Article Text

Abstract
Kidney biopsies to elucidate the cause of chronic kidney disease (CKD) are performed in a minority of persons with CKD living in high-income countries, since associated conditions—that is, diabetes mellitus, vascular disease or obesity with pre-diabetes, prehypertension or dyslipidaemia—can inform management targeted at slowing CKD progression in a majority. However, attributes of CKD may differ substantially among persons living in low-income and middle-income countries (LMICs). We used data from population or community-based studies from five LMICs (China, urban India, Moldova, Nepal and Nigeria) to determine what proportion of persons with CKD living in diverse regions fit one of the three major clinical profiles, with data from the US National Health Nutrition and Examination Survey as reference. In the USA, urban India and Moldova, 79.0%–83.9%; in China and Nepal, 62.4%–66.7% and in Nigeria, 51.6% persons with CKD fit one of three established risk profiles. Diabetes was most common in urban India and vascular disease in Moldova (50.7% and 33.2% of persons with CKD in urban India and Moldova, respectively). In Nigeria, 17.8% of persons with CKD without established risk factors had albuminuria ≥300 mg/g, the highest proportion in any country. While the majority of persons with CKD in LMICs fit into one of three established risk profiles, the proportion of persons who have CKD without established risk factors is higher than in the USA. These findings can inform tailored CKD detection and management systems and highlight the importance of studying potential causes and outcomes of CKD without established risk factors in LMICs.
- epidemiology
- indices of health and disease and standardisation of rates
- cross-sectional survey
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com
Key questions
What is already known about this topic?
A growing number of studies have evaluated the prevalence of chronic kidney disease (CKD) in low-income and middle-income countries; thus, we can estimate how many persons have CKD in many low-income and middle-income countries.
We can say less about who has CKD: no comparisons have been performed to determine whether attributes of persons with CKD living in low-income and middle-income countries differ from those persons with CKD living in high-income countries.
Nephrologists perform kidney biopsies to elucidate cause in a minority of persons with CKD. Associated conditions—primarily, diabetes mellitus, vascular disease or obesity with pre-diabetes, prehypertension or dyslipidaemia—can offer a sufficient explanation to inform management targeted at slowing CKD progression.
What are the new findings?
We find that a majority of persons with CKD, about two-thirds, living in five low-income and middle-income countries fit one of the three predefined risk factor profiles.
The relative proportion of each differs substantially, with diabetes most common in urban India, vascular disease most common in Moldova and obesity with prehypertension, pre-diabetes or dyslipidaemia most common in China.
In contrast to the USA, where nearly 85% of persons with CKD have one of the three associated conditions, more people are in the ‘CKD without established risk factors’ category, especially in Nigeria, where the high proportion of persons with significant albuminuria suggested the important contribution of apolipoprotein-1 nephropathy.
Recommendations for policy
This approach of describing attributes of persons with CKD can help to tailor screening, detection and management strategies within each country.
Our approach also highlights the need to study correlates and outcomes of persons with CKD without established risk factors in low-income and middle-income countries; it is possible that these persons have novel risk factors for CKD, or alternatively, we need to apply different thresholds to define CKD in diverse populations.
Introduction
A growing number of studies in countries around the world indicate that roughly 10% of adults have evidence of chronic kidney disease (CKD),1 2 a finding that holds true across regions and income categories. While we know more about how many persons have CKD, we know less about who develops CKD in low-income and middle-income countries (LMICs) and whether the attributes of persons who develop CKD in LMICs differ substantially from those in high-income countries (HICs). In the USA3 and other HICs,4 5 associated diabetes mellitus, vascular disease and/or obesity are present in a majority of persons with CKD.
Many experts speculate that attributes of persons with CKD do differ substantially in LMIC, which experience a higher burden of infectious disease, urinary stone disease, low birthweight and, in some regions, primary glomerular disease.6 7 In several regions, a form of tubulointerstitial nephritis deemed CKD of unknown aetiology has been increasingly recognised, although its cause or causes have remained elusive.8 Determining what proportion of persons with evidence of CKD living in LMIC fit profiles similar to those of persons with CKD in HIC could be the first step towards understanding whether CKD screening strategies in LMIC need to target different populations and whether preventive efforts should be directed to different types of risk factors than in HIC.
Unlike HICs where population-based studies are often performed on an ongoing basis, surveillance systems to evaluate trends in, and/or attributes of, chronic diseases are weak in LMICs. We found existing data on characteristics of persons with CKD from population-based studies in five low, lower-middle and upper-middle income countries: China, India, Moldova, Nepal and Nigeria. Across this range of settings and in comparison with data from the USA, we describe the proportion of persons with CKD fitting one of three profiles—diabetes mellitus, vascular disease and obesity with pre-diabetes, prehypertension or dyslipidaemia—and the characteristics of persons who do not share any of these attributes.
Methods
We used data from six population-based studies, three of which (from Nepal, Nigeria and Moldova) were conducted with support from the International Society of Nephrology (ISN) and using a standard data collection template (ISN Kidney Disease Data Center (KDDC)).9 Data from urban India (Center for Cardiometabolic Risk Reduction in South Asia (CARRS) surveillance study)10 11 and China12 are drawn from surveys with representative sampling techniques; the publicly available US National Health and Nutrition Examination Survey (NHANES)13 1999–2006 cohorts provides the comparator data set (table 1). In generating our analytic sample, we excluded individuals who were younger than 20 years and with missing data on urine or serum markers of CKD. All studies obtained institutional review board approval at their coordinating institutions and adhered to principles outlined in the Declaration of Helsinki.
Design and sample size of studies included in analysis
Definition of CKD
With the 2012 Kidney Disease Improving Global Outcomes guidelines14 as a reference, we defined a participant as having CKD with albuminuria (albumin:creatinine ratio (ACR) ≥30 mg/g creatinine and/or Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI)15 estimated glomerular filtration rate (eGFR) <60 mL/min/1.73 m2). We used the race-adjusted coefficients for eGFR calculation for the Nigeria data. When incorporating data from the ISN KDDC, we assessed albuminuria as an approximate equivalent of ACR using an algorithm that relies on ACR, protein:creatinine ratio and protein dipstick, strictly in this order.9 16 We categorised persons having albuminuria if ACR ≥30 mg/mmol creatinine, protein:creatinine ratio ≥150 mg/g or protein dipstick 1+ or above. Protein dipstick was most often used in Nepal (online supplementary table 1).
Supplementary file 1
Definition of profiles
On the basis of published data from the US Renal Data System3 on clinical attributes of persons with CKD in the USA, we created four profiles:
Diabetes: fasting glucose ≥7.0 mmol/L or glycosylated haemoglobin (A1c≥6.5%) or self-reported diabetes.17
Vascular disease: self-reported history of coronary artery disease, myocardial infarction, congestive heart failure, stroke or current or former regular smoking.
Obesity with an additional cardiovascular risk factor: we categorised a person as obese if he or she had abnormal waist circumference as defined by sex-specific and ethnicity-specific cut-offs.18 In addition, to fit in this profile, he or she had either fasting glucose (5.6–6.9 mmol/L), haemoglobin A1c (5.7%–6.4%), measured systolic blood pressure ≥130 mm Hg and diastolic ≥85 mm Hg, triglycerides ≥1.7 mmol/L or low high-density lipoprotein <1.0 mg/dL for men or <1.3 mg/dL for women.18
CKD without established risk factors: persons without any risk factors as outlined in profiles 1–3.
Online supplementary table 2 lists available data and associated measurement methods for profiles across studies; online supplementary table 3 lists acceptable ranges for laboratory tests used when defining profiles.
Statistical analyses
For all harmonised data elements among the six cohorts (online supplementary table 3), we report means (±SD) and proportions as appropriate. For the three representative studies (from China, urban India and the USA), we report N, means and proportions. After categorising persons into mutually exclusive profiles in sequence from profiles 1 to 3, we report the relative proportion of persons with CKD in one of the four profiles. Since haemoglobin A1c was available in only two studies, we performed sensitivity analyses using fasting glucose thresholds alone in these studies.
In considering missing data, all non-affirmative responses were treated as absent condition for comorbidities dependent on self-report.19 For measured markers (eg, fasting glucose or waist circumference), the missingness was low among persons with CKD (<10%, see online supplementary table 4) and was considered in the following way: in calculating the proportion with diabetes (profile 1), for example, if a participant was missing haemoglobin A1c or missing fasting glucose and did not self-report diabetes, he/she was labelled as having a ‘missing’ diabetes status. However, if a participant had an abnormal value for either fasting glucose or haemoglobin A1c, he/she was treated as having diabetes. We evaluated and report any differences in missingness of data elements required to categorise a participant with CKD in profiles 1–3 across the studies. All statistics for NHANES, CARRS and China studies take into account complex survey design including subpopulation methods when appropriate. We used SAS V.9.4 (Cary, North Carolina).
Results
Table 1 briefly describes methods of each study included in this analysis. Table 2A describes participants with available information on CKD markers (urine albumin and serum creatinine data) in the studies with representative sampling design. Mean age was higher in the USA, as were self-reported rates of smoking and cardiovascular disease. More people in China and urban India had blood pressure measured in the highest categories (≥140 mm Hg systolic or ≥90 mm Hg), although prevalence of hypertension was similar to the USA. Diabetes prevalence and proportion of people in the highest fasting glucose categories was highest in urban India. Unadjusted CKD prevalence ranged from 8.09% to 15.15%.
Characteristics of persons living in USA, China and urban India, as captured by studies performed using a representative sample
Characteristics of participants in population-based International Society of Nephrology Kidney Disease Data Center studies in Moldova, Nepal and Nigeria
Table 2B describes participants in the community-based ISN KDDC screening studies. Women were more likely to participate; in Moldova, participants were older and more likely to report cardiovascular disease and have hypertension or diabetes. Participants in Nepal reported the highest rates of smoking. At 20.9%–25.4%, unadjusted CKD prevalence was higher in the ISN studies than in the population-representative design studies.
Online supplementary table 4 reports these characteristics for persons categorised as having CKD. In the USA, urban India, China and Moldova, albuminuria alone was the most common form of CKD, whereas in Nepal and Nigeria, eGFR <60 mL/min/1.73 m2 (with and without albuminuria) was most common. Significant albuminuria (≥ 300 mg/g) was most common in Nigeria.
Profiles of CKD
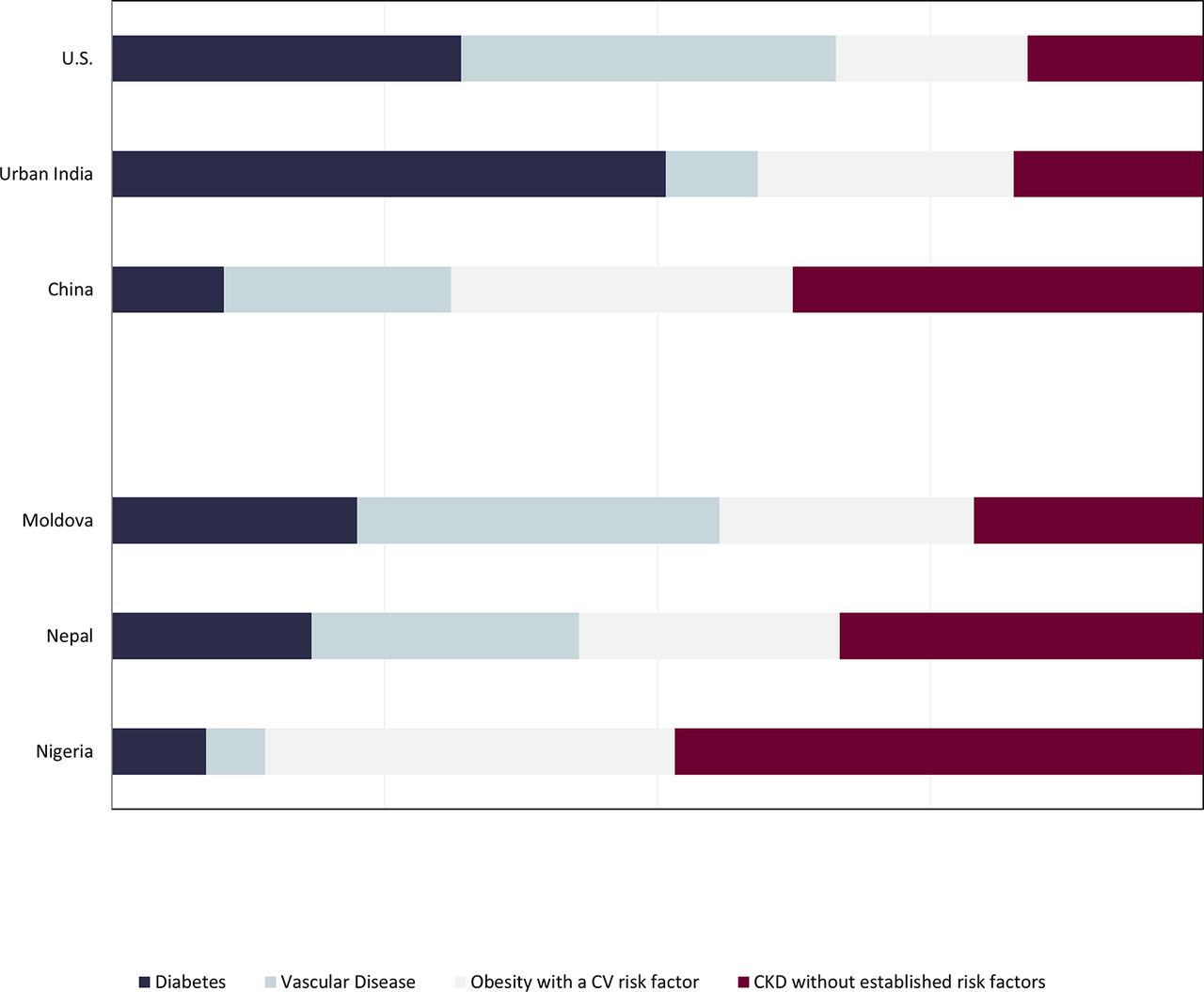
Figure 1 depicts the relative prevalence of the four profiles and the overall proportion of persons with CKD in each country fitting these profiles. In the USA, many persons with CKD did fit one of the three profiles with accompanying established risk factors, with only 16.1% (95% CI 13.0% to 19.2%) lacking one of these risk factors. We found similar results in urban India (17.4%, 95% CI 13.4% to 21.4% in profile 4); diabetes mellitus was most common (50.7%, 95% CI 44.9% to 56.6%). Compared with other countries, more Chinese persons with CKD did not have one of the associated established risk factors (37.6%, 95% CI 35.2% to 40.1%), but more than 60% did fit into one of the three profiles, with vascular disease (20.8%, 95% CI 18.7% to 22.9%) more common than in India and obesity with a cardiovascular risk factor most common of the three predefined risk profiles (31.3%, 95% CI 29.0% to 33.6%).
In the KDDC studies, a high proportion of persons with CKD from Moldova could be categorised into one of the three profiles, with vascular disease most common in Moldova (33.2%, 95% CI 27.8% to 38.9%) and prevalence of CKD without established risk factors (21.0%, 95% CI 15.6% to 26.7%) similar to that of USA and urban India. In Nepal, vascular disease (24.5%, 95% CI 22.9% to 26.1%) or obesity with a metabolic risk factor (23.9%, 95% CI 22.3% to 25.5%) was similarly common, and a higher proportion of persons (33.3%, 95% CI 31.7% to 34.7%) had CKD without established risk factors. Nearly half of the participants (48.4%, 95% CI 43.7% to 53.5%) in Nigeria did not have accompanying risk factors.

Profiles of persons with CKD. In all countries except Nigeria, a majority of persons (>60%) fit one of the three predefined risk profiles. Diabetes and CKD were most common in urban India; vascular disease and CKD were most common in Moldova; obesity with prehypertension, pre-diabetes or dyslipidaemia was most common in China. CKD, chronic kidney disease; CV, cardiovascular.
Characteristics of persons without established risk factors (profile 4)
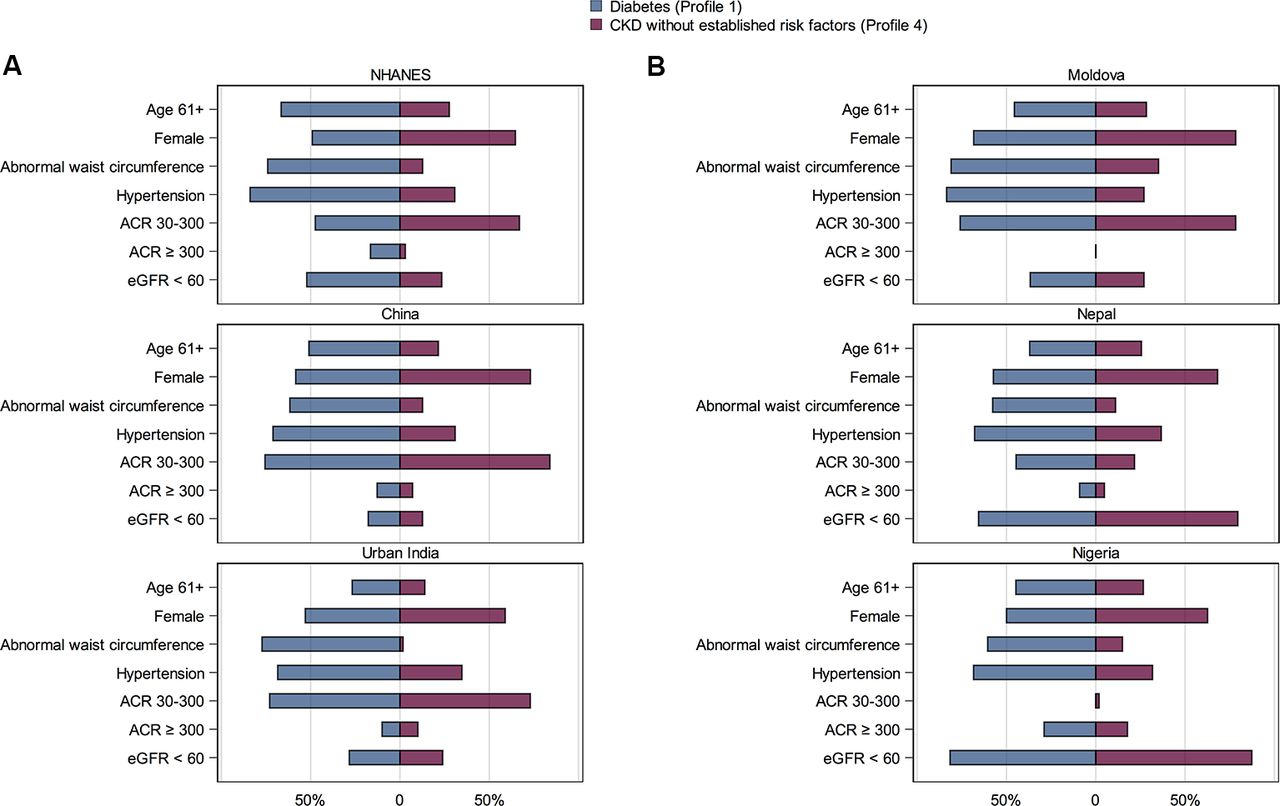
In-depth exploration of harmonised data on persons falling in profile 4 (figure 2A,B) showed that, in contrast to persons with diabetes and associated CKD (profile 1), a majority were less than 61 years in age, with normal waist circumference and without a diagnosis of hypertension. About one-third of persons in profile 4 had hypertension (range of prevalence 27.0% (Moldova) to 35.9% (China)). The distribution of CKD, that is, the proportion of persons with ACRs 30–300 mg/g or with eGFR <60 mL/min/1.73 m2, did not seem to vary by profiles within country; significant albuminuria was most common in Nigeria for both profiles 1 and 4.
Supplemental analyses relying solely on fasting glucose thresholds did not demonstrate any significant differences in proportions of persons in profile 4 in NHANES and urban CARRS (online supplementary table 5).
Notably, 10.4% of NHANES participants in profile 4 had missing data for other profiles, a proportion comparable with or higher than other studies (1.1%–11.4%) with the exception of the ISN KDDC study in Moldova. Missingness of waist circumference data was high in this study; thus 27% of persons in profile 4 had missing data for other profiles.

{kind=link}
{kind=link}
Characteristics of persons with CKD without established risk factors versus those with CKD and diabetes. (A) Among participants of population-based studies. (B) Among participants of International Society of Nephrology Kidney Disease Data Center studies. Persons without established CKD risk factors were younger and more likely female; about one-third had hypertension. Within each country, the distribution of albuminuria and eGFR <60 mL/min/1.73 m2 did not differ substantially between the two profiles. ACR, albumin:creatinine ratio; CKD, chronic kidney disease; eGFR, estimated glomerular filtration; NHANES, National Health and Nutrition Examination Survey.
Discussion
Spanning several regions of the world, our study of persons with CKD demonstrates that a majority have accompanying diabetes mellitus, vascular disease or obesity with a cardiovascular risk factor. While this association does not imply causation, management of the disorders defining these profiles can substantially mitigate risk for end-stage renal disease (ESRD) and cardiovascular events in persons with CKD.20–22 Our analysis thus confirms that public health policies in urban India, China, Nepal or Moldova to reduce smoking or improve diet and physical activity or primary care guidelines to optimise glycaemic control are likely to significantly attenuate the downstream burden of CKD. At the same time, the proportion of persons with CKD who do not have established risk factors is larger in LMICs in comparison with the USA, implying that, in order to detect a larger range of CKD, LMICs will need to identify region-specific risk factors (eg, haematuria for regions with high expected rates of IgA nephropathy23 or herbal use in regions with medicinal aristolochic acid24).
Evidence regarding the prevalence of CKD in LMICs has been growing,1 2 but few studies have been performed using a representative sampling technique or with measures of potential attributes. Even in the studies we were able to collate, participants likely under-reported or were underdiagnosed for some profiles. Fewer than 1% of participants in the Nigeria study self-reported cardiovascular disease, for example, and fewer than 7% reported smoking. Yet even if we were to double the proportion of persons with CKD and associated vascular disease (profile 2) in the Nigeria study, nearly 40% would remain in the category of CKD without established risk factors. The high rates of moderate or high albuminuria in this group hint at the influence of apolipoprotein-1 nephropathy,25 which may explain why, while the prevalence of diabetes mellitus or vascular disease was relatively low in Nigeria, the prevalence of CKD has been reported to be similar to other LMICs.26 The higher proportion of persons with CKD without established risk factors in China and Nepal also deserves further study. In both countries, moderate or high levels of albuminuria were not striking or disproportionate features of ‘profile 4.’ Several non-allopathic Chinese medications used to treat liver, urinary and cardiovascular disease contain aristolochic acid, a known nephrotoxin that causes non-proteinuric CKD.27 Infectious aetiologies such as HIV could either directly or indirectly, through complications of treatment, contribute to CKD in persons without other established risk factors.28 Unusual CKD cases or causes have been reported elsewhere as well,29 30 and a broad brush approach as applied here and suggested by others8 has the potential to identify novel risk factors for CKD.
Our approach also highlights the need for studies investigating thresholds for diagnosis of CKD in LMICs. For example, albuminuria is a predominant manifestation of CKD in the two most populous regions in the world (urban India and China), but experts have proposed considering an alternate ACR threshold to define albuminuria in some regions, particularly due to the lower expected creatinine excretion in persons with lower muscle mass or less meat intake—which could falsely increase the ratio. Jafar et al 31 showed that the urine albumin-to-creatinine cut-off of ≥30 mg/g had reasonable high correlation with 24-hour urine excretion in the Indo-Asian population. Further studies evaluating persistence of albuminuria and its association with cardiovascular and renal outcomes are crucial to determine how albuminuria relates to cardiovascular and kidney endpoints in LMICs and if region-specific or other varying definitions of albuminuria need to be applied. A similar argument applies to eGFR, for a multitude of reasons but one prominent example: given the lower-protein diets in some regions, perhaps persons would start to experience the higher cardiovascular risk, anaemia or mineral bone disorders at higher levels of serum-creatinine based eGFR than the <60 mL/min/1.73 m2 threshold currently applied worldwide.
We do want to emphasise that, in every other country except Nigeria, a substantial majority of persons with CKD seemed to fit one of the three predefined profiles, derived from data on attributes of persons with CKD in HICs. The relative contribution of diabetes and vascular disease differed across the countries and could help to refine the ‘best-buy’ approach to CKD management. As borne out by data from the Million Death Study capturing the increasing number of kidney failure deaths in India and with a lions’ share attributable to diabetes mellitus,32 diabetes prevention and treatment would likely substantially reduce the CKD burden in urban India. In Moldova, smoking reduction and vascular risk management may be more relevant. Obesity with a cardiovascular risk factor was consistently associated with between 20% and 30% of persons with CKD across all countries. Performed in a range of ethnicities, several studies have established obesity as a risk factor for incident ESRD.21 33 34 We need innovative approaches that integrate CKD detection and triage into the management of obesity, vascular disease and diabetes35; limited resources for renal replacement therapy that might be applied to persons who progress to ESRD in LMICs lend greater urgency to this need.
This analysis has several strengths. Most importantly, information was either uniformly collected (for the three LMICs incorporated by the ISN) or easily harmonised. Three of the cohorts were nationally representative (China, urban India and the USA), and those that were not captured have diverse populations in terms of age, sex and other clinical characteristics to allow for reasonable inferences. Sample sizes were reasonably large, allowing for precise estimates of means and proportions. Serum and urine were collected from most participants, which allowed for identification of perso0ns with albuminuria/proteinuria as well as those with reduced kidney function.
There are also several important limitations. In addition to under-reporting of some lifestyle factors (eg, tobacco use) and medical history that were captured only by self-report, the higher prevalence of CKD in the ISN KDDC studies points to a degree of self-selection among participants. Thus, the profile categorisations from these studies may not be fully generalisable but rather may indicate distribution of CKD profiles within country-specific, clinic-based populations. As such, it is possible that proportion of persons with CKD without traditional risk factors is higher in the general population than in a population willing to attend screening. Moreover, the ISN KDDC laboratory methods for measurement of creatinine were not standardised, which could introduce bias both for comparison of the CKD prevalence between study sites and for adequate calculation of eGFR with the CKD-EPI, which assumes creatinine standardisation. However, in each of the ISN KDDC countries, creatinine measurement was calibrated according to manufacturing guidelines, which should have prevented major bias. Since urine dipstick, rather than quantitative measures, was the predominant form of proteinuria assessment in Nepal, there is potential for higher misclassification of persons as having CKD36 in this study in particular, although proteinuria determined on urine dipstick alone also confers higher risk for progressive kidney disease.37
While few data elements were missing, only one serum and one urine sample were obtained. As such, we would expect some misclassification of CKD, which could be mitigated had the programme obtained three or more serum or urine samples. The criteria we used for determining profiles 1, 2 and 3 (diabetes mellitus, vascular disease and obesity with one or more cardiovascular risk factors) are imperfect. Therefore, even if we were to accurately estimate the prevalence of CKD, we could misclassify persons by profile. Differences in missingness could result in misclassification into profile 4 as well; we noted this problem in particular for Moldova, which could mean that potentially even fewer than the currently estimated 21% of persons with CKD would have CKD without established risk factors. Replication of our approach would thus require careful attention to missingness of data elements defining profiles 1–3. Finally, for persons falling in profile 4, we had limited additional information to evaluate potential correlates for CKD (eg, birth weight, occupation, underlying rheumatologic disease, medication use or family history).
In summary, using nationally representative data from three populous countries (one HIC and two LMICs) and uniformly collected data from three smaller LMICs, we categorised persons within three common profiles of CKD. We found that the majority of persons with CKD in each of these widely disparate countries have CKD in association with diabetes mellitus, vascular disease or obesity. Screening and detection efforts could be streamlined by considering these subtypes of risk. Region-specific definitions for CKD markers, novel genetic susceptibilities and/or environmental influences should be considered in regions with higher than expected CKD prevalence and/or where a disproportionate fraction of persons with CKD do not have one of these three risk profiles.
Acknowledgments
We thank the doctors, nurses, local students, volunteers and organisations involved in the country screening programs for their active participation and support, which made collection of clinical data in the International society of nephrology kidney disease data center study database possible. We also thank the study coordinators, research assistants and participants of the US national health and nutrition examination survey, India center for cardiometabolic risk reduction in South Asia and China kidney disease studies for their participation in these large-scale efforts.
References
Footnotes
Handling editor Seye Abimbola
Contributors SA and GMC conceived the analysis. GR, VJ, DP, LZ and MEM-R provided feedback on the analysis plan. YZ led the analyses. WJW, NP and SC assisted with data cleaning and merging. KMVN, NT and VM reviewed multiple drafts. SA led the writing. All authors reviewed and approved the final draft.
Funding SA is supported by the National Institute for Diabetes and Digestive and Kidney Health (grant no. K23 DK101826). GMC is supported by the National Institute for Diabetes and Digestive and Kidney Health (grant no. K24 DK 085446). The Center for Cardiometabolic Risk Reduction in South Asia (CARRS) study was supported by the National Heart, Lung and Blood Institute (contract no. HHSN2682009900026C, CARRS study). The China study was supported by the Ministry of Science and Technology. The International Society of Nephrology (ISN) Kidney Disease Data Center screening programs in Moldova, Nepal and Nigeria were funded partly by a dedicated grant from the ISN Research and Prevention Committee.
Competing interests None declared.
Ethics approval All individual studies collated in this analysis underwent IRB approval at their respective institutions. Only de-identified data were used in this analysis.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement De-identified data used in this analysis are available to collaborators after review by steering committee members of the individual studies.