Article Text

Abstract
Background Critical illness is a leading cause of morbidity and mortality in sub-Saharan Africa (SSA). Identifying patients with the highest risk of death could help with resource allocation and clinical decision making. Accordingly, we derived and validated a universal vital assessment (UVA) score for use in SSA.
Methods We pooled data from hospital-based cohort studies conducted in six countries in SSA spanning the years 2009–2015. We derived and internally validated a UVA score using decision trees and linear regression and compared its performance with the modified early warning score (MEWS) and the quick sepsis-related organ failure assessment (qSOFA) score.
Results Of 5573 patients included in the analysis, 2829 (50.8%) were female, the median (IQR) age was 36 (27–49) years, 2122 (38.1%) were HIV-infected and 996 (17.3%) died in-hospital. The UVA score included points for temperature, heart and respiratory rates, systolic blood pressure, oxygen saturation, Glasgow Coma Scale score and HIV serostatus, and had an area under the receiver operating characteristic curve (AUC) of 0.77 (95% CI 0.75 to 0.79), which outperformed MEWS (AUC 0.70 (95% CI 0.67 to 0.71)) and qSOFA (AUC 0.69 (95% CI 0.67 to 0.72)).
Conclusion We identified predictors of in-hospital mortality irrespective of the underlying condition(s) in a large population of hospitalised patients in SSA and derived and internally validated a UVA score to assist clinicians in risk-stratifying patients for in-hospital mortality. The UVA score could help improve patient triage in resource-limited environments and serve as a standard for mortality risk in future studies.
- Africa
- critical illness
- early warning score
- MEWS
- qSOFA
- hospital mortality
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known about this topic?
Critical illness is a frequent cause of morbidity and mortality in sub-Saharan Africa.
Most critical care in sub-Saharan Africa takes place on general wards where human and material resources are limited.
A standard method for determining mortality risk can assist in clinical decision making.
What are the new findings?
A universal vital assessment (UVA) score was derived and validated in a large number of hospitalised patients from six countries in sub-Saharan Africa.
The UVA score was created using readily available clinical variables and could be applied in any resource-limited acute care setting.
The UVA score outperformed the modified early warning score (MEWS) and the quick sepsis-related organ failure assessment (qSOFA) score in predicting risk of death of hospitalised patients.
Recommendations for policy
The UVA score could assist clinicians in making triage decisions about appropriate level of care.
The UVA score may also help clinicians identify patients at moderate to high risk of death who could benefit from further diagnostic testing to determine underlying causes of illness or infection.
The UVA score may be useful in standardising risk of death of patients in future studies.
Introduction
In sub-Saharan Africa (SSA), critical illness in adults is a frequent and increasing cause of hospital admission and subsequent death, the majority of which is attributed to infection.1 Successful outcomes from critical illness depend on rapidly identifying deteriorating patients and intervening with therapies such as antimicrobials, fluid resuscitation and source control.2 However, intensive care units (ICUs) are unavailable in many district hospitals in SSA.3 Therefore, most critical care in SSA is administered on the general wards of district hospitals where diagnostic and therapeutic interventions are constrained.4
A better understanding of the severity of a patient's illness in resource-limited environments could improve allocation of human and material resources, and inform triage decisions in settings where a higher level of care is available. There are few examples of early warning scores (EWS) guiding therapy in hospitals in Africa. Use of the South African Triage Score in a rural emergency department in South Africa, in Botswana and in Somaliland led to undertriage and overtriage.5–7 A trial of an EWS to trigger nursing assessments on a surgical ward in South Africa showed no difference in outcomes compared with standard care, but a study in Uganda showed that targeted monitoring and resuscitation of adults with sepsis on admission can improve outcomes.8 9 Large investments in ICU infrastructure are unlikely to occur soon in these environments, but improved resource-appropriate assessment of patients on general wards may improve outcomes from critical illness.
The degree of aberration in vital signs can be used to assess illness severity and guide therapeutic interventions.10 Accordingly, vital signs have been incorporated into scoring systems such as the modified early warning score (MEWS) to identify deteriorating patients admitted to hospital.11 Recently, a consensus panel developed new definitions of sepsis that incorporated a clinically derived quick sepsis-related organ failure assessment (qSOFA) score to identify patients with infection and high risk of death.12 There are few EWS derived from patients in SSA and they were performed in small populations at single sites with varying performance.13 14 Therefore, we pooled data from hospital-based cohort studies conducted throughout SSA to (1) determine predictors of mortality, (2) create an accurate and easy-to-use universal vital assessment (UVA) score and 3) compare the performance of the UVA score in predicting mortality with that of MEWS and qSOFA.
Methods
Study design
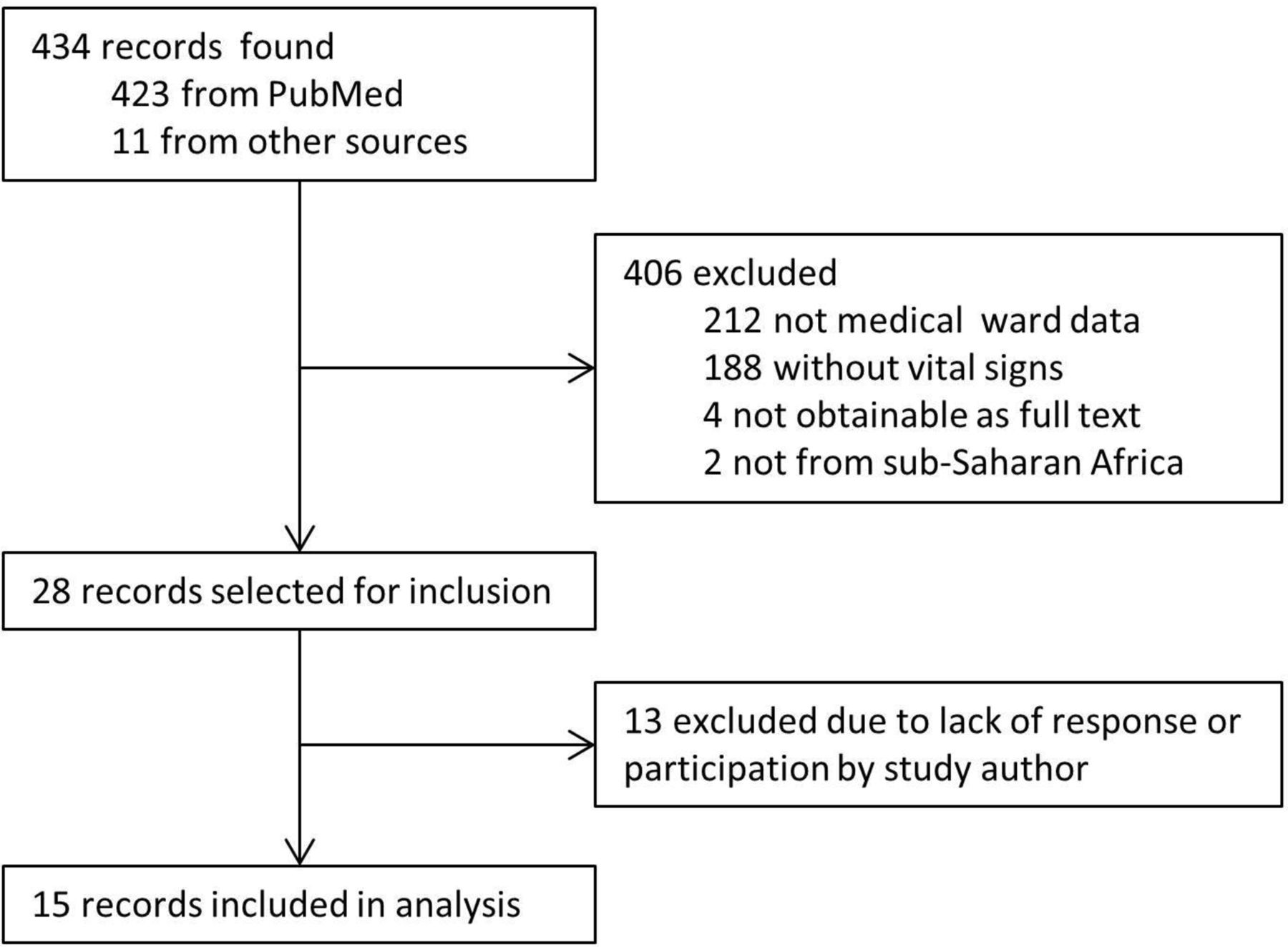
We conducted a retrospective cohort study using pooled data from hospital-based cohort studies throughout SSA. To identify appropriate cohorts for inclusion in the study, we performed a systematic literature search using PubMed with the following medical subject headings: (‘Hospital mortality’ or (‘hospitalization’ and ‘mortality’)) and ‘Africa South of the Sahara’. We limited the search to adults ≥19, the years 2000–2015 and the English language. This search provided 423 records. We also found 11 records from other sources, including 9 found from the references of the searched records and 2 unpublished data sets offered by corresponding authors. Of these 434 records, we selected 28 that fulfilled our criteria that included patients from SSA admitted to a medical ward with vital sign data and mortality outcomes. We then contacted the corresponding author to ask permission to access their de-identified study database. All included research on human subjects was approved by the appropriate ethics committee and conformed to the principles embodied in the Declaration of Helsinki.
Study population
We predefined selected variables to include in our models that were likely to be available in resource-limited clinical settings. Since we planned a comparison of the performance of the UVA score with that of MEWS and qSOFA, we ensured that the variables included in these scores were also included in our pooled data. The variables in the combined data set were admission temperature, heart and respiratory rate, systolic blood pressure (SBP), diastolic blood pressure (DBP), oxygen saturation, Glasgow Coma Scale (GCS) score, white blood cell (WBC) count, haemoglobin concentration, platelet concentration, whole blood lactate concentration, HIV serostatus, CD4+ T cell (CD4) count and in-hospital mortality. We converted alert, voice, pain, unresponsive (AVPU) and GCS scores to each other as needed.15 To avoid negative numbers and outliers in our data that likely represented data entry errors or spurious values, we included clinical data points in the combined data set if they were positive, within the 1st and 99th percentile of a given variable, and within accepted limits for GCS score (3–15) and oxygen saturation (≤100%). All patients included in the analysis had an outcome recorded for in-hospital mortality and greater than 50% of the following clinical variables: temperature, heart rate, respiratory rate, SBP, DBP, GCS and oxygen saturation.
Missing values
Missing values were handled using the k-nearest neighbours single imputation method.16 In order to determine ORs for clinical as well as laboratory variables, we imputed missing data by subsets. The largest subset consisted of only age, sex, temperature, heart rate, respiratory rate, SBP, DBP, oxygen saturation, GCS score, HIV serostatus, CD4 count (if HIV-infected) and in-hospital mortality (n=5573). The other subset consisted of the same variables with lactate and at least one of WBC count, haemoglobin concentration or platelet concentration (n=1513). All variables except in-hospital mortality and HIV serostatus were imputed.
Descriptive and statistical analyses
We used the χ2test for comparisons of proportions and the Mann-Whitney U test for comparisons of continuous variables to compare baseline characteristics of patients who did or did not die in hospital. We considered a two-sided p value <0.05 significant for all statistical tests. We used R (R Foundation for Statistical Computing, Vienna, Austria) for all analyses and used the Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis (TRIPOD) and Strengthening the Reporting of Observational Studies in Epidemiology checklists in analysing and reporting this study.17
We created logistic regression models for the entire cohort that included clinical data with and without HIV serostatus, and clinical plus laboratory data. We calculated variance inflation factors to determine multicollinearity. We reported ORs and validated these models internally using 10-fold cross-validation (TRIPOD type 1b model study) to estimate the performance on a new sample of observations from the same patient population. The final models were evaluated using log-likelihood ratios. We evaluated the ability of the model to discriminate in-hospital mortality using the area under the receiver operating characteristic curve (AUC) following 10-fold cross-validation.
In order to create an easy-to-use clinical UVA score, we created a point-based scoring system. We used the Bayesian model averaging package in R to select the clinical variables that produced the model with the minimal Bayesian information criterion.18 We then used the rpart package in R to create decision trees for each selected clinical variable on in-hospital mortality. For the decision tree analysis, we upsampled in-hospital mortality to adjust for the class imbalance of mortality. We then determined decision tree splits by selecting the complexity parameter that resulted in the smallest error using 10-fold cross-validation. We built a linear regression of in-hospital mortality on each selected variable at its decision tree split point.19 We divided each beta coefficient in the linear regression model by the smallest absolute value significant beta coefficient. We then assigned a point value for the variable range using the rounded value. We then summed points for each patient to create a UVA score. We compared the decision tree cut-offs derived from the multivariate logistic regression model with decision tree cut-offs that were adjusted after clinical interpretation. We selected the best UVA point-based scoring model after a comparison of the performance of the candidate models.
We compared the performance of the UVA score with MEWS and qSOFA (table 1). MEWS was selected over the National Early Warning Score (NEWS) since supplemental oxygen, a component of NEWS, was not recorded in our pooled data. We assessed the performance of the scores in the original clinical data set, as well as in subsets that included patients with a known HIV serostatus, suspected infection as the cause of admission and patients without a clinical diagnosis. We determined the optimal UVA score cut-off for sensitivity, specificity and positive predictive value (PPV), and determined low, medium and high-risk of mortality groups by creating UVA score cut-offs that divided the study population into three approximately equal groups.
Components of UVA, MEWS and qSOFA scores
Results
The combined study population included 13 cohort studies of adult hospitalised patients from Gabon, Malawi, Sierra Leone, Tanzania, Uganda and Zambia (figure 1).9 13 14 20–29 We also included unpublished hospital data from patients with sepsis in Zambia (n=209) and patients with meningitis in Uganda (n=141) (table 2). This resulted in 5944 patients, a number that was reduced to 5573 patients after applying our data filters (figure 2). Of 5573 patients included in the analysis, 2829 (50.8%) were female, the median (IQR) age was 36 (27–49) years, 2122 (38.1%) were HIV-infected and 996 (17.3%) did not survive to discharge from hospital (table 3).
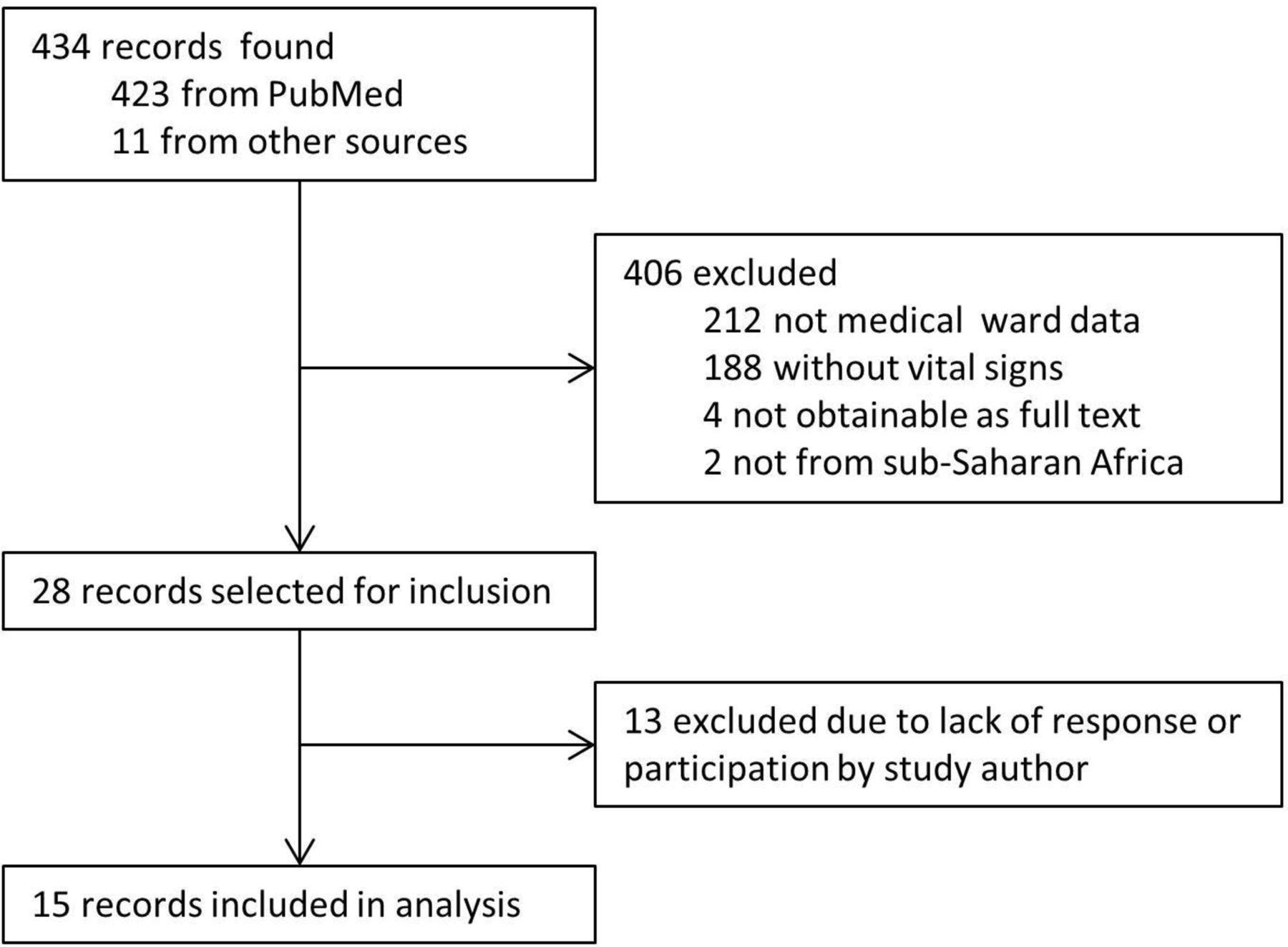
Study selection of pooled hospital-based cohort studies conducted in six African countries from 2009 to 2015 included in the derivation and validation of the universal vital assessment score.

A flow chart of patients pooled from hospital-based cohort studies conducted in six African countries from 2009 to 2015 included in the derivation and validation of the universal vital assessment score.
Hospital-based cohort studies conducted in six African countries from 2009 to 2015 contributing to pooled data for the derivation and validation of the universal vital assessment score
Population characteristics of patients pooled from hospital-based cohort studies conducted in six African countries from 2009 to 2015 according to outcomes
In the multivariable logistic regression model, there was an association between in-hospital mortality and HIV infection (adjusted OR (aOR) 2.9, 95% CI 2.3 to 3.7) and increasing lactate (aOR 1.07, 95% CI 1.02 to 1.12). There was an inverse relationship between in-hospital mortality and temperature (aOR 0.85, 95% CI 0.81 to 0.9), oxygen saturation (aOR 0.98, 95% CI 0.97 to 0.99), GCS score (aOR 0.75, 95% CI 0.73 to 0.78) and haemoglobin concentration (aOR 0.91, 95% CI 0.87 to 0.95) (table 4). The AUC was highest for the clinical data alone model (AUC=0.74, 95% CI 0.72 to 0.76) and the clinical data plus known HIV serostatus model (AUC=0.78, 95% CI 0.76 to 0.79), and lowest for the model that included laboratory values (AUC=0.71, 95% CI 0.68 to 0.74).
Multivariate adjusted odds ratios for in-hospital mortality associated with clinical and laboratory data from patients pooled from hospital-based cohort studies conducted in six African countries from 2009 to 2015
The UVA points-based scoring system was derived from the known HIV serostatus population, which was used because of the high OR for in-hospital mortality for HIV (table 5). The Bayesian model averaging model indicated that temperature, heart rate, respiratory rate, DBP, oxygen saturation, GCS and HIV were the variables that produced the minimal Bayesian information criterion. For the sake of clinical simplicity, we replaced DBP with SBP, the decision tree cut-off for respiratory rate was changed from 34 to 30 breaths/min and the cut-off for GCS was changed from <14 to <15.12 The AUC (95% CI) of the UVA score before the change was 0.75 (0.73 to 0.77), which was not significantly different from the performance of the final UVA score model.
Clinical variables and their cut-offs for the universal vital assessment point-based scoring model
Overall, the UVA score model performed well with an AUC (95% CI) of 0.77 (0.75 to 0.79) and outperformed MEWS (AUC 0.70, 95% CI 0.68 to 0.71) and qSOFA (AUC 0.69, 95% CI 0.67 to 0.72) (table 6). In hospitalised patients without a clinical diagnosis (n=2420), the AUC (95% CI) was 0.74 (0.70 to 0.78).13 14 28 The UVA score performed similarly in patients with clinically suspected infection as the cause of admission (n=3153), with an AUC (95% CI) of 0.75 (0.72 to 0.77).9 20–27 29 In a subset of patients with complete data that did not require imputation (n=1348), the UVA score AUC (95% CI) was 0.77 (0.73 to 0.80). Since pulse oximetry is not always available in resource-limited settings, we removed oxygen saturation from the UVA score and found that the performance remained similar with an AUC (95% CI) of 0.76 (0.74 to 0.78). To fully simulate a real-world application where clinical data are often incomplete, we tested the UVA score in the entire pooled data set with a mortality outcome without data imputation (n=5903) and found that the AUC (95% CI) for the UVA score was 0.75 (0.73 to 0.77) compared with 0.69 (0.67 to 0.70) for MEWS and 0.68 (0.66 to 071) for qSOFA. Finally, we conducted a sensitivity analysis whereby we imputed either an HIV negative or positive serostatus for all missing HIV serostatus values (n=2171) and tested the UVA score. The UVA score AUC (95% CI) was 0.76 (0.75 to 0.78) and 0.76 (0.74 to 0.78) when HIV negative and HIV positive serostatus were imputed, respectively.
A comparison of the performance of UVA, MEWS and qSOFA scores by population subgroups of patients pooled from hospital-based cohort studies conducted in six African countries from 2009 to 2015
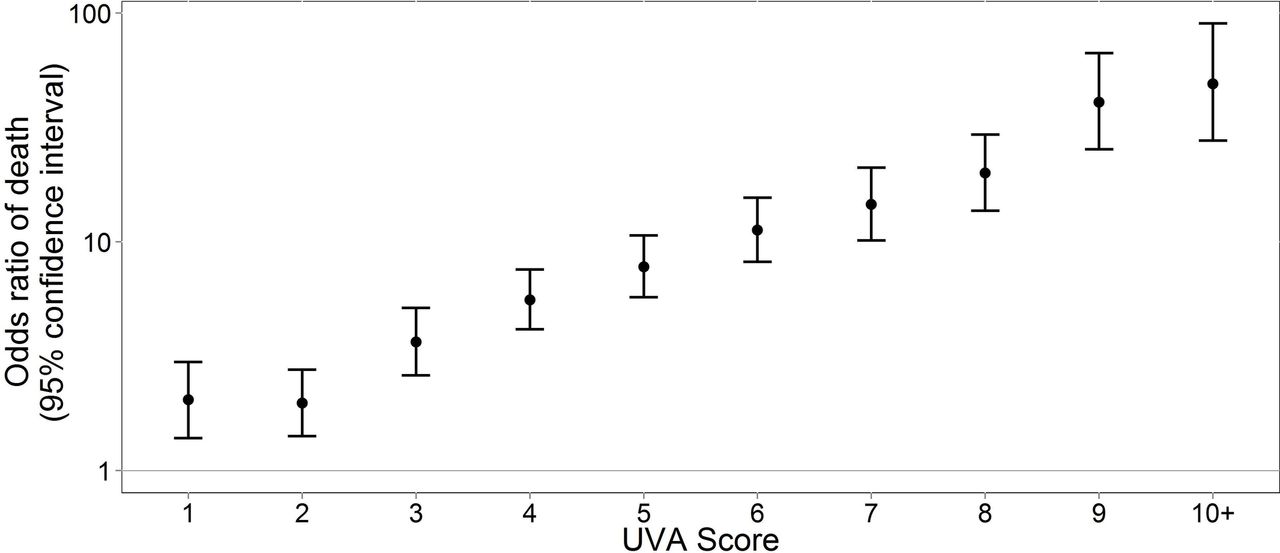
There was a positive relationship between the UVA score and in-hospital mortality, and patients in the medium (UVA score 2–4) and high (UVA score >4) risk groups were 2.76 and 10.41 times more likely to die in hospital compared with the low risk patients (UVA score 0–1), respectively (figures 3 and 4; table 7). A UVA score of 4 provided the best combined sensitivity (72%) and specificity (69%) along with a PPV of 33%. This outperformed both a MEWS score of 5, which had a sensitivity of 72%, a specificity of 58% and a PPV of 26%, and a qSOFA score of 2, which had a sensitivity of 71%, a specificity of 59% and a PPV of 27%.
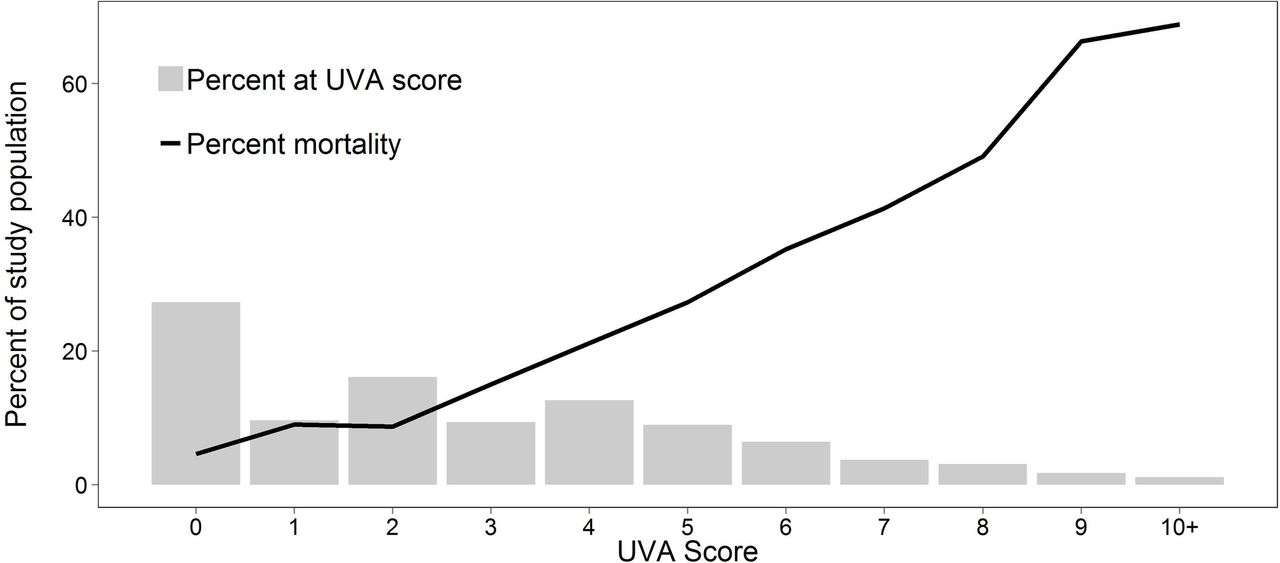
The frequency and associated mortality of universal vital assessment (UVA) scores for all patients pooled from hospital-based cohort studies conducted in six African countries from 2009 to 2015.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Adjusted ORs with 95% CIs for in-hospital mortality associated with universal vital assessment (UVA) score point values for patients pooled from hospital-based cohort studies conducted in six African countries from 2009 to 2015.
Universal vital assessment score risk categories for patients pooled from hospital-based cohort studies conducted in six African countries from 2009 to 2015
Discussion
In this study of the largest pooled cohort of hospitalised adults in SSA, we found that the risk of in-hospital mortality could be easily calculated by a UVA score that incorporated values for temperature, heart rate, respiratory rate, SBP, oxygen saturation (where available), GCS and HIV serostatus. Patients in the medium and high risk groups had 3-fold and 10-fold increased odds of death when compared with patients in the low risk group, respectively. Therefore, clinical application of the UVA score could improve triage decisions in areas where human and material resources are limited, allowing for the greatest efforts to be applied to the most critically ill patients. The UVA score could also be used as a standard measure of mortality risk in future studies.
A MEWS score ≥5 was independently associated with in-hospital mortality in medical and surgical patients in a study in Uganda, and a NEWS score of ≥7 was associated with increased mortality in patients from an ICU in Tanzania.30 31 However, we found that the UVA score performed better than MEWS perhaps due to differences in age, chronic illness, respiratory compromise and HIV prevalence between the derivation cohorts. The importance of severity of illness scores in patients with infection was recently highlighted by the new consensus sepsis-3 definitions that incorporated mortality risk scores including qSOFA that were derived from large data sets from North America and Europe.12 Due to the clinical aspects of the score, qSOFA was also suggested as being useful in resource-limited settings.12 32 However, qSOFA performed poorly in comparison to the UVA score in our cohort including notably in subsets of patients with suspected infection. In contrast, the UVA score had an AUC of 0.77, which was similar to the AUC of qSOFA (0.80) in the original sepsis-3 derivation cohort, and maintained its high performance in patients with suspected infection.12 Accordingly, the UVA score should be prospectively evaluated for use in similar environments to identify patients at highest risk of in-hospital mortality including infected patients with probable sepsis.
Vital sign assessment is the cornerstone of monitoring critically ill patients. In sophisticated ICUs, patients are continually monitored for changes in vital signs that might indicate a change in clinical status. This level of monitoring is generally not possible in resource-limited environments where patients are likely to have vital signs assessed only once per day.33 However, even a single deranged vital sign value signalled clinical deterioration in an ICU in Tanzania and increasing numbers of deranged values increased the odds of mortality.30 A subsequent treatment algorithm based on abnormal vital signs improved targeted clinical responses and mortality outcomes for hypotensive patients.34 Since the UVA score provides a vital assessment across six clinical variables plus HIV serostatus, the information gathered is more nuanced and therefore provides additional clinical information about a patient's risk of death. It is possible that iterative evaluations of the UVA score in hospitalised patients could guide therapeutic interventions.
Although fever suggests infection, we found an inverse relationship between temperature and mortality in this cohort of patients. This finding is consistent with other observational studies that showed that hypothermia is associated with poor outcomes in critically ill patients. For example, in one ICU study, patients with septic shock had a higher mortality if they were hypothermic than if they were febrile.35 In another ICU study, there was an increase in mortality rate with increasing severity of hypothermia, but fever at presentation was not associated with mortality.36 Additionally, severe hypothermia increased the risk of developing ICU-acquired infection in a study of ICU patients in France.37 Meanwhile, fever may afford host protection through increased immune function from production of heat shock proteins, inhibition of micro-organism growth and increased antimicrobial effectiveness.38 In patients with sepsis in Uganda, a temperature <35.5°C was associated with mortality, but a temperature of >37.5°C was not.9
Oxygen saturation is also a component of the UVA score. In a study from Rwanda, the prevalence of hypoxaemia defined as oxygen saturation <90% in ward patients was 12% with an associated mortality of 49%, which was similar to the 47% patient mortality in the ICU.39 Given the high mortality associated with hypoxaemia, particularly in patients with sepsis, it is important to identify patients with low oxygen saturation.21 Fortunately, pulse oximetry devices are increasingly available in resource-limited settings through such efforts as the Global Pulse Oximetry Project.40 Acknowledging that pulse oximetry remains unavailable in some resource-limited settings, we determined that the UVA score performed well even without including oxygen saturation. However, when feasible, measuring a patient's oxygen saturation may provide additional information about their mortality risk and prompt administration of supplemental oxygen where it is available.
Decreasing GCS was a strong predictor of in-hospital mortality. A GCS less than 15 was assigned the highest point value in the UVA score and was sufficient to place a patient in at least a medium mortality risk category. This is congruent with prior studies in resource-rich and resource-limited settings. AVPU and GCS scores were included in MEWS and qSOFA, which are in use in North America and Europe.11 12 A poor Karnofsky Performance Score, a measure of functional status, was also strongly associated with early and late mortality in septic patients hospitalised in Uganda.24 Similarly in another study from Uganda, patients who were able to ambulate on admission had a 60-day mortality of 5% compared with 25% if they had an unstable gait, or 50% if they were bedridden.41 In Ugandan septic patients, GCS and mid-upper arm circumference were independently associated with mortality even if patients were successfully resuscitated to lactate clearance in the first 6 hours of treatment.20 Our findings in this study further support that any change in level of consciousness or functional status should prompt evaluation and monitoring in patients admitted to hospital in SSA.
Adding HIV serostatus considerably improved the performance of the clinical logistic regression model and was also a feature of the UVA score. Although there is a link between HIV infection and chronic cardiovascular diseases, data regarding the role of HIV infection in mediating the physiological response to acute illness including infection are scant.42 Therefore, we are not aware of a direct connection between HIV infection and vital sign changes during an acute illness. It is more likely that the importance of HIV infection as a predictor of mortality reflects underlying immunosuppression and chronic illness. Unfortunately, despite increasing availability of antiretroviral therapy throughout the time period of our pooled data (2009–2015), CD4 counts have remained low for HIV-infected patients in SSA at the time of presentation to care and treatment.43
In our study, the median CD4 count was very low for all patients included in the HIV-infected regression model, making it difficult to use CD4 count to discriminate between those who survived or died as they were likely to have a similarly high risk for opportunistic infections such as tuberculosis and associated mortality. Several studies from SSA have identified disseminated tuberculosis as a leading cause of infection and mortality in hospitalised HIV-infected patients.44 Wasting, as measured by a reduced mid-upper arm circumference, is also associated with both HIV infection and mortality in SSA, but was not fully captured in our pooled data.20 Hospitalised HIV-infected patients are also likely to have low functional status and be less likely to be ambulatory.24 41 Taken together, the association between HIV infection, disseminated tuberculosis, wasting and low functional status likely contributes to a high prevalence of mortality in hospitalised patients in SSA.
We envision the UVA score being useful both as a screening tool for patients admitted to hospital and as a tool to identify patients on the ward who are deteriorating and may require additional investigation and treatment. A UVA score of 4 provided optimal sensitivity, specificity and PPV for mortality, but we expect clinicians will determine the UVA score threshold that works best for their needs and patient population. For example, the UVA score PPV will change depending on the prevalence of mortality in the patient population. Since the UVA score was built on admission data, prospective validation studies should incorporate repeated measures to determine how UVA score trends predict mortality. Thereafter, depending on institutional resources, prospective evaluation of UVA score-based interventions such as additional diagnostic testing, increased monitoring or treatment algorithms could take the form of a simple before-and-after study or ideally more sophisticated study designs, including a randomised cluster study which can account for confounders and control for the effect of time.45 A mixed-methods approach that includes a quantitative and qualitative data analysis could also be useful to evaluate adherence to clinical interventions and the processes of implementation of an EWS that are unique to settings in SSA.46
There are several limitations to this study, including its retrospective design. Additionally, we only conducted our search for English-language papers in PubMed, so it is possible we missed additional relevant data due to selection or publication bias. We combined heterogeneous data from studies conducted over a long period of time with different enrolment criteria and patient treatments, and only included admission data in order to develop a UVA score, which may have led to case ascertainment bias. Larger data sets from individual studies may have biased the results of our analyses of the complete cohort. However, creating a reliable UVA score from different populations recruited in different settings throughout SSA could be considered a strength of this work. Data were not complete for each data set, which could have also biased our results. Since omitting patients with missing variables from our analysis would reduce our sample size and power, we imputed missing values. Differences between sites with large amounts of missing data, which required imputation, were therefore diminished. Many of the patients in this cohort did not have a recorded clinical diagnosis, so it is possible that the performance of the UVA score may vary in different clinical subsets. Importantly, the UVA score performed well in a large subset of patients with suspected infection, suggesting it is useful in identifying patients with sepsis. Finally, future studies are required to determine the generalisability of the UVA score.
Conclusion
We derived and internally validated a UVA score to assist clinicians in risk-stratifying patients for in-hospital mortality in SSA. The UVA score outperformed MEWS and qSOFA in our pooled data set but should be prospectively studied and externally validated in similar environments.32 The UVA score could assist clinicians in making triage decisions about the appropriate level of care required for a patient. It may also help clinicians identify patients at moderate to high risk of death that could benefit from further diagnostic testing to determine underlying causes of illness or infection. Additionally, the UVA score may be useful in standardising risk of death of patients in future studies. Such future studies could employ the UVA score iteratively in order to test its ability to guide daily risk of mortality and clinical decisions, and assess impact on patient outcomes.
Acknowledgments
We thank Karen Knight for assistance with our literature search, and Eric Houpt, James Platts-Mills and Elizabeth Rogawski for their critical review of the manuscript.
References
Footnotes
Contributors CCM and LEB designed the study and analysis. SAA, AA, BA, MA, TB, PB, JAC, MPG, MAMH, STJ, ODJ, JK, SL, AM, MO, MPR, JR, JS, WMS, RS and IW all contributed data. CCM, RH, KJS and LEB collected data and prepared the data sets. CCM, RH, KJS, JA and LEB analysed the data. CCM and RH drafted the manuscript. CCM and LEB reviewed, edited and revised the manuscript, as well as supervised all the processes. All authors interpreted data and revised the manuscript critically for intellectual content. Finally, all the authors read and approved the final version.
Funding Data collection in Lusaka, Zambia, was supported by the National Institutes of Health Office of the Director and Fogarty International Center through the International Clinical Research Fellows Program at Vanderbilt University (R24 TW007988 to BA). Data collection in Moshi, Tanzania, was supported by the International Studies on AIDS Associated Co-infections, US National Institutes of Health (U01 AI062563 to JAC). RH received a University of Virginia Harrison Undergraduate Research Award to support this work. Funding for studies in Masaka, Mbarara and Kampala, Uganda, was provided to CCM, SAA, AA, MA, PB, STJ, AM, WMS and RS by the Pfizer Initiative in International Health and the Center for Global Health at the University of Virginia. This initiative was conceived to fund global infectious disease research and exchange programmes between postdoctoral fellows and students from the University of Virginia and several international partners to conduct research on global health issues. The major purpose of this programme was to foster and enhance bidirectional research training. An independent board at the University of Virginia determined the research proposals that were funded. Pfizer provided funds to promote the initiative but had no role in the planning, execution or analysis of research protocols, including the study described in this article.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.