Article Text

Abstract
Universal health coverage generates significant health and economic benefits and enables governments to reduce inequity. Where universal health coverage has been implemented well, it can contribute to nation-building. This analysis reviews evidence from Asia and Pacific drawing out determinants of successful systems and barriers to progress with a focus on women and children. Access to healthcare is important for women and children and contributes to early childhood development. Universal health coverage is a political process from the start, and public financing is critical and directly related to more equitable health systems. Closing primary healthcare gaps should be the foundation of universal health coverage reforms. Recommendations for policy for national governments to improve universal health coverage are identified, including countries spending < 3% of gross domestic product in public expenditure on health committing to increasing funding by at least 0.3%/year to reach a minimum expenditure threshold of 3%.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial Non Derivative (CC BY-NC-ND 4.0) license, which permits users to copy, distribute and transmit an article as long as the author is attributed, the article is not used for commercial purposes, and the work is not modified or adapted in any way. See: http://creativecommons.org/licenses/by-nc-nd/4.0/legalcode
Statistics from Altmetric.com
Key questions
What is already known about this topic?
Universal health coverage can generate significant health and economic benefits.
Despite costing more to national governments in the short term universal health coverage pays back its initial debt to national economic growth in multiples.
Access to healthcare contributes to early childhood development.
What are the new findings?
This analysis draws out determinants of successful universal health coverage systems and barriers to progress with a focus on women and children.
Next steps for governments are suggested in 10 policy recommendations to improve universal health coverage.
Key recommendations for policy
Invest in good quality accessible primary healthcare as the foundation of universal health coverage.
Countries spending <3% of GDP in public expenditure on health should commit to increase funding by at least 0.3%/year.
Introduction
Universal health coverage (UHC) can generate significant health and economic benefits to populations1 and enable governments to reduce inequity.2 Despite costing more to national governments in the short term, UHC pays back its initial debt to national economic growth in multiples. Access to healthcare is important for women and children, including establishing breastfeeding and immunisation, and contributes to early childhood development.
The Lancet Commission on Investing in Health in 2013 found that the economic benefits of achieving a grand convergence of global health outcomes for infectious diseases and for maternal and child health would outweigh the costs by a factor of between 9 and 20 over 20 years from 2015 to 2035.3 When implemented well UHC can contribute to nation-building.4–6 UHC has an important role to play in global health security efforts through building a strong frontline health system, strengthening access to vital services and funding robust surveillance systems.7–9
There is a huge wealth of technical and policy materials on UHC from Asia, and the rate of production has increased since UHC was formalised as a sustainable development goal target. This analysis synthesises the best available evidence to inform political decision-makers in Asia and Pacific by identifying critical lessons emerging from the region and suggesting policy recommendations. A summary of the methods used is shown in box 1.
Methodological approach
Structured literature search including grey literature. Keywords used for searching PubMed, Google Scholar, and United Nations publication banks. Documents were selected based on relevance to UHC, Asia and Pacific, and maternal and child health.
Interviews with more than 35 stakeholders across the region to identify policy priorities and lessons from experience.
Data review including health financing data and progress made in delivering health outcomes for women and children for the countries of Asia and Pacific.
What is UHC?
UHC is defined by the WHO as a means to ensuring that “all people obtain the health services they need without suffering financial hardship when paying for them”.10 UHC combines two benefits: first, everyone is covered by a package of good quality health services; and, second, UHC provides financial protection from healthcare costs.
Several critical elements underpin UHC, including an efficient, equitable and resilient health system; a financing system that does not impoverish users; access to essential medicines and technologies; sufficient numbers of motivated and skilled health workers; efficient administrative and governance arrangements; and transparency in tracking progress. Achieving UHC requires countries to advance health services. The proportion of the population covered should extend to encompass all people in a country (universal population coverage). The range of services covered should expand as resources permit, including sufficient investment in essential public health functions. Services must be accessible and be of adequate quality to be effective. And, the proportion of the financing required to deliver services should be increasingly drawn from pooled funds raised through compulsory prepayment mechanisms, including general or specific taxation or public social insurance.
UHC has increasingly become the focus of the global health agenda.11 In 2012, Margaret Chan called UHC, “the single most powerful concept that public health has to offer”.12 Adopting and sustaining a UHC system is as much a political process as a technical one. UHC begins with and is sustained by genuine political commitment by national leaders. Choosing how to advance UHC is different in each country's context, but countries that have made progress with UHC have experienced a range of benefits (table 1).
Where are Asia and Pacific countries on the UHC journey?
There are never enough resources to fund all the health services that the population can consume. UHC needs to operate within reasonable financial constraints. The Lancet Commission on Investing in Health (2013) shows that as economies grow, countries that increase their public health expenditure (PHE) to more than 3% of gross domestic product (GDP) can make faster progress reducing health outcome disparities and provide a basic package of care (and 4% of GDP is even better).3
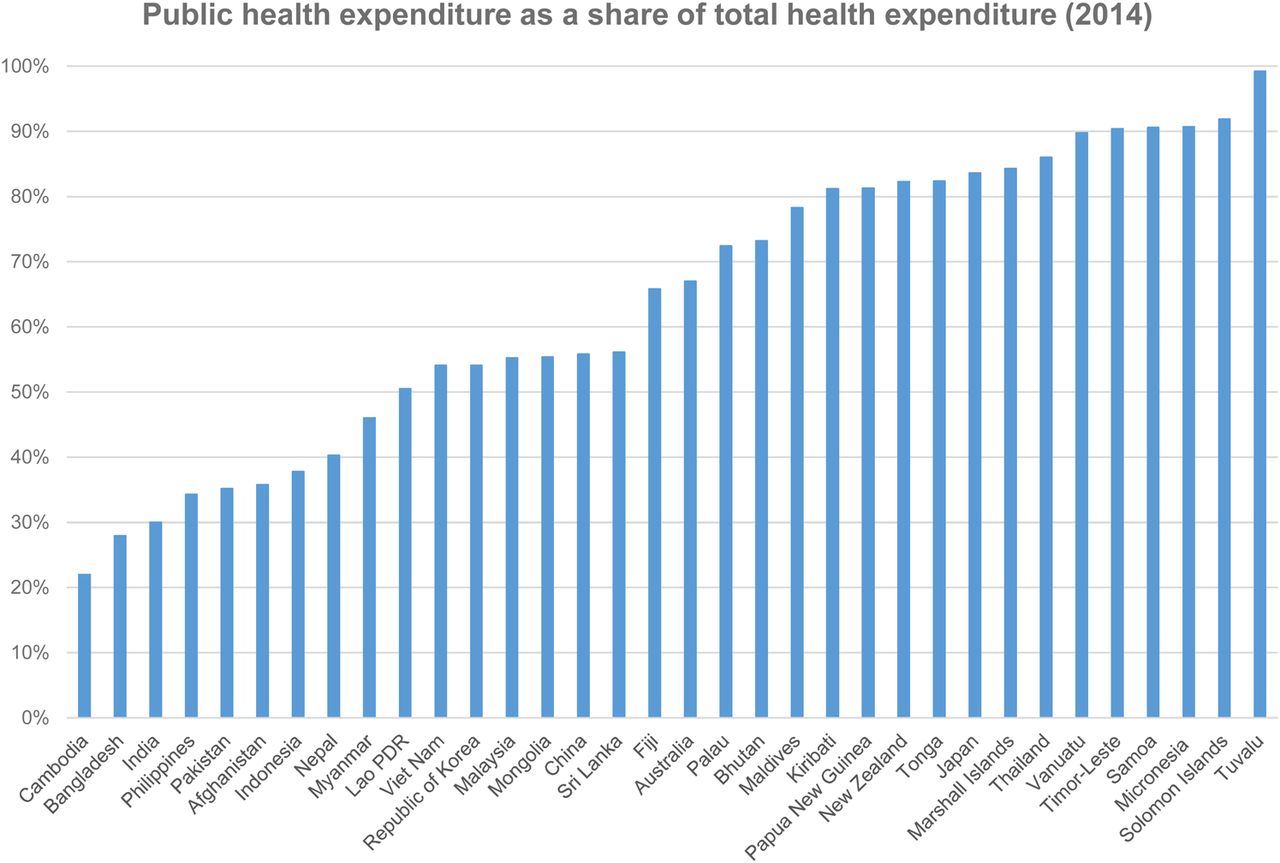
Resources available for health come either from public mechanisms (tax funding, social insurance and external aid) or through private mechanisms such as private insurance schemes, direct out-of-pocket (OOP) payments and some limited use of personal health savings accounts. Total health expenditure (THE) calculates spending on health from all sources of financing, including public and private sources. Figure 1 shows the total and public health spending in Asia and Pacific, expressed as a percentage of GDP, and figure 2 shows PHE as a share of THE (2014).

THE and PHE in Asia and Pacific countries World Bank 2014. THE, total health expenditure; PHE, public health expenditure.

Public health expenditure as a share of total health expenditure World Bank 2014.
Most countries spend <4% for public expenditure on health. The higher the PHE as a share of THE, the more control a country has over how it can allocate resources equitably to respond to its burden of disease.
What should countries do to accelerate progress towards UHC?
Using evidence and experience from the Asia and Pacific region, this analysis identifies a series of insights to support countries as they seek to improve UHC within their own context.
UHC is a political process from the start
Across Asia and Pacific, political leaders have recognised that successful UHC reforms are extremely popular and can be a potent political tool to help win and sustain power. UHC can generate huge benefits for some groups in society but can have significant costs for other groups. This, in turn, can result in considerable political costs and benefits (in terms of popularity) for governments and political leaders overseeing reform processes. Given the high political stakes involved, it is not surprising that UHC reforms in the region have often been led by the head of state (eg, Prime Minister Hayato Ikeda in Japan (1963), President Park Chung Hee in the Republic of Korea (1977) and most recently President Joko Widodo in Indonesia (from 2014)). In particular, fulfilling the equity principle underlying UHC (that healthy and wealthy people subsidise services for the poor, vulnerable and sick) requires a strong role for the state in establishing and governing a progressive health financing system. Many analyses of large-scale UHC programmes in Asia have cited political reasons as the main motivation behind these reforms.20 ,24 ,25
Closing primary healthcare gaps is the foundation
Closing primary healthcare gaps should be the foundation of UHC reforms.26 Countries that want to make rapid progress towards UHC should prioritise primary healthcare, including prevention and health promotion as a first step. Well-structured, efficient primary health services can meet most of the health needs of the population. Engaging communities and removing barriers to access is a core dimension of strengthening primary care. These measures include removing non-financial access barriers, including perceptions about poor quality; language and cultural barriers; lack of appropriate services (eg, for adolescents); indirect costs; and poor community engagement in health. Some of these barriers can be addressed through strengthening health services while others, such as the indirect costs of accessing care, may involve other social protection measures such as cash transfers.
Improve the quality of care through sustained health systems strengthening
For many countries, the risk is that UHC is launched, entitlements are announced, but the services promised are not available.27 Promises concerning service coverage have to translate into usage in practice. Although hard to measure, quality is generally thought to encompass several defining features, including patient safety, effectiveness, people-centredness and delivering integrated services. Perceived quality is what patients think about the quality of care they receive and it is judged by the experience of attending health services. The main determinants of quality include availability of drugs; qualified, available and respectful health staff; and integrated, appropriate services that meet community needs.1
Make progress with social and economic determinants of health
Health services alone do not engender health and there are a number of important contributors to health that lie outside the health sector's direct authority. Nutrition underpins health to such an extent that it is linked to 45% of child deaths.28 Water, sanitation and hygiene; gender empowerment; household income (poverty); quality of housing; infrastructure; and education (especially for girls and women) all drive health outcomes.29 Countries and states that have made the most progress in improving the social and economic determinants of health can also demonstrate the best health outcomes. Other policies can have a significant impact on the promotion of healthy behaviour, including, for example, excise taxes on tobacco products, taxes on sugar and sweeteners, legislation to enforce the use of bicycle helmets, seatbelts and other measures.
Public financing is critical
Public financing is critical and directly related to more equitable health systems.30 As countries in Asia and Pacific have become wealthier, their health financing systems have developed in similar ways. First, as their economies have grown they have spent more on health as a share of their GDP, indicating a growing societal demand for health services. In common with the rest of the world, high-income countries in the region now spend around 9% to 12% of their GDP on health, middle-income countries spend between 5% and 9%, and low-income countries spend < 5%. Second, the composition of the health financing systems has changed, with the share of public financing (from general taxation and social health insurance) growing over time and replacing private voluntary financing (mostly in the form of OOP health financing). This is demonstrated across the region where private financing dominates in low-income and lower-middle-income countries, whereas public financing is dominant in higher-income countries.
These health financing trends show that economic growth is the main driver of increasing overall health spending, and it is political pressure from populations that lead governments to enact legislation to give public financing a dominant role.31 Populations and politicians have realised that only publicly governed health financing systems can enforce the cross-subsidies required from the rich to the poor and the healthy to the sick, which are necessary to achieve UHC. Politically driven financing transitions have been evident across Asia and Pacific over the last few decades, with many countries socialising their health financing systems, for example, Japan (1963), Republic of Korea (1977), Thailand (2001), Nepal (2008), China (2009) and Indonesia (2014).
Large increases in public funding gives countries the financial resources to increase the availability and quality of health services while reducing the burden on households financing health services out of their own pockets. Figure 3 shows that in countries spending more than 3% of GDP of public finances on health, OOP spending was <20% of THE. This is important because below this level OOP spending tends to be less catastrophic and impoverishing in nature.32

{kind=link}
{kind=link}
{kind=link}
Public health financing replacing out-of-pocket expenditure in Asia and the Pacific World Bank 2014.
Pool funds to increase efficiency and equity
Moving away from financing a health system through direct OOP payments requires introducing or strengthening forms of prepayment and the pooling of health funds to protect the population against the financial risk of paying for services. Pooling funds can drive equity.19 ,21 In creating these pools, it is important to emphasise that only publicly governed risk pools, where contributions are compulsory and progressive (related to people's ability to pay), can meet the equity requirements for UHC. Private voluntary insurance schemes do not achieve this outcome because there is an incentive to exclude high-need people in society and for richer or healthier members to refuse to pay higher contributions. Those less likely to use health services tend not to join, which limits cross-subsidisation. All countries can take steps towards increasing cross-subsidisation even if fully combining all public pools of funds is not immediately feasible.
Priority setting for equity is a political process
Priority setting is the process of deciding what health services should be covered under UHC, and who should benefit and when. Priority setting is an inherently political process and is often controversial since it leads to choices about who in society will benefit from public resources and who will not. If countries used cost-effectiveness analysis, including explicit and transparent methods such as health technology assessment, to re-allocate available health funding to equity-enhancing health interventions, many more lives could be saved. Few countries can afford to immediately fund a full package of services to all citizens and the vast majority take incremental steps over time.5 One key decision to be taken in working towards UHC is whether to prioritise coverage of people with a basic package of care or to extend the quality and range of services to be offered to a more limited group, such as the formally employed. Coverage of the whole population with a defined range of services leads to improved population outcomes and lower inequalities than covering a narrow group of citizens with higher quality services.33 This approach also promotes equity and embeds the principles of cross-subsidy from the start.34 ,35
Engage the private sector to support UHC
Across Asia and Pacific, the majority of outpatient health services are delivered by private health providers, although in most countries inpatient care is still mainly delivered in public-sector hospitals.36 The challenge for countries is to find ways to engage private providers, maximising their potential to increase the coverage of basic services to all people while minimising their incentives to oversupply and overcharge for services. Whereas public financing is essential for UHC, when it comes to the provision of services there is much more scope to deliver services through a mixture of public and private providers.
Make UHC a long-term proposition
Although one political party may seize an opportunity to launch UHC, ultimately, a UHC system has to be seen as a national goal, belonging to all and one that needs sustained, enduring, cross-party and intergenerational commitment.5 In Japan, Republic of Korea, Sri Lanka, Thailand and other countries with well-developed UHC systems, populations have come to expect UHC as their right and politicians stand on platforms that include how—not whether—they will protect and advance that right.24 Reaching this ‘tipping point’ on the UHC journey is a vital milestone if the system is to become resilient in the face of inevitable challenges. As a dynamic process, UHC needs to contend with: the ebb and flow of national economic growth that can stall UHC; population health needs that change constantly due to ageing, migration, old and new diseases; the health impacts of climate change; and, natural disasters.
Build accountability through transparent progress tracking and monitoring
The UHC journey is unique to each country. Maintaining momentum towards the achievement of UHC goals requires timely and reliable data, the willingness to undertake course corrections at periodic intervals and a strong sense of accountability to citizens. Open and transparent accountability helps policymakers maintain commitment and focus. It helps to ensure resources are used as intended. And, it supports citizen empowerment to track progress and provide feedback, deepening citizen engagement. Most countries that have made progress with UHC also have good data collection and analysis at the heart of their systems founded on a health management information system.
Policy recommendations
Each country's UHC journey will be different: there is no blueprint. Yet, there are some important determinants of success. Every country can make progress from their current position. All countries, regardless of their economic status, can increase domestic revenue for health by improving tax collection, adjusting tax rates and introducing new progressive taxes, including taxes on alcohol, tobacco and other commodities. Box 2 makes 10 policy recommendations for countries aiming to advance UHC.
Ten policy recommendations for countries aiming to advance UHC
Ten policy recommendations:
Make UHC a ‘whole of government’ decision linked to nation-building and achieving citizen development;
Engage political actors, including the head of state, parliamentarians, administrators and powerful interest groups across the political and social spectrum;
Engage beyond health to strengthen the critical drivers of UHC systems such as tax collection and budget management;
Invest in good quality accessible primary healthcare as the foundation of UHC and a precondition for success;
Be willing to develop differentiated strategies and to pay more to address equity and remove barriers to access for the poorest;
Countries spending <3% of GDP in public expenditure should commit to increase funding by at least 0.3%/year;
Take steps towards combining funds from all sources to create the largest pool of resources possible to maximise cross-subsidisation;
Establish a transparent priority-setting process to determine what should be included in the UHC package;
Engage the private sector through strengthened regulation, negotiated payment systems, and partnership;
Strengthen accountability through developing and monitoring clear, explicit and measureable targets.
Success is possible through policy change and maintenance of a UHC system. An independent review of the first 10 years of Thailand's Universal Coverage Scheme (UCS) showed a dramatic reduction in the proportion of OOP health expenditure and falls in catastrophic health expenditure and impoverishment due to healthcare costs.17 Between 1996 and 2008 the incidence of catastrophic healthcare expenditure among the poorest quintile of UCS members fell from 6.8% to 2.8%. Furthermore, the incidence of non-poor households falling below the poverty line because of healthcare costs fell from 2.71% in 2000 to 0.49% in 2009. The review calculated that the comprehensive benefit package provided by the UCS and the reduced level of OOP expenditure protected a cumulative total of 292 000 households from health-related impoverishment between 2004 and 2009.
UHC is a whole of government decision linked to nation-building. It needs to engage stakeholders beyond the health system and critically the head of state to achieve success. Strengthening primary care is critical coupled with ongoing increases in public investment. Massive change at scale with the potential to change lives is possible through a combination of learning the successful lessons from countries further on in the UHC journey, and taking the policy steps necessary to secure change.
References
Footnotes
Handling editor Seye Abimbola
Twitter Follow Rob Yates at @yates_rob and Douglas Noble at @douglasnoblemd
Contributors AB drafted the first version, and RY and DJN edited the manuscript. This paper is based on a longer thematic report released on 7 November 2016 at the Asia Pacific High Level Meeting on Child Rights.
Funding This work was funded from the resources of Unicef and Chatham House.
Disclaimer This paper is based on a longer thematic report presented on November 7th and 8th, 2016 at the UNICEF High Level Meeting on South-South Cooperation for Child Rights in Asia and the Pacific. The opinions expressed in this paper are solely those of the authors and do not necessarily represent the views or policies of UNICEF or any other agency.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.