Article Text

Abstract
Background Investments in faculty exchanges to build physician workforce capacity are increasing. Little attention has been paid to the expectations of host institution faculty and trainees. This prospective qualitative research study explored faculty and resident perspectives about guest faculty in paediatric departments in East Africa, asking (1) What are the benefits and challenges of hosting guest faculty, (2) What factors influence the effectiveness of faculty visits and (3) How do host institutions prepare for faculty visits?
Methods We recruited 36 faculty members and residents from among four paediatric departments in East Africa to participate in semistructured interviews which were audio recorded and transcribed. Data were qualitatively analysed using principles of open coding and thematic analysis. We achieved saturation of themes.
Results Benefits of faculty visits varied based on the size and needs of host institutions. Emergent themes included the importance of guest faculty time commitment, and mutual preparation to ensure that visit goals and scheduling met host needs. We documented conflicts that developed around guest emotional responses and ethical approaches to clinical resource limitations, which some hosts tried to prepare for and mitigate. Imbalance in resources led to power differentials; some hosts sought partnerships to re-establish control over the process of having guests.
Conclusions We identified that guest faculty can assist paediatric institutions in building capacity; however, effective visits require: (1) mutually agreed on goals with appropriate scheduling, visit length and commitment to ensure that the visits meet the host's needs, (2) careful selection and preparation of guest faculty to meet the host's goals, (3) emotional preparation by prospective guests along with host orientation to clinical work in the host's setting and (4) attention to funding sources for the visit and mitigation of resulting power differentials.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known about this topic?
Existing studies describe academic institution partnerships such as the Medical Education Partnership Initiative, focus primarily on undergraduate medical education or research, and note North–South power imbalances and a need for faculty development.
Results from two small qualitative studies about guest faculty carried out in single institutions indicated that hosts have positive feelings about guest faculty, though concerns include cultural differences, poorly aligned expectations, need for more mutual partnership and ethics of guest faculty clinical decisions.
What are the new findings?
This study explored host perspectives of guest faculty anonymously, in detail and at multiple sites in East Africa with interviews carried out by an East African physician.
Hosts shared experiences of benefits and challenges with stories that highlighted sources of conflict, the need for mutuality and partnership in planning, careful guest selection and preparation particularly for working clinically with limited resources, and attention to power imbalances and resources.
Recommendations for policy
Guest faculty visits may be more effective with the following: (1) mutually agreed on goals with appropriate scheduling, visit length and commitment to ensure that the visits meet the host's needs, (2) careful selection and preparation of guest faculty to meet the host's goals, (3) emotional preparation by prospective guests along with host orientation to clinical work in the host's setting, (4) attention to funding sources for the visit and mitigation of resulting power differentials.
Formal partnerships may improve mutuality of faculty exchanges, mitigate inherent power imbalances and allow for more sustained, trusting and open relationships.
Background
In countries suffering from high levels of poverty, capacity for training healthcare workers is often limited by numbers of existing faculty and subspecialty expertise. The Lancet Commission on Education of Health Professionals for the 21st Century called for sharing and strengthening educational resources, and linking educational institutions worldwide.1 Many medical education programmes such as Rwanda's Human Resources for Health and the Peace Corp's Seed Global Health rely on guest faculty to enhance training opportunities.2–4
Given the dearth of paediatricians in many countries, multiple global networks collaborate to improve paediatric education, and several academic paediatric centres in high and low-income countries are developing partnerships.5–8 We studied new paediatric residency programmes in low-income countries and found common early reliance on guest faculty with both positive and negative attributes.9
Host perspectives of guest faculty are not well represented in the literature. A qualitative study of nine host physicians at one institution noted themes of (1) culture, context and concern, (2) expectations, intentions and miscommunications, and (3) partnership and the desire to share and gain knowledge.10 A survey of surgical and anaesthesia trainees in Uganda found that while the majority agreed that visiting faculty improved their training, many reported a neutral or negative impact on patient care and discomfort with the ethics of visiting faculty's clinical decisions.11
Most studies about global partnerships focus on undergraduate medical education, with common elements of success including ownership of the agenda by African partners, frequent communication between partners and a focus on developing local expertise onsite at the African institution.12 ,13 In specialty fields such as paediatrics, the literature is composed primarily of project descriptions.14–17 There are emerging competencies in global health for professionals that are pertinent to, but not specific for, the roles of guest faculty.18–21
We report a prospective qualitative study in medical education designed to explore the perspectives of faculty and residents at academic institutions in East Africa regarding guest faculty. The study was guided by three key research questions: (1) What are the benefits and challenges of hosting guest faculty? (2) What are the major factors or guest faculty behaviours that influence the efficacy of guest faculty teaching? and (3) How do host institutions prepare for guest faculty visits.
Methods
This research used a grounded theory approach to explore guest faculty visits, employing a stratified purposeful sampling strategy. We recruited academic centres in East Africa by emailing all paediatric chairpersons in three countries—Uganda, Tanzania and Kenya. These countries were selected given their use of English in medical training and existence of multiple faculty exchanges. Of the six programmes contacted, four agreed to participate. Programmes ranged in size from 2 to 80 paediatric ‘registrars’ or residents, with faculty sizes varying from 8 to 35. The programmes had been in existence between 26 and 92 years.
We identified three subgroups: senior faculty with leadership roles, junior faculty and paediatric residents. We aimed to interview three individuals in each subgroup at each institution for a total of 36 participants. Research logistics required that we establish the sample in advance; we felt that 36 participants would allow for a fully saturated theory. We developed loosely structured sets of questions, reflecting the differing roles of faculty and residents, to guide exploration of different aspects of guest faculty visits (see online supplementary appendix 1).
The sole interviewer (DM) is a Kenyan physician working towards her PhD, who was recruited separately as a paid research assistant. She recruited potential participants by email and at departmental meetings. All 36 in-depth, semistructured interviews were conducted between October and December 2014. Interviews were audio recorded and transcribed. In order to promote more candid discussions, we kept participant and institution names anonymous and removed identifying information after transcription.
Data were qualitatively analysed with the assistance of OpenCode V.4.01 software,i using principles of open coding and thematic analysis to identify broad patterns in the collected data. Modified axial coding using hierarchy coding maps was used in order to identify and clarify relationships between themes and to explore causal relationships. Three individuals separately coded the interviews and met to compare and resolve any differences. Multiple coding and cross-checking were used in the initial analysis in order to optimise inter-rater reliability. Additional comparison reviews were carried out across the coding to assure intra-rater and inter-rater reliability. These ongoing reviews allowed for communication between coders to explore alternative interpretations and explanations of the themes and patterns uncovered. Saturation of themes was achieved.
This study was reviewed and approved by an institutional review board in each country in which interviews were done, in addition to all author institutions including Boston Children's Hospital IRB, Kenyatta National Hospital/University of Nairobi Ethics Review Committee, Research and Ethics Committee of Makerere University College of Health Sciences, Uganda National Council for Science and Technology, Muhimbili University of Health and Allied Sciences Directorate of Research and Publications, and Tanzania Commission for Science and Technology.
Results
We interviewed 36 individuals as per our protocol. We had a slightly higher representation from senior faculty as we included department chairpersons, and had fewer respondents from one institution due to faculty unavailability (table 1).
Participant demographics
The participating institutions varied in numbers of guests hosted, ranging from 2 to 10/year, with the global approach to guests appearing to evolve with institutional growth. At larger programmes, senior faculty described hosting many guest faculty early in the institution's existence with lower reliance on guests as the base of local faculty grew. The goals of guest visits also evolved, focusing more on training in specific areas or subspecialties. As programmes grew, some became more selective in the type of guests they were willing to host. There was variation in the degree of effort institutions put into preparing for and hosting guests.
All three subgroups described similar guest experiences, though residents focused more on the benefit of shared knowledge and teaching styles while faculty frequently focused on programmatic aspects.
Themes
We identified five general themes, many of which were significantly interlinked with subthemes focusing on factors or guest behaviours that influenced the efficacy of guest visits. Emergent themes included:
Engagement: the degree to which guest faculty interacted with host faculty and trainees, including time spent and commitment.
Understanding of local context: how well guest faculty knew the local context with regard to culture, common diseases, clinical work with limited resources and teaching needs.
Meeting the needs of hosts: the degree to which the visit was designed to meet the host's needs.
Host and guest resources: the monetary and non-monetary resources required for visits.
Preparation and planning: efforts undertaken by both the guest and host to plan and prepare for the visit.
Benefits
All 36 respondents indicated some benefit to hosting guest faculty (table 2) even at institutions in which hosting guests was a lower priority. Almost all respondents appreciated sharing of knowledge and approaches to clinical problems.
Quotes on benefits
For smaller institutions with fewer (8 to 10) faculty, guest faculty filled gaps by teaching locally unavailable subspecialties and by providing additional faculty to interface with numerous trainees.
Almost all senior faculty and a majority of junior faculty appreciated the guests’ ability to help build faculty capacity, predominantly in areas of research and clinical care. A few respondents noted guest faculty involvement in the development of subspecialty fellowship programmes previously unavailable in the region. In several instances, guest exchanges allowed for trainees and junior faculty to establish networks that assisted in training and research funding. A majority of senior faculty described guest faculty who were able to expand clinical care capacity through training and materials, such as the ability of one centre to perform peritoneal dialysis. The senior faculty also noted that guests appeared to learn as much as they taught. A few faculty members spoke of the benefits of ongoing relationships with guest faculty, including networking, mentorship and resulting camaraderie.
What was effective and what was challenging?
Stories about effective guest faculty visits were often mirrored by stories of challenges within the same theme, and subthemes often were identified under multiple, sometimes overlapping, themes (figure 1).
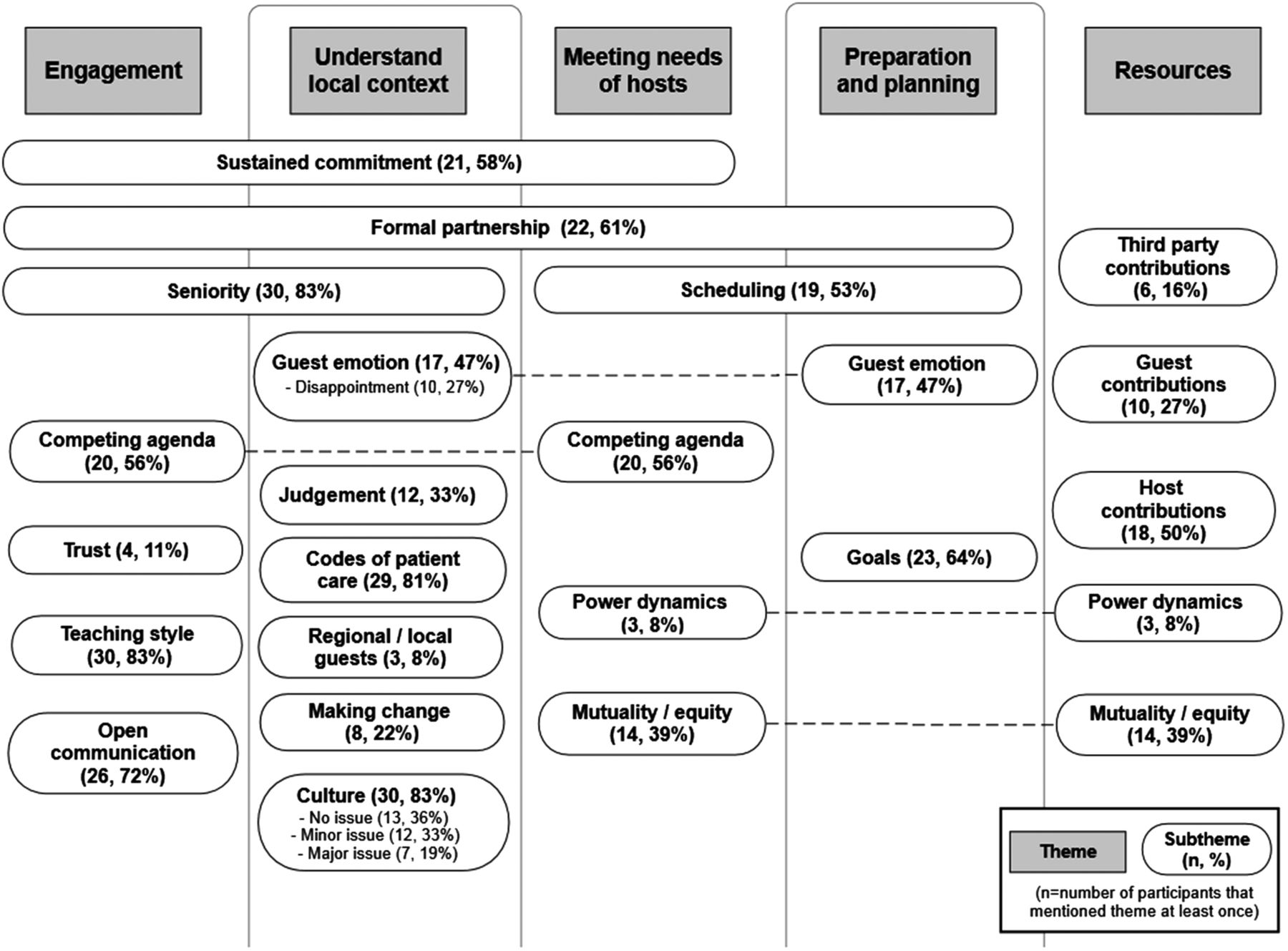
{kind=link}
Themes and corresponding subthemes of factors affecting guest faculty effectiveness.
Engagement
Guest faculty who made longer or repeat visits were viewed as more effective across subgroups (table 3). Short visits were occasionally appropriate for sharing specific desired expertise; however, most respondents described short visits (defined by them as a few days up to 2 weeks) as disruptive and of minimal benefit. Repeat visits were viewed as the most effective.
Quotes on engagement
A majority of faculty members noted challenges of competing visit agendas. Fifteen faculty members described guest faculty interactions that were limited by other academic focuses such as research, and 10 faculty members described guests whose primary goal appeared to be vacation and to ‘see Africa’. This subtheme was strongly linked to resources, with many hosts unwilling to request much of guests who were on personal leave and self-funding their visit.
Fourteen respondents preferred the expertise of more senior guests, and some institutions only approved senior faculty visits. However, 11 individuals felt that there was no difference in efficacy of junior versus senior guests. The junior faculty's lack of experience was offset by flexible schedules allowing for longer stays, increased adaptability, fewer competing agendas and increased engagement in clinical teaching.
Many residents and a few faculty members appreciated the collegial learning environment created by some guests, in contrast to the host institution's more hierarchical approach. Similarly, they noted the significant time that guest faculty spent with trainees. Increased engagement led to partnerships characterised by friendship, open communication and trust. While formal evaluations of guest faculty visits were rare unless required by a third party, respondents noted that strong relationships with guest faculty allowed for reciprocal constructive feedback.
Guest understanding of local context
Almost all host faculty and residents described frustrations with guests who had minimal experience in limited resource settings, and who lacked pertinent clinical knowledge. Some guests framed discussions about patient management in a way that placed the burden of resource limitations on the host (table 4).
Quotes on understanding local context
Almost half of all respondents across the three subgroups told stories of guest emotional responses to clinical resource limitations. A third of respondents described emotions causing major conflict or resulting in guests leaving early, and a minority of junior faculty and small majority of senior faculty described judgemental responses by guest faculty. A third of the faculty and residents described some guests as ‘disappointed’, stemming from a lack of clinical resources, the slow pace of change or the guests’ own sense of inefficacy.
With the exception of frustration around limited clinical resources, the majority of the respondents reported that cultural differences rarely led to significant conflicts. A third of the respondents indicated that culture was no issue, as either the guests themselves were worldly and well-travelled, or the hosts ‘have seen a lot and are quite accommodating’. Another third of the respondents described minor cultural differences which were recognised but did not create much conflict, such as guests’ focus on timeliness, direct communication with trainees and patients and informal dress.
Seven respondents described cultural differences that resulted in major conflict, many of which pertained to patient care including when resuscitation was appropriate, disclosing information to paediatric patients or obtaining parental consent. In these stories, host faculty acknowledged having a more ‘paternalistic'approach to medical decisions, while guests desired direct engagement with parents and patients. The other major conflicts involved guests’ direct and sometimes emotional communication styles when providing feedback, which was perceived by the hosts as ‘blunt or rude.’
Meeting needs of hosts
Scheduling visits appropriately was a concern for a majority of the faculty and residents (table 5). Fitting guests into an ongoing curriculum was challenging, particularly for institutions which relied on guests to teach specific subspecialties. Shared planning of the curriculum worked best, with challenges described when guest faculty did not cover the requested topics. A few faculty members described challenges managing multiple guests from different institutions who visited simultaneously.
Quotes on meeting needs of hosts
Faculty respondents described formal partnerships as most helpful in ensuring that guest faculty visits met the host's needs Within formal partnerships, there was mutual planning for shared goals, clearer expectations on both sides, better evaluation for impact and host faculty maintained greater control over guest visits and resulting teaching.
A majority of the senior faculty spoke of a lack of mutual expectations of host and guest faculty. Several faculty members illustrated this concept with stories of guests who arrived uninvited and expected to work clinically while understanding that would never occur in their home institutions. Several host faculty noted a need for more reciprocal faculty exchanges. Only five respondents described having partnerships where trainee or faculty exchange was bilateral.
Resources
Lack of host resources for guest visits was a substantial challenge noted by almost all faculty members and a minority of residents. Many respondents indicated that they would appreciate having more guest faculty but did not have adequate resources to host them. Guests’ provision of time and funding for visits altered the power dynamic such that some hosts felt unable to control the flow of guests (table 6). Even within formal partnerships, host institutions sometimes strained to provide agreed on lodging or transportation.
Quotes on resources and preparation
Preparing for and incorporating guests
Almost all respondents described collaborative planning efforts as vital to the efficacy of a guest's visit. A majority of the faculty suggested that effective visits require jointly determining the goals, and subsequently deciding appropriate visit length and frequency. Depending on the goals, they could establish a formal partnership which allowed for more accountability, mutuality and equity, and ability to seek third party funding. Partnership development, described by a few senior and junior faculty members, was often a dynamic process beginning with one visit and evolving into more substantial programming as the relationship grew.
Senior host faculty felt they could improve guest efficacy if they appropriately selected guests for expertise and experience. At one institution, multiple senior faculty members described purposely orienting guests and assigning host faculty or administrative contacts to mitigate the guests’ potential emotional responses. A few faculty members proposed inviting more regional faculty as guests.
Discussion
Our resulting themes and stories that were shared point to a struggle of ambivalence, with respondents recognising the advantages of hosting guest faculty, but also identifying situations where it was not beneficial, with hosts having to mitigate associated problems. In some instances, the burden of hosting guests went beyond resources and administration, and involved strained relationships and conferred guilt. We heard many stories of gaps in understanding between guests and hosts. While the overall themes are reflected in the existing literature on global health and cultural competencies, several new threads emerged that are important to making faculty visits effective and equitable.
Who should be guest faculty?
Whether guest faculty stayed for years, or gave a single lecture, visits were most valued if the goals were agreed on and tailored to the host institution. Visit duration and guest selection for expertise were dependent on those goals. While wisely recognising that ‘before you come the second time, you must have the first time,’ faculty struggled to determine which guests might become true collaborators. Institutions most needing guests to ‘fill gaps’ often relied on guests to fund visits and consequently accepted some visitors who were more of a drain than a benefit. Moving away from a ‘beggars cannot be choosers’ mentality requires addressing significant resource inequalities to empower host institutions to screen potential guest faculty as some more established programmes already do. More inquiry is needed to determine what degree of stringency is warranted to deter medical tourism and needless diversion of resources, but also allows for initial visits from less experienced guests who may grow to become beneficial partners.
Our respondents most appreciated guests who could dedicate themselves to building relationships via a sustained commitment. Experience in global settings and adaptability were both prized. While senior guests were acknowledged to have more experience and more knowledge to share, they were often perceived as less available, less adaptable and having more competing agendas than junior guest faculty. Several of our respondents spoke of the desire to select guests with specific expertise that was needed by their institution, which is unsurprising given the lack of paediatric subspecialists in many parts of the globe. Sending and hosting institutions should be mindful of guest selection depending on the goal of the faculty exchange, and potential guests should themselves consider if they are appropriate for the suggested role.
Several respondents noted that the ‘guests’ were always westerners. Lack of host resources may limit potentially fruitful regional collaborations and desired bilateral exchanges. Literature on ethical partnerships does point to the need for bilateral exchange; however, funding remains a significant barrier, and concurring with our participants’ experiences, true bilateral exchange and ‘south-south’ exchanges remain infrequent.22 ,23
Cultural differences over resource limitations
We were surprised that two-thirds of the respondents reported that cultural differences were rarely a cause for conflict during faculty visits. Most of the described conflicts involved guest faculty who were emotional, judgemental or aggressively seeking change in response to perceptions of poor quality care. This friction often stemmed from guests’ inexperience when confronting true clinical resource limitations. Cultural differences that were anticipated—such as differences in dress—were much better tolerated.
The literature around global health and culture distinguishes between cultural competency, meaning knowledge of different cultures and cultural humility, defined in recent literature as ‘having an interpersonal stance ie, other-oriented rather than self-focused, characterised by respect and lack of superiority toward an individual’s cultural background and experience’.24–26 An inexperienced guest's desire to advocate for each individual patient and improve systems of care may put them in conflict with local providers with a more global view of the community's needs and resources. An approach of cultural humility and learning how to affect change in that specific setting allows for more collaborative approaches to achieve those same goals.
While most global health competencies include domains focused on culture, communication and professionalism, these are challenging areas to assess.18 ,19 ,21 Both sending and hosting institutions need more effective methods to identify guest faculty who may have difficulty adjusting to work in resource-limited settings. More inquiry is needed into effective preparation for global health work, particularly regarding development of adaptability and cultural humility. One novel programme for paediatric residents uses simulation to elicit emotional responses to working with limited clinical resources.27 Much of the literature about global health electives encourages mandated preparation for medical trainees and opportunities for debriefing after travelling.28 ,29 Such systems are generally less available for faculty members who may have less institutional support for global work.
While evaluation was considered important, our respondents indicated that there were few if any established formal feedback systems. Several respondents mentioned reports written by guests about the host institution following a visit. Most feedback to guests was informal, predicated on either previous formation of strong interpersonal relationships or individual guest faculty seeking feedback from residents. A few third party organisations that arranged faculty exchanges required formal guest evaluations. It is unclear if lack of feedback stemmed from a culture of politeness towards guests, or differentials in access to resources and resulting power imbalances; however, some faculty members did note that joint evaluation was a benefit of formal partnerships. We suggest that a system of feedback to guest faculty should be incorporated into all visits. Such a system would aid hosts in deciding whether to invite a particular guest faculty member for a return visit, and may help guest faculty be more effective on subsequent visits. In the context of partnerships, institutional exchange of feedback may facilitate improved processes in selecting and preparing guest faculty and encourage institutional ownership on the part of sending institutions to address negative feedback with ineffective faculty.
Challenges posed by power imbalances
Power imbalances are a clearly acknowledged friction in developing effective global health partnerships.13 ,30–33 In a review of partnerships for global health research, Bradley declared that “asymmetry between partners remains the principal obstacle to productive research collaboration.”34 In 1998, the Swiss Commission for Research Partnerships with Developing Countries (KFPE) proposed 11 principles for research partnerships, and many such as deciding on objectives together, building mutual trust, sharing information and monitoring and evaluating the collaboration were reflected in our findings.35 The Canadian Coalition for Global Health Research has developed a partnership assessment tool to assist partners in developing and maintaining equitable and effective partnerships, which also promotes an early focus on developing mutual goals and clear roles for both partners.36 While remarkably similar principles for good partnership have been promoted in global health research over the past few decades, our results are evidence that the implementation of these principles is inadequate given the experiences of guest faculty visits as described by our respondents.
Our results corroborate the need to carefully consider the downstream effects of sourcing funds for faculty visits.36 When hosts lacked control over visit resources, the resulting power imbalances limited the hosts' ability to invite guest faculty with desired expertise. This effect was more pronounced for smaller programmes that had a greater need of guest resources. This resource imbalance affected mutuality even in long-term partnerships as evidenced by the lack of desired bilateral exchange. The Medical Education Partnership Initiative, which funded partnerships between medical schools in the USA and Africa, was exemplary in granting host institutions greater control over resources and goals to allow for better alignment of visits with host institutions' needs and more mutual and efficacious partnerships.37
A few senior faculty members also remarked on the need for their own programmes to be more directive and specific regarding their institutional goals. Host articulation of a clear strategic plan may allow for better alignment of guests with host goals, promoting more effective visits and less frustration on both sides. While a formal partnership was often viewed as the means to aligned goals, the preferential focus should be the goals of the hosts. The host establishing specific goals even prior to developing a partnership may also make for better institutional partnerships, reduce the number of inoperative memorandums of understanding and allow for joint efforts in pursuing resources to meet those goals, thus further improving balance in power.
Limitations and strengths
This research was undertaken in East Africa, with guest faculty mostly hailing from the USA, Canada and Western Europe. As such, history and lingering colonial influence may affect both host and guest personal and institutional interactions. While similar influences are most likely present in other low-income countries seeking to expand medical education programmes, the specific context may alter the patterns of interactions noted here. Our inquiry was also specific to paediatric programmes. Further research might explore if these themes hold true for visiting faculty in other subspecialties and settings.
Our author group includes those with experience as guest and host faculty from each of the three participating countries, representing a strength, and also potentially introducing biases. The interviews were carried out by a Kenyan physician researcher. We believe her shared culture in medicine, along with providing confidentiality and anonymity, allowed the respondents to speak freely about their experiences.
Conclusion
Strengthening graduate medical education is a necessary step towards decreasing inequalities in healthcare around the globe. Guest faculty can aid in expanding capacity of paediatric academic centres in low and-middle income countries; however, effective visits require: (1) mutually agreed on goals with appropriate scheduling, visit length and commitment to ensure that the visits meet the host's needs, (2) careful selection and preparation of guest faculty to meet the host's goals, (3) emotional preparation by prospective guests along with host orientation to clinical work in the host's setting, (4) attention to funding sources for the visit and mitigation of resulting power differentials and (5) mutually agreed on methods for bilateral evaluation. Formal partnerships may improve mutuality of faculty exchanges, mitigate inherent power imbalances and allow for more sustained, trusting and open relationships.
Acknowledgments
The authors would like to thank David N Williams for his invaluable assistance in the design and analysis and reporting of the study, Linda Barnes for training in qualitative interview techniques, and Duncan Maru, Jonathan Borus and Ramnath Subbaraman for their insightful editing.
References
Footnotes
Handling editor Seye Abimbola
Contributors CMR substantially contributed to study conception and design, to acquisition, analysis and interpretation of data, drafted the manuscript, critically revised the manuscript and gave final approval for the manuscript to be published. LG and DM substantially contributed to study conception and design, to acquisition, analysis and interpretation of data, critically revised the manuscript and gave final approval for the manuscript to be published. MS substantially contributed to data analysis and interpretation, critically revised the manuscript and gave final approval for the manuscript to be published. EK substantially contributed to study conception and design, critically revised the manuscript and gave final approval for the manuscript to be published. SB-K and AL substantially contributed to study conception and design, to acquisition and interpretation of data, critically revised the manuscript and gave final approval for the manuscript to be published. All the authors agree to be accountable for all aspects of work ensuring integrity and accuracy.
Funding This study was funded by grants from the Global Pediatric Education Consortium and the Boston Children's Hospital Global Pediatrics Program.
Competing interests None declared.
Ethics approval This study was reviewed and approved by Boston Children's Hospital IRB, Kenyatta National Hospital/University of Nairobi Ethics Review Committee, Research and Ethics Committee of Makerere University College of Health Sciences, Uganda National Council for Science and Technology, Muhimbili University of Health and Allied Sciences Directorate of Research and Publications, and Tanzania Commission for Science and Technology.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.
↵i Umeå University, Umeå, Sweden.