Article Text

Abstract
Introduction Visceral leishmaniasis (VL) is a neglected parasitic disease with a high fatality rate if left untreated. Endemic in Morocco, as well as in other countries in the Mediterranean basin, VL mainly affects children living in rural areas. In Morocco, the direct observation of Leishmania parasites in bone marrow (BM) aspirates is used to diagnose VL and meglumine antimoniate (SB) is the first line of treatment. Less invasive, more efficacious and safer alternatives exist. In this study we estimate the cost-effectiveness of alternative diagnostic-therapeutic algorithms for paediatric VL in Morocco.
Methods A decision tree was used to estimate the cost-effectiveness of using BM or rapid diagnostic tests (RDTs) as diagnostic tools and/or SB or two liposomal amphotericin B (L-AmB) regimens: 6-day and 2-day courses to treat VL. Incremental cost-effectiveness ratios, expressed as cost per death averted, were estimated by comparing costs and effectiveness of the alternative algorithms. A threshold analysis evaluated at which price L-AmB became cost-effective compared with current practices.
Results Implementing RDT and/or L-AmB treatments would be cost-effective in Morocco according to the WHO thresholds. Introducing the 6-day course L-AmB, current second-line treatment, would be highly cost-effective if L-AmB price was below US$100/phial. The 2-day L-AmB treatment, current standard treatment of paediatric VL in France, is highly cost-effective, with L-AmB at its market price (US$165/phial).
Conclusions The results of this study should encourage the implementation of RDT and/or short-course L-AmB treatments for paediatric VL management in Morocco and other North African countries.
- visceral leishmaniasis
- health economics
- diagnostics and tools
- treatment.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known about this topic?
Visceral leishmaniasis (VL) is a life-threatening parasitic disease endemic in the Mediterranean basin. In Morocco and other countries in northern Africa VL mainly affects children living in poor rural areas.
In Morocco, VL is diagnosed by microscopy which requires an invasive procedure (bone marrow (BM) aspiration) and cases are treated using a toxic drug (meglumine antimoniate) which requires long and painful intramuscular injections.
Less invasive diagnostic tools (rapid diagnostic tests (RDTs)) and safer, short-course and more effective antileishmanial drugs (liposomal amphotericin B (L-AmB)) are available but their use in low-income and middle-income countries is limited due to their high cost.
What are the new findings?
Our cost-effectiveness analysis shows that using RDTs would be more effective and less costly than BM aspiration to diagnose paediatric VL.
More importantly, our study shows that treating children suffering from VL with short-course L-AmB regimens is also cost-effective in Morocco.
Recommendations for policy
RDT and short-course L-AmB regimens should be implemented to diagnose and treat paediatric VL in Morocco and other countries in the Maghreb.
The Ministries of Health in those countries and WHO should negotiate with the manufacturer of L-AmB to reduce the price of this drug to ensure all patients with VL in North Africa have access to the best treatment.
Introduction
Visceral leishmaniasis (VL), also known as kala-azar, is a neglected protozoal disease transmitted by sandflies.1 VL, caused by Leishmania infantum, is endemic in the Mediterranean basin, southern Caucasus, China and South America.1 Fatal unless treated, in northern African countries VL mainly affects children living in rural areas with low access to diagnosis and treatment.2 3 In Morocco, where an average of 152 cases were reported from 2004 to 2008 and 300 to 600 cases are estimated per year,4 VL is diagnosed and treated at district hospitals. According to the national guidelines,5 VL can be diagnosed by microscopic examination of bone marrow (BM) aspirate or using serological tests (eg, ELISA and Immunofluorescence Antibody Assay) in patients presenting with clinical symptoms: splenomegaly, fever and pancytopenia. Serological tests are usually not available in public hospitals so BM aspiration is the standard diagnostic method.6 BM, which is usually obtained by sternal aspiration in children, is an invasive and painful procedure with a variable and low sensitivity, ranging from 60% (95% CI 50% to 90%) to 77% (95% CI 71.5% to 81.5%).7 8 Meglumine antimoniate (SB) (20 mg of SB/kg/day parenterally for 20 days) is the first line of treatment. SB treatment is painful, requires long hospitalisation and is highly toxic. The case fatality rate in children treated with SB is high in North African countries9–16compared with other endemic countries such as Greece.17 Other factors such as concomitant infections or late diagnosis, more common in North African patients with VL, may increase the toxicity-related mortality. Liposomal amphotericin B (L-AmB) (18–25 mg/kg in six doses—days 1 to 5 and 10) is the second line of treatment in Morocco.5 L-AmB is the safest and most effective antileishmanial drug but it is rarely used in Morocco6 due to its high cost.18 Thus, the current standard of care of paediatric VL in Morocco is the examination of BM aspirates and the administration of 20 doses of SB for diagnosis and treatment, respectively. The median total cost associated to managing a paediatric VL case in Morocco is US$520 (IQR US$316–658).6 More sensitive and less invasive tests and safer drugs for VL exist but are not implemented in Morocco mainly due to high costs.
In the past 15 years, there have been major advances in the management of paediatric VL caused by L. infantum. An accurate rapid diagnostic test (RDT) for VL is available,19 with an associated sensitivity of 83.2% (95% CI 74.1% to 90.8%) and specificity of 99.8% (95% CI 99% to 100%) (Cruz et al, unpublished). This RDT only requires a small blood sample obtained by finger prick and could be used as a diagnostic tool in hospitals attending VL suspects.1 More importantly, SB has been replaced by L-AmB to treat VL in European countries where this disease is also endemic. Two L-AMB regimens are being implemented: 3–4 mg/kg/day of L-AmB on days 1 to 5 and 10 (total dose 18–24 mg/kg)20–22 in Spain and Italy and 10 mg/kg daily of L-AmB for two consecutive days (total dose 20 mg/kg)17 23 24 in France and Greece. Please note that the treatment used in Spain and Italy is the second-line treatment in Morocco.5 These treatments which are expensive due to the cost of L-AmB (US$165 per phial)23 have been proven cost-effective in Europe as they are safer, more efficacious and reduce the hospitalisation of patients compared with SB treatments.17 21 23
The reasons explaining why a child suffering from VL in Morocco does not receive the same treatment as a child suffering the same disease 14 km further north (the distance between Morocco and Spain) are usually associated to the cost of L-AmB. However, the cost-effectiveness of the shorter and safer L-AmB treatments for VL has never been assessed in the Moroccan or North African context. Furthermore, the cost of L-AmB can be reduced. WHO and Gilead, the manufacturer of Ambisome, the only L-AmB currently registered as a VL drug, agreed to reduce the price of L-AmB to US$18 per phial for the public sector and not-for-profit organisations to treat patients with VL in the most VL-endemic countries (eg, India, Nepal or Bangladesh). In 2015 WHO received a request from the ministries of health of Algeria, Morocco and Tunisia so as to get L-AmB at a WHO-negotiated price with the aim of introducing it as the first-line treatment for VL. WHO discussed the situation with the manufacturer, Gilead, which agreed to move forward and initiate the formalities to make that happen (Ruiz-Postigo, personal communication).
In this study we estimated the cost-effectiveness of using RDT to diagnose and/or L-AmB regimens to treat paediatric VL in Morocco compared with current standard of care (ie, BM and SB). We also estimated the impact of reducing the cost of L-AmB on the cost-effectiveness ratios. The results of this study should help the ministry of health and paediatricians in Morocco in deciding if the RDT and/or L-AmB treatments should be implemented to manage paediatric patients with VL. The results will also inform the ministry of health on the current negotiations to reduce the cost of L-AmB. The information generated in this study may trigger changes in the health policies in Morocco, and in other North African countries facing similar clinical and epidemiological challenges.
Methods
Study design
Current practices for the management of suspected cases of VL in Morocco; microscopic examination of BM for diagnosis and treatment with 20 mg/kg a day of SB for 20 days (strategy A), were compared with the adoption of RDT for diagnosis and two different short-course regimens of L-AmB: (1) 6-day course: 3 mg/kg a day on days 1 to 5 and 10,21 and (2) 2-day course: 10 mg/kg a day for two consecutive days.17 24
Six strategies were compared. By combining the two diagnostic tools (BM and RDT) and the three VL treatments (SB, and two L-AmB regimens) the following strategies (A to F) were considered: (A) BM for diagnosis and SB for 20 days for treatment (current practices); (B) BM for diagnosis and 6-day course L-AmB for treatment, (C) BM for diagnosis and 2-day course L-AmB for treatment, (D) RDT for diagnosis and SB for 20 days as treatment, (E) RDT for diagnosis and 6-day course L-AmB for treatment, and (F) RDT for diagnosis and 2-day course L-AmB for treatment (table 1).
Diagnostic-treatment strategies for paediatric visceral leishmaniasis (VL) management in Morocco
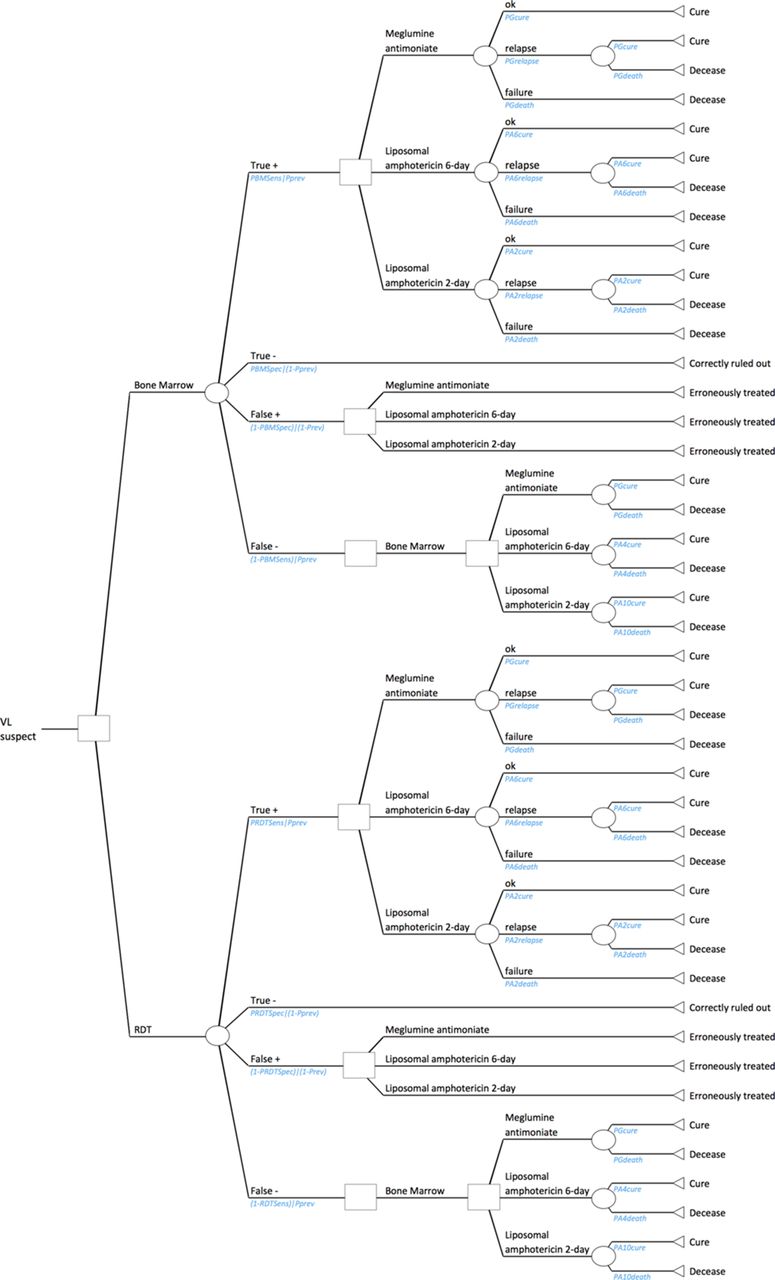
A decision tree was employed to evaluate the cost-effectiveness of the different strategies by estimating the costs and effects associated with each strategy of a theoretical cohort of 100 children with suspected VL (figure 1).25 A suspect case was defined as a child living in a VL-endemic area in Morocco presenting with VL symptoms: persistent fever and splenomegaly. In our model a VL suspect attending a district hospital in Morocco was either diagnosed by BM aspiration or RDT. If the patient was confirmed as a patient with VL it was then treated either with SB, a 6-day course or a 2-day course L-AmB.

The decision tree. The figure illustrates the possible outcomes of a theoretical visceral leishmaniasis (VL) suspect attending the Moroccan healthcare. The outcome is determined by the diagnostic tool (bone marrow (BM) aspiration or rapid diagnostic test (RDT)) and treatment regimen (meglumine antimoniate (SB), 2-day course or 6-day course liposomal amphotericin B (L-AmB)) used, which represent the six strategies analysed in the study.
Modelled effects
The probabilities used in the decision analysis model were obtained from previous studies. The probability that a VL suspect was a true VL case was obtained from the prevalence of the disease among the suspected cases in Morocco.6 Sensitivity and specificity of the diagnostic tools (BM or RDT) were adopted from studies on L. infantum VL,8 including an unpublished work by Cruz et al.
Once diagnosed, sensitivity and specificity of the diagnostic test determined four possible outcomes. First, a true positive case would imply treating the patient, resulting in three different outcomes depending on the probabilities associated to the treatment: complete cure, death or relapse. When a relapse occurs, we assumed the patient would receive the same treatment as earlier and be cured or die according to the respective probabilities. Second, a true negative case would correctly rule the patient out and exit the model alive. Third, a false positive case would wrongly be treated with a small risk of death related to the toxicity of the drug used.26 Finally, although a false negative case would translate into no treatment, we assumed that the severity of symptoms would make the practitioner take a BM test to confirm VL infection. The patient would be cured or die according to the probabilities associated to the treatment.
All probabilities of cure, death and relapse associated with SB,3 9–17 27 28 as well as both L-AmB regimens,17 20–24 29 30 were obtained from a literature search on VL caused by L. infantum in North Africa or Europe (see online supplementary annex S1). Due to the lack of reliable estimates in Morocco, we disregarded patients’ perception of health improvements or drug resistance issues; and assumed full compliance to treatment given that the nature of treatment regimens implied hospitalisation for completion. However, we included relapses, as they are commonly reported in the Mediterranean basin.17
Hospitalisation, treatment and diagnostic costs
Hospitalisation costs, including diagnostic tests and treatments, were retrieved from primary data collected in 2014.6 Individual clinical and cost records consisted of resources for the management of confirmed VL cases. The use of each resource was multiplied by the respective unit official price to obtain an estimation of costs for the healthcare provider.31 32
In our model, patients received the complete treatment during hospital admission. We used the mean hospitalisation daily cost for inpatient VL and multiplied it by the length of stay (number of days) to estimate the total hospitalisation cost, which included hotel costs and other diagnostic tests and treatments not directly related to VL treatment and diagnosis. The total number of hospitalisation days depended on the test capacity to diagnose VL and the treatment duration related to each drug regimen. The number of days before starting treatment slightly varied depending on the diagnostic tool considered, while the number of days after starting treatment substantially differed between drug regimens (table 2).
Input variables of the deterministic and probabilistic cost-effectiveness analysis
The VL diagnosis cost reported in a previous study in Morocco was used.6 A personal communication estimation from the WHO’s Head of the Leishmaniasis Control Programme (Ruiz-Postigo, personal communication) was used as price of an RDT which was later contrasted by other works published in the literature.33 34
Since the VL treatment cost directly depended on the number of phials required according to patient’s weight, we applied the distribution of the patients’ weights in our sample to the theoretical cohort of 100 children in our model (see online supplementary material in Tachfouti et al).6 We employed the price of L-AmB reported in the literature,23 and used the local price of SB6 incorporating uncertainty by considering the international market price.35 As a supplementary analysis we used the WHO-Gilead negotiated price (US$18 per phial) of L-AmB. The total cost of VL treatment was estimated for the three drug regimens as:

being

Costs were discounted at a 3% rate, converted to US$2014 and inflation adjusted.36 37
Analyses
Cost-effective analysis
We undertook a deterministic cost-effective analysis by taking the most likely values for the parameters used in the model. We further adopted a probabilistic approach to incorporate uncertainty in the model parameters.38 As showed in table 2, parameters were expressed as probability distributions. Distributions and ranges were obtained either from our estimations6 or from published articles.3 5 6 9 11–17 20–24 27–30 32–35 39–42 For those parameters where no data were available, probability distributions were constructed assuming standard deviations (SD) of 1%, 10%, 15%, 20% or 100%, depending on the parameter’s level of potential uncertainty.
For each strategy, we computed associated expected costs and deaths in the absence of disease detection or adequate response to treatment. Incremental costs and deaths averted were used to compute the incremental cost-effectiveness ratios (ICERs) between two strategies. Monte Carlo simulations were used to estimate 95% CIs for all input parameters and for model outcomes.43
WHO cost-effectiveness thresholds for disability-adjusted life-years averted were employed to identify cost-effective (ICER below three times the World Bank estimation of 2014 Moroccan Gross domestic product (GDP) per capita) and highly cost-effective alternatives (ICER below the World Bank estimation of 2014 Moroccan GDP per capita, US$3 190).44 If an alternative strategy would reduce the mean cost with respect to current practices it will be denoted as cost-saving.
Acceptability curves
Acceptability curves were constructed to represent the probability of the alternative strategies to be cost-effective depending on a theoretical willingness-to-pay per death averted.45
Sensitivity analysis
We undertook one-way sensitivity analysis to determine the impact on cost-effectiveness results of changes in selected parameters (see online supplementay table S2). These checks included varying the cost of BM at a reduced price ($5.90 per unit), the price of SB at the officially subsidised price ($1.70 per phial), the prevalence level among the clinical suspects (decreasing it to 50% of suspects and increasing it to 100%), a fixed reduced mortality rate (2%) and increased efficacy (93.4%) for SB regimen, assumed 100% cure in patients treated again with L-AmB, and adopting alternative values of BM sensitivity (60%, ranging from 50% to 90%) and specificity (100%),7 as well as RDT sensitivity (92%, 91.49%–92.92%) and specificity (95%, 94.30%–95.48%).19
Moreover, we checked for changes in results derived from a reduction in the uncertainty of parameters collected on site (days before receiving diagnosis and days until receiving treatment), as parameters that were modelled based on individual data accounted higher uncertainty than those in which an SD was assumed. We applied specific SDs of 15% to the most likely values following log-normal distributions, as done for L-AmB parameters.
Threshold analysis
We finally carried out a probabilistic threshold analysis to identify at which price the adoption of L-AmB regimens (strategies B and C) became cost-effective interventions compared with current practices. We graphically represented ICERs and their respective CIs for marginal reductions of L-AmB price from its market price to zero.
Microsoft Excel 2007 was used for data analysis.
Results
Cost-effective analysis
Table 3 presents the expected costs and effects of each strategy of the probabilistic analysis taking the market price of L-AmB, ordered from the cheapest to the most expensive. Each strategy was compared with the one immediately cheaper. Strategy D was the least costly strategy and dominated current practices (strategy A) by slightly increasing the deaths averted due to improvements of the diagnostic performance. Current practices (strategy A) in Morocco remained the least effective strategy, while strategy F resulted in the most effective one. Strategy B although highly effective, was the most costly strategy of all the combinations of diagnosis and treatment considered in the study. Overall, strategies with treatment regimens based on L-AmB (strategies B, C, E and F) were more expensive but averted more deaths than strategies based on SB (strategies A and D), regardless of the diagnostic tool used. Two-day course L-AmB strategies (strategies C and F) averted more deaths and were clearly cheaper than 6-day course L-AmB strategies (strategies B and E). Furthermore, strategies using RDT as a diagnostic tool (strategies D, E and F) were less costly and slightly more effective than strategies using BM aspiration. Results of the deterministic analysis (see online supplementary table S3) were similar to those obtained from the probabilistic analysis.
Probabilistic results: cost-effectiveness (C-E) analysis of management of 100 VL suspects (L-AmB at market price)
Table 4 shows the results of the cost-effectiveness analysis when comparing current practices (strategy A) to each remaining strategy. Adopting RDT as the diagnostic tool if SB is maintained as the treatment regimen (strategy D) it dominated current practices by reducing the cost by US$10 269 (95% CI 9 412 to 11 127) without decreasing efficacy. When comparing the use of L-AmB maintaining BM as the diagnostic tool, only the 2-day course regimen (strategy C) became cost-effective compared with current practices, as the 6-day course L-AmB (strategy B) ICER was lower than the WHO threshold. When compared with current practices, strategy C allowed to avert 4.82 (95% CI 4.77 to 4.88) deaths by increasing to US$16 118 the cost of managing a 100 paediatric VL suspects, resulting in an ICER of US$3 486 (95% CI 3 059 to 3 913) per death averted. By adopting both the RDT and the L-AmB treatment regimens, the 2-day course (strategy F) became a highly cost-effective strategy (value below the GDP per capita) as it averted almost 4.93 (95% CI 4.87 to 4.98) deaths by increased cost of managing a 100 paediatric VL suspects in US$5 742 US$ (95% CI 3 468 to 8 017), resulting in an ICER of US$1 136 (95% CI 658 to 1 614) per death averted. Strategies in which treatment consisted of a 6-day course L-AmB (strategy B and E) were not cost-effective alternatives to current practices at the market price of L-AmB. As shown in the supplementary analysis, if Morocco would get L-AmB at US$18/phial, all the strategies using L-AmB-based regimens would be cost-saving compared with strategies using SB (see online supplementary table S4).
Probabilistic results: pairwise comparison between current practices (strategy A) and the other strategies to assess for cost-effectiveness
Acceptability curves
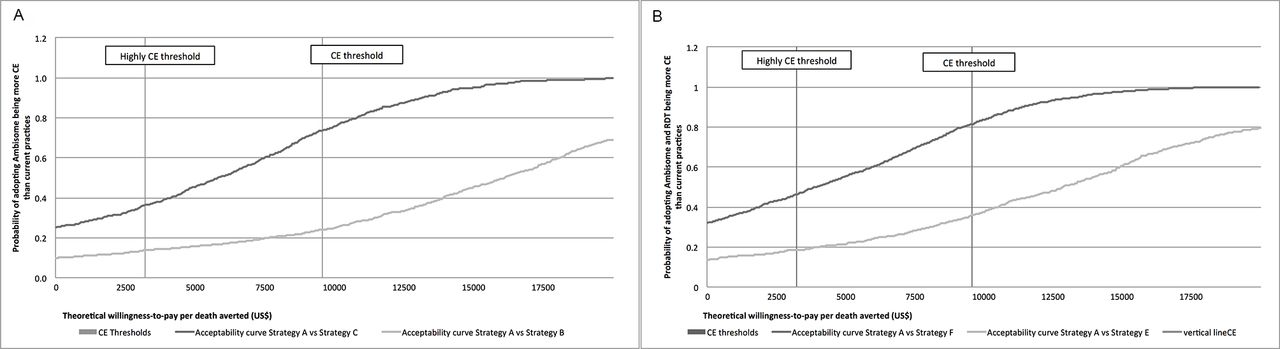
Figure 2 shows the cost-effectiveness acceptability curves when the market price of L-AmB is used. When evaluating the introduction of L-AmB (figure 2A), strategy C was cost-effective in 74% of simulations and strategy B in 24% of them. When evaluating the adoption of RDT and L-AmB (figure 2B), strategy F was cost effective in 82% of simulations, and strategy E in 36% of them. Two-day L-AmB regimen strategies involved cost-savings in 25% (strategy C) and 32% of simulations (strategy F).
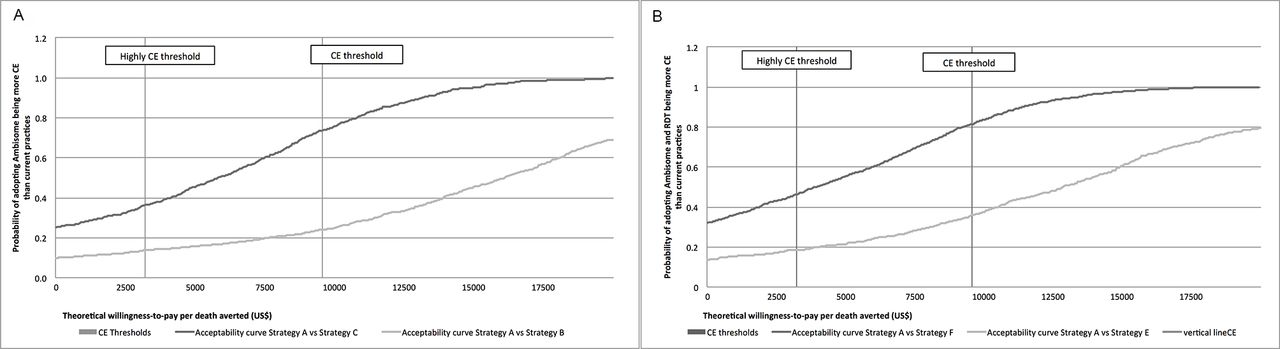
Cost-effectiveness acceptability curves. (A) Compares current practices (strategy A: bone marrow (BM) aspiration to diagnose and meglumine antimoniate (SB) to treat) with the adoption of two different short-course liposomal amphotericin B (L-AmB) regimens: strategy B - light grey and strategy C - dark grey. (B) Compares current practices with the adoption of both, rapid diagnostic test (RDT) to diagnose and two different short-course L-AmB regimens: strategy E - light grey and strategy F - dark grey. For both figures, the y-axis represents the probability of the strategies to be cost-effective for each level of willingness-to-pay per death averted (x-axis). The vertical lines represent thresholds for cost-effective(US$9 571, corresponding to three times the Moroccan GDP per capita) and high cost-effective (US$3 190, corresponding to the Moroccan GDP per capita) interventions.
Sensitivity analysis
Modifying the SB or BM prices, the sensitivity and specificity of BM or RDT, SB mortality and efficacy and VL prevalence among suspects did not alter the outcome of the cost-effectiveness analysis (see online supplementary table S5). More precisely, the univariate analysis of the BM price, alternative sensitivity and specificity values for BM and RDT and VL prevalence had a negligible impact on costs and effectiveness, while fixing SB mortality rate to 2% increased effectiveness but costs associated with those alternative remained invariant, as were the conclusions of the cost-effectiveness evaluation. Decreasing the SB price to its subsidised value reduced the total cost of SB-based strategies (A and D) by 12% to 14%.
Threshold analysis
Results from the threshold analysis are represented in figure 3 and detailed in online supplementary table S6. Strategy B (6-day L-AmB) was not cost-effective when the cost per L-AmB phial was above US$140. The 6-day L-AmB treatment would be cost-effective with phial prices ranging from US$100 to US$140 and would be highly cost-effective with L-AmB price below US$100/phial (ICER of 3865; 95% CI 3182 to 4548). If the price per phial of L-AmB could be reduced below US$75, the 6-day L-AmB treated would be cost saving. Strategy C (2-day L-AmB) remained cost-effective for all prices of L-AmB considered (max US$180/phial) and resulted highly cost-effective at prices of US$175/phial (ICER of 3 073; 95% CI 2527 to 3 619) or below. If the price of L-AmB was reduced below US$140/phial the 2-day L-AmB regimens (strategy C) would be cost saving.

{kind=link}
{kind=link}
{kind=link}
Threshold analysis. The figure evaluates at which price the use of liposomal amphotericin B (L-AmB) became cost-effective compared with current practices. The horizontal lines represent the cost-effective (CE) (US$9 571) and highly CE (US$3 190) thresholds. Strategy B is a combination of diagnoses based on bone marrow (BM) and microscopic examinations and treatment of 6-day course L-AmB, while strategy C is a combination of diagnosis based on BM and microscopic examinations and treatment of 2-day course L-AmB.
Discussion
Based on the results of this study the Ministry of Health (MoH) in Morocco should implement the use of RDT to diagnose paediatric patients with VL without further delay. The treatment of patients with VL should also be reviewed: L-AmB should be used to treat VL in children in Morocco. The MoH in Morocco and other North African countries in collaboration with WHO should negotiate the price of L-AmB with Gilead.46 The negotiations should aim at reducing the cost of an L-AmB phial below US$140 so the 6-day 3 mg/kg L-AmB regimen, currently the second line of treatment in Morocco,5 replaces the toxic SB-based treatment. However a price below US$75 per phial would be preferred as it would ensure this L-AmB-based regimen is implemented immediately as it will be cost-saving. This cost per phial remains significantly higher than the one currently applied in other VL-endemic countries like India or Bangladesh (US$18/phial). If Morocco and other countries in North Africa could purchase L-AmB phials at this cost, treating VL in children would be significantly cheaper and safer than using SB (see online supplementary table S4).
As an alternative, the MoH in Morocco could adopt the treatment regimen used in France and Greece to treat paediatric patients with VL: 2-day 10 mg/kg L-AmB.17 22 This strategy is cost-effective even when the market price of L-AmB is used (US$165/phial). However, as before, reducing the cost per phial (below US$140) would facilitate the implementation of this L-AmB-based regimen. There is evidence that the 2-day L-AmB regimen is a safe and effective treatment for paediatric VL17 22 but it is still not recommended by WHO.1 Clinical trials in Morocco and other countries in North Africa should be conducted to demonstrate the efficacy of 2-day L-AmB regimen to treat L. infantum VL in children in the region. These results may prove valuable for other regions with similar VL epidemiology, such as the Caucasus,47 Albania,48 South America or China.1 However, further research is needed to evaluate if the introduction of L-AmB-based regimens would yield cost-effective results in regions with different health systems and economic contexts.
The adoption of RDT and L-AmB-based regimens to manage patients with VL in the Maghreb is supported by experts in the region46 as they have a number of advantages, in particular from the patient’s perspective, that have not been considered in our study. For example using RDT would reduce the discomfort in children as they are significantly faster, less invasive and less painful than BM aspiration.29 L-AmB regimens are safer, have fewer side effects and lower case fatality rates than SB,49 and they are less painful than SB treatments that require intramuscular injections for 20 days. L-AmB treatments also reduce the number of hospitalisation days. This has an impact on the cost of the treatment as shown in our and other studies,23 and it also benefits the patients and their families by reducing the indirect costs associated with caregivers accompanying the patients, such as the time lost from productive work or housekeeping activities, cost of transport and other out-of-pocket expenses. Those indirect costs can be significant in the VL context.31 50 The results of our cost-effectiveness analysis are thus conservative. Including the patient’s perspective would have increased the cost-effectiveness of the alternative strategies proposed.
In our study we evaluated the use of RDT to diagnose VL at the hospital level as it is one of the options suggested by WHO.1 We did not assess the use of RDT in primary health centres as the prevalence of VL in Morocco is lower compared with in countries where this strategy is implemented (eg, India).51 However the use of RDT in peripheral health centres to triage or diagnose VL suspects may be an option to consider if the VL-endemic areas in Morocco continue to expand.52 Similarly, in our model we assumed that SB treatment was performed in the hospital as indicated by the national guidelines.5 However a recent study6 showed that a significant number of children suffering from VL in Morocco receive an ambulatory treatment in primary health centres. This approach reduces considerably the costs per patient (US$307) but it is not recommended by experts or WHO1 as SB treatment requires close monitoring.
The cost data used in the model were based on individual-level data collected in hospitals in Morocco.6 In contrast, the estimates of RDT, BM accuracy and L-AmB treatments efficacy used in the model were obtained from other L. infantum-endemic areas, as clinical trials evaluating their performance are scarce in North African countries.53 Notwithstanding, as shown in the sensitivity analysis, varying those key parameters did not have a significant impact on the cost-effectiveness results. Our model neither considers the natural history of the disease,54 nor a dynamic transmission of it,55 but it remains easy to understand and potentially more useful for health policy decisions.
Despite the results of our cost-effectiveness study both BM and SB have their place in paediatric VL management in Morocco. For example, BM is used to search for haematological malignancies such as leukaemia, which are part of the differential diagnosis for VL. And SB treatments, which are still in use in some European countries,29 48 56 can help treat patients with VL not responding to L-AmB treatment.57
Conclusion
The high cost should not limit the use of better diagnostic tools and safer treatments to manage paediatric patients with VL in Morocco. The results of this study should trigger the implementation of RDT and L-AmB to diagnose and treat VL in children in Morocco and other countries in the Maghreb. The data generated should also help the MoH in those countries and WHO to negotiate the price of L-AmB with Gilead to ensure all patients with VL in the Maghreb, and in particular paediatric patients, are treated with the best antileishmanial drug.
Acknowledgments
The authors thank Dr Cruz and Dr Ruiz-Postigo for providing relevant data for the analysis. ISGlobal is a member of the CERCA Programme, Generalitat de Catalunya.
Acknowledgments
The authors thank Dr Cruz and Dr Ruiz-Postigo for providing relevant data for the analysis. ISGlobal is a member of the CERCA Programme, Generalitat de Catalunya.
References
Footnotes
Contributors Study design: ES and AP; Data collection: SA, NT and AN; Data analysis: SA and ES; Data interpretation: SA, NT, AN, ES and AP; Writing first draft: SA, ES and AP; Writing final paper: SA, NT, AN, ES and AP.
Funding Funding was provided by Thrasher Research Fund, Salt Lake City, USA—Early Career Award # 12021 (https://www.thrasherresearch.org/). The funders of the study had no role in the study design, data collection and analysis, interpretation or reporting of this work, or the decision to submit the work for publication.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.