Article Text

Abstract
The WHO Safe Childbirth Checklist (SCC) was developed to ensure the delivery of essential maternal and perinatal care practices around the time of childbirth. A research collaboration was subsequently established to explore factors that influence use of the Checklist in a range of settings around the world. This analysis article presents an overview of the WHO SCC Collaboration and the lessons garnered from implementing the Checklist across a diverse range of settings. Project leads from each collaboration site were asked to distribute two surveys. The first was given to end users, and the second to implementation teams to describe their respective experiences using the Checklist. A total of 134 end users and 38 implementation teams responded to the surveys, from 19 countries across all levels of income. End users were willing to adopt the SCC and found it easy to use. Training and the provision of supervision while using the Checklist, alongside leadership engagement and local ownership, were important factors which helped facilitate initial implementation and successful uptake of the Checklist. Teams identified several challenges, but more importantly successfully implemented the WHO SCC. A critical step in all settings was the adaptation of the Checklist to reflect local context and national protocols and standards. These findings were invaluable in developing the final version of the WHO SCC and its associated implementation guide. Our experience will provide useful insights for any institution wishing to implement the Checklist.
- child health
- health policy
- maternal health
- obstetrics
- prevention strategies
© World Health Organization [2017]. Licensee BMJ. This is an open access article distributed under the terms of the Creative Commons Attribution N-Noncommercial IGO License (CC BY 3.0 IGO), which permits use, distribution, and reproduction for non-commercial purposes in any medium, provided the original work is properly cited. In any reproduction of this article there should not be any suggestion that WHO or this article endorse any specific organization or products. The use of the WHO logo is not permitted. This notice should be preserved along with the article's original URL.
Statistics from Altmetric.com
Key questions
What is already known about this topic?
Provision of life-saving interventions alone is not enough to reduce maternal and neonatal mortality; coverage needs to be matched with improvements in the quality of care.
WHO Safe Childbirth Checklist (SCC) aims to ensure proven essential maternal and perinatal care practices are performed by skilled birth attendants on admission, just before birth, soon after birth and on discharge.
Implementing such novel tools requires a carefully deliberated implementation strategy. It is important to test them in a diverse range of settings to help design the appropriate implementation support.
What are the new findings?
WHO established the WHO SCC Collaboration to explore questions addressing compliance, barriers to and success factors of effective and sustained use of the Checklist (pilot edition) in a range of settings around the world.
Most collaboration members established teams to lead the implementation of the Checklist, often with the use of formal training sessions as an initial step to launch the Checklist. This was often followed by ongoing supervision to monitor and encourage Checklist use.
The WHO SCC was easy to use and was felt to be of high value. End users with more experience, those who had not received any training and those who lacked supervisory support were more uncertain about the use and success of the Checklist.
A critical step in all settings was the adaptation of the Checklist to reflect local context and national protocols and standards.
Recommendations for policy
This work confirms the need for engaging key stakeholders, assessing the baseline situation and establishing a team of people with a wide range of professional backgrounds and roles before formally launching a novel tool such as the WHO SCC.
It is valuable to assess the initial knowledge and attitude of both supervisors and end users to better target training efforts.
Local adaptation with ongoing supervision, effective coaching and monitoring and sharing of data will encourage and motivate end users towards sustainable use of the tool.
Introduction
Despite significant progress in the delivery of maternal and child healthcare in recent years, there is still a high burden of mortality and morbidity among women of reproductive age and in the newborn.1–3 This is particularly so in low and middle-income countries. In 2015, it was estimated that 303 000 women died around the time of pregnancy and childbirth.3 Furthermore, approximately 2.7 million newborns died within the first month of life which represents 45% of all deaths in those under the age of 5.1 There were also 2.6 million stillbirths, half of which were estimated to have occurred during labour.2 Many of these deaths could have been prevented.1–4
Much of the early work in this field focused on improving access, such as facility-based deliveries by skilled birth attendants. This however resulted in a higher proportion of preventable deaths occurring at the health facilities.2 4 Subsequently, a WHO-led multicountry study suggested that the provision of life-saving interventions alone is not enough to reduce maternal mortality, but that provision needs to be matched with improvements in the quality of the care.5 Indeed, poor quality of care has been identified as the single major barrier to improving mortality and morbidity around the time of birth.5 6
To address this challenge, WHO has embarked on several initiatives, such as Every Newborn Action Plan7 and the Strategies Toward Ending Preventable Maternal Mortality.8 These include targets to reduce stillbirth and maternal and newborn mortality. The United Nations and WHO have also confirmed their commitment to address preventable maternal and neonatal deaths with the launch of the Sustainable Development Goals and the Global Strategy for Women's, Children's and Adolescents’ Health (2016–2030). This provides a framework for the implementation, follow-up and review of progress towards relevant targets.
In light of the clustering of morbidity and mortality around the time of childbirth and of the need for practical tools for improvement of the quality of care, WHO have also developed the WHO Safe Childbirth Checklist (SCC).9 10 This Checklist, built on the success of the WHO Safe Surgical Checklist,11 aims to help birth attendants through the process of the childbirth and the management of complications as they arise.
The Checklist is a list of essential evidence-based practices drawn from existing WHO guidelines. These practices should be performed at every birth to ensure the best outcome. The best practices are organised around four ‘pause points’, in other words critical moments where the birth attendant should pause to confirm what they are supposed to do or check if they have completed essential birth practices. The four pause points are: on admission, just before birth, soon after birth and on discharge. An early pilot study has shown that it markedly improves the delivery of essential practices by healthcare workers,9 thereby contributing to the improvement of quality of care.
More extensive information about the Checklist can be found on WHO website: http://www.who.int/patientsafety/implementation/checklists/childbirth/en/.
The WHO SCC collaboration and evaluation
Previous experience implementing such novel tools revealed the importance of testing them in a diverse range of settings and providing appropriate implementation support.12–14 When WHO released the WHO Surgical Safety Checklist, it was evident that success was driven by the presence of a defined implementation strategy.15
WHO therefore established a research collaborative—the WHO SCC Collaboration (the Collaboration)—to explore factors influencing use of the Checklist (pilot edition) in a range of settings around the world.16 Between November 2012 and March 2015, a total of 34 interested institutions working in over 200 sites in 29 countries across all six WHO regions registered projects with the Collaboration, and agreed to conduct implementation research and share their experiences as their projects progressed. Groups explored a range of questions that addressed compliance, barriers to and success factors of effective and sustained use of the Checklist. Members, as listed in table 1, were involved in frequent webinars and provided regular progress reports throughout the duration of the collaborative.
Collaboration members: location and institution leading the study
As part of the Collaboration, a formal evaluation was undertaken by WHO, Ariadne Labs and the Harvard T H Chan School of Public Health, that looked at facilitating factors and barriers to using the Checklist across different settings and helped inform the development of the final version of the WHO SCC and its implementation guide.17 Project leads from each collaboration site were asked to distribute two surveys: the first targeted end users experience of using the Checklist, and the second targeted implementation teams—those involved in planning, leading or helping with introduction of the Checklist—and their experience of introducing the Checklist at the targeted facility or group of facilities.
Over the 6-week evaluation data collection period, a total of 134 end users and 38 implementation teams responded to the surveys from 39 sites, across 19 countries. Lessons from Evaluation present the key findings from this process.
Lessons from the evaluation
Implementation process
For the most part, collaboration members established formal implementation teams. Over half modified the Checklist before introduction (58%) with a view to adapting it to their local context. For example, several teams removed HIV and replaced it with a hepatitis B check as this was felt to be more of an issue for their respective populations.
Nearly all teams reported that they had trained end users to use the Checklist (95%) and several stated that they had also organised question and answer sessions. However, although most end users received education about the purpose of the Checklist prior to its introduction (83%), fewer than two-thirds stated they were trained to use it (64%). Even fewer were coached or supervised while using the Checklist (34%).
When training was undertaken, topics included introduction on the importance of the Checklist and patient safety and how to use the Checklist, but also technical skills around the areas covered by the Checklist, such as hand hygiene or plotting a partograph. Two organisations reported using simulation and one completed ‘training of trainers’ for obstetricians and the nurse matron.
The implementation teams generally found the Checklist easy or very easy to introduce (81%). Most reported that they had adequate support from senior leadership (84%) throughout the introduction phase of the Checklist. However, 41% of teams reported that they had less financial resources than needed while 30% reported inadequate human resources to support implementation of the Checklist.
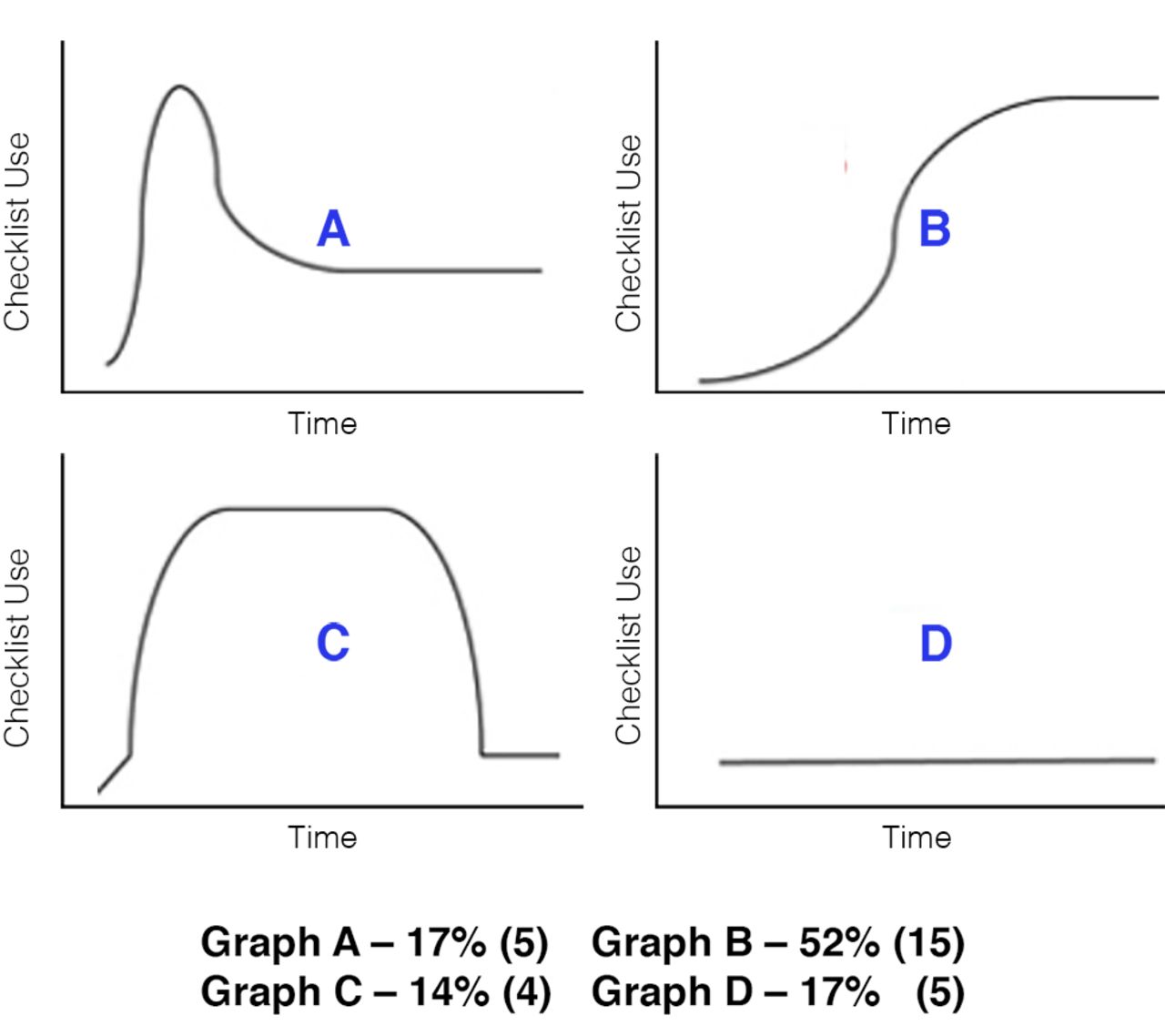
When presented with different curves showing how the Checklist might have been taken up over time, the majority of respondents identified with an initial slow then rapid and steady use over time (s-shaped curve B in figure 1).
{kind=link}
Uptake of the Checklist over time as perceived by implementation teams.
Implementation results
End users were willing or extremely willing to use the Checklist when first introduced (79%). They themselves reported that midwives and nursing staff were the most willing, while obstetricians/gynaecologists were the most resistant.
End users found the Checklist easy to use (33% very easy, 57% easy). The proportion who received training were more likely to report the Checklist as easy/very easy to use (70%) compared with those who had not received any training (15%).
Some 67% of end users thought that the Checklist improved their practice around the time of childbirth. They commented that the Checklist was helpful in preparation for delivery and in reminding to complete all essential steps, while providing early identification of risks and complications.
“It has enabled us to quickly detect risk… and for the prompt management of complications of mother and newborn.” (End user)
Nursing staff and medical doctors were more likely to believe that the Checklist improved practice than midwives, of whom majority felt it did not. Nearly three quarters of respondents felt the Checklist improved awareness of patient safety, and more than two-thirds of respondents felt that the Checklist improved communication and teamwork in their facility. Once again, midwives were less likely to believe the Checklist improved awareness or communication and teamwork. Respondents with more years of experience, those who had not received any formal training and those who did not have any supervisory support were less likely to believe that the Checklist improved practice, awareness of patient safety or communication and teamwork.
Implementation teams felt that the Checklist was of high value; 62% felt that significant or very significant progress had been made in the safety of childbirth as a result of using the Checklist. A large majority felt that using the Checklist significantly improved maternal and newborn care (72%) and nearly all of the teams said they would want the Checklist to be used for a family member or close friend (92%). Some 86% said that they would like to see the Checklist used in their facility in the future.
“Our use of the checklist highlights deficiencies in certain areas of practice. Obstetric emergencies were generally managed well but hand hygiene required improvement. There were deficiencies in preparation for key steps—partly highlighting a lack of key equipment.” (Implementation lead)
“The Checklist is a good idea and is easy to use. The uptake of this pilot study to global use will be a welcome development.” (Implementation lead)
Facilitating factors
End users and implementation team respondents were asked to list three factors that contributed positively to use of the Checklist. Responses included: characteristics of the tool, the way in which it was implemented and strong leadership (table 2). One end user noted that it worked ‘to establish a relationship of trust between the provider and patient’, while a common theme was well articulated by another end user who stated that ‘the checklist acts as a guide in monitoring and supervising labor hence enhancing patient's care and safety.’
Most commonly cited factors that contributed positively to use of the Checklist
Leadership engagement was considered critical by the implementation teams, most notably in motivating staff to use the Checklist and ensuring adequate supplies. The process of adaptation to reflect local context and ensure buy-in was also noted as useful in engaging leaders. Involvement of patient safety and quality assurance units were also among the top factors that contributed positively to use of the Checklist.
“Leadership engagement at the facility and from obs/gyn who helped with adaptation, training and ongoing supervision”
“Interest of the Obs/Gyn experts of the country who helped us to contextualise and adapt the checklist, and to train the medical doctors who are involved with the implementation of the checklist.” (Implementation lead)
Training, the availability of ongoing monitoring and supervision following training, as well as motivation were considered key to success. Many sites had senior staff who were trained to mentor, supervise and encourage others to use the Checklist.
Some facilities made the Checklist mandatory which was thought to facilitate implementation.
Challenges to implementation
Both end users and implementation teams also faced a number of challenges.
Challenges reported by the implementation teams included initial staff resistance, an initial impression of complexity about using the Checklist, the need for local adaptation and lack of supplies (both of the Checklist itself and essential birth supplies).
End users most commonly reported challenges relating to the working environment. Some examples include the inability to use the Checklist when they were too busy or understaffed and lack of awareness of the Checklist by other staff (due to turnover or other unspecified reasons).
However, both groups also reported effective solutions, which they implemented in response to a number of these challenges. These are presented in table 3. Training and ongoing supervision were cited as the main solutions, alongside ensuring the availability of key supplies. Several teams also varied the physical location and form of the Checklist, such as creating wall posters of it.
Challenges to implementation and suggested solutions
Conclusion
The experiences of end users and implementation teams using the WHO SCC (pilot edition) across a range of settings from high to low-income countries highlight the need to engage local leadership, enable local ownership and ensure local relevance and acceptability in facilitating initial implementation and successful uptake. Adaptation of the Checklist is essential to ensure consistency with local guidelines and to prompt willingness among end users to adopt the Checklist. Several studies have highlighted similar key factors to successful implementation.15 18 19 In addition, obstetricians and non-specialist medical doctors were the most resistant to using the Checklist. However, it was the midwives who felt that the Checklist did not improve practice. Implementation efforts should focus on overcoming reluctance from these professional groups through early engagement and education, for example.20
It is also important to ensure training and provide supervision throughout the implementation process. Unsurprisingly, those who received training or were supervised were more likely to believe that the Checklist improved practice, increased awareness of patient safety and/or improved communication and teamwork. This is in line with previous studies15 and further supports the role of coaching.21 Furthermore, we experienced a variety of challenges in implementing and using the Checklist. End users most commonly cited that they were too busy or understaffed to use the Checklist or that a lack of awareness of the Checklist by other staff had hampered its effective use. Teams also faced challenges with supplies, both with essential birth supplies and the Checklist itself. Implementation teams used an array of solutions to address these challenges, many of which focused on multidisciplinary education and regular training sessions.
The responses from which we have drawn these insight were subjective. It is important to conduct formal external evaluation which should include measurement of compliance with Checklist use, impact on adherence to essential birth practices and ultimately whether or not it improves maternal and neonatal outcomes. Many of the Collaboration members have undertaken research in these areas and have already set about publishing their results.20 Ariadne Labs are also currently undertaking a randomised controlled trial in India to explore the effect of Checklist use on maternal and newborn outcomes.21 The WHO SCC Collaboration was invaluable in helping us develop the ultimate version of the WHO SCC3 and its Implementation Guide. These were formally launched in December 2015 and are available on the WHO website.17 The Guide provides further details on the key facilitating factors identified in this evaluation, and highlights important factors for engagement, launch of the Checklist and ongoing support. The implementation guide is targeted for the facility level but it includes advice for a national level approach.
The Checklist is in line with the comprehensive WHO Framework for Improvement of the Quality of Maternal and Newborn Care22 that aims to achieve coverage of key practices, people-centred outcomes and eventually improved health outcomes. Eight standards of care have been developed to assist countries translate the framework into practice, and to make it even more explicit and actionable, each standard is accompanied by several quality statements that have been formulated to drive measurable improvements in the quality of care around the time of childbirth. These are valuable tools for policymakers22 providing a basis for broader national level quality improvement strategies. As part of the national efforts, WHO particularly encourages low and middle-income countries to implement the WHO SCC in health facilities, using the implementation guide to help inform the implementation process and support the sustained use of the Checklist.
Acknowledgments
The authors would like to thank Dr Gulmezoglu and Mr Banica for their oversight and support of this project, as well as the WHO SCC Collaboration members.
References
Footnotes
PWRG and BNS are joint first authors.
Contributors WRGP and SBN are joint first authors. All authors contributed to the writing and editing of the manuscript. WRGP, SBN and IL were responsible for the conception of the WHO Safe Childbirth Checklist Collaboration, which was subsequently run by SBN and WRGP with oversight of KT, NDK, NR, NK, LRH, KS and MM. All authors contributed to the design of the survey and subsequent analysis. TRD undertook statistical analysis.
Disclaimer The author(s) is(are) staff member(s) of the World Health Organization. The author(s) alone is(are) responsible for the views expressed in this publication and they do not necessarily represent the views, decisions or policies of the World Health Organization.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.
Data sharing statement WHO Safe Childbirth Checklist is available online at .