Article Text

Abstract
Introduction Improving health systems performance, especially in low-resource settings facing complex disease burdens, can improve population health. Specifically, the efficiency and effectiveness of supply chains and procurement processes for pharmaceuticals, vaccines and other health products has important implications for health system performance. Pharmaceuticals, vaccines and other health products make up a large share of total health expenditure in low-income and middle-income countries (LMICs), and they are critical for delivering health services. Therefore, programmes which achieve cost savings on these expenditures may help improve a health system's efficiency, whereas programmes that increase availability of health products may improve a health system's effectiveness. This systematic review investigates whether changes to supply chains and procurement processes can achieve cost savings and/or improve the availability of drugs in LMICs.
Methods Using the PRISMA guidelines for systematic reviews, we searched PubMed, Embase, CINAHL and the Health Economic Evaluation Database to identify.
Results We identified 1264 articles, of which 38 were included in our study. We found evidence that centralised procurement and tendering can achieve direct cost savings, while supply chain management programmes can reduce drug stock outs and increase drug availability for populations.
Conclusions This research identifies a broad set of programmes which can improve the ways that health systems purchase and delivery health products. On the basis of this evidence, policymakers and programme managers should examine the root causes of inefficiencies in pharmaceutical supply chain and procurement processes in order to determine how best to improve health systems performance in their specific contexts.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known about this topic?
Pharmaceuticals, vaccines and other health products are an important component of a strong health system. Procurement processes and supply chains are critical for purchasing and delivering these products.
What are the new findings?
Centralising procurement for health products can yield cost savings across many contexts.
Efforts to improve supply chain management can increase the availability of health products in low-income and middle-income countries, especially by reducing stock outs. However, there is no single approach to improving supply chains that should be used in all contexts.
Recommendations for policy
Policymakers and practitioners should consider the root causes of programmatic challenges to purchasing and distributing health products in their context and identify specific interventions that can strengthen these processes.
Introduction
Health systems performance along key outputs, such as equity, efficiency, effectiveness and responsiveness, has important implications for population health.1 ,2 Specifically, maximising ‘technical efficiency’ of the health system, or the amount of outputs generated by a given cost (or other input), can increase total fiscal space for health in a country, thereby freeing up resources for additional programmes or activities.1–3 Improving the effectiveness of the health system in its delivery of services can improve population health and build trust in the health system.
Pharmaceuticals, vaccines and other health products constitute a key component of health systems by providing important treatments to populations. Pharmaceutical health expenditures make up a large share of health spending: in low-income and middle-income countries (LMICs), the total pharmaceutical expenditure as a share of total health expenditure in 2006 varied from 7.7% to 67.6%.4 Access to pharmaceuticals, such as essential medicines, remains a challenge, with only 61.5% of select essential medicines available in select LMICs.5
Improved procurement and supply chain management can reduce costs and address the problem of supply shortages,6 which adversely affect health outcomes by interrupting treatment and, in the case of certain drugs, possibly leading to drug resistance. In LMICs, where procurement and supply chain management tend to be complex and fragmented, these types of improvements can be critical for strengthening the health system.7 Changes to the procurement and supply chain processes include centralising or decentralising purchasing, improving data systems to monitor and inform purchasing (eg, early-warning systems), improving infrastructure or processes along the supply chain to reduce wastage and altering the methods for financing purchases, among others.
Given the high spending on pharmaceuticals, vaccines and other health commodities and their importance for population health outcomes, this systematic review aims to answer two questions regarding the performance of a health system: (1) do efforts to improve supply chains and procurement processes yield cost savings for health systems in LMICs, and (2) do these efforts lead to increased availability of drugs, vaccines or other health commodities in LMICs? We use these two criteria as evidence for changes to health system performance for several reasons. Both metrics are objective and captured through routine data collection in the management of many health systems. Any change in spend without a commensurate change in the quantity or quality of products purchased will indicate a change in the technical efficiency of the health system. Changes in supply availability, as measured by a reduction in stock outs or several other measures, is a useful indicator of whether health facilities (eg, hospitals, clinics and pharmacies) can effectively deliver certain services to patients.
To the best of our knowledge, no systematic review has attempted to answer these questions, which are critical for policymakers and programme managers looking to improve health systems performance and maximise population health outcomes.
Methods
This systematic review follows the criteria and methodology described in the PRISMA guidelines on systematic reviews.8
Search process and criteria
This search relied on an internal protocol developed by GS and RA. The protocol was not registered externally. We searched PubMed, Embase, CINAHL and the Health Economic Evaluation Database. The main search that was conducted on 22 March 2016 was as follows (for PubMed), with an additional search term for LMICs, and any publication from before that date was eligible for our review:
(“Materials Management, Hospital”[Mesh] OR “Pharmaceutical Preparations/supply and distribution”[Mesh] OR materials management[tiab] OR (supply chain*[tiab] AND (redesign*[tiab] OR improv*[tiab] OR oversight[tiab] OR management[tiab])) OR ((purchas*[tiab] OR procure*[tiab]) AND (“Pharmaceutical Preparations”[Mesh] OR drug*[tiab] OR medicine*[tiab] OR pharmaceutical*[tiab])))
AND
(“Cost Savings”[mesh] OR “Cost Benefit Analysis”[mesh] OR “Efficiency”[mesh] OR cost[tiab] OR costs[tiab] OR efficienc*[tiab] OR economies of scale[tiab] OR economies of scope[tiab] OR productivity[tiab] OR stock out*[tiab] OR stockout*[tiab] OR out of stock[tiab] OR drug suppl*[tiab]).
We also conducted several additional searches based on a review of citation lists from relevant publications and based on recommendations from public health researchers.
Study selection and eligibility criteria
After conducting our search, all titles were reviewed for relevance. After excluding irrelevant titles, we read all abstracts and, when appropriate, full articles to determine the relevance of the article for our research question and the availability of relevant data for inclusion. In order to be included in the study, the publication had to meet the following criteria:
Report on an effort, such as a program or policy intervention, aiming to improve or modify the supply chain or procurement processes for pharmaceuticals, vaccines or other health products. (For the purpose of simplicity, we often refer to all commodities under consideration in this review simply as products or health products.)
Report on the impact of the programme or policy on costs to the health system or availability of pharmaceuticals, vaccines or other health products. Cost comparisons could be reported using any cost ratio or change in cost figure and could report costs from the provider or patient perspective. Availability of products could be reported as the frequency of stock outs, or an indirect indicator for availability, such as number of emergency orders.
Report results from an actual intervention, rather than a computer model or simulation.
Report results from a low-income or middle-income country.
Be original research about an intervention published in a peer-reviewed format (as opposed to an editorial, literature review, opinion piece, interview, etc).
Have a complete article available (as opposed to just an abstract).
Be published in English.
Data collection process
In order to extract data for this review, we piloted an Excel-based data collection tool that was used to capture results from a preliminary search, the results of which were presented at the Harvard Ministerial Leadership Program in the summer of 2016. On the basis of our experience with this initial process, we modified the tool accordingly and finalised a tool which collected the following information: author, year, title, publication, abstract, country, continent, geographic level of intervention (subnational, national or international), description of the intervention, relevant outcome metric and result on relevant outcome metric. The relevant outcome metric had to involve some comparison or change in costs either from the patient or provider perspective in quantitative terms or change in product availability, and the summary measures for the review follow from these outcome metrics. Results which did not provide evidence of cost changes, such as baseline costing studies, were excluded. GS conducted a first review of all references in the search, and the list was reviewed by all coauthors in order to identify missing references or references which had been improperly included.
Risk of bias
At the level of individual studies, there is the possibility that authors are more likely to report positive outcomes (eg, programmes that resulted in cost savings or reduced stock outs) than negative outcomes. In addition, because many references describe programmatic activities that do not use experimental designs, it may be difficult to obtain the statistical significance of quantitative findings. Nonetheless, we have chosen to include all studies that report changes in costs as a result of a relevant programme in order to demonstrate to policymakers the range of potential impacts that supply chain and procurement projects can have.
Across all studies, there is also a risk that authors have publication bias or only report selective outcomes for their programmes. In addition, there is a risk that the literature under-reports findings from these kinds of programmes in general, since the peer-review process may favour rigorous experimental designs, which are not necessarily appropriate for programmatic health systems improvements, over other types of programme evaluations.
Results
Study selection
We reviewed 1264 articles and identified 25 references which specified the cost implications from changing supply chain or procurement practices—8 from Latin America, 5 from the Middle East/North Africa, 5 from Sub-Saharan Africa, 4 from Asia, 1 from Eastern Europe, 1 focused on a programme on multiple continents and 1 reporting separate results from programmes in Latin America and the Middle East. Of these 25 references, 9 reported result from a nationwide intervention, 10 from an intervention within parts of a single nation (eg, a city or region) and 6 from an intervention that spanned multiple countries. We also identified 15 studies reporting a change in availability of pharmaceuticals, vaccines or other health products as a result of these types of programmes—12 from Sub-Saharan Africa, 2 from Asia and 1 from Latin America. (Of the latter 15 studies, 2 were also included in the 25 reporting cost implications, making for a total of 38 studies included in the review.) See figure 1 for the study selection for inclusion in this systematic review.
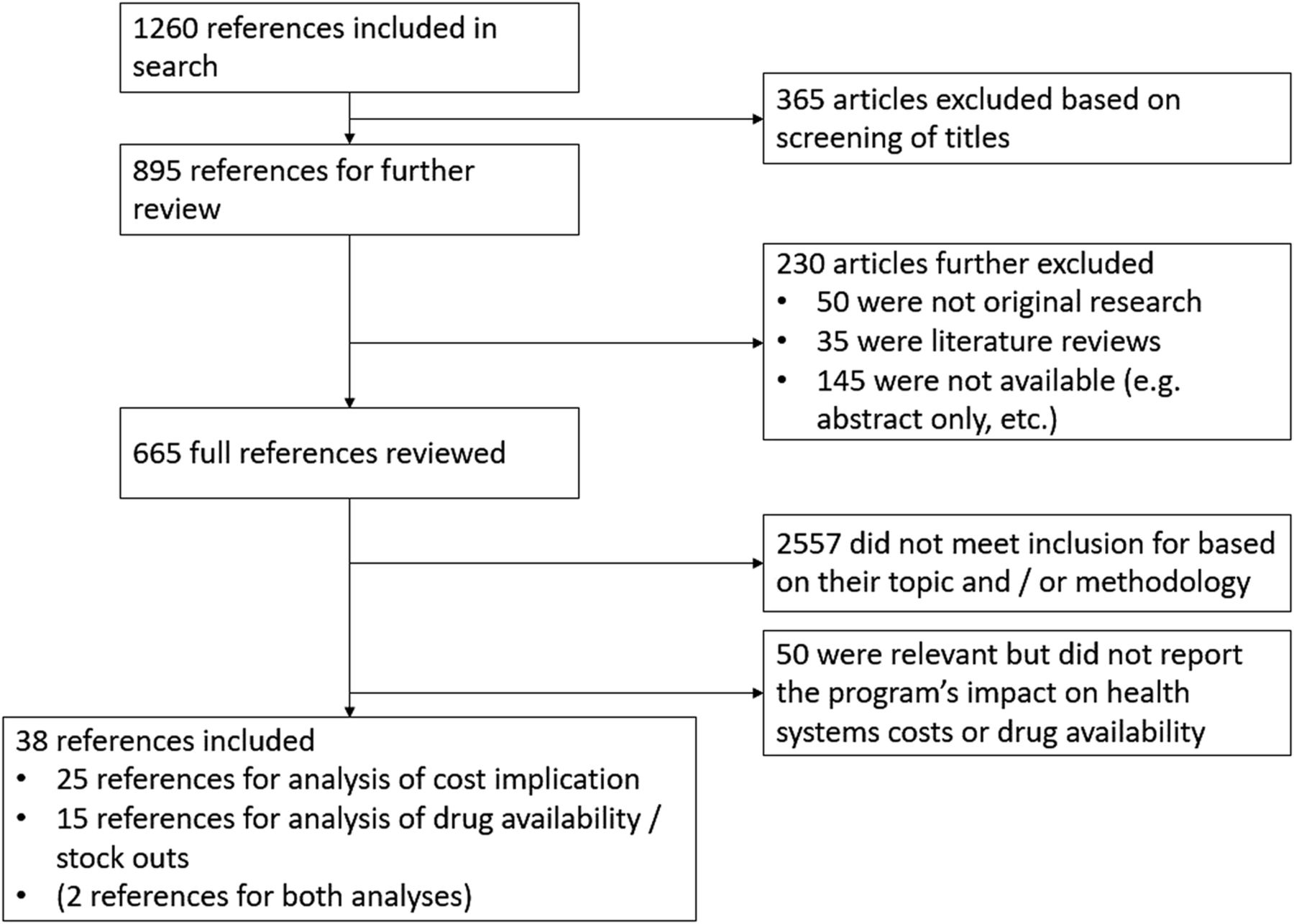
{kind=link}
Study selection for inclusion in systematic review.
Of the 25 references analysing the cost implications of supply chain or procurement changes, 23 found a reduction in costs to the health system. Of these, 12 focused on cost savings from some form of centralised procurement or tendering process. The other references which demonstrated cost savings included supply chain management projects, comprehensive drug policies at the national, district or city level and other types of interventions. Of the two references that did not exclusively demonstrate savings, one reference analysed centralised procurement processes in multiple Middle Eastern countries and found that some countries achieved cost savings compared to local procurement, while other countries experienced cost increases.9 One reference that studied the impact of requiring bioequivalence studies as part of the drug procurement process found that the programme resulted in price increases due to an increased failure rate on these studies.10
Of the 15 references analysing changes in health product availability, 13 found improvements, and 8 of these were from supply chain management programmes. One reference about supply chain management programme in Tanzania found a reduction in unaccounted antimalarials and antihelminthics, but an increase in stock outs for oral rehydration salts (ORS).11 One reference about a centralised procurement process for antimalarials in Kenya found that a delay in the process, and the awarding of the tender to a relatively new, unknown company, resulted in a nationwide increase in stock outs.12
The full list of references meeting inclusion criteria can be found in tables 1 and 2.
Full list of references with cost implications from programmes
Full list of references with drug availability implications from programmes
Comprehensive drug system policies
Three references described comprehensive policies and programmes to improve drug procurement and supply chains at either the national or municipal level. In Brazil, a series of policies by the Ministry of Health aimed to promote the use of multisource drugs (those which can be purchased from multiple manufacturers or distributors), development of the national pharmaceutical industry and aggressive price bargaining for select drugs, such as antiretroviral treatments (ARVs), under the provisions in the TRIPS agreement.13 These initiatives resulted in a 79% reduction in the annual cost per person of ARVs in 6 years (from 1997 to 2003).
In China, the National Essential Medicines Scheme, established in 2009 as part of broader health sector reform, included four components: a National Essential Drugs List, a zero-mark-up policy, reimbursement for drugs on the Essential Drugs List and public procurement of drugs.14 An evaluation of this scheme in three provinces found that it resulted in a 17.5% reduction in cost of drugs needed to treat pneumonia or bronchitis (p<0.05) and a 48.4% reduction in cost of drugs needed to treat gastroenteritis (statistical significance not reported).
In Delhi, India, a 1997 comprehensive drug policy included the development of an Essential Drugs List, a central pooled procurement system and programmatic activities to promote rational drug use.15 This policy was found to result in 30% savings on the cost of drugs to the Government of Delhi and to increase the availability of key drugs from 40% to 70% before the policy's implementation to >90% after its implementation.
Centralised procurement and tendering processes
We found the most references demonstrating cost savings from centralised procurement and tendering processes. These references included joint procurement across multiple countries, including the Gulf Cooperation Council (GCC) of Bahrain, Kuwait, Oman, Qatar, Saudi Arabia and UAE,16 ,17 the PAHO Expanded Program on Immunisation (EPI) which included many Latin American countries16 and the Eastern Caribbean Drug Service (ECDS) which serviced nine small Caribbean countries.18 We found references from two countries—Jordan and Mexico—that described centralised procurement at the national level. In Jordan, a Joint Procurement Directorate bids for drugs across four different government agencies, and this programme achieved 5.2–17% cost savings on drugs procured.19 ,20 In Mexico, a Commission to purchase ARVs and other drugs established in 2008 achieved cost savings of US$52.1 million—US$121.8 million in its first 4 years, although the prices for ARVs were still above those of other upper-middle income countries.21–23 At the subnational level, references found cost savings from an Intermunicipal Health Consortium which coordinated procurement for multiple municipalities in Brazil24 and centralised procurement at hospitals or hospital systems in Serbia25 and Brazil.26 No references found that centralised procurement reduced stock outs or improved availability of health products.
Supply chain/cold chain management
Three references identified cost savings from efforts to improve supply chain management. Of these three references, one programme in Nigeria aimed at strengthening laboratory services in hospitals reduced the costs of conducting laboratory tests by increasing the total volume of tests and then purchasing reagents in bulk at reduced costs. Another reference found that a modification of methods to store and transport vaccines in Tunisia resulted in a 20.16% reduction in energy costs for vaccine storage and distribution. A third reference found that transitioning to a vendor-managed inventory (VMI) system, in which customers automatically send inventory information to the supplier who then creates and fills order to replenish the inventory, resulted in an increase in unit costs per vaccine, but reductions in total logistics costs and unopened phial wastage led to an 18% reduction in overall programme costs.27
An additional eight studies found improvements in availability of health products from supply chain management programmes, suggesting that these initiatives can improve health systems performance by ensuring access to products for populations. For example, certain references documented programmes to improve data systems or processes to track and monitor drug inventory, including an mHealth application,28 improved human-related processes and meetings relating to the supply chain,29 ,30 and a web-based stock management system for rural clinics in Haiti.31 Three references identified programmes that changed the process for ordering drugs: one programme in Senegal used an informed Push Model, in which projected demand dictates quantities of drug orders, to reduce stock outs for contraceptives,32 whereas a Pull Model, which uses clinic or customer demand to inform drug orders, improved drug availability in Tanzania and Uganda.11 ,33
Other types of programmes
In addition to the types of programmes listed above, we found limited evidence for the impact of a number of other types of initiatives related to supply chain management or procurement on health systems costs and availability of health products. Three references described revolving drug funds (RDFs), which maintain drug inventory by beginning with an initial donation or free contribution of drugs, and then maintaining inventory by selling these drugs at cost (plus a mark-up in some cases) and then purchasing replacement drugs. One reference found that in South Sudan, drug prices were 40% cheaper in the RDF than those purchased by the Central Medical Supplies Public Organisation, and two references found increased availability of vaccines or essential drugs in RDFs in Guinea34 and Nigeria.35 Two references reported on the Affordable Medicines Facility-malaria (AMFm), which provided subsidies to manufacturers of artemisinin-based combination therapies (ACT) at the global level, and which resulted in price reductions for ACTs to consumers36 and increased availability of ACTs in various countries in Sub-Saharan Africa.36 ,37 Other references reported cost savings from public procurement of drugs (compared to private sector only) in Mali,38 the implementation of an IT system to purchase hospital supplies in India39 and the direct purchase of drugs from commercial suppliers rather than through government channels in Sierra Leone.40
Discussion
With this review, we aimed to synthesise the evidence on whether programmes to improve supply chain and procurement can achieve cost savings or improve health product availability in LMICs. Our findings indicate that multiple approaches to strengthening purchasing and supply systems in LMICs can improve the system's performance. These findings have significant implications for policymakers, discussed below. They also have limitations, discussed in the next section.
Opportunities to improve procurement and supply exist at every level of the health system
The breadth of findings in this review suggests that governments and other organisations can take multiple approaches to improving the procurement and delivery of health products. On the one end of the spectrum, the AMFm represents an example of a comprehensive, international agreement that built on existing global governance structures to improve availability of antimalarials. Our review also included examples of national programmes to improve drug supply, such as those in China, Brazil and Mexico, and initiatives all the way down to the clinic and community levels. These findings suggest that there is no ‘one-size-fits-all’ approach to improving the performance of health systems and the provision of health products. Therefore, we believe that policymakers should use a problem-driven approach to understanding and addressing the root causes of problems in their drug procurement and supply systems.
Different supply chain management systems can yield similar results in different contexts
Following from the point above, it is worth noting that our review identified a variety of techniques to strengthen supply chains in different countries, and, in some cases, these approaches conflicted with each other. Indeed, our review identified references that demonstrated improved drug availability from ‘pull’ and ‘push’ systems, which take opposite approaches in how to determine drug order quantities. Similarly, some references focused on using technology to improve inventory management, while others focused on improving teamwork and the human elements of supply chain management, and both types of initiatives achieved positives results. These findings further reinforce our point that policymakers and programme managers should examine the specific context of their systems and identify root causes of their inefficiencies in order to determine how to improve them.
Centralised procurement has the potential to achieve cost savings across many contexts
In contrast to the first two points, which emphasise that different contexts require different types of interventions in order to achieve improvements in health system performance, we found that centralised procurement/tendering achieved cost savings in the Middle East, Brazil, the Caribbean, Mexico, other parts of Latin America and several countries in Asia and Africa. It also achieved cost savings when centralising procurement across countries, within a single country, or across multiple municipalities or health centres. Although centralised procurement is certainly not a panacea for improving health systems efficiency, these findings suggest that by creating economies of scale and improved purchasing power, centralised procurement and tendering can reduce health systems costs in many contexts. This is a particularly noteworthy finding since many countries are moving to decentralise their health systems.41 ,42
Limitations of the evidence, risks of bias and directions for future research
This systematic review has several limitations that are worth noting. First, the studies included in this review used many different types of metrics to quantify the impact of supply chain and procurement programmes on health systems costs and product availability. Because of this situation, it is difficult to compare or synthesise findings across studies. When analysing impacts on health systems costs, references used metrics such as total absolute cost savings, cost savings as a percentage of spend in previous years and percentage of individual products which had lower costs from 1 year to another. They also use costs to the health system and to the patient; changes to costs to the patient may not actually reflect a change to health systems efficiency. Further, since efficiency is achieved by a reduction in costs without a commensurate reduction in (quality of) outputs, or vice versa, but many studies only report total cost savings, it is difficult to determine conclusively that these cost savings result in a true efficiency improvement to the health system. (On the other hand, studies which demonstrate a reduction in cost per drug or cost per person treated do likely reflect an improvement in efficiency.)
Second, because these findings are context-specific, one cannot predict the impact that a specific programme reported in this review would have in another context. Although the body of evidence presented in this study suggests that health systems can improve their performance by undertaking efforts to improve supply chain and procurement processes, policymakers and programme managers must keep in mind that the most effective programmes tend to achieve improvements when they address the root causes of inefficiencies in the system, so a programme that works in one context may fail in another.
Third, reductions in costs and improvements in drug availability both improve health system performance, but in different ways. As already discussed, cost reductions can serve as a proxy indicator for efficiency improvements. On the other hand, increases in availability of products can improve the effectiveness of health facilities providing services. Although stock out reductions may result in indirect cost savings (eg, by reducing how often patients default from drug treatment), they may also increase costs simply because the health system has to purchase and provide more drugs (paid for either by institutional payers or patients). Weighing the importance of reducing costs versus increasing the availability of health products is the job of practitioners and cannot be determined by this review.
Fourth, even though we find that many programmes either reduce costs or improve drug availability, these interventions have other shortcomings which limit their effectiveness as interventions to improve health systems performance. For example, implementation of RDFs has had many challenges, such as fund decapitalisation due to unanticipated changes in procurement costs, inflation or exchange rates, failure to recover costs and other issues.43 Centralised or pooled procurement may require increased coordination and governance arrangements among purchasers, and it may be important to avoid relying exclusively on a single supplier to ensure that alternative supplies are available, especially in the case of emergencies.44 VMI can lead to challenges, inter alia, integrating technologies between customer and supplier and dependency on the supplier for monitoring inventory.45 Describing the advantages and limitations of each of these types of programmes is beyond the scope of this review. We recommend that practitioners consult a reference text, such MDS-3: Managing Access to Medicines and Health Technologies, for detailed information on the logistical considerations for different types of supply chain and procurement programmes.46
Finally, as discussed already, biases in the publication of individual studies limit the generalisability of study. In particular, there are very few studies which reported negative outcomes from supply chain or procurement improvement programmes; our experience working in health systems in LMICs suggests that it is very unlikely that so few programmes fail. Therefore, the results of this study are likely biased by researchers tending only to publish positive outcomes from these types of initiatives. Nonetheless, the research still provides compelling evidence that these types of programmes can help improve health systems performance when implemented properly.
In the future, we recommend that researchers, programme planners and policymakers should work together to better understand which types of supply chain and procurement programmes can improve health systems performance in which types of contexts. It is also important to understand better the key barriers and enablers of success for these types of programmes. Health systems experts should also identify a common set of indicators and metrics for measuring improvements in supply chains in order to standardise reporting and simplify comparisons across programmes. These may include the metrics used in this research, or other key indicators such as the frequency of counterfeit medicines and the frequency of medicine expirations.
Conclusions
This systematic review aimed to determine whether efforts to improve procurement and supply chains for pharmaceuticals, vaccines and other health products can achieve cost savings and improve drug availability in LMICs. Our findings indicate that many different types of initiatives can achieve these improvements. While the evidence suggests that centralised procurement has the potential to improve efficiency across multiple contexts, other efforts require more context-specific implementation.
Acknowledgments
The authors thank Michael Sinclair and Brian Dugan from the Harvard Ministerial Leadership Program for their support in preparation of this report. The authors thank Paul Bain at the Harvard Library for help developing the search strategy for this review.
References
Footnotes
Handling editor Seye Abimbola.
Contributors GS and RA jointly conceived of the concept for this paper. GS designed the search methodology with a Harvard librarian, screened all references and drafted the initial manuscript. RA checked the final list of references included. GS and RA revised subsequent versions of the manuscript.
Funding An original draft of this paper was commissioned by the Harvard Ministerial Leadership Program, a joint initiative of the Harvard TH Chan School of Public Health, Harvard Kennedy School of Government and the Harvard Graduate School of Education in collaboration with Big Win Philanthropy and with the support of the Bill and Melinda Gates Foundation, Bloomberg Philanthropies, the GE Foundation and the Rockefeller Foundation.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.