Article Text

Abstract
Context South Africa has the most HIV infections of any country in the world, yet little is known about the adolescent continuum of care from HIV diagnosis through viral suppression.
Objective To determine the adolescent HIV continuum of care in South Africa.
Data sources We searched PubMed, Google Scholar and online conference proceedings from International AIDS Society (IAS), International AIDS Conference (AIDS) and Conference on Retrovirology and Opportunistic Infections (CROI) from 1 January 2005 to 31 July 2015.
Data extraction We selected published literature containing South African cohorts and epidemiological data reporting primary data for youth (15–24 years of age) at any stage of the HIV continuum of care (ie, diagnosis, treatment, retention, viral suppression). For the meta-analysis we used six sources for retention in care and nine for viral suppression.
Results Among the estimated 867 283 HIV-infected youth from 15 to 24 years old in South Africa in 2013, 14% accessed antiretroviral therapy (ART). Of those on therapy, ∼83% were retained in care and 81% were virally suppressed. Overall, we estimate that 10% of HIV-infected youth in South Africa in 2013 were virally suppressed.
Limitations This analysis relies on published data from large mostly urban South Africa cohorts limiting the generalisability to all adolescents.
Conclusions Despite a large increase in ART programmes in South Africa that have relatively high retention rates and viral suppression rates among HIV-infected youth, only a small percentage are virally suppressed, largely due to low numbers of adolescents and young adults accessing ART.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known about this topic?
The incidence of HIV infection among adolescents and young adults in South Africa is high.
Perinatally HIV-infected children are ageing to adolescence and young adulthood.
Adolescents and young adults have lower retention in care and lower viral suppression rates than older adults.
What are the new findings?
There are an estimated 720 000 HIV-infected youth aged 15–24 in South Africa.
Overall 10% of HIV-infected youth in South Africa are virally suppressed.
Among the estimated 867 283 HIV-infected youth aged 15–24 years in South Africa in 2013, 14% accessed antiretroviral therapy (ART).
Of those on therapy, approximately 83% were retained in care and 81% were virally suppressed.
Recommendations for policy
Increasing antiretroviral treatment in adolescents and young adults.
Improving adolescent-friendly services to increase retention and viral suppression rates.
Preparation and planning for transition care for HIV-infected youth.
Introduction
South Africa has the highest number of HIV infections of any country in the world with an estimated 6.8 million total infections.1 Access to antiretroviral therapy (ART) did not begin until 2004, a delay that contributed to high numbers of perinatal HIV infections in the late 1990s and early 2000s.2 Even with the implementation of the South African National Antiretroviral Treatment Programme, enrolment was slow due to political, cultural, infrastructure, geographic and economic issues.3 ,4 Many perinatally HIV-infected infants died during the delays in ART rollout.3 ,5
With improved access to ART, perinatally HIV-infected infants are surviving into adolescence and early adulthood.2 At the same time, adolescents and young adults, particularly females aged 15–24, have a high incidence of new HIV infections.6 These two groups, perinatally infected and non-perinatally infected adolescents and young adults, make up a significant portion (11%) of South Africa's total number of HIV infections.
Now, with more than 10 years of an established national ART programme and its increased scale up in recent years, South Africa has the largest national ART programme in the world.2 ,7 Backed by emerging evidence, national ART guidelines support earlier initiation of ART with simpler, more potent and less toxic regimens leading to increased numbers of individuals accessing treatment.8 The scale-up has contributed to high levels of viral suppression, lower mortality rates and decreased HIV transmission among large adult populations in South Africa.2 ,9–11
Several groups have evaluated the continuum of HIV care (from HIV infection to diagnosis, linkage to care, retention in care, ART initiation and viral suppression) in adults from resource-rich countries. Analyses indicate that only a small number of HIV-infected individuals are fully benefitting from therapy.2 ,12–14 In sub-Saharan Africa, ∼24% of HIV-infected individuals successfully navigate the continuum of care and are virally suppressed.2 An analysis of the adolescent and young adult continuum of care in the USA estimated that only 6% of HIV-infected youth were virally suppressed.13 The continuum of care for HIV-infected adolescents and young adults in South Africa has not previously been described.
The purpose of this analysis is to assess the number perinatally and non-perinatally HIV-infected adolescents requiring ART and surviving into adulthood. Preparing for this growing population has major implications for South Africa's national treatment programme, including the need for adolescent-friendly HIV prevention and treatment programmes as well as transition to adult services for HIV-infected youth.
Below, we present the results of a systematic review estimating the number of adolescents and young adults infected with HIV in South Africa, the number of those on ART and HIV-related mortality. In addition, we report results from our meta-analysis on the percentage of HIV-infected adolescents in South Africa who are retained in care and virally suppressed.
Methods
We searched PubMed, Google Scholar and online conference proceedings from the International AIDS Society (IAS), the International AIDS Conference (AIDS) and the Conference on Retrovirology and Opportunistic Infections (CROI) from 1 January 2005 to 31 July 2015. Key words and medical subject headings relevant to age (ie, adolescent, adolescence, teen, youth, young adults) were cross-referenced with terms associated with the HIV continuum of care (ie, retention, loss to follow-up, viral suppression, ART, virological failure, outcomes and transition). We sought unpublished data from the South African Department of Health and major academic centres in Johannesburg, Durban, Pietermaritzburg and Cape Town. We reviewed literature in English reporting primary observational data from South African cohorts or epidemiological studies that included specific age ranges, including adolescents and young adults within our target age group of 15–24 years. We attempted to contact the corresponding authors of studies that included ages outside of this range. Because studies reported variable age ranges, we included studies in our analysis that reported primary data on youth, including the ranges of 15–24 years. We report age ranges as described by the original authors; therefore, this analysis includes adolescents and young adults as young as 9 years old and as old as 29 years old due to different binning of age groups by original authors.
We used epidemiological data from South African HIV antenatal HIV prevalence rates, reported number of live births and estimated mother-to-child HIV transmission rates to estimate the annual number of HIV-infected infants born each year in South Africa.
In our meta-analysis, we calculated pooled proportions, with corresponding 95% CIs, for retention in care and viral suppression using the DerSimonian and Laird Random Effects (RE) model, with double arcsine transformation to stabilise the variance.15 ,16 Meta-analyses were performed in MetaXL (V.3.1, EpiGear International, Queensland, Australia) (Barendregt JD, Doi SA. MetaXL User Guide. 2015;Version 3.1). Heterogeneity was assessed with the I2 statistic.17 We planned analyses by relevant subgroups, focusing on age groups and study endpoints, to examine anticipated variation in the outcomes of interest.
Findings
Our systematic review found 119 relevant articles in the published literature addressing the continuum of care for HIV-infected adolescents in South Africa. As indicated in figure 1, 78 were excluded due to insufficient primary data reported; 15 were excluded since they contained only adult data; eight were excluded for only including paediatric data (with ages <15 years); seven were excluded since they reported cohorts outside of South Africa and an additional four were excluded since they did not report results for the ages 15–24 in the primary outcomes. We searched 1266 conference abstracts from IAS/AIDS and CROI from 1 January 2005 to 31 July 2015 and found 12 that included primary data from South African cohorts involving adolescent retention or viral suppression. Six of these studies were excluded for insufficient primary outcome data. Overall, there were 13 sources that contained sufficient data to be included in the meta-analysis with two studies containing both retention and viral suppression data.
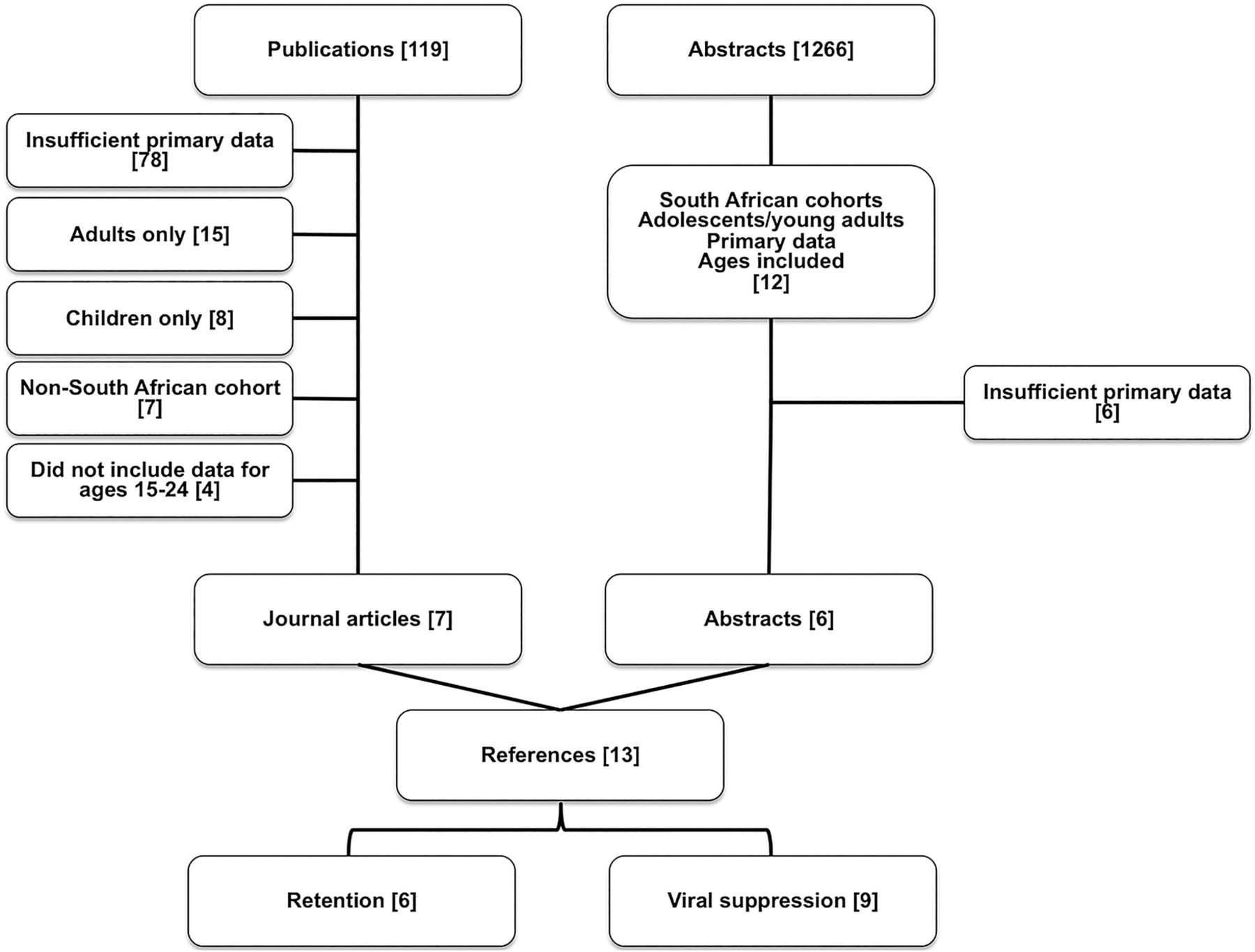
Flow diagram of literature reviewed for meta-analysis of retention in care and viral suppression for HIV-infected adolescents and young adults in South Africa published or presented between 1 January 2005 and 31 July 2015.
Systematic review
Overview of HIV Infections among Adolescents and Young Adults in South Africa.
Currently, HIV-infected adolescents and young adults in South Africa are a combination of two separate epidemics, perinatally HIV-infected youth and newly acquired HIV among adolescents and young adults. The South African National HIV Prevalence, Incidence, and Behavior Survey in 2012 estimated that up to a total of 720 000 youth aged 15–24 are infected with HIV.6 By 2013 statistics, South Africa estimated that 8.5% of the estimated 10 203 329 adolescents and young adults aged 15–24 were infected with HIV totalling 867 283 infections.18 Joint United Nations Programme on HIV/AIDS (UNAIDS) estimated there were 320 000 HIV-infected adolescents aged 10–19 in 2013.19 These estimates contain both perinatally infected and non-perinatally infected youth; however, they do not extrapolate on the percentages in each category.
Perinatal infections
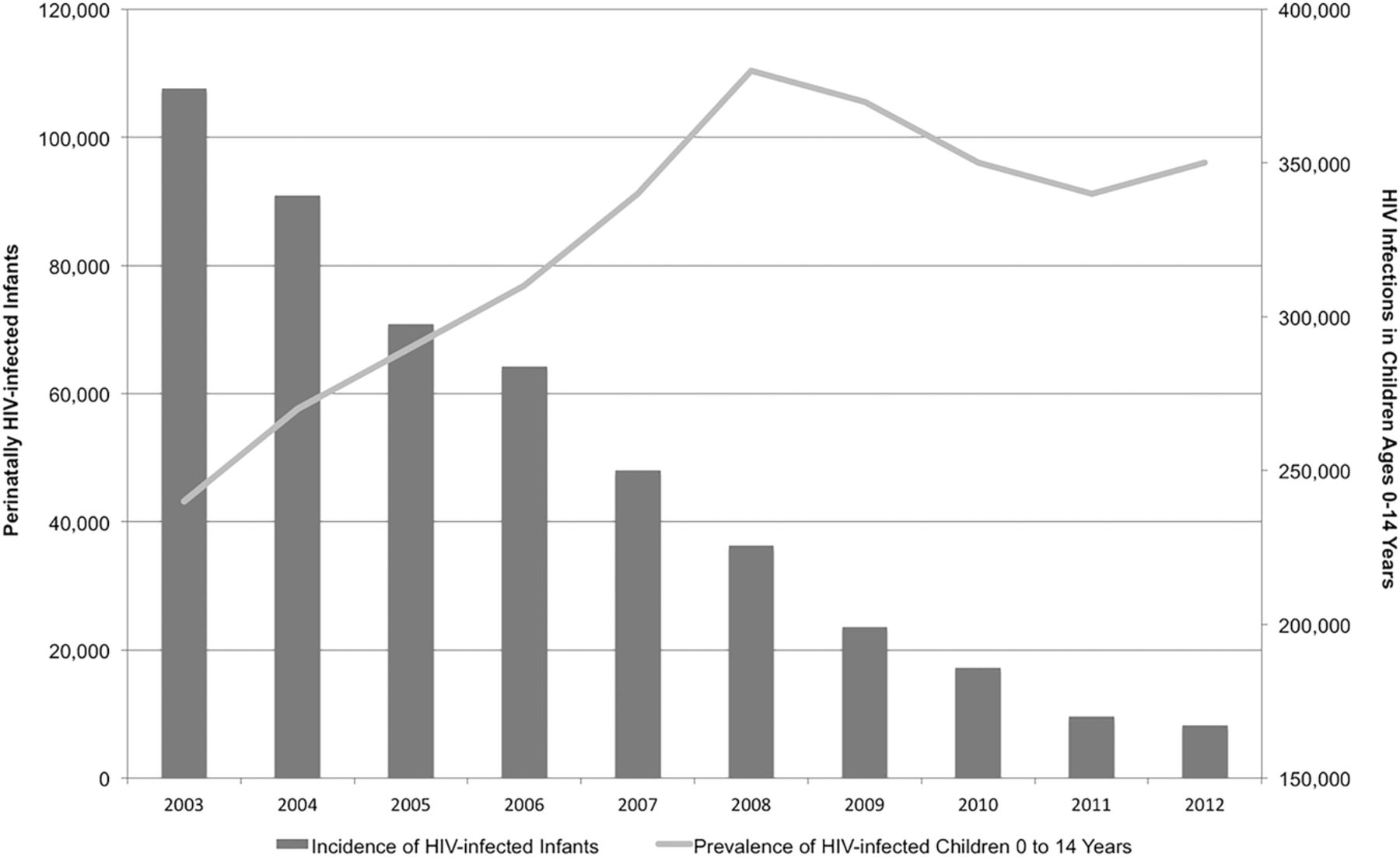
In 2003, before the implementation of the South African National HIV Treatment Programme, national HIV prevalence among women attending antenatal clinics was 27.9%; yet, the number of pregnant women who tested for HIV was <50%.20 ,21 Low testing rates and limited prevention of mother-to-child HIV transmission (PMTCT) services led to a mother-to-child HIV transmission rate of 23% in 2003.22 With 1 677 415 infants born in South Africa in 2003,21 ,23 this translates to 107 639 newly HIV-infected infants. By 2005, after ART became available in South Africa, the national HIV antenatal clinic prevalence rate rose to 30.2%, but the mother-to-child transmission rate decreased to 17%. The 1 380 496 births in 2005 translated into 70 875 newly HIV-infected infants. By 2012, the expansion of ART services and PMTCT, including updated PMTCT guidelines in 2008 and 2010, led to decreasing mother-to-child HIV transmission rates (2.4%); however, with 1 168 403 births and a 29.5% antenatal clinic prevalence rate, this translated into 8272 newly HIV-infected infants.6 ,7 ,21 ,24 The decline in infections from 2003 to 2012 represents a 92% reduction in new paediatric HIV infections in 9 years, as indicated in figure 2.6 ,7 ,21 Since the rollout of ART in South Africa, there has been a steady decrease in the mother-to-child transmission rate. UNAIDS estimated that in 2014 there were 65 000 averted perinatal HIV infections by PMTCT in South Africa.1
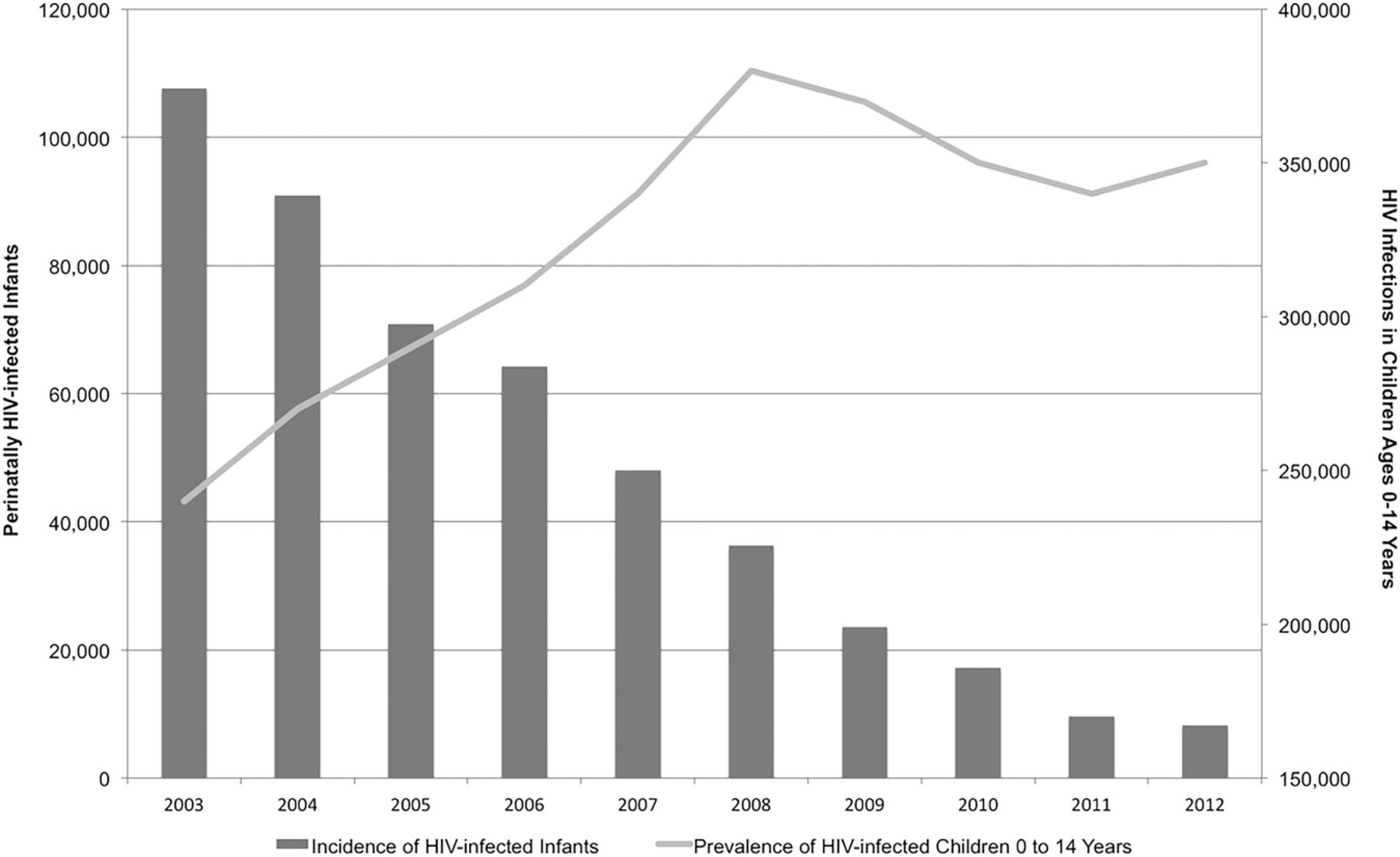
Systematic review: Perinatally HIV-infected infants in South Africa, total HIV-infected children aged 0–14 and the approaching wave of HIV-infected adolescents expected to enter adult care by 2023.
Incidence of HIV among adolescents
A national survey in 2012 estimated that 139 000 new infections occurred among youth aged 15–24.6 The number of new infections disproportionally affects females who account for 81% of these new infections.6 The overall HIV incidence was 2.5 in females aged 15–24 compared with 0.6 for males of the same age.6
Antiretroviral therapy
In 2012, a nationally representative survey conducted in South Africa estimated 103 000 (95% CI 72 000 to 144 000) youth aged 15–24 were on ART, comprising 14% of HIV-infected adolescents in South Africa and 1.5% of South Africans on ART.6 Estimates in large urban academic centres in Johannesburg, Cape Town and Durban have differing percentages of their total ART programme that are comprised of adolescents: Johannesburg at 6.7% for those aged 15–24; Cape Town at 0.8% for those 12–17 and Durban 11.1% for those aged 10–19 (M Archary. KwaZulu-Natal Adolescent ART data. Personal Communication 2015; D Evans. Themba Lethu Clinic Adolescent Data. Personal Communication 2015; C Orrell. Masi and Gugulethu Adolescent Data. Personal Communication 2015). Based on 2013 population estimates, we estimate that 124 070 (14%; 95% CI 10% to 20%) adolescents and young adults aged 15–24 in South Africa are receiving ART (figure 4).
Meta-analysis
Retention in care
Results of our meta-analysis of six studies estimate that the proportion of South African HIV-infected adolescents on ART who were retained in care within the first 1– 2 years of therapy is 83% (95% CI 68% to 94%; I2=99%), as indicated in table 1 and figures 3A and 4.25–30 No differences were seen when comparing this proportion by timing end point or age group.
Published literature from 1 January 2005 to 31 August 2015, addressing the continuum of care for HIV-infected adolescents and young adults in South Africa
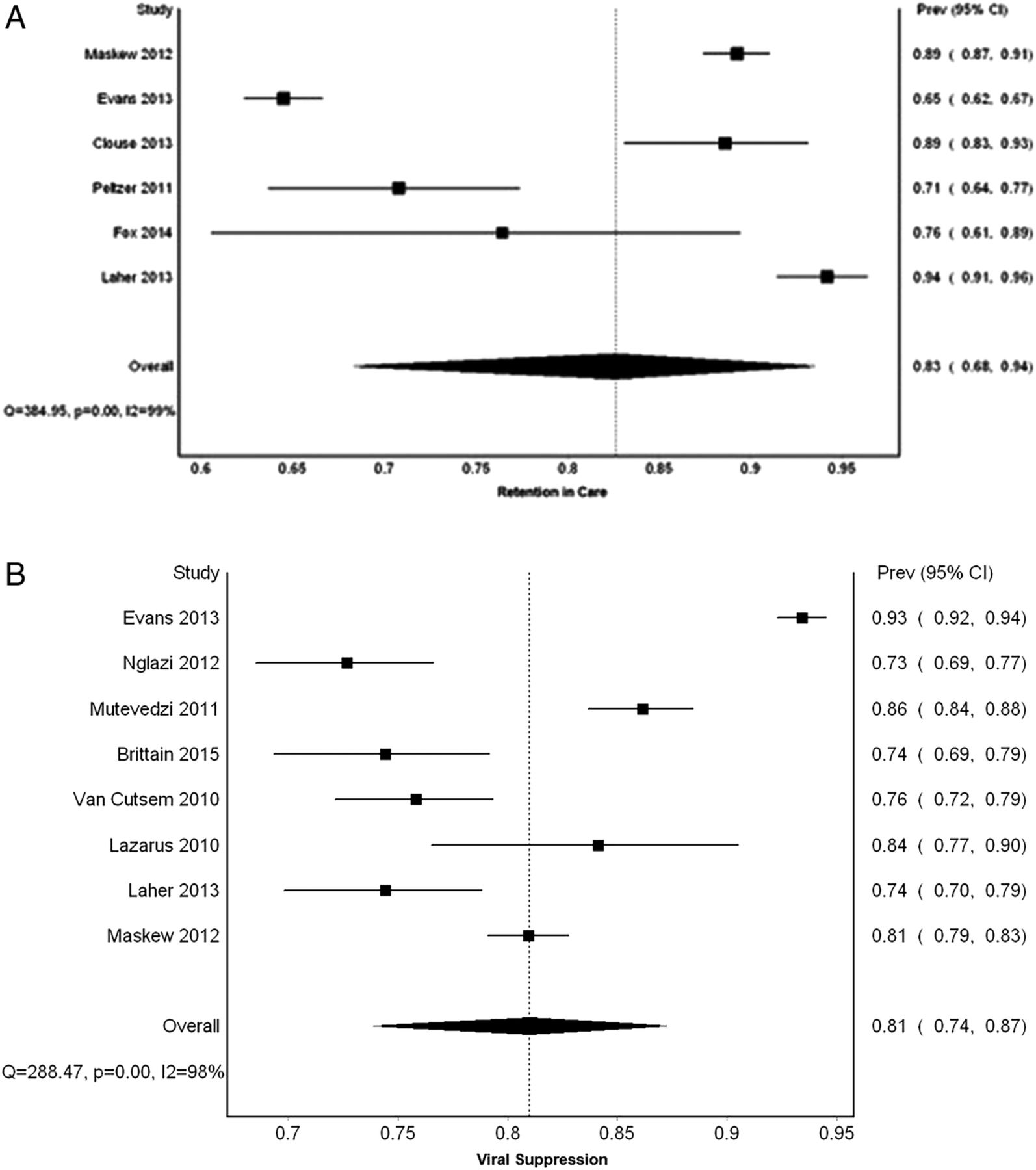
(A) Meta-analysis retention: Forest plot of the proportion of HIV-infected adolescents and young adults in South Africa retained in care. (B) Meta-analysis viral suppression: Forest plot of the proportion of virally suppressed HIV-infected adolescents and young adults in South Africa.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Estimate of the absolute number of South African HIV-infected adolescents and young adults aged 15–24 completing the HIV continuum of care.
Viral suppression
Based on our meta-analysis of eight studies, we estimate the proportion of South African adolescents and young adults on ART who were virally suppressed to be 81% (95% CI 74% to 87%; I2=98%), as indicated by table 1 and figures 3B and 4.26 ,28 ,29 ,36–39 ,41 No differences were seen when comparing this proportion by timing end point or age group.
Mortality
Globally, from 2005 to 2012, the overall number of HIV-related deaths decreased by 30%; however, deaths in HIV-infected adolescents over the same time period increased by 50%.42 In 2013, in South Africa alone, there were more than 9500 deaths among HIV-infected adolescents.19 Despite having low ART initiation rates, lower retention in care and more virological failure, multiple cohorts in South Africa did not see an increase in mortality rates among adolescents and young adults in care and on ART.25 ,26 ,30 ,36 ,43–48
Discussion
South Africa has had a dramatic increase in the number of HIV-infected individuals on ART in the last several years; however, the percentage of adolescents fully benefiting from treatment remains low. Compared with HIV-infected adolescents in the USA, South Africa has a lower percentage of youth receiving ART treatment (14% vs 25%), yet it does have similar rates of retention in care (11% vs 11%) and higher rates of viral suppression (10% vs 6%).13 ,49 South Africa also has a higher number of infections at 867 283 compared with 78 949 in the USA. Despite a higher viral suppression rate, 709 773 more adolescents are not virally suppressed in South Africa compared with the USA. Descriptions of the continuum of care for HIV-infected adolescents in others settings have not been described, limiting further comparisons.
South African studies with direct comparison between adolescents and adults indicate lower retention and viral suppression among youth. Six studies in South Africa documented significantly poorer retention in care rates for adolescents compared with adults with ORs ranging from 1.55 to 2.25.25 ,26 ,33 ,34 ,38 ,50 For example, a large cohort from Gauteng and Mpumalanga with more than 42 000 patients showed retention rates for adolescents aged 15–24 at 65% compared with adults over 25 years of age at 78%.26 Five separate South African observational cohorts reported significantly lower HIV viral suppression rates among adolescents and young adults (range: 73–93%) after ART initiation compared with adults (range: 88 –97%).26 ,36 ,38 ,50 ,51
Despite HIV-infected adolescents having lower rates of retention in care and viral suppression rates compared with adults, mortality rates among adolescents in comparative studies are similar to adults.25 ,26 ,30 ,36 ,43–48 This likely reflects the delayed mortality in newly HIV-infected youth that die after ageing into adulthood. With high retention and viral suppression rates among adolescents in South Africa, strategies to improve HIV diagnosis and early ART initiation in adolescents could drastically improve the continuum of care for youth in South Africa.
Low ART treatment rates among adolescents currently are inversely related to the high number of new HIV infections in this age group. Youth who are newly infected are less likely to qualify for ART based on National HIV Treatment Guidelines (CD4 below 500 cells/mm3 at the time of this writing) due to asymptomatic disease and higher CD4 counts.52 The cohort of sexually active, HIV-infected and viremic youth could have a large impact on HIV transmission rates in South Africa and warrants consideration for public health investment.
Expansion of proven treatment and prevention programmes for adolescents and young adults could reduce the high incidence of HIV infections in this age group. Recent evidence has shown the benefit of test-and-treat strategies for prevention of HIV regardless of clinical stage or absolute CD4, assuming individuals stay in care.53 Clinical evidence is also building for initiation of ART at higher CD4 counts.54 ,55 Recently, the WHO recommended universal treatment for HIV-infected individuals, including adolescents and young adults.52 ,56 ,57 In addition, pre-exposure prophylaxis, recently endorsed by the WHO, has been shown to decrease HIV transmission in several cohorts and may be useful in people engaging in high-risk sexual behaviour.57–60 However, concern about poor adherence among adolescents suggests that this strategy will require careful planning, monitoring and research.
The high HIV incidence rate among South African females aged 15–24 in particular calls for HIV prevention efforts in this group. Incidence rates for all other age groups have decreased over the past decade; however, incidence remains steadily high in females aged 15–24.2 ,6 The risk of HIV acquisition among adolescent females is thought to be higher if there is a greater than 5-year difference in the age between female and male sexual partners.6 ,61 Several studies suggest that this age discrepancy is driven by sexual relationships between older males and younger females as transactional sex.62–70 However, a recent study from rural KwaZulu-Natal, South Africa did not see an increase in HIV incidence among younger females with older male partners.71
There is an expected oncoming wave of perinatally HIV-infected children ageing into adolescence who will require adult services in the next 5–10 years. Infants surviving and initiating ART in the mid-2000s are now transitioning into adolescence. Additionally, ∼25–30% of perinatally infected children are slow progressors who can survive undiagnosed and untreated well into adolescence.72 ,73 As this wave of perinatally HIV-infected adolescents mature, combined with the high number of new infections among older adolescents, a large number of adolescents will transfer from paediatric or adolescent-based clinics to adult services.74–77 These already overwhelmed institutions are poorly prepared for the increased patient population. In addition, these individuals have different needs from patients currently in care at adult services. With many chronic illnesses, this transition is often associated with lapses in adherence and poor clinical outcomes.78–81 Revolving care providers, lack of youth-friendly services, rigid scheduling and decreased adult caregiver involvement have marred this transition process.82–84 More research is needed to investigate optimal practices for transitioning HIV-infected youth to adult services.
This review has several limitations. First, it relies on published data and therefore could be subject to publication bias, likely biasing adolescents to lower rates at each step of the continuum of care. We did, however, obtain estimates of the continuum of care from primary data from several large urban settings in Durban, Johannesburg, Pietermaritzburg and Cape Town. In addition, this review relied on retrospective observational data, which were mostly from large urban centres. It is possible that this data is not representative and generalisable to adolescents in rural settings. The analysis for viral suppression assumes that all participants in each cohort are alive, in care and do not have missing data. Since this was a retrospective review of the literature, we were unable to include clinical data such as CD4 improvement, weight gain and documentation of opportunistic infections. There was also considerable heterogeneity in the estimates for retention in care and viral suppression, which could not be explained by the variation in study endpoints or age group. Additional efforts are needed to try and explore the sources of this heterogeneity.
Conclusion
The oncoming wave of HIV-infected adolescents entering adult care could put a strain on already limited resources. These adolescents have different needs than adults and have lower viral suppression and retention rates. More research must be conducted to optimise retention in care, ART treatment and transition care for HIV-infected adolescents in South Africa.
Acknowledgments
The authors would like to thank Thobekile Sibaya, Denise Evans and Catherine Orrell for assisting with data collection. They would also like to thank Holly Zanoni for her assistance with the figures and formatting.
References
Footnotes
Handling editor Seye Abimbola
Contributors BCZ conceptualised and designed the study, performed the literature review, assisted with the analysis, drafted the initial manuscript, reviewed and revised the manuscript and approved the final manuscript as submitted. SB and JEH carried out the initial analyses, reviewed and revised the manuscript and approved the final manuscript as submitted. MA and ITK provided information on data sources, method design and critically reviewed the manuscript and approved the final manuscript as submitted.
Funding BCZ is supported by the National Institute of Health (grant number 5T32AI 052074).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.