Article Text

Abstract
Introduction In high-income countries, a reduced clinical threshold for obstetric interventions such as labour induction (LI) and prelabour caesarean delivery (PLCD) has played a substantial role in increasing rates of late preterm births. However, the association between provider-initiated delivery and perinatal outcomes have not been studied in a multicountry setting including low-income and middle-income countries.
Methods 286 hospitals in 29 countries participated in the WHO Multi-Country Survey on Maternal and Newborn Health and yielded 2 52 198 singleton births of at least 34 weeks in 2010–2011. We used an ecological analysis based on generalised estimating equations under multilevel logistic regression to estimate associations between hospital rates of PLCD and LI with rates of late preterm birth (34–36 weeks), stillbirth and intrahospital early neonatal death, in relation to country development based on the Human Development Index (HDI).
Results Rates of LI were higher in hospitals from very high-HDI (median 10.9%) and high-HDI (11.2%) countries compared with medium-HDI (4.0%) or low-HDI (3.8%) countries. Rates of PLCD were by far the lowest in low-HDI countries compared with countries in the other three categories (5.1% vs 12.0%–17.9%). Higher rates of PLCD were associated with lower perinatal death rates (OR 0.87 (0.79, 0.95) per 5% increase in PLCD) and non-significantly with late preterm birth (1.04 (0.98, 1.10)) regardless of country development. LI rates were positively associated with late preterm birth (1.04 (1.01, 1.06)) regardless of country development and with perinatal death (1.06 (0.98, 1.15)) only in middle-HDI and low- HDI countries.
Conclusion PLCD was associated with reduced perinatal mortality and non-significantly with increased late preterm birth. LI was associated with increases in both late preterm birth and, in less-developed countries, perinatal mortality. Efforts to provide sufficient, but avoid excessive, access to provider-initiated delivery should be tailored to the local context.
- Maternal health
- Obstetrics
- Cross-sectional survey
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known about this topic?
Four recent reviews have independently reported that over the past five to 15 years, caesarean delivery (CD) and preterm birth rates have increased, while stillbirth and neonatal death rates have decreased.
Ecological studies suggest that adverse neonatal outcomes decline with higher CD rates only up to a certain threshold.
We are aware of no systematic reviews on global estimates or trends in prelabour caesarean delivery (PLCD) or labour induction (LI).
What are the new findings?
In the context of 29 countries of varying Human Development Indices (HDIs), hospitals with higher LI rates had higher risks of late preterm birth and (in low-HDI and medium-HDI countries) of perinatal death.
Those with higher rates of PLCD had lower perinatal mortality rates.
Recommendations for policy
Routine labour induction after 41 weeks in high-income settings is known to reduce the risk of stillbirth and perinatal death, but when performed earlier in gestation may increase the risk of late preterm birth and, in low and middle-income settings, of perinatal death.
The evidence concerning PLCD suggests a trade-off in less-developed settings between a reduced risk of perinatal death and a higher risk of late preterm birth.
Introduction
Over the last several decades, global stillbirth1 and neonatal mortality2–4 rates have declined, while preterm birth rates have remained stable or have even increased in many countries.5 It is estimated that perinatal mortality rates have reduced by over a quarter over the past 15 years, with global estimates for 2015 of 18.4 stillbirths per 1000 total births1 and 14.0 early neonatal deaths4 per 1000 live births. Although preterm birth and stillbirth share many risk factors, and preterm birth is the leading cause of neonatal mortality,6 rates of preterm birth—estimated to be 11.1% of all live births in 2010—appear to have increased in many countries over the past 10 years5 despite more generalised improvements in income,6 education and nutrition globally.7
Increased provision of obstetric interventions such as labour induction (LI) and prelabour caesarean delivery (PLCD) could explain these seemingly contradictory trends. LI and PLCD can save the mother and/or the fetus if provided to the appropriate population, even at the cost of increasing rates of early deliveries.8–13 Caesarean delivery rates have increased globally from an estimated 15% in 2002 14 to nearly 19% in 2015.15
Whether such increases in provider-initiated births have been beneficial or harmful has been the subject of considerable debate. An analysis of births in 39 high-income countries reported an association between the increase in interventions and increased rates of preterm birth, especially at late preterm (34 to 36 weeks) gestations.16 17 Studies in the USA have reported that the increase in intervention rates explain the increase in preterm birth rates10 but has not contributed to reducing fetal deaths under 40 weeks of gestation.18 19 However, most studies are limited to high-income countries, where clinical threshold for interventions is already quite low.
On the other hand, a recent report showed that despite a sharp global rise in caesarean section rates, sub-Saharan Africa had barely seen an increase over the last 10 years.15 Even in countries such as Brazil20 and China21 where excessive CD is of concern, reports continue to show wide socioeconomic disparities in access to such interventions when required.22 23
Compared with the vast literature on overall rates of CD and their potential maternal and neonatal consequences, we are aware of no previous study from low-income or middle-income countries assessing whether use of LI and/or PLCD are associated with improvement in perinatal survival and increased risk of late preterm birth. Such findings would help judge whether further provision of obstetric interventions would help reduce perinatal mortality but might also increase late preterm birth rates. Thus, we used a multicountry database on deliveries in 29 countries—mostly those of low and middle income—to investigate these issues.
Methods
Data source
We carried out a secondary analysis of data from the WHO Multi-Country Study on Maternal and Newborn Health (WHOMCS), a cross-sectional study whose primary aim was to collect information on intrahospital, early severe maternal outcomes (ie, maternal deaths and near-miss complications taking place before hospital discharge during the first postpartum week) among all deliveries from a sample of health facilities in Africa, Asia, Latin America and the Middle East. Detailed methods of the survey, including the stratified, multistage cluster sampling strategy, have been documented elsewhere.24 25
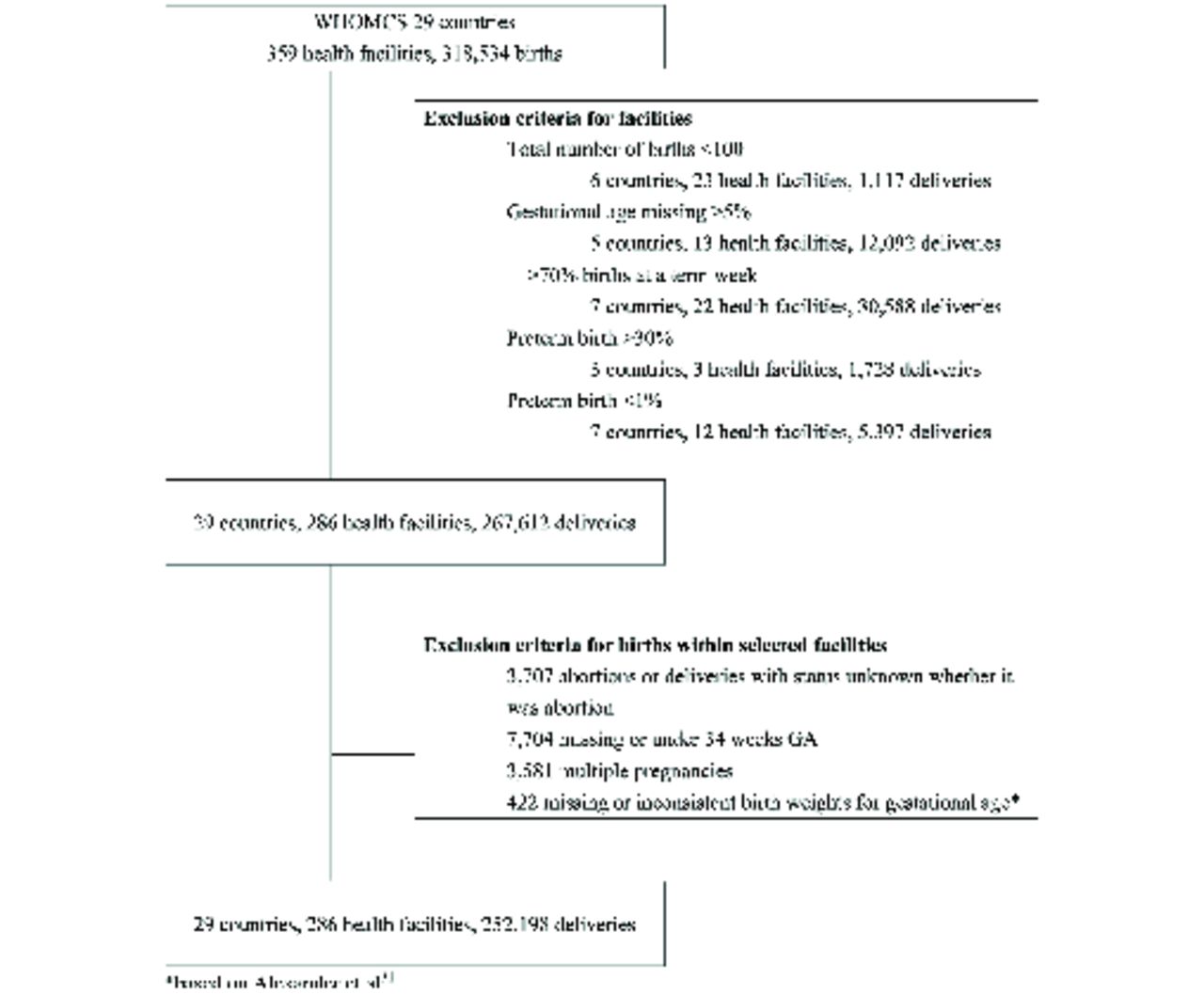
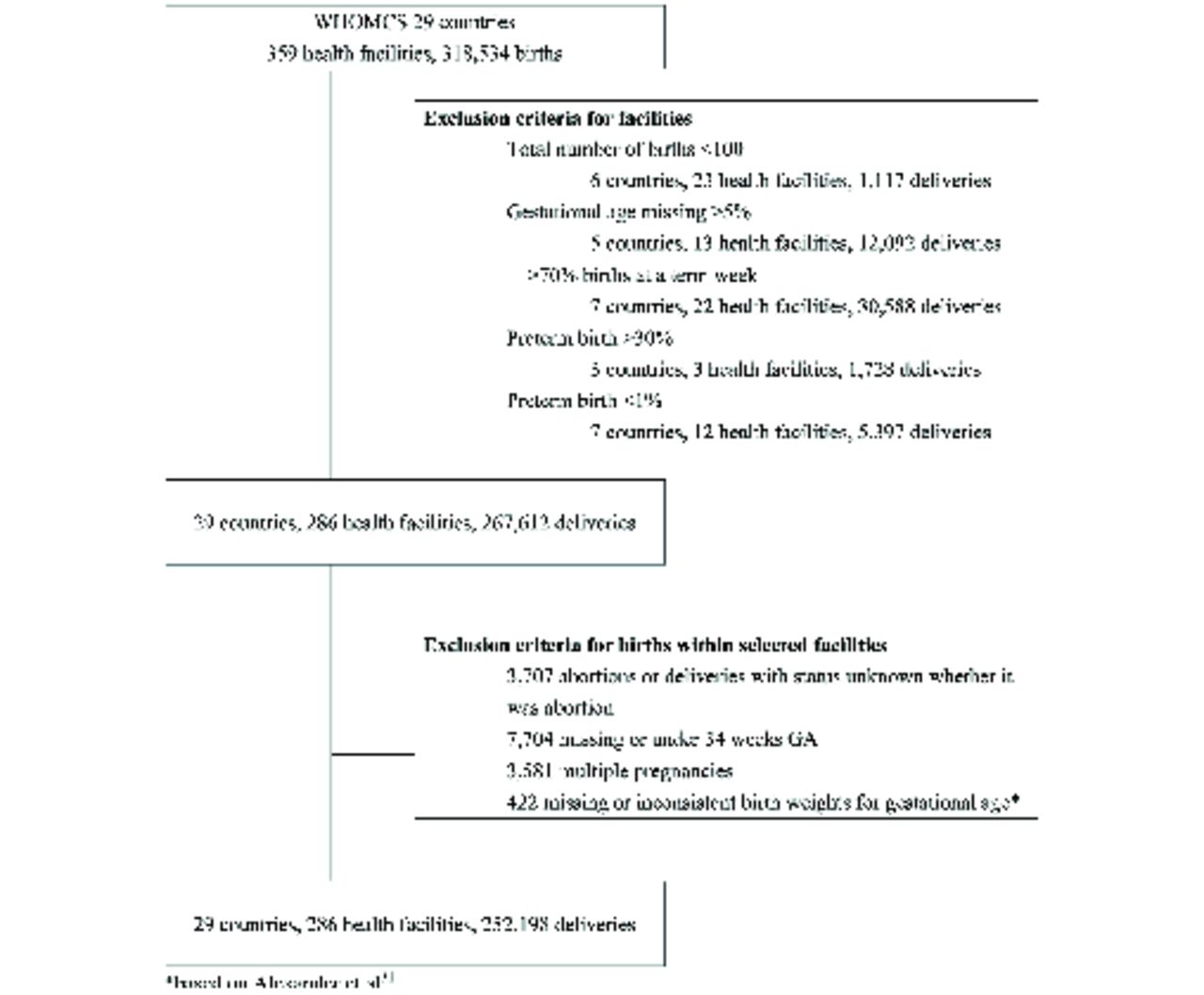
Briefly, the capital city and two randomly selected provinces (probability proportional to population) were sampled in each of the 29 participating countries. From a list of all facilities in each sampled jurisdiction with at least 1000 deliveries per year and the capacity to perform caesarean delivery, up to seven facilities were selected for participation (probability proportional to number of deliveries). A total of 359 health facilities were selected, and at each facility, trained health staff collected data on all women who were admitted for delivery or experienced severe maternal outcomes during the study period, regardless of gestational age or site of delivery. For each woman, data on demographic and reproductive characteristics, pregnancy outcomes, maternal and newborn morbidity and mortality and their management were collected directly from the medical records using a standardised form. In total, 318 534 deliveries at 359 health facilities (hospitals) in 29 countries were observed during the data collection period between May 2010 and December 2011.
Study population
We used a two-stage process to select health facilities (hospitals) and individual deliveries (figure 1). First, we excluded facilities in which gestational age data were missing for >5% of all deliveries and those with an unreliable distribution of gestational age (facilities at which more than 70% of all deliveries occurred at a specific week, or at which more than 30% or less than 1% of all deliveries were preterm) or had under 100 total deliveries. This exclusion led to 286 health facilities from the initial 359. At the individual level, from the 268 177 records at the 286 selected health facilities, we excluded births of less than 34 completed weeks gestation (who were not at risk of late preterm birth), multiple births and births with missing or implausible birth weight for gestational age (using the criteria of Alexander et al).26 The remaining 252 198 deliveries from 286 facilities in 29 countries constituted our final study population. Details of the excluded facilities and births are provided in online supplementary appendix 1.
{kind=link}
Derivation of study population. WHOMCS, WHO Multi-Country Study on Maternal and Newborn Health.
Variables and measurements
In the WHOMCS study, gestational age was based on the best obstetric assessment according to local practices. The method used to assess individual gestational age was not recorded and thus may or may not have included the use of ultrasound.
Onset of labour (LI, PLCD or spontaneous labour)), mode of delivery (vaginal or caesarean), vital status at birth (stillbirth or live birth), intrahospital neonatal survival (to the seventh day of life or discharge, whichever came first), infant sex, birth weight, gestational age, as well as maternal age (in years), marital status (married or not married), years of education, parity and number of previous caesarean sections were the pertinent variables available in the WHOMCS dataset. Intrapartum caesarean delivery (IPCD) was defined as the combination of onset of labour (whether induced or spontaneous) and CD.
We calculated the proportion of mothers with the following characteristics for each hospital: low maternal age (<20 years), advanced maternal age (≥35 years), unmarried, education of <6 years, primiparous and at least one previous caesarean section, as well as the proportion of births with LI, PLCD, IPCD, late preterm births (at 34 to 36 completed weeks of gestation), stillbirth, early neonatal death and perinatal death (stillbirth or intrahospital neonatal death).
Human Development Index
As an indicator of country development, we classified countries according to the United Nations Development Programme HDI ranking, as reported in 2012.27 As HDI is based on multiple indicators—that is, income per capita, life expectancy and years of education—rather than one, there was a group consensus that studies using this survey would group countries by HDI25 28 rather than based on other national indicators (such as maternal mortality, neonatal mortality, income per capita). The participating countries in the WHOMCS were categorised into four groups: very high (HDI ranking 1–50: Japan, Qatar, Argentina), high (HDI ranking 51–100: Mexico, Lebanon, Peru, Brazil, Ecuador and Sri Lanka); medium (HDI ranking 101–150: Jordan, China, Thailand, Mongolia, Occupied Territory of Palestine, Paraguay, Philippines, Vietnam, Nicaragua, India and Cambodia); or low (HDI ranking >150: Kenya, Pakistan, Angola, Nigeria, Nepal, Uganda, Afghanistan, Democratic Republic of Congo and Nigeria) (countries are listed in order of HDI).
Statistical analysis
We conducted an ecological analysis of 286 hospitals within 29 study countries, with hospital as the unit of analysis. The numerator for each study outcome at each hospital is the number experiencing each outcome (late preterm birth, stillbirth or intrahospital early neonatal death), while the denominator is the number of live births (for late preterm birth and early neonatal death) or of total births (for stillbirth) at or above 34 weeks of gestation. We used generalised estimating equations29 under logistic regression to estimate hospital-based ORs (and their 95% CIs for the outcomes, while accounting for clustering of hospitals within countries.
The primary associations of interest were with obstetric interventions that could modify late preterm birth rates: LI and PLCD. However, IPCD rates can also influence fetal outcomes (intrapartum stillbirth and neonatal death caused by asphyxia), although not late preterm birth rates. Analyses of neonatal outcomes (stillbirth and intrahospital early neonatal death) therefore included all three obstetric interventions (LI, PLCD and IPCD) in regression models, while analyses of late preterm birth included only LI and PLCD. In addition to the obstetric interventions, all regression models also included hospital-level proportions of maternal characteristics (percentage of births with mothers of low maternal age (<20 years), advanced maternal age (≥35 years), unmarried, education <6 years, primiparous and with previous caesarean section) and country HDI. To assess effect modification by level of country development, we also examined models containing a multiplicative interaction term (obstetric intervention × HDI) for each intervention. We defined significant interaction as the p value for the interaction being <0.10, and when it was so, we conducted stratified analysis in two HDI subgroups: very high/high HDI and medium/low HDI. All analyses were carried out using the GENMOD procedure (with binomial distribution and logit link function) in SAS V.9.4.
Results
Table 1 shows the distribution of participants and maternal characteristics by country HDI. Only three countries comprising 25 hospitals and 16 774 individuals were from very high HDI countries. Teenage pregnancies were most frequent in hospitals in high (11.6%) and low (11.5%) HDI countries, advanced maternal age pregnancies were most frequent in hospitals in very high (22.1%) and high (13.2%) HDI countries. Unmarried mothers were more frequent in hospitals located in very high (10.4%) or high (10.3%) HDI countries, whereas low maternal education was more frequent in hospitals located in middle (69.8%) or low HDI (66.7%) countries. Primiparous mothers were least frequent in hospitals from low HDI countries (34.4%). Previous caesarean section rates were similar in hospitals from countries of very high (9.4%), medium (9.6%) and low (9.8%) HDI but substantially higher in hospitals from high (15.8%) HDI countries.
Distribution of participants and maternal characteristics (in per cent) by country HDI
Table 2 shows hospital characteristics by country HDI. Rates of prelabour and intrapartum CD (ie, total CD rates) were highest in hospitals located in high HDI countries (PLCD: 17.9%, IPCD: 20.5%), while rates of PLCD was by far the lowest in hospitals in low HDI countries (5.1%). Rates of LI were much higher in hospitals from very high (10.9%) and high (11.2%) HDI countries compared with hospitals from medium (4.0%) or low (3.8%) HDI countries.
Hospital characteristics (in per cent) by country HDI
Rates of stillbirth and intrahospital early neonatal death (and thus of perinatal death) were highest in hospitals from low-HDI countries (stillbirth: 1.9%; intrahospital early neonatal death: 0.8%). Surprisingly, rates of late preterm birth were similar across hospitals in the four HDI strata (p=0.33) with the median at 4.0%–4.8%. Characteristics by country are shown in online supplementary appendix 2.
Table 3 shows the adjusted ORs (and their 95% CIs) between hospital rates of interventions (LI, PLCD and IPCD) and hospital rates of late preterm birth, stillbirth, early neonatal death and perinatal death, while accounting for hospital-level maternal characteristics, country HDI and clustering of hospitals within countries.
Association between hospital intervention rates (per 5% increase) and perinatal outcomes in all countries
Hospital LI rates were positively and significantly associated with late preterm birth (1.04 (1.01 to 1.06) per 5% increase in LI) and non-significantly with stillbirth (1.04 (0.97 to 1.11)), early neonatal death (1.04 (0.98 to 1.10)) and perinatal death (1.04 (0.98 to 1.10)). The association between LI and perinatal death was modified by country HDI (p=0.07): 1.06 (0.98 to 1.15) for medium/low-HDI and 0.99 (0.97 to 1.02) for very high/high-HDI.
Hospital PLCD rates were non-significantly associated with higher hospital late preterm birth rates (1.04 (0.98 to 1.10) per 5% increase in PLCD), but were significantly associated with lower rates of stillbirth (0.84 (0.76 to 0.94)), early neonatal death (0.92 (0.85 to 0.99))and perinatal death (0.87 (0.79 to 0.95)). The association between higher PLCD rates with lower stillbirth (p value for interaction=0.02) and perinatal death (p value for interaction=0.05) rates were stronger in medium/low-HDI countries (0.82 (0.73 to 0.93) for stillbirth; 0.85 (0.76 to 0.95) for perinatal death) than in very high/high-HDI countries (0.90 (0.82 to 0.98) for stillbirth; 0.94 (0.89 to 1.00) for perinatal death).
Hospital IPLCD rates at 34 weeks and above were not significantly associated with rates of stillbirth (0.98 (0.86 to 1.12) per 5% increase in IPCD), early neonatal death (1.02 (0.95 to 1.09)) or perinatal death (0.99 (0.89 to 1.10)). However, a significant interaction was observed between hospital IPCD and HDI for early neonatal death (p=0.02) and perinatal death (p=0.04); in stratified analyses, the association was null in medium/low-HDI countries (1.01 (0.91 to 1.12) for early neonatal death and 0.99 (0.87 to 1.12) for perinatal death) but positive for early neonatal death (1.16 (1.05 to 1.30)) and perinatal death (1.06 (1.03 to 1.10)) in very high/high-HDI countries. Although PLCS rates and IPCD rates differed between very high-HDI and high-HDI countries, results of analyses restricted to high-HDI countries only were very similar to those for the two HDI categories combined.
Discussion
We found that hospitals with higher rates of LI had higher rates of late preterm birth, and in low and middle-HDI countries, perinatal death. Hospitals with higher rates of prelabour caesarean section had lower rates of perinatal death but a non-significant increase in risk of late preterm birth. Thus, prelabour caesarean section showed a more favourable risk–benefit profile as compared with induction of labour, by showing an association with reduction in perinatal mortality. It should be noted though that maternal and neonatal adverse outcomes related to the mode of delivery were not assessed beyond hospital discharge or after the first postpartum week.
Population-based studies on the effects of obstetric interventions have been limited, compared with the descriptive global estimates literature on perinatal mortality,1 6 preterm birth5 and caesarean delivery,15 probably reflecting the paucity of representative population-based data on such interventions. The most frequently used method of data collection in most low-income country studies has been household surveys, which require the mother’s recall of services provided around the time of birth often 2 to 5 years after delivery. In our study, LI and PLCD rates were extracted from maternity hospital records shortly after birth. Rates of these interventions were lowest in hospitals in low-HDI countries, while rates of stillbirths and intrahospital early neonatal deaths (and thus perinatal deaths) were highest in those countries.
Previous studies have reported a reduction in stillbirths in the post-term period in association with rising rates of LI,18 19 supporting the results of randomised trials of routine induction after 41 weeks, which is currently recommended in many organisations and countries.30 31 On the other hand, studies from the USA, where induction of labour and mode of delivery are now included on birth registrations, have shown that increase in LI in the 1990–2000s were highly correlated with the contemporaneous increase in preterm birth rates,16 results consistent with our finding that increased provision of labour induction at the hospital level was associated with higher rates of late preterm birth in both high-income and low-income countries. We were unable to identify any study assessing global trends in induction rates. While the observed association between increased labour induction rates and adverse birth outcomes could be due to residual confounding caused by selective referral of high-risk cases to better-equipped hospitals able to perform these interventions, our results suggest that further provision of induction may not improve birth outcomes in either high-income or low-income countries.
More evidence is available on the association of CD with neonatal outcomes,15 32–34 although most studies have not been able to separate prelabour from intrapartum CD. Global estimates of CD rates have increased alarmingly; among 121 countries, all of them except for Guinea and Nigeria experienced an increase between 2005 and 2014.15 In their global estimate of CD rates, Betrán et al have reported that rates have increased least in sub-Saharan Africa.15 The association of higher PLCD rates with reduced rates of stillbirth and perinatal death was stronger in the least-developed countries yet persisted in high HDI-countries where overuse of CD has been reported.20 21 23 35 We recently reported that the increase in CD rates observed between two WHO surveys (conducted in 2003–2005 and 2011–2012)28 did not appear to contribute to improved neonatal outcomes observed in these countries.36 Findings from these and our current study suggest that the increase in PLCD has occurred mostly where it is not needed, but that improved access to that invention among those in need could improve birth outcomes, although at the cost of higher preterm birth rates.
It is of note that in our study, late preterm birth rates were positively associated with provision of interventions but did not differ by HDI. Higher development could both decrease spontaneous preterm birth rates, owing to better maternal health, but increase provider-initiated preterm birth, thus reflecting the complex aetiology of preterm birth and the difficulties in identifying effective preventive interventions.
To our knowledge, ours is the first report of an association between hospital provider-initiated birth rates and perinatal outcomes among deliveries in facilities in low-income and middle-income countries. We limited our analysis to deliveries above 34 weeks in order to eliminate pregnancies with extreme pathologies leading to spontaneous or provider-initiated early preterm birth, as such pathological pregnancies would more likely be referred to specialised hospitals. Our database included information on onset of labour and mode of delivery, as well as detailed individual demographics, other risk factors and birth outcomes such as gestational age, vital status at birth and intrahospital early neonatal death. We used perinatal death (stillbirth or early neonatal death) as our main outcome, as the registration practices for stillbirths versus early neonatal deaths may be inconsistent, especially in low-HDI countries.37 Our ecological design should minimise the potential for confounding by clinical indication of the association between obstetric interventions and birth outcomes, which inevitably occurs when analysed at the individual level.38 Nonetheless, the ecological design also suggests the need for caution in interpreting the observed associations, which may not be causal because of unmeasured confounding due to common ecological causes of the obstetric interventions and adverse perinatal outcomes.
Our study is also subject to several limitations. First, our data were limited to outcomes occurring during admission in the first 7 days after birth. We thus were unable to analyse long-term morbidities and other important outcomes such as child development, which should also be considered when balancing the risks and benefits of obstetric interventions. Second, our outcomes focused on the fetus and infant and did not include those of the mother. CD has known adverse effects on the mother, such as increased risk of maternal morbidity such as infectious complications, as well as complications of subsequent pregnancies. Our study may also have been limited by the method used to estimate gestational age, which was based on local practices. Since these practices vary widely in developing countries and the use of early obstetric ultrasound is not available in many of these settings, errors in gestational age estimation may have led to misclassification of some cases of preterm birth. Another limitation concerns the validity of the distinction between prelabour versus intrapartum CD, which may have varied widely across hospitals, even within countries. Even though trained staff extracted the data from hospital records using strict criteria for making those distinctions, their consistency in coding is limited by the quality of the notes written by the individual clinicians. Both of these data quality limitations should have been non-differential with respect to the study outcomes, however, and thus would have biased the observed associations towards the null.
Finally, our data were cross-sectional, rather than longitudinal, and thus the interpretation of our results should be limited to comparisons between hospitals rather than on temporal changes within hospitals. Moreover, our study is limited by its ecological design. Despite our control for individual-level factors, unmeasured characteristics of the mothers, pregnancy complications and aspects of the clinical care provided may well have led to residual confounding of the associations we studied. The positive association we observed between IPCD and perinatal mortality may in part be due to constraints to effective labour monitoring and interventions to expedite labour by induction and augmentation and increasing the risk of worsened perinatal outcomes. However it is also likely that the association is reflecting unmeasured risk differences (residual confounding by indication) at the hospital level and/or selective referral of high-risk cases (women in labour with signs of fetal distress) to hospitals that can perform caesarean section. Likewise, causal interpretations of the associations between PLCD, LI and birth outcomes should also be made with caution. In particular, our findings should not be used to justify obstetric interventions in the absence of strong clinical indications; recent studies suggest that both too much, too soon and too little, too late use of obstetric interventions can cause harm.39 Future studies, ideally with longitudinal population-based data, should further explore the optimal frequency and timing of interventions. We urge clinicians to heed the WHO recommendation that ‘Every effort should be made to provide caesarean sections to women in need, rather than striving to achieve a specific rate’.40
Conclusion
In this ecological analysis, rates of PLCD were associated with reductions in perinatal mortality, but also with increases in late preterm birth. LI rates were positively associated with both late preterm birth and, in less-developed countries, perinatal mortality. Efforts to provide sufficient, but avoid excessive, access to provider-initiated delivery should be tailored to the local context.
Acknowledgments
We wish to thank all members of the WHO Multicountry Survey on Maternal and Newborn Health Research Network, including regional and country coordinators, data collection coordinators, facility coordinators, data collectors and all staff of participating facilities who made the survey possible. This article represents the views of the named authors only and not the views of their institutions or organisations.
References
Footnotes
Contributors MK and JV initiated the concept. MK, NM, TG designed the study. NM and XZ conducted the analysis, NM wrote the initial manuscript and MK provided oversight of the process. All authors critically reviewed data tables and the initial draft and approved of the final draft. NM had full access to all of the data in this study and take complete responsibility for the integrity of the data and the accuracy of the data analysis.
Competing interests None declared.
Patient consent Our article does not include personal medical information about an identifiable living individual.
Ethics approval WHO Ethical Review Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Aggregated data are available on request from authors.