 81 Evidence from studies on international migration suggests that clinician skills are in high demand in urban locations82 and in high-income countries.83 84
Unlike the PNFP sector, health system-facilitated absenteeism was more prevalent in the public sector, where more favourable norms accepting of worker absenteeism existed, signifying weak health workforce governance. Relatedly, individual motives for absenteeism derived their legitimacy from health system inefficiencies such as salary delays, and medicines and supplies running out, which were most apparent in the public sector. Other studies in low and middle income countries (LMIC) settings have reported healthcare workers’ complaints of low salaries,85 86 unfairness of the employer,16 22 lack of accommodation87 88 and engagement in dual practice,13 14 although these are often reported in isolation or in relation to health system outcomes other than absenteeism. The present study adds to this evidence that such perceptions of inadequate working conditions are likely precursors of absenteeism.
Perceived financial pressures that engendered seeking supplemental income and/or career progression existed in both the public and PNFP sectors, highlighting the existence of wider environmental contributors to health workforce absenteeism. Apart from gendered child care roles,19 85 and attendance at burials and weddings,21 other social-cultural pressures such as social class expectations and sick caring roles are limited in the absenteeism literature of the health workforce in low-income and middle-income countries. This highlights a need for increased prominence of social-cultural and anthropological evaluations of health workforce absenteeism in these settings. Intuitively, policy makers and health managers of health systems where the workforce is predominantly female, as in Uganda, need to explore and potentially institute proven workplace adjustments that are responsive to work–family needs such as providing kindergarten and child care services64 65 89 for reducing gendered-role absenteeism.
Although healthcare workers’ absenteeism was mostly reported in relation to system influences, it does not fit the ‘withdrawal’ model, which suggests that workers take absence for escaping hostile work environments.35 56 Nor did the predominant absenteeism fit the ‘sickness’ or ‘work-stress’ models, both of which envisage that absenteeism results when work demands exceed resources available to workers.9 56 75 90 Rather, healthcare workers negotiated their absence to guarantee their daily livelihood through dual practice, while striving to accomplish agreed work routines, in order to portray their health facilities as functional. In this regard, we argue that it was the healthcare workers’ plight to ensure performance of their ‘sub-optimal’ negotiated task load, while struggling personally for financial sustenance. Therefore, we propose the term ‘negotiated absence’ as the most appropriate descriptor for the form of public health sector absenteeism in this study’s setting.
The existence of ‘negotiated absence’ stemming majorly from system inefficiencies and societal discourses generates both policy and research implications. First, public health policy needs to improve workforce governance,24 65 79 and indeed consider that maintaining the workforce accounts for more than half of the sector’s expenditure,91 which could potentially improve the system’s effectiveness. Evidence from this study suggests that there is an opportunity for the PNFP and public sector to benchmark provision and learn about workforce governance methods.92 93 Second, it is imperative that averting wider health system challenges could reduce health workforce absenteeism, for example through increasing financial allocation to decentralised services,94 maintenance of infrastructure and avoiding stock-outs of supplies and medicines.88 Third, greater involvement of the health workforce in decision-making for healthcare delivery could improve the prioritising of better working conditions and increase accountability for work attendance.31 33
From a research perspective, the dominant PETS studies appear of limited value in low-income countries for assessing the magnitude of, and eliciting reasons for, healthcare workers’ absenteeism. This is in part because of the complex nature of the organisation of a healthcare worker’s schedule, involving off-site working and multiple unstructured on-site tasks.18 19 Measurement is further complicated by scenarios such as the shared concealment of reasons for a colleague’s absence, perhaps to avoid sanctions being made against the staff as a whole. There is need for time-based computational approaches, which are independent of paper-based systems, to account for worker availability and work productivity. Further research to improve the measurement and understanding of absenteeism in resource-limited settings is therefore warranted.
Study limitations
This study did not use ethnographic approaches such as participant observation to validate interview findings. In some interviews, participants changed their narratives possibly to provide ‘front-stage views’, a form of impression management.95 However, the use of credibility check group interviews96 97 attempted to address this gap.
Although 95 interviews for attaining data saturation are a large sample in qualitative research, our experience showed the necessity for exploring a delicate topic questioning sanctionable behaviour such as absenteeism. Participants were generally mindful about the possible ramifications of the interviews, and it took continuous rapport-building and revisiting the consent tenets to maintain participants’ trust. Additionally, a rich data account from a stratified sample to gain maximum variability including the public, PNFP, hospital, health centres, supervisors and supervisees demanded data saturation within each sample strata.
Conclusion
This study found evidence for motivational (planned) absence, only in situations where reasons for absenteeism were individually motivated. Thus the theory of planned behaviour76 and the economic rational choice models,77 78 which explain motivational behaviour change, were limited in explaining the more prevalent system and socially constructed contributors to workforce absenteeism. Similarly, work-related stress90 and sickness absence models9 were of limited explanatory relevance in this study’s setting. There is need for ethnographic approaches and comparative case studies in similar resource-poor settings to enhance generalisability of findings. Further exploratory theoretical evaluation of ‘negotiated absence’ is necessary to increase the understanding of health sector absenteeism.
Finally, although this study covered only five health facilities in three rural districts of a single region in Uganda, the thematic findings are not novel as they generally resonate with the situation in several low-income countries. The contribution of this study lies in providing a more detailed, contextualised and nuanced account of the precursors to absenteeism related to common health system inefficiencies, which appear highly prevalent in low-income countries.
Acknowledgments
The authors would like to thank all the research participants who provided time and shared their experiences. The authors would also like to thank Erimiah Kyanjo, our research assistant, and The University of Manchester Doctoral Academy, and the Centre for Primary Care, Makerere University School of Public Health and its PhD forum for providing a scholarly learning environment. Finally, we acknowledge the comments of two anonymous reviewers, which contributed to improving this article.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
Footnotes
Handling editor Stephanie M Topp
Twitter Raymond Tweheyo @RTweheyo.
Contributors RT conceptualised the study, carried out data collection and analysis, and was responsible for the write-up and drafts of the manuscript. CR, LD, GD-W, SK and SC refined the study concept, protocol and data collection methods, and read all versions of this manuscript. CR, GD-W and SC additionally took part in the analysis.
Funding This study is part of a PhD project funded by The University of Manchester President’s Doctoral Scholar Award. Additional research funding was obtained from the African Population and Health Research Council, APHRC (African Dissertation Doctoral Fellowship), as well as a research bursary from the Department of Health Policy Planning and Management of Makerere University School of Public Health, Uganda.
Competing interests None declared.
Patient consent Research consent forms were signed by participants. This was not an intervention, and it did not involve patients.
Ethics approval Ethics approvals were obtained from The University of Manchester Review Committee (Ref: Ethics/13212), Makerere University School of Public Health Higher Degrees and Ethics Review Committee (Ref: HDREC13/06/2014), and the Uganda National Council for Science and Technology (Ref: SS3522). Further permissions were sought from District Health Officers, and Medical Superintendents at hospitals. All participants provided written informed consent.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.