Article Text

Abstract
Background: Trends in cardiovascular risk factors among UK adults present a complex picture. Ominous increases in obesity and diabetes among young adults raise concerns about subsequent coronary heart disease (CHD) mortality rates in this group.
Objective: To examine recent trends in age-specific mortality rates from CHD, particularly those among younger adults.
Methods and results: Mortality data from 1984 to 2004 were used to calculate age-specific mortality rates for British adults aged 35+ years, and joinpoint regression was used to assess changes in trends. Overall, the age-adjusted mortality rate decreased by 54.7% in men and by 48.3% in women. However, among men aged 35–44 years, CHD mortality rates in 2002 increased for the first time in over two decades. Furthermore, the recent declines in CHD mortality rates seem to be slowing in both men and women aged 45–54. Among older adults, however, mortality rates continued to decrease steadily throughout the period.
Conclusions: The flattening mortality rates for CHD among younger adults may represent a sentinel event. Deteriorations in medical management of CHD appear implausible. Thus, unfavourable trends in risk factors for CHD, specifically obesity and diabetes, provide the most likely explanation for the observed trends.
Statistics from Altmetric.com
In the UK, mortality rates from coronary heart disease (CHD) have continued to decline steadily since the late 1960s.1 Improvements in population risk factors and in medical treatments for patients with CHD both contributed substantially to the declines seen between 1981 and 2000.2 Nevertheless, CHD remains the leading cause of death and exacts a heavy social and economic toll. Furthermore, concern has recently been expressed that in the USA the rate of decline in mortality from CHD has slowed during the 1990s compared with earlier decades.3
Does the UK risk following American trends? The increases in the prevalence of obesity and diabetes in the UK since the 1980s are potential warning signs that the hard fought gains in cardiovascular mortality improvements might be arrested or even reversed.4 5 Furthermore, the declines in total cholesterol concentrations during the 1990s have been modest, even though prescription of statins has escalated.6 7 Although tobacco use continues to decline, the adult prevalence of smoking still remains well above 20%; moreover, the large number of UK adults who are totally sedentary during leisure time has probably increased since the 1990s.7 As a result of these conflicting trends in the various risk factors, the earlier falls in deaths from CHD may soon be blunted.5
Unfavourable trends in some cardiovascular risk factors have been particularly worrying among younger adults. Between 1993 and 2003, some of the largest relative increases in obesity and diabetes have occurred among adults aged <45 years.7 Furthermore, mean concentrations of cholesterol have fallen little or even increased among some of the younger age groups.7 Moreover, the previous decline in smoking rates may be levelling off among young adults; the smallest reduction has been seen in men aged 25–34.8 Thus, it is reasonable to suggest that those adverse trends in CHD mortality rates may be detected first among young adults.
Although previous reports have emphasised the continuing declines in the age-adjusted CHD mortality rate among UK adults,1 trends in age-specific rates have received little attention. The objective of our study was therefore to examine trends in the age-specific rates for CHD among UK adults from 1984 to 2004, particularly among younger adults.
METHODS
Vital statistics data were obtained for the England and Wales population.1 4 We limited our analyses to people aged 35 years and older. The underlying cause of death from CHD was determined using the International Classification of Diseases (ICD)-9 codes 410–414 for 1984–98 and ICD-10 codes I20–I25 for 1999–2004. Population counts from the England and Wales census were used to calculate rates. We used census counts for the years 1981, 1991 and 2001 and between-census estimates for the other years. Age adjustment was performed using the direct method to the estimated England and Wales population of the year 2001.
Plots of rates on a log scale, and plots of annual absolute changes in the age-specific mortality rates were smoothed using 5-year moving averages. A joinpoint regression was fitted to provide the estimated annual percentage change and to detect points in time at which significant changes in the trends occur (Joinpoint software, version 3.0), and we used a Bayesian information criterion (BIC) approach to select the most parsimonious model that best fitted the data.9 10 A maximum number of three joinpoints was allowed for estimations. For each annual percentage change estimate, we also calculated the corresponding 95% confidence interval (95% CI).
RESULTS
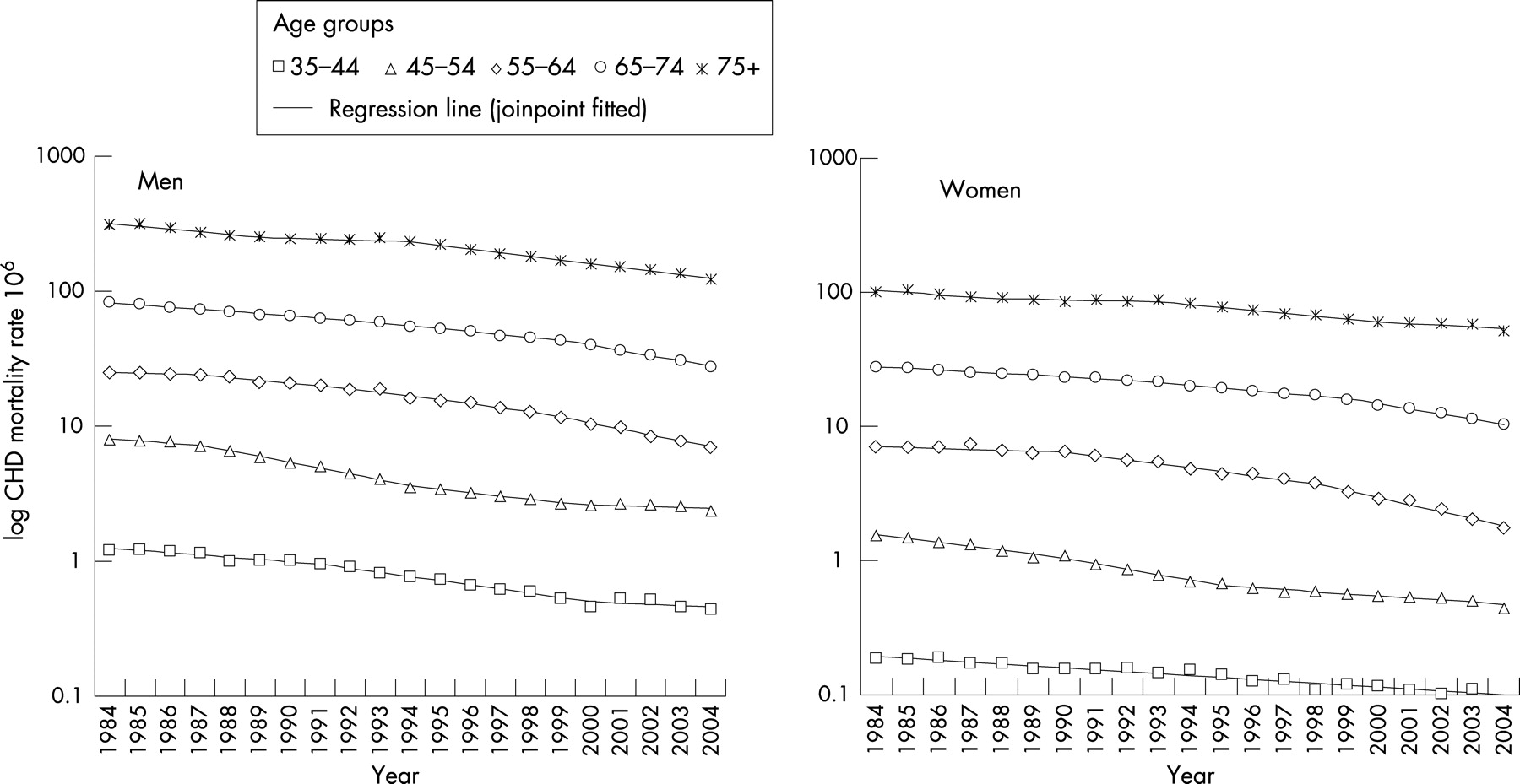
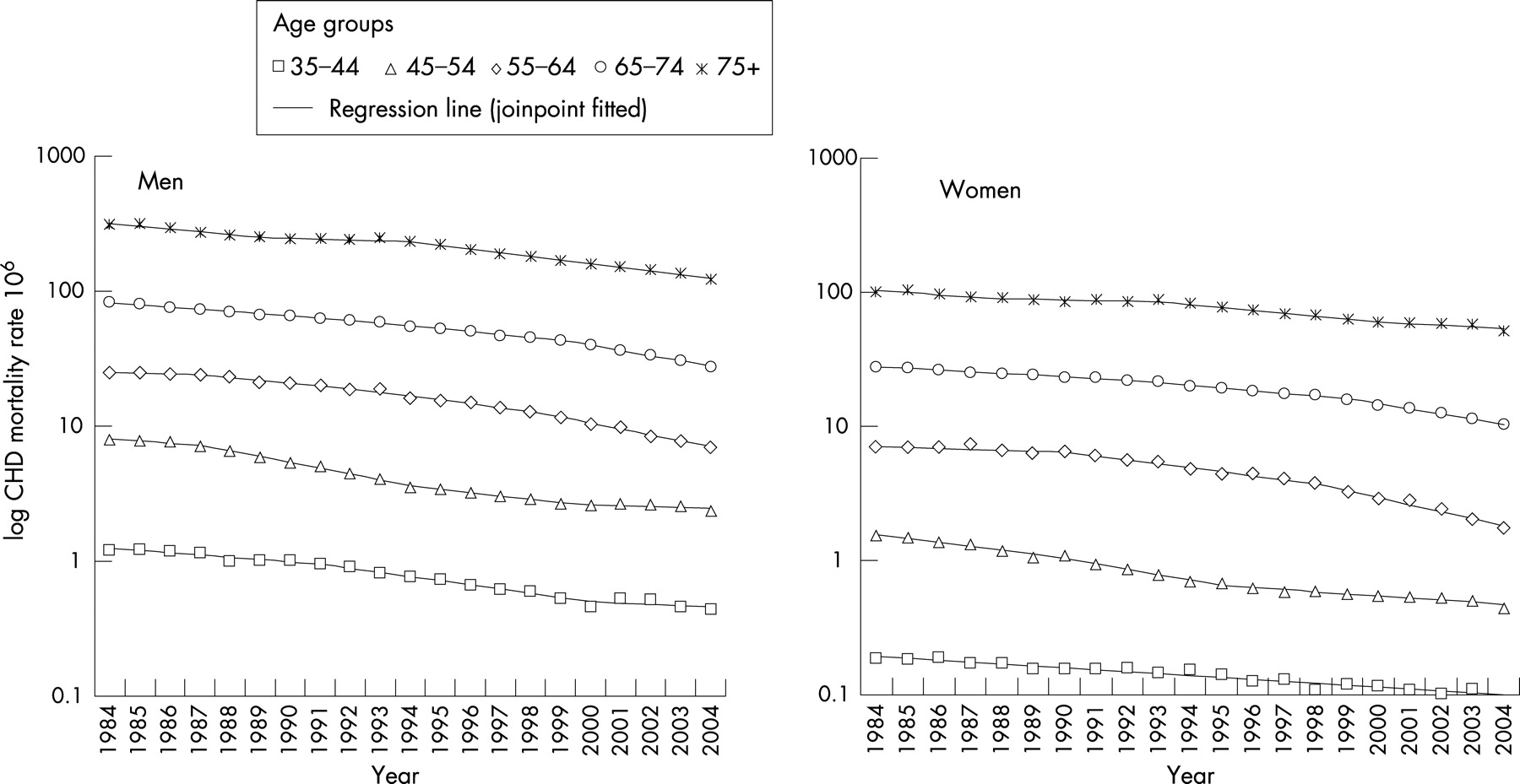
The overall age-adjusted mortality rate for CHD declined from 1984 to 2004, by 54.7% in men and 48.3% in women (fig 1). The average annual rate of decline for men was 2.7% during the 1980s increasing to 3.7% during the 1990s (1.7% increasing to 3.5% in women). From 2000 through 2004, the average annual rate of decline was even greater, 5.4% for men and 4.2% for women.

The overall age-adjusted rates concealed striking differences in the age-specific rates (fig 2 and table 1). Comparison of the first and last period identified in the joinpoint regression analysis, shows that the rate of decline has slowed for men aged 35–44 and 45–54 (reduction in the annual percentage change of 35% and 47%, respectively). Furthermore, for men aged 35–44, the annual percentage change for the period 2000–2004 was not significantly different from 0. For older men (aged over 55), the rate of decline continued to increase throughout the period. Data on model fit and selection are presented in the appendix.
{kind=link}
{kind=link}
Among women aged 45–54, the annual percentage change was reduced by about 39% in the period 1998–2004 (table 1). Rates in the age group 35–44 apparently continued to decline; however, the numbers of events was very low.
DISCUSSION
Recent trends for CHD mortality in younger UK adults are disquieting. The previous falls in age-specific mortality rates seem to be flattening in men and women aged under 55 years. Thus far, rates in older adults continue to decline. These patterns are confirmed when the absolute annual changes in rates are examined.
Changes in CHD mortality rates generally reflect changes in incidence rate and, to a lesser extent, case-fatality rate.11 Unfortunately, unbiased data about CHD incidence in the UK are limited, especially in younger groups. Studies using hospitalisation rates represent a proxy, which can be difficult to interpret.12 However, population-based data from Scotland and from the two UK MONICA centres reported substantial decreases in CHD incidence from the mid-1980s to the mid-1990s,11 13 14 which continued beyond 2000.14 15 Case fatality after myocardial infarction has also improved since the mid-1980s.11 16
The unfavourable coronary mortality rate trends during the 1990s among those aged under 55 years require urgent explanation. These trends have occurred despite the increasing use of evidence-based treatments such as angioplasty, thrombolysis and ACE inhibitors.2 This suggests that recent unfavourable trends in risk factors in young adults may explain these changes, specifically increases in obesity and diabetes, compounded by stable cholesterol levels and a smoking prevalence stubbornly persisting above 25%.7 Material deprivation might also be an important factor in younger adults. It has been reported that among younger adults, deprivation is strongly associated with ischaemic heart disease mortality and could be understood as an upstream risk factor for CHD acting through the established risk factors as mediators.17 18 This is a potential target for intervention, although it may be more effective to influence risk factor prevalence through population level interventions.19
A vigorous public health response is needed, particularly increased efforts to improve diet.20 Initiatives to accelerate the past declines in smoking must also be strengthened. Policy changes nationally and internationally potentially offer the most effective and cost-effective interventions.21 Messages about caloric restriction and increased physical activity will also need to be amplified. In addition, clinicians should be aware of the stable mortality rate for CHD among younger adults in recent years and vigorously counsel their patients about appropriate lifestyle behaviours using recent guidelines. However, younger people and those in a less advantaged socioeconomic position have less success in changing their behaviour,22 emphasising the importance of interventions to endorse healthier environments at the population level through policy and health promotion.
The party is over, and complacency runs a high risk. The flattening trends in CHD mortality rates among younger adults suggest that the cardiovascular disease epidemic is not being controlled. However, timely interventions could counteract the adverse risk factor trends before they kill more young adults.
Acknowledgments
Martin O’Flaherty was an MRC research fellow and Earl Ford was employed by the CDC. The funding sources have not been involved in any step of this research.
Appendix
Model selection using a Bayesian information criterion (BIC) approach
The BIC approach finds the model with the best fit by penalising the cost of extra parameters, which although fitting the data well, are less parsimonious.9 10
The k-joinpoint model with the minimum value of BIC(k) is selected as the final model. For example, for men aged 35–44 the best model is the one with two joinpoints, with a BIC of −13.98, and for women aged 75+ the best model was the one with three joinpoints, with a BIC of −10.83.
REFERENCES
Footnotes
Competing interests: None.
Funding: Martin O’Flaherty was an MRC Research Fellow and Earl Ford was employed by the CDC. The funding sources have not been involved in any step of this research.