Article Text

Abstract
Background Measles vaccines (MV) have sex-differential effects on mortality not explained by protection against measles infection.
Objective The authors examined whether whole-cell diphtheria–tetanus–pertussis (DTP) vaccine has sex-differential and non-specific effects.
Data sources and eligibility Following previous reviews and a new search, the effect of DTP on mortality up to the next vaccination was assessed in all studies where DTP was given after BCG or DTP was given after MV and there was prospective follow-up after ascertainment of vaccination status.
Setting High-mortality countries in Africa and Asia.
Methods The initial observation of negative effect of DTP generated six hypotheses, which were examined in all available studies and two randomised trials reducing the time of exposure to DTP.
Main outcome Consistency between studies.
Results In the first study, DTP had negative effects on survival in contrast to the beneficial effects of BCG and MV. This pattern was repeated in the six other studies available. Second, the two ‘natural experiments’ found significantly higher mortality for DTP-vaccinated compared with DTP-unvaccinated children. Third, the female–male mortality ratio was increased after DTP in all nine studies; in contrast, the ratio was decreased after BCG and MV in all studies. Fourth, the increased female mortality associated with high-titre measles vaccine was found only among children who had received DTP after high-titre measles vaccine. Fifth, in six randomised trials of early MV, female but not male mortality was increased if DTP was likely to be given after MV. Sixth, the mortality rate declined markedly for girls but not for boys when DTP-vaccinated children received MV. The authors reduced exposure to DTP as most recent vaccination by administering a live vaccine (MV and BCG) shortly after DTP. Both trials reduced child mortality.
Conclusions These observations are incompatible with DTP merely protecting against the targeted diseases. With herd immunity to whooping cough, DTP is associated with higher mortality for girls. Randomised studies of DTP are warranted to measure the true impact on survival.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
MV has sex-differential non-specific effects for child survival. We examined whether DTP vaccine has negative effects for survival, particularly for girls.
We tested six hypotheses suggesting that DTP may have negative health consequences if found to be true.
Furthermore, we conducted two randomised trials reducing the time of exposure to DTP as most recent vaccination by providing a live vaccine shortly after DTP.
Key messages
All available studies suggest that the effect of DTP on child survival is opposite of the effects of BCG and MV. In the two natural experiments, DTP-vaccinated children had significantly higher mortality than DTP-unvaccinated children.
Among DTP-vaccinated children, girls have higher mortality than boys in all studies, whereas the tendency is the opposite for BCG- and measles-vaccinated children. DTP administered after MV in randomised trials of MV is associated with increased female but not male mortality.
Reducing time of exposure to DTP as the most recent vaccination with BCG or MV reduce child mortality.
Strengths and limitations of this study
Since the healthiest children are vaccinated first, one would expect DTP to be associated with a benefit. However, all the data suggest consistently that DTP is associated with a negative effect for girls.
A randomised trial of the effect of DTP on overall survival could not be conducted. There is a need to conduct such studies now.
Introduction
Overall, routine vaccinations have beneficial effects on child survival in high-mortality countries.1 It is assumed that the effect on child survival is proportional to vaccine efficacy and the burden of the targeted infection.2 However, routine vaccinations may have non-specific effects (NSE) on child survival—that is, effects not explained by prevention of the vaccine-targeted infections.1 3 4 Such effects are presumably due to vaccines affecting susceptibility to unrelated infections. NSE were initially demonstrated by the high-titre measles vaccine (HTMV) incident. Though protective against measles infection, HTMV was associated with a twofold increased female mortality if the children got diphtheria–tetanus–pertussis (DTP) after HTMV.5 In contrast, standard measles vaccine (MV) is associated with a reduction in mortality, which is not explained by prevention of acute measles infection,6–20 and with reduced mortality for girls relative to boys5 7 13 17 21–31; for example, the female–male mortality rate ratio (MRR) declined from approximately 1.00 to 0.65 after the first MV campaigns in two rural areas of Senegal.13 17
Following the studies of HTMV and standard MV, we examined the NSE of other vaccines.1 32–81 BCG was associated with a beneficial effect on mortality, whereas DTP had no such effect, the effects being statistically different for the two vaccines.1 Subsequent studies corroborated that BCG has beneficial effects for girls.38 40 On the other hand, DTP appeared to have a negative effect for girls.26
With the increasing evidence for NSE of vaccines, the Working Group on the Non-specific Effects of Vaccines (WGNSEV) has formulated and prioritised six trials, which would help to optimise the current vaccination schedules so that they maximise the reduction in child mortality in high-mortality areas.82 Two priority trials to examine the beneficial NSE of BCG and MV have now been completed.3 65 79 In trials of BCG at birth versus delayed BCG among low birth weight (LBW) children, neonatal mortality was reduced by 48% (95% CI 18% to 67%) (WGNTEV, trial 1).65 79 In a large trial of an additional dose of MV at 4.5 months of age,3 per-protocol analysis showed that children receiving two doses of MV at 4.5 and 9 months of age had a 30% lower mortality between 4.5 and 36 months of age than children receiving the currently recommended single dose of MV at 9 months of age (WGNTEV, trial 2). There was a negative interaction with neonatal vitamin A supplementation (VAS): among the children who had not received VAS, the reduction in mortality was 50% between 4.5 and 36 months of age. When cases of measles infection were excluded, the reduction in mortality was 45%. With such strong support for the importance of the beneficial NSE of live vaccines, there are good reasons to examine carefully the possible negative NSE of inactivated whole-cell DTP.
Though several meta-analyses have shown that well-conducted observational studies can provide the same results as randomised trials,83 84 observational studies have historically ranked lower as evidence for a treatment effect than randomised studies. Hence, it is desirable to conduct randomised studies to test the NSE of vaccines, including the possible negative effect of DTP. However, once a vaccine is recommended by WHO, it becomes difficult to withhold the vaccine in randomised trials to measure the NSE of the vaccine. A possible way to test DTP would be to randomise children to either the current regimen of vaccination at 6, 10 and 14 weeks of age or to delayed vaccination at 6–8 months of age just before measles vaccination at 9 months of age (WGNSEV, trial 6). However, this has been deemed unethical by WHO committees.85 Hence, the hypothesis that DTP has a negative effect on mortality can only be tested indirectly, first by making logical deductions about epidemiological trends and testing these in other data sets and, second, by testing the implications in randomised trials. The more deductions can be generated and found to be consistent in unrelated data sets, the more likely it is that the underlying hypothesis represents a causal process. We have tested our initial observation that DTP was associated with increased mortality1 in several other data sets and subsequently generated five new deductions. These six linked observations suggest that DTP increases mortality in girls in areas with herd immunity to whooping cough. Hence, reducing exposure to DTP as the most recent vaccination should reduce child mortality. In two randomised trials, we tested whether reducing exposure to DTP by vaccinating with MV at 4.5 months of age after DTP3 (WGNSEV, trial 2) and by BCG revaccination at 19 months after DTP booster vaccination (WGNSEV, trial 3) reduced child mortality. This proved to be the case in both trials.
Methods: materials and assumptions
The initial hypothesis about a negative effect of DTP on child survival was formulated in a paper published in 2000.1
Data sources
There have been very few studies of routine immunisations and their effect on child mortality in high-mortality countries. A previous WHO-sponsored literature review from 20012 found only two studies of the effect of DTP on mortality.1 18 During the last 10 years, several new studies have become available and studies of DTP and mortality have been reviewed three times.61 81 86 In 2011, we conducted a new PubMed search for publications on ‘mortality’ or ‘death’ in relation to one of the vaccine terms ‘DTP’, ‘DPT’, ‘diphtheria-tetanus-pertussis’ or ‘pentavalent vaccine’ (see supplementary flow diagram). To be relevant, a study had to report total mortality following DTP vaccination in a defined population of children in high-mortality countries (Africa and Asia). The methodological exclusion criteria are discussed below. This search identified 444 papers: based on reading the abstract or paper, 122 papers were classified as reviews, commentaries and cost-effectiveness analyses without primary data; 99 papers were not from a high-mortality country in Africa or Asia; 117 papers had no mortality data or were not about children; 43 papers were not related to DTP and 33 papers were disease-specific studies or case reports. Hence, we retained 30 studies, and an additional five studies were known from vaccine reviews or other sources.9 18 47 78 87 These studies are briefly presented in tables 1 and 2. Most of the identified studies were conducted in Guinea-Bissau or were reanalyses of data from longitudinal studies in Africa, including studies from Congo,22 Gambia,31 Ghana,74 Malawi,30 53 Senegal5 and Sudan22 (tables 1 and 2). Seven studies were a result of WHO's Global Advisory Committee on Vaccine Safety request that other groups reanalyse existing data sets to examine the effect of DTP on child mortality.44–49 58 Fourteen studies had information on DTP provided before MV (table 1); two studies were partly overlapping,3 52 so only one of them was used in the hypothesis-specific tables.52 Three studies had specific morbidity but no mortality data (table 1). Nine studies had information on mortality when DTP was administered after MV (table 1). Nine studies were not used for the reasons discussed in the following paragraph. Table 1 indicates whether the studies had general and sex-specific mortality rates or only data from case–control and hospital case death studies with no follow-up.
Studies used in the analysis
Studies not used in the analysis due to simultaneous vaccination (see study exclusion criteria, p. 3)
Study exclusion criteria
We excluded studies that had survival bias and studies in which DTP had been administered with BCG or MV. First, in our previous review of DTP and mortality,61 studies with retrospective updating of vaccine information had survival bias which produced misleading estimates of the effect of DTP60 61 (table 2). Second, the recommended vaccination schedule used in Bissau while most of these studies were conducted is depicted in figure 1. Our hypothesis has focused on vaccinations, which have been administered in the sequence recommended by WHO: BCG first, followed by three doses of DTP and oral polio vaccine (OPV) and then MV (figure 1). However, delays in vaccination programmes are common and vaccinations are often given simultaneously: BCG with DTP or DTP with MV.44 45 47 48 58 77 These combinations have different NSE.22 28 53 57–59 64 66 77 Hence, studies in which most children received BCG and DTP simultaneously or DTP and MV simultaneously were not included (see table 2).

Vaccination schedule in Guinea-Bissau. Note: the vaccination schedule in Guinea-Bissau was changed in 2008. Pentavalent vaccine (DTP + hepatitis B virus + Hib) has replaced DTP, yellow fever is administered with measles vaccine and the booster doses of DTP and OPV have been removed. DTP, diphtheria–tetanus–pertussis; OPV, oral polio vaccine.
Analyses
The issues associated with analysing incomplete vaccination data have been presented more fully in an appendix (supplementary material). Many studies have analysed simultaneously the effect of several vaccines over several years, for example, 2 or 5 years of age.44–48 This would be appropriate if each vaccine had an independent and permanent programming effect on the immune system. However, the NSE of vaccines apparently influence general susceptibility to infectious diseases and that effect seems to be strongest while a vaccine is the most recent vaccination.81 We therefore focused on studies in which the effect of a specific vaccine could be analysed from the time it was administered until the next vaccine was given.
In most survival analyses, the estimates of the effects of vaccines on survival are obtained by comparing mortality at the same age for vaccines, which are recommended to be given sequentially. This comparison is inherently biased (‘frailty bias’) because the healthiest children are likely to receive the recommended vaccine first (see appendix). Comparisons of sequential vaccinations should be interpreted cautiously. However, if a vaccine, in spite of the expected lower mortality, is associated with a higher mortality than the previous vaccine, this is an indication that the vaccine in question may be associated with an absolute increase in mortality. We have also emphasised the comparison of female and male mortality rates among children who have received the same vaccine. In the pre-vaccination era, post-neonatal child mortality was similar for boys and girls in West Africa (figure 2). All data from Africa also suggest that girls and boys are treated equally with respect to vaccination, the age of vaccination and coverage being the same for boys and girls. In these circumstances, a deviation of the female–male MRR from 1.0 for children who have received a specific vaccine as the most recent vaccination would suggest that this vaccine is associated with sex-differential NSE.

Female–male mortality ratios in community studies from the prevaccination era in West Africa (see supplementary table 1).
Statistical analyses
Estimates are presented as reported in the published papers or have been calculated based on the deaths and person-years reported in the papers. Tests for interaction have been used to assess whether MRR for different vaccines were similar for vaccinated versus unvaccinated children and for girls versus boys.
Presentation
For each of the six deductions, we present a short section on the deduction which generated a new hypothesis and how studies were selected, a section on the observations which followed the hypothesis and a section discussing possible methodological problems and conclusions in relation to the observation. The development of the hypotheses is summarised in figure 3. The sequence of presentation follows more or less the sequence in which these hypotheses were generated: observations I–III deal with the effect of DTP when administered after BCG (or no vaccine) and observations IV and V with the effect of DTP administered after MV. Observation VI relates to the effect on female mortality of changing from DTP to MV vaccination. Finally, we present the two trials, which were conducted to reduce the duration of exposure to DTP as the most recent vaccination.

The research process. DTP, diphtheria–tetanus–pertussis; HTMV, high-titre measles vaccine; MV, measles vaccine.
Results
Developing the hypothesis: DTP has negative NSE and sex-differential effect on child survival
As described under the Methods section, 444 studies were screened for inclusion and 35 were retained as potentially relevant to the final analyses (tables 1 and 2).
Observation I. Contrasting effects of DTP, BCG and MV
Deduction and study selection
Unexpectedly, a study from rural Guinea-Bissau reported differential effects of DTP, BCG and MV within the same population1; mortality was low after BCG, increased after the first DTP vaccination (DTP1) and reduced again after MV. We tested the pattern of contrasting MRR for different vaccines in all studies that reported data on the primary DTP vaccination (after BCG and before MV) as well as BCG and/or MV vaccinations (see table 1).
Observation
A case–control study from Benin18 had previously reported the same tendencies in relative mortality for the three vaccines (figure 4). We tested these trends in a further five studies. All studies found the same pattern: mortality was low after BCG and MV but increased after DTP vaccination (figure 4, supplementary table 2). The difference in effect on survival of BCG versus DTP was statistically significant in six of six studies and for DTP versus MV in three of five studies. DTP vaccination compared with no DTP vaccination was associated with increased mortality in all seven studies, being significant in three studies.
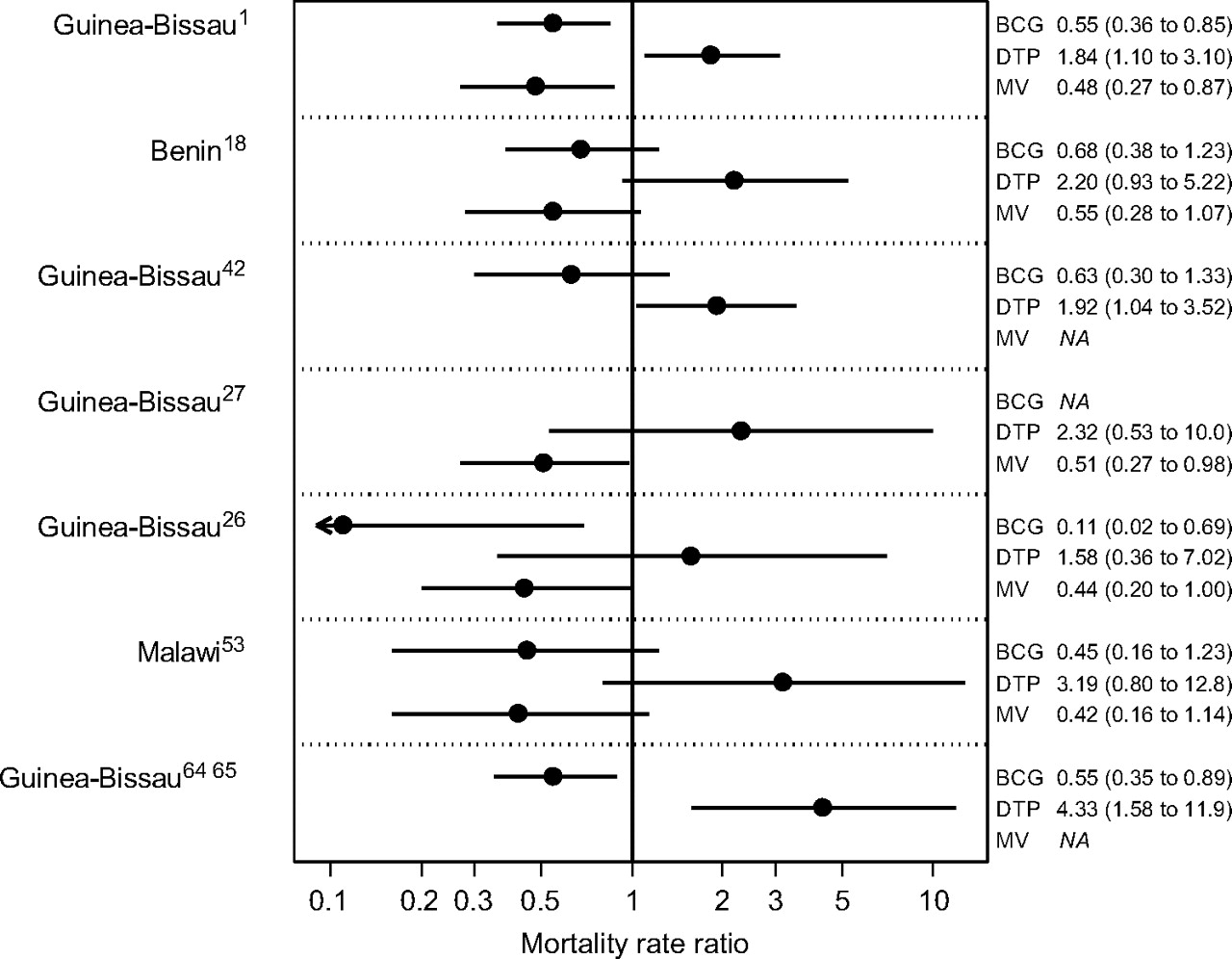
Mortality ratios for different routine vaccinations within the same study (observation I) (see supplementary table 2). DTP, diphtheria–tetanus–pertussis; MV, measles vaccine.
In most studies, DTP-unvaccinated children had received BCG. However, in the first 2 years of the study of the introduction of DTP in the rural areas of Guinea-Bissau,42 only 36 children had received BCG. If the BCG-vaccinated children were excluded, DTP-vaccinated children had a mortality rate of 14.7 per 100 person-years (27/183.4) compared with 5.3 per 100 person-years (9/169.4) for the DTP-unvaccinated children, the adjusted MRR being 2.62 (95% CI 1.08 to 6.35); the negative effect was similar for girls (MRR =2.63 (95% CI 0.76 to 9.05)) and boys (MRR =2.60 (95% CI 0.85 to 7.94)) (unpublished data). Hence, DTP may be associated with increased mortality either when it is given to previously unvaccinated children or to children who have previously received BCG.
Methodological considerations and implications
In the initial study,1 the trends were strong enough to document a differential effect of BCG and DTP, even though we did not limit the analysis to the most recent vaccination but used a landmark approach with multivariable analysis to estimate the effect of BCG and DTP in the same age range. A stricter censoring of the observational period to the age range in which DTP predominates would have provided stronger estimates: for example, the MRR estimate for DTP2 and DTP3 was reported to be 1.38 (95% CI 0.73–2.61)1 but became 1.75 (95% CI 0.86 to 3.59) when follow-up was restricted to 9 months to reduce the confounding effect of MV, which is usually given at 9 months of age.50
DTP and OPV are usually given together, and it is therefore difficult to distinguish the effects of these vaccines. However, when we first introduced DTP in rural areas of Guinea-Bissau, the effect was particularly strong during the first year when no OPV was available and only DTP was administered.42 In a second study,43 DTP administered with OPV had a worse effect than OPV alone. Furthermore, when only OPV was given during a polio eradication campaign, the impact of OPV was, if anything, beneficial.36 Hence, we assume that any negative effect of combined DTP and OPV vaccination is due to DTP.
It has been proposed that a negative effect of DTP could be due to sick children getting vaccinated first because they come more frequently to be treated at health centres.18 90 91 However, both nurses and mothers are usually reluctant to vaccinate sick children.42 46 67 If the increased mortality among DTP-vaccinated children occurred because sick children had been preferentially recruited for the DTP group, then there should have been a non-random clustering of deaths in the DTP group. This was not the case.26 42 For example, in the study of the introduction of DTP,42 it was noted that the median time to death was 95 days in the DTP group and 80 days in the unvaccinated group. The survival curves in the studies comparing DTP-vaccinated and DTP-unvaccinated children also indicate that there is no clustering of early deaths in the DTP group.1 42 53 64 Consistent with the tendency of nurses and physicians not to vaccinate sick children, current data suggest that DTP vaccination is associated with a strong positive selection bias, with healthier and wealthier children coming first for vaccination.1 42 53 64 Due to ‘frailty bias’ among the DTP-unvaccinated children, DTP should be expected to be associated with a beneficial effect on child survival. The opposite effect of DTP observed in all studies in figure 4 is therefore worrying. Furthermore, BCG and MV are associated with a beneficial effect, and it is therefore unlikely that a negative selection bias for being vaccinated explains the effect of DTP. Hence, since DTP is associated with a higher mortality than BCG, the data in figure 4 clearly suggest that DTP is associated with increased mortality. BCG, DTP and MV have different effects on survival, and since BCG and MV have been found in randomised trials to have a beneficial NSE, DTP apparently has a negative NSE.
Observation II. Comparing DTP-vaccinated and DTP-unvaccinated children in studies with limited selection bias
Deduction and study selection
The consistently opposite effect of inactivated DTP compared with live BCG and MV suggested that mortality might be increased after DTP vaccination. A small randomised trial of MV used DTP as a control vaccine; three of 27 DTP-vaccinated children died during 18 months of follow-up compared with none of 26 measles-vaccinated children.9 No large-scale randomised study has examined the impact of DTP vaccine on survival. In the absence of randomised trials, we looked for studies with limited selection bias with respect to who received or did not receive DTP. Among the studies indicated in table 1, only two studies could be said to have limited self-selection for DTP vaccination.42 43
Observations
First, the Bandim Health Project introduced DTP in 20 villages in rural Guinea-Bissau in the mid-1980s, at a time when vaccines were not generally available in rural areas. This is the only study in the global literature of what happened when DTP was introduced in a high-mortality country. Controlling for background factors, the DTP-vaccinated children had a twofold higher mortality (MRR=1.92 (95% CI 1.04 to 3.52)) during 6 months of follow-up compared with DTP-unvaccinated children, even though unvaccinated children had worse nutritional status.42 Some children were travelling when the team visited the villages every sixth months, some had fever and were therefore not vaccinated, and vaccines were not available at some visits.42 Unvaccinated children had limited access to vaccination elsewhere until our next visit.
In a second study, DTP was not available in several periods in Bissau city in 2001. Some children, who were due to receive DTP and OPV, received only OPV when they came for vaccination to a health centre, whereas others received both vaccines. We compared the case death of hospitalised children at the only paediatric ward in Bissau according to their vaccination status. Children who had received both OPV and DTP as their most recent vaccines had a significant threefold higher case death compared with children who had received OPV but not DTP when they had come to a health centre. The case death was threefold higher for both boys and girls, though this difference was not statistically significant for either boys or girls individually (unpublished data). Controlling for background factors did not change the estimate.43 67
Methodological considerations and implications
Several observational studies have estimated the effect of DTP without survival bias (figure 4). Since these studies did not find the expected benefit for DTP-vaccinated compared with DTP-unvaccinated children, DTP may have negative effects on child survival. The negative effect of DTP in the two studies with limited self-selection for DTP vaccination was not due to sick children being more likely to receive DTP vaccination.90 DTP-vaccinated children had slightly better nutritional status in both studies and few42 or no vaccines43 were given during follow-up. Hence, these two studies provide further support for the hypothesis that DTP is associated with an increase in mortality rate.
Observation III. Sex-differential effects of DTP
Deduction and study selection
HTMV, MV and BCG have sex-differential effects.5 11 40 We therefore examined whether DTP had sex-differential effects. Nine of the 13 studies of DTP before MV (table 1) had information on sex-specific mortality rates.1 9 18 43
Observations on mortality
The studies of the relative mortality of girls and boys after DTP administered before MV are summarised in figure 5 (supplementary table 3). Girls had higher mortality than boys in all nine studies, the difference being statistically significant in four studies. In nearly all studies, DTP was administered after BCG. In the two studies in which some children had received VAS, the female–male MRR was higher among those who had received VAS than among those who had received placebo (supplementary table 3). In the study of vaccination status and in-hospital mortality,27 the sex-differential effect of DTP applied to all major disease categories, including pneumonia, diarrhoea and presumptive malaria. The three studies with mortality data for unvaccinated children suggested a slightly lower mortality for unvaccinated girls than for unvaccinated boys, but the difference was not statistically significant.

Female–male (F/M) mortality ratios for diphtheria–tetanus–pertussis (DTP)-vaccinated children in studies of DTP administered after no previous vaccine42 or after BCG (other studies) and before measles vaccine (observation III) (see supplementary table 3).
In all studies that had information on DTP as well as BCG or MV, the female–male MRR was low after BCG and MV vaccinations and high after DTP (figure 6). The difference in the female–male MRRs between DTP and MV was statistically significant in five of five studies (supplementary table 4).

Female–male mortality ratios for diphtheria–tetanus–pertussis (DTP)-, BCG- and measles vaccine (MV)-vaccinated children (observation III) (see supplementary table 4).
Observations on morbidity
In community studies with complete information on vaccinations, the female–male incidence rate ratio among DTP-vaccinated children was 6.25 (95% CI 2.06 to 18.9) for cryptosporidium, 1.93 (95% CI 0.89 to 4.21) for rotavirus infection, 1.51 (95% CI 1.04 to 2.20) for infection with other diarrhoea-causing enteropathogens and 1.32 (95% CI 1.03 to 1.70) for infection with enteropathogens not causing diarrhoea.55 56 In one study of measles infection, the female–male RR for hospitalisation varied significantly depending on the most recent vaccination, being 1.21 (95% CI 0.82–1.77) for DTP before MV and 0.28 (95% CI 0.11–0.68) for MV alone.75
Methodological considerations and implications
Several trials of early MV before 9 months of age have had a control group of children who were not measles vaccinated before 9–10 months of age.7 22 51 These studies were not included in the present analysis of the sex-differential effect of DTP as most studies used another vaccine as a ‘control’ vaccine. In the studies using inactivated polio vaccine (IPV) as the control vaccine, the female–male MRR was 1.52 (95% CI 1.02 to 2.28) between enrolment and the receipt of MV.51 In Senegal, where the control group received placebo at the same time as DTP–IPV at 5 months of age, the female–male MRR was 1.41 (95% CI 0.53 to 3.76) between 5 and 10 months of age. However, since most children in Senegal had received DTP and BCG simultaneously, the study was not included in figure 5.
It could be suggested that girls have a higher mortality than boys in the age group in which DTP predominates and that the sex-differential effects of DTP vaccination are age specific rather than vaccine related. We therefore compared mortality or morbidity rates of DTP and MV-vaccinated boys and girls within the same age group in the studies with relevant data26–28 55 (figure 7). In all studies, the female–male mortality or morbidity ratio was high after DTP and low after MV, the difference being statistically significant in three of five studies (supplementary table 5). Hence, the pattern is more likely to be vaccine specific than age specific.

Mortality or morbidity patterns among diphtheria–tetanus–pertussis (DTP)-vaccinated and measles-vaccinated children of similar age (observation III). One additional study of female–male twins could not be presented graphically because one group had no deaths; this study had significant differential effects of DTP and MV (see supplementary table 5).
The higher relative mortality of DTP-vaccinated girls compared with DTP-vaccinated boys in these studies is not merely a trivial repetition of the same study design with the same potential biases. Very different study designs were used, including studies of female–male twin pairs,28 vaccination cards collected after death,31 vaccination status measured just before a war period with high mortality,26 vaccination status assessed at hospitalisation27 and children receiving DTP at discharge from a hospital.54 It cannot be explained by nutritional status because girls did not have worse nutritional status than boys at DTP vaccination (data available upon request). The contrasting female–male MRRs between DTP and BCG or MV also excludes the possibility that the higher female–male MRR after DTP was due to a generally higher female mortality rate in Africa. Since most of the present studies (figures 5 and 6) also documented increased mortality of DTP-vaccinated children relative to BCG- and MV-vaccinated children (figure 4), the higher female than male mortality rates or case death ratios for DTP-vaccinated children presented in supplementary tables 3–5 cannot be explained by a beneficial effect of DTP for boys. Hence, these studies support the hypothesis that DTP is associated with increased female mortality when DTP is given after BCG.
Observation IV. HTMV trials and DTP
Deduction and study selection
The consistent sex-differential effects of DTP suggested a solution to an earlier enigma. In the late 1980s, randomised trials found that HTMV administered at 4–5 months of age was associated with a twofold higher mortality in girls.5 Control children received IPV or placebo at 4–5 months of age plus standard-titre MV at 9–10 months of age. Though girls have a lower mortality after standard MV (observation III), HTMV-vaccinated girls had a higher mortality than HTMV-vaccinated boys and a higher mortality than control girls after 9–10 months of age (when control children had received standard MV). HTMV was administered early, and most children received DTP/IPV after MV. We examined whether DTP/IPV administered after HTMV could explain the increased female mortality in all the HTMV trials with information on vaccinations after HTMV.5 22 92 Another HTMV study with mortality data was performed in Haiti,29 but DTP vaccination status was not reported.
Observations
In a reanalysis of all the West African trials, we found no increase in the female–male MRR for children who did not receive the planned DTP/IPV vaccination after HTMV (female–male MRR =0.96 (95% CI 0.69 to 1.34)). In contrast, twice as many girls as boys died among children who received DTP/IPV after HTMV.5 Girls in the HTMV group who received DTP/IPV at 9–10 months of age had an MRR of 2.35 (95% CI 1.41 to 3.91) from 9 months to 5 years of age compared with control girls receiving standard MV at the same age.5 Hence, the real cause of increased female mortality after HTMV was probably that most children received DTP after being given HTMV at 4–5 months of age, while control children received DTP before being given standard MV at 9 months of age.
We tested this further in a reanalysis of the two other African studies of HTMV with mortality data.22 92 First, in Congo, children did not receive DTP after HTMV and girls had no excess mortality, the female–male MRR being 0.40 (95% CI 0.13 to 1.27). Second, in Sudan, children did receive DTP after HTMV, and the female–male MRR was 3.89 (95% CI 1.02 to 14.83) from 5 months to 3 years of age. This study collected data on vaccination status at enrolment but not on vaccinations during follow-up. Excess female mortality was found only among children who had not received all doses of DTP prior to enrolment and so presumably received missing doses during follow-up. The excess female mortality increased significantly with the number of doses of DTP missing at enrolment and therefore likely to be given during follow-up. Hence, DTP is likely to have caused the increased female mortality.
Methodological considerations and implications
The hypothesis that DTP causes excess female mortality after BCG generated the deduction that the excess mortality in the HTMV trials could be due to a similar process of DTP vaccinations causing excess female mortality after HTMV. HTMV-vaccinated girls who received DTP/IPV after HTMV were found to have higher mortality than both HTMV-vaccinated boys who received DTP/IPV after HTMV and control girls who had received MV later in infancy. Since girls who received DTP/IPV after HTMV had higher mortality than control girls receiving MV at 9–10 months of age, the increased female–male MRR after HTMV cannot be ascribed to reduced mortality among boys who received DTP/IPV after HTMV. Hence, HTMV may have been withdrawn for the wrong reason. The increased mortality among girls after HTMV appears to have been caused by the administration of inactivated vaccines after HTMV and not by a direct effect of HTMV itself.
Observation V. DTP after measles vaccination associated with increased female mortality
Deduction and study selection
The Sudan trial22 suggested that the number of missing DTP vaccinations prior to MV explained the subsequent excess mortality of girls in this trial. We therefore tested whether missing doses of DTP at enrolment was associated with increased female mortality in other trials of MV, which had documented DTP vaccination status at the time of enrolment, and where DTP and MV were not administered simultaneously. Apart from the Sudanese study,22 information was available from five other MV trials: one from Congo22 and four from Guinea-Bissau.51 The four trials from Bissau covered all MV trials conducted in Bissau before we introduced the requirement that children had to have received DTP3 prior to enrolment.3 Furthermore, we reviewed observational studies of DTP administered after MV (tables 1 and 2). Several studies have information on DTP and MV administered simultaneously,22 31 53 57 66 77 but only three studies had information on DTP administered after MV.31 57 74
Observations
In the six randomised trials of early MV compared with children who had received DTP3 at enrolment, mortality was significantly increased among children who were missing DTP3 at enrolment (and presumably received additional doses of DTP after MV) with a MRR of 1.60 (95% CI 1.14 to 2.24) (figure 8). However, the negative effect was found only for girls. Compared with children who had received DTP3 prior to MV, girls likely to receive DTP after MV had a MRR of 2.36 (95% CI 1.43 to 3.89), whereas there was no difference for boys. The effect was significantly different for girls and boys (p=0.031, test of homogeneity) (supplementary table 6).

Mortality after enrolment in measles vaccination trials according to diphtheria–tetanus–pertussis (DTP) status at enrolment: missing DTP vaccinations versus fully DTP vaccinated (observation V) (see supplementary table 6 with two additional small studies which could not be presented due to undefined estimates).
The observational studies also suggested that DTP after MV is associated with increased female mortality. In a large trial of VAS after 6 months age in Ghana,74 the female–male MRR was 1.62 (95% CI 1.02 to 2.63) during the 2 years of the study among children who had received only one to two doses of DTP and were likely to receive DTP during follow-up. The excess female mortality in this study was also stronger among the children who received VAS rather than placebo. At the paediatric ward in Bissau, children who had received DTP after MV rather than MV alone as the most recent vaccination had an increased in-hospital mortality and the trend was stronger for girls, though the effect was not statistically significant in this small study.43 In a Gambian community study, vaccination cards were collected in connection with a verbal autopsy interview: measles-vaccinated girls who died were 3.34 (95% CI 1.15 to 9.74) fold more likely to have received DTP3 after MV than girls who did not die.31
Methodological considerations and implications
The six measles trials did not register all vaccinations during follow-up. However, most children did receive the missing doses of DTP: at least 85% received missing doses of DTP in Guinea-Bissau.51 In general, children missing doses of DTP might have less compliant mothers or have less access to healthcare and therefore have higher mortality during follow-up. However, these children were enrolled in trials and had the same access to healthcare, and it seems unlikely that minor delays in the administration of DTP can explain the differences in mortality. Furthermore, the effect was found only for girls, making it unlikely that the overall effect is due to selection bias. The few other studies with information on mortality for children who had received DTP after MV also suggested a stronger negative effect for girls. Hence, the data suggest that administration of DTP after MV increases mortality and that this effect is stronger in girls than boys.
Observation VI. Mortality declines when DTP-vaccinated girls receive MV
Deduction and study selection
Without a control group, it is difficult to ascertain the overall effect of DTP on child mortality. However, the increased female–male mortality ratio after DTP and the reduced ratio after MV (figure 6) suggested that mortality would decline for girls once they receive MV. We therefore assessed the change in mortality levels for boys and girls in the transition from DTP to MV. There were three community studies among the studies in observation III (figure 6) with information on both DTP and MV mortality rates.26 31 53
Observations
In the transition from DTP to MV, mortality decreased for girls in all three studies (figure 9). This pattern is illustrated for two of the studies in figure 10. For boys, mortality increased in two studies and declined less markedly than for girls in one study. The effect of MV was statistically different for boys and girls in two of the three studies (supplementary table 7).

Mortality rate ratios for measles vaccine age group versus diphtheria–tetanus–pertussis age group (observation VI) (see supplementary table 7).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Methodological considerations and implications
In two studies, we used data for individuals with known vaccination status within the respective age groups. In the Gambia, it was known that the coverage was very high but individual vaccination data were not available and the comparison could therefore only be made for all children in the age groups. We analysed the community data sets used in figure 6, and girls experienced a pronounced decrease in overall mortality when MV replaced DTP. As discussed above, this change could not be ascribed to an age effect (figure 7).
Testing the hypothesis: the negative effect of DTP may be reduced with a subsequent vaccination with MV or BCG
The six observations in this paper support the hypothesis that DTP has negative NSE and sex-differential effect on child survival. It has been considered unethical to test DTP in a randomised study.85 Instead we tested an implication of the hypothesis in two randomised trials.3 69
Deduction
If overall mortality is increased when DTP is the pre-dominant vaccine (observations I, II and VI), it might reduce mortality if a live vaccine were given shortly after DTP to change the immunological profile and reduce exposure to DTP as most recent vaccine. As shown in figure 10, which presents data from The Gambia and Malawi, mortality is increased between 2 and 8 months of age (especially in girls), the age at which DTP is likely to be the most recent vaccine, and around 18 months of age, the age at which booster DTP vaccination has been administered in The Gambia. Hence, mortality might be reduced if MV were administered earlier than 9 months of age or a BCG revaccination was given shortly after the 18 months booster dose of DTP.
First test: early measles vaccination
We conducted a randomised trial of an additional dose of MV at 4.5 months of age to test whether early MV is associated with reduced mortality for girls.3 To prevent the problem with increased mortality among girls getting DTP after MV,51 only children who had already received DTP3 were enrolled in the trial.3 68 Compared with the control children who had DTP3 as the most recent vaccination, MV tended to have a beneficial effect for girls, the MRR between 4.5 and 9 months of age being 0.46 (95% CI 0.19 to 1.11) for girls and 0.94 (95% CI 0.44 to 2.01) for boys.3 Many of the children in this trial had received VAS at birth, and VAS had a negative effect on child survival. VAS at birth is not WHO policy, and among children who had not received VAS at birth, early MV compared with DTP3 as the most recent vaccination was associated with a threefold reduction in mortality between 4.5 and 9 months of age (MRR =0.33 (95% CI 0.13 to 0.86)), the estimate being 0.30 (95% CI 0.07 to 1.31) for girls and 0.36 (95% CI 0.10 to 1.26) for boys.
Second test: booster BCG vaccination
Since booster DTP and OPV are usually administered at 18 months of age in Guinea-Bissau, we enrolled children at 19 months of age in a trial of BCG revaccination.69 Among children who had received booster DTP before enrolment, BCG revaccination was associated with a threefold reduction in mortality, the MRR being 0.36 (95% CI 0.13 to 0.99)69 with a similar effect in girls and boys. Children who had not received booster DTP before enrolment were encouraged by health personal to come back and receive missing DTP vaccinations. In this group, BCG revaccination was associated with increased mortality, the MRR being 1.78 (95% CI 1.04 to 3.04). In general, the effect of BCG revaccination may have been better for girls since girls had a significantly lower risk of hospitalisation than boys after BCG revaccination (female–male hospitalisation ratio 0.65 (95% CI 0.46 to 0.93)), the annual incidence rates being 3.1% for girls and 4.8% for boys. Among controls, the female–male hospitalisation ratio was 1.00 (95% CI 0.70 to 1.43), the incidence rates being 3.8% for both girls and boys.69
Methodological considerations and implications
Since live vaccines usually have a good effect for girls, the proposed changes in vaccination schedule represented attempts to reduce the negative effects by administering live vaccines after inactivated DTP. Both randomised studies showed an effect consistent with our hypothesis; bias is unlikely to have had any effect. Both studies also showed that there may be unimagined interactions with other immune interventions; in the MV trial, neonatal VAS removed the beneficial effect of early MV, and in the BCG revaccination trial, getting DTP after BCG revaccination doubled mortality. It is not possible to determine whether the beneficial effect of early MV or BCG revaccination is due to a reduction in the negative effect of DTP or to beneficial NSE of these vaccines. However, both studies suggest that it is beneficial to reduce exposure to DTP as most recent vaccination by using a live vaccine.
Discussion
Main findings
Our observations are not compatible with DTP merely preventing the targeted diseases. Observations I, II and IV–VI indicate that mortality is increased after DTP vaccination compared with children who have BCG or MV as their most recent vaccination. Observations III–VI suggest that DTP has sex-differential effects on mortality, the negative effect of DTP being worse for girls. Hence, most excess mortality associated with DTP is due to increased female mortality. As summarised in table 3, most studies reflect what happens when DTP is administered after BCG or MV. In both situations, DTP is associated with an increase in overall mortality, the effect being particularly negative for girls. One study42 suggests that the effect of DTP is also negative when it is given to totally unvaccinated children (table 3).
Evidence for the effect of DTP in relation to the sequence of vaccinations
To test the implications of these observations, we conducted two trials to reduce the time of exposure to DTP as the most recent vaccination by administering MV or BCG shortly after the last DTP vaccination. The effect was beneficial in both trials. These results are in glaring contradiction to the increasing number of randomised trials showing that BCG and MV have beneficial NSE in high-mortality countries.3 65 69 79 81 The randomised trials confirm previous observational studies of the beneficial effects of BCG and MV.
Strengths and weaknesses
In spite of the limitation of observational studies and the variability in how the different data sets were collected, the studies produced consistent results. Most observations were repeated in several studies and generated new deductions, which were tested in all the available data sets. Furthermore, several randomised trials or re-interpretations of randomised trials now support the hypothesis that DTP has negative effects, particularly for girls.5 51 52 69 72–74
The inherent tendency is to dismiss observations conflicting with the current disease-specific paradigm as probably due to uncontrolled confounding.90 93 However, confounding is unlikely to explain the twofold increase in mortality in the only community study of the introduction of DTP,42 the threefold decrease in hospital case death when DTP was missing,43 the fourfold increase in mortality when DTP was given after BCG in a trial of early BCG vaccination to LBW children,64 the twofold increase in mortality when DTP was administered after HTMV5 or standard MV (supplementary table 6) and the twofold increase in mortality when vitamin A was given to girls likely to receive DTP during follow-up.74
Since our group produced most of these studies, it could be said that these observations are due to publication bias because studies were published only if they showed a negative effect of DTP.93 Although this is not the case, it is difficult to provide evidence other than the fact that all data sets reanalysed in collaboration with other African research groups documented similar patterns.5 22 31 53 74
Analytical designs and conflicting interpretations
In the first design, we compared DTP-vaccinated versus DTP-unvaccinated children in a survival model comparing sequential vaccinations at the same age. Given the positive selection bias associated with DTP or, alternatively, the frailty bias associated with not getting DTP, the negative effect of DTP in all studies using a landmark approach or case–control design is noteworthy.61 Both the contrasting estimate for the different vaccines and the natural experiment studies support the hypothesis that DTP increases mortality. In contrast to observations I and II, some studies using a sequential vaccination comparison have produced beneficial estimates for DTP.44–49 58 However, several of these studies had survival bias due to retrospective updating of vaccination status (table 2,60 61). We obtained similar (falsely) positive estimates for DTP when we reanalysed our own data with survival bias.62 Furthermore, these studies mostly administered BCG and DTP simultaneously, whereas we administered DTP after BCG as currently recommended by WHO. We have shown in a randomised trial of BCG at birth to LBW children that the negative effect of DTP was much stronger among the children who received BCG at birth and DTP 6–7 weeks later than among children who received BCG and DTP more or less at the same time.64 Finally, social selection and frailty bias were important in the studies that produced beneficial estimates for DTP.46 59
In the second design, we compared the mortality rates of girls and boys, and all studies suggested that mortality is relatively increased for girls when DTP is the most recent vaccination, whereas the opposite is true after BCG and MV vaccinations. These studies are methodologically less complicated as long as we can be sure that the children are unlikely to receive other vaccinations during follow-up. There is no clear indication of a gender-specific selection bias which could explain this pattern, and the fact that the female–male MRR is increased after DTP but reduced after MV and BCG excludes the possibility that these patterns are mainly due to selection bias. It has been suggested that the higher female–male MRR after DTP could be due to reduced male mortality after DTP.94 However, several of our observations demonstrate that this is not the explanation. First, DTP administered after BCG is associated with increased mortality in both boys and girls (observations I and II). Second, mortality was increased twofold when girls received DTP/IPV after HTMV (observation IV) or after standard MV, while this was not the case for boys (observation V). Third, female mortality is reduced once DTP-vaccinated girls get MV (observation VI).
Interpretation
Our six observations on DTP are consistent with the hypothesis that DTP without simultaneous administration of BCG or MV has a negative effect for girls compared with both DTP-unvaccinated girls and DTP-vaccinated boys.80 Furthermore, we deduced the hypothesis that DTP after MV might have been the explanation of the increase in female mortality in the HTMV trials, and the results of all the available studies are consistent with this hypothesis (observation IV). We also deduced that if an inactivated vaccine like DTP were associated with higher female–male MRR, similar effects might occur with other inactivated vaccines. Both hepatitis B vaccine and IPV were associated with increased female mortality.37 51 Though it has not been possible to conduct a randomised trial of delaying the primary series of DTP vaccinations, we did randomise children at 4.5 months of age to early MV in an attempt to reverse the adverse effect of DTP and we achieved a threefold reduction in mortality.3 Likewise, BCG revaccination after DTP booster vaccination reduced mortality threefold.69 It is unlikely that DTP has no negative sex-differential effects when such consistent deductions can be generated.
The majority of studies have been conducted in communities with herd immunity sufficient to eliminate deaths from whooping cough, and our studies do not reflect what would happen in a situation without general DTP vaccinations. There are very few community studies that have assessed the impact of pertussis on child mortality in high-mortality countries in the pre-vaccination era. The best community study was conducted in the 1970s in Kenya in the initiation phase of the vaccination programme; the case death was assessed to be 1.3% for all ages and pertussis was 6% of the infant deaths.95 Given the major increases in mortality in observational studies and the reduction in mortality in the randomised studies, it seems likely that DTP would also be associated with increased mortality for girls in situations without herd immunity.
Possible biological mechanisms of NSE
Our work is based on the hypothesis that a vaccine may affect the immune system in a sex-differential manner during the period when it is the most recent vaccination.80 Studies of specific infections suggest that vaccines may enhance or reduce susceptibility to these unrelated infections in a sex-differential manner.38 55 56 75 Presumably, the NSE could also be due to changes in the control of infections, with vaccines enhancing or reducing the severity of subsequent infections. This possibility has yet to be examined in epidemiological studies.
Immunological studies have shown that vaccines may influence the response to unrelated antigens. In animal studies, inactivated vaccines like DTP are associated with a Th2 profile, whereas live vaccines of the same antigens produce a Th1 profile, and this difference is important for the response to a subsequent challenge.96–103 This difference may be more important for girls.102 In animal studies, some infections prime the immune response to other pathogens, resulting in so-called heterologous immunity, which may be either protective or detrimental.4 104 Some human infections may have a similar importance; for example, we have found in several studies that measles infection may reduce the mortality from other causes after the acute phase of measles infection.19 105 106 Furthermore, the very rapid reduction in mortality in randomised trials of BCG vaccination at birth suggests that BCG is training the innate rather than the adaptive immune system in a beneficial manner.79 107 However, it may still be difficult to believe that a single vaccination like BCG, DTP or MV—in an environment with numerous concurrent and competing infections—could have such profound sex-differential NSE on overall mortality. However, the vaccines with strong NSE are all given by parenteral injection, which bypasses the natural immune barriers, and this could have an important influence on their effects on the immune system.
Other factors affecting the immune system may influence the NSE of DTP, for example, season, other vaccines and micronutrient interventions.70–74 76 We have already alluded to the fact that combinations of DTP and BCG, or DTP and MV, have distinct effects, which cannot be deduced from the patterns described in the present hypothesis.5
Conclusions and implications
There are no definite criteria for imputing causality in observational studies, though the Hill criteria108 are often invoked. The present data on DTP comply with the criteria of strength of association, dose–response relationship,27 42 temporal sequence, consistency between different studies and specificity of the association. Most people would also request biological plausibility. However, as Hill noted, only biological processes that are already known are plausible.108 When exploring a phenomenon with unknown biological mechanisms, the main criterion for scientific fruitfulness is consistency of observations. We developed six linked hypotheses, which suggest that DTP is consistently associated with higher female mortality. Furthermore, we conducted two randomised trials to reduce exposure to DTP, and both trials suggested that this was beneficial. If randomised trials are deemed unethical, the present study represents the best possible evidence for the hypothesis that one of the most widely used routine vaccines has negative sex-differential effects. The finding that DTP has adverse effects has several implications.
International organisations and donors have chosen to use DTP3 coverage as the main indication of the effectiveness of national vaccination programmes.109 110 This leads to DTP vaccination campaigns and to vaccinations being administered out of sequence.66 Both DTP vaccinations before 9 months of age and DTP administered after MV suggest that DTP is associated with many unnecessary deaths. Given the potential for negative effects from DTP, MV coverage should be used to monitor the effectiveness of national vaccination programmes rather than DTP coverage.
Randomised trials are warranted to assess the ‘true’ impact of DTP on child survival.82 First, several observational studies have found that early DTP vaccination is particularly harmful.55 64 and it would therefore be desirable to examine whether delaying DTP vaccinations reduces this negative effect (WGNSEV, trial 6). However, this design is likely to be particularly controversial,85 and it may therefore be more strategic to further test whether an early two-dose MV schedule at 4 and 9 months can improve child survival (WGNSEV, trial 2).3 Second, administering DTP with or after MV may be harmful,22 44 53 57–59 66 77 and trials are therefore needed to assess whether the vaccination programme should forbid such out-of-sequence vaccinations (WGNSEV, trial 4). Third, SAGE (WHO Strategic Advisory Group of Experts on immunisation) has recently recommended a booster dose of pertussis vaccine given in the second year of life.111 This recommendation could increase mortality (see figure 10). As suggested by the WGNSEV, the effect of a booster dose of pertussis should be tested in a randomised controlled trial (RCT) measuring the impact on overall survival by providing a live vaccine shortly after booster DTP (trial 3).82 Alternatively, before being introduced, a booster dose of DTP should be tested in a randomised trial.
We should also consider whether immunity to DTP could be obtained with a different vaccine having no negative effects in a situation with herd immunity.112 In the current vaccination schedule (see figure 1), DTP is the most recent vaccination for 49.5 months for the first 5 years of life if booster DTP is given and for 7.5 months if no booster is given. This could be reduced to 3–4 months if an additional dose of MV were given at 4 months of age and a live vaccine were given 1 month after a DTP booster. This could be further reduced if the initial series of three doses of DTP were reduced to two doses in countries with a booster dose of DTP.
The WGNSEV recommended six trials to assess the beneficial effects of BCG and MV and the potential negative effects of DTP. The three priority trials (trials 1–3) have been completed and have clearly shown that NSE are important. A small trial similar to trial 4 has also found negative effects of DTP.77 The two remaining trials (trials 5–6) are less relevant or feasible. Trial 5 would test DTP without aluminium, but this could not be done without major funding to get a new vaccine licensed. Trial 6 tests a delayed DTP schedule, which is controversial and has become less relevant due to the beneficial effect of early MV.3 Hence, to advance the understanding of the NSE of vaccines, the most important steps may be that other groups repeat the three priority trials.82 Many new vaccines are being tested and introduced at the moment. It would seem important that potential NSE and sex-differential effect of the new vaccines be tested through carefully controlled before–after studies, phased introduction studies or randomised trials.
The global health community has conducted no trial to document that BCG, DTP, OPV and MV have the intended effects on child survival and only those effects. Randomised controlled trials have now shown major beneficial NSE of BCG and MV3 65 69 79 and negative effects of HTMV.5 The common assumption that vaccines have mainly disease-specific preventive effects is no longer tenable. The data presented here suggest that DTP has a negative effect for girls. Experts have recognised that WHO-sponsored studies reporting a beneficial effect of DTP had methodological problems,113 and Global Advisory Committee on Vaccine Safety has declared that it will keep a watch on the evidence of NSE of vaccines, including a potential deleterious effect of DTP vaccination.114 Despite this, policy has not changed and studies have not been organised to resolve the issues. In a culture that prides itself on being evidence based, such inconsistencies between policy and evidence should not be acceptable. We can only hope that the global health community will seek to establish the much-needed evidence for the current vaccination policies to ensure that immunisation confers maximum benefit on children in high-mortality countries.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online material 1
- Data supplement 2 - Online table
- Data supplement 3 - Online material 2
Footnotes
To cite: Aaby P, Benn C, Nielsen J, et al. Testing the hypothesis that diphtheria–tetanus–pertussis vaccine has negative non-specific and sex-differential effects on child survival in high-mortality countries. BMJ Open 2012;2:e000707. doi:10.1136/bmjopen-2011-000707
Contributors The first draft was written by PA. All authors contributed to the papers which form the basis for this hypothesis and to the final version of the present paper. PA will act as guarantors of the study.
Funding The Bandim Health Project received support from DANIDA and the Danish National Research Foundation. PA holds a research professorship grant from the Novo Nordisk Foundation. CB is funded by the European Research Council (ERC-2009-StG, grant agreement number 243149). The Research Center for Vitamins and Vaccines (CVIVA) is supported by the Danish National Research Foundation.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data available. The authors' own data sets are available through data sharing agreements (see http://www.bandim.org/).