- Tessa Heestermans1,
- Joyce L Browne1,
- Susan C Aitken2,3,
- Sigrid C Vervoort4,
- Kerstin Klipstein-Grobusch1,5
- 1Julius Global Health, Julius Center for Health Sciences and Primary Care, University Medical Center Utrecht, Utrecht, The Netherlands
- 2Ndlovu Research Consortium, Elandsdoorn, South Africa
- 3Department of Medical Microbiology, University Medical Centre Utrecht, The Netherlands
- 4University Medical Centre Utrecht Cancer Center, Utrecht, The Netherlands
- 5Division of Epidemiology & Biostatistics, School of Public Health, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
- Correspondence to Dr Joyce L Browne; J.L.Browne{at}umcutrecht.nl
- Received 12 July 2016
- Revised 30 October 2016
- Accepted 1 November 2016
Abstract
Objective The rapid scale up of antiretroviral treatment (ART) in sub-Saharan Africa (SSA) has resulted in an increased focus on patient adherence. Non-adherence can lead to drug-resistant HIV caused by failure to achieve maximal viral suppression. Optimal treatment requires the identification of patients at high risk of suboptimal adherence and targeted interventions. The aim of this review was to identify and summarise determinants of adherence to ART among HIV-positive adults.
Design Systematic review of adherence to ART in SSA from January 2002 to October 2014.
Methods A systematic search was performed in 6 databases (PubMed, Cochrane Library, EMBASE, Web of Science, Popline, Global Health Library) for qualitative and quantitative articles. Risk of bias was assessed. A meta-analysis was conducted for pooled estimates of effect size on adherence determinants.
Results Of the 4052 articles screened, 146 were included for final analysis, reporting on determinants of 161 922 HIV patients with an average adherence score of 72.9%. Main determinants of non-adherence were use of alcohol, male gender, use of traditional/herbal medicine, dissatisfaction with healthcare facility and healthcare workers, depression, discrimination and stigmatisation, and poor social support. Promoters of adherence included counselling and education interventions, memory aids, and active disclosure among people living with HIV. Determinants of health status had conflicting influence on adherence.
Conclusions The sociodemographic, psychosocial, health status, treatment-related and intervention-related determinants are interlinked and contribute to optimal adherence. Clinics providing ART in SSA should therefore design targeted interventions addressing these determinants to optimise health outcomes.
Key questions
What is already known about this topic?
Rapid scale-up of antiretroviral therapy (ART) resulted in the highest number of HIV-positive people using ART worldwide. Non-adherence to ART is the most common reason for treatment failure.
Several systematic reviews have addressed determinants of adherence and showed determinants of adherence to differ per region of the world.
What are the new findings?
This systematic review combined quantitative and qualitative articles to determine predictors for (non-)adherence. Main determinants identified for non-adherence were use of alcohol, male gender, use of traditional/herbal medicine, dissatisfaction with healthcare facility and healthcare workers, depression, discrimination and stigmatisation, and poor social support. Promoters of adherence included counselling and education interventions, memory aids, and active disclosure of HIV status.
Qualitative articles provided insights into underlying reasons for identified determinants for (non-)adherence
Recommendations for policy
A thorough understanding of factors associated with ART (non-)adherence allows for targeted interventions. We propose a number of interventions that could be implemented in healthcare services throughout sub-Saharan Africa to increase ART adherence.
Introduction
Around 36.7 million people worldwide are currently living with HIV, of which 52% reside in sub-Saharan Africa (SSA).1 With the introduction of antiretroviral therapies (ARTs), HIV is increasingly becoming a chronic manageable disease.2 As a reflection of global roll-out efforts, the number of people living with HIV and receiving ART has increased by a third since 2013 and in 2015 about 17 million people received ART globally. Treatment success requires both a sustainable supply of ART to clinics and lifelong adherence to treatment by patients.1 ,3 ,4 The importance of improving treatment adherence has resulted in a vast number of publications focussing on this topic.
Non-adherence is the most common reason for treatment failure,5 with potential risk to develop drug resistance through suboptimal viral suppression. Subsequent transmission of first-line ART-resistant HIV strains increases demand for second-line treatment often associated with poorer patient health outcomes and increasing healthcare costs.5–7 For these reasons, a thorough understanding of determinants of adherence to ART are paramount.8
Studies on ART adherence showed that predictors and risk factors differ per region of the world, necessitating context-specific development of non-adherence profiles.9 ,10 This will enable healthcare providers to offer tailored care for patients at risk of non-adherence.11 The objective of this study was to identify and summarise determinants of adherence to ART among HIV-positive adults in SSA. For a comprehensive overview, both qualitative and quantitative studies were included,12 as qualitative studies may identify key themes not found, described or discussed in larger quantitative studies.
Methods
Protocol and registration
The systematic review was conducted in accordance with the PRISMA guidelines13 and the Cochrane Handbook for Systematic reviews;14 the study protocol was registered in PROSPERO (ID: CRD42014014476).
Eligibility criteria, information sources and search strategy
A systematic literature search was performed in the following electronic bibliographic databases: PubMed/MEDLINE, The Cochrane Library, EMBASE, Web of Science, POPLINE, and the Global Health Library for all publications up to 27 October 2014. Search terms composed of MeSH and combined text for domain: ‘HIV positive adults receiving ART in SSA’, outcome ‘Patient Compliance’ and determinant ‘Risk factors’, ‘Determinants’ or ‘Predictors’. For the complete search strategy see online supplementary data 1. Filters were applied to exclude articles regarding infants, children and geographical locations other than SSA. All duplicates were removed using EndNote X7.15 No restriction based on year of publication, study design or language was applied. Given the comprehensive approach of the search, references were not checked, except those from a recent global systematic review,11 which did not yield additional articles.
supplementary data
Study selection
Titles and abstracts were independently screened for inclusion eligibility by two out of three reviewers (TH, JLB, SCA). Inclusion criteria were: study population of 15 years or older, living in SSA, HIV-positive, currently receiving ART, and available adherence information. Age cut-off was based on previous systematic reviews and WHO/UNICEF Health Indicator guideline.16 Studies reporting on non-SSA populations were only included if the abstract indicated data were presented stratified for SSA participants. Eligible studies could be qualitative and/or quantitative. Animal, biomedical studies, case reports, non-peer-reviewed published reports of proceedings, conference abstracts, secondary analyses, without main focus on the region of SSA and studies that are written in neither English nor Dutch were excluded. Discrepancies between reviewers in this process were discussed and resolved by full-text evaluation. In case of incomplete data or unavailable full-text articles, two attempts were made to contact the corresponding author via email, no reaction resulted in exclusion of the study. Post hoc, a random 10% of 332 articles excluded based on region was assessed if the article contained any results for SSA. This was not the case.
Data collection process and data items
Data extraction was performed using a standardised data extraction form. For each article, name of the first author, publication year, country and geographical region, that is, Central-Africa, East-Africa, Southern Africa and West-Africa following the index of National Library of Medicine—Medical Subject Headings,17 study design, aim of study, study setting, adherence outcome, sample size, treatment status (initiating or already on ART), adherence assessment method and determinants/risk factor outcome were retrieved. Determinants were coded according to themes: sociodemographic and socioeconomic, treatment and health facilities, psychosocial, health status, and counselling and education interventions. These themes were adjusted where necessary in the writing process to assure that all determinants fitted within the framework.
Data extraction was carried out by a single reviewer (TH), who was not blinded for journal and author details. If clarifications on data extraction were needed, one of the two reviewers was contacted (JLB, SCA). Ten per cent of the qualitative studies were randomly controlled for uniformity in data extraction by a second reviewer (SCV). If data from the same study were used in multiple articles, the article reporting on the largest sample size or data source was used. For longitudinal studies, adherence measurement of the first time point was used to facilitate comparability across studies and to reduce loss to follow-up bias.
Quality assessment and risk of bias in individual studies
Quantitative studies
For quality assessment of quantitative studies, an adapted version of the Cochrane Collaboration tool was applied as previously used in comparable reviews.18 ,19 Studies were scored according to the following criteria: blinding of researcher or clinicians, selection of study population, completeness and origin of data (measurements performed by authors or database research), clarity of outcome definition, and whether and how confounders were taken into account. Risk of bias was assigned as low, high or unclear risk, according to the quality assessment tool previously described.14
Qualitative studies
Qualitative articles were scored on their risk of bias using a previously developed approach by Vervoort et al20 focussing on (1) participants of the study: nature of sample, recruitment strategy, population, sample size; (2) data collections: validity measurements, quality of data collector, interview type, data triangulation, thickness of data; and (3) data analysis: coding procedure, interpretation, validity measurements and triangulation analysis. Bias risk was assigned as one of the following levels: satisfactory (S), dubious or not mentioned (D), and unsatisfactory (U). The nature of the sample was described as convenience (C) or purposive (P).
Mixed-method studies
Studies which combined qualitative and quantitative methods were scored by both risk of bias assessments listed above.
Summary measures, synthesis of results and risk of bias across studies
Meta-analysis was performed to obtain a summary measure based on pooled estimates on adherence determinants derived from the respective ORs, relative risks (RR) and corresponding 95% CI. If complete numbers of (non-)events were available, RRs were converted into ORs. If this was not possible, separate analyses for ORs and RRs were presented. Determinants reported in at least two studies were weighted based on the inverse of the variance as an estimate of statistical size. Owing to lack of reported risk estimates, not all studies included in this systematic review were suitable to be included. Statistical analyses were performed with RevMan V.5.3; (Review (RevMan) [Computer program]. Copenhagen: The Nordic Cochrane Centre The Cochrane Collaboration, 2014.) statistical significance was set at a two-sided p value of <0.05. Heterogeneity was measured using the I2 statistic.21 Possible publication bias was assessed visually through funnel plots per determinant.
Determinants were described narratively when based on qualitative data, or if pooling of results was not possible due to the nature of the data, using a mixed-methods approach. For mixed-methods studies, results were analysed as either quantitative or qualitative depending on reported outcome.
Results
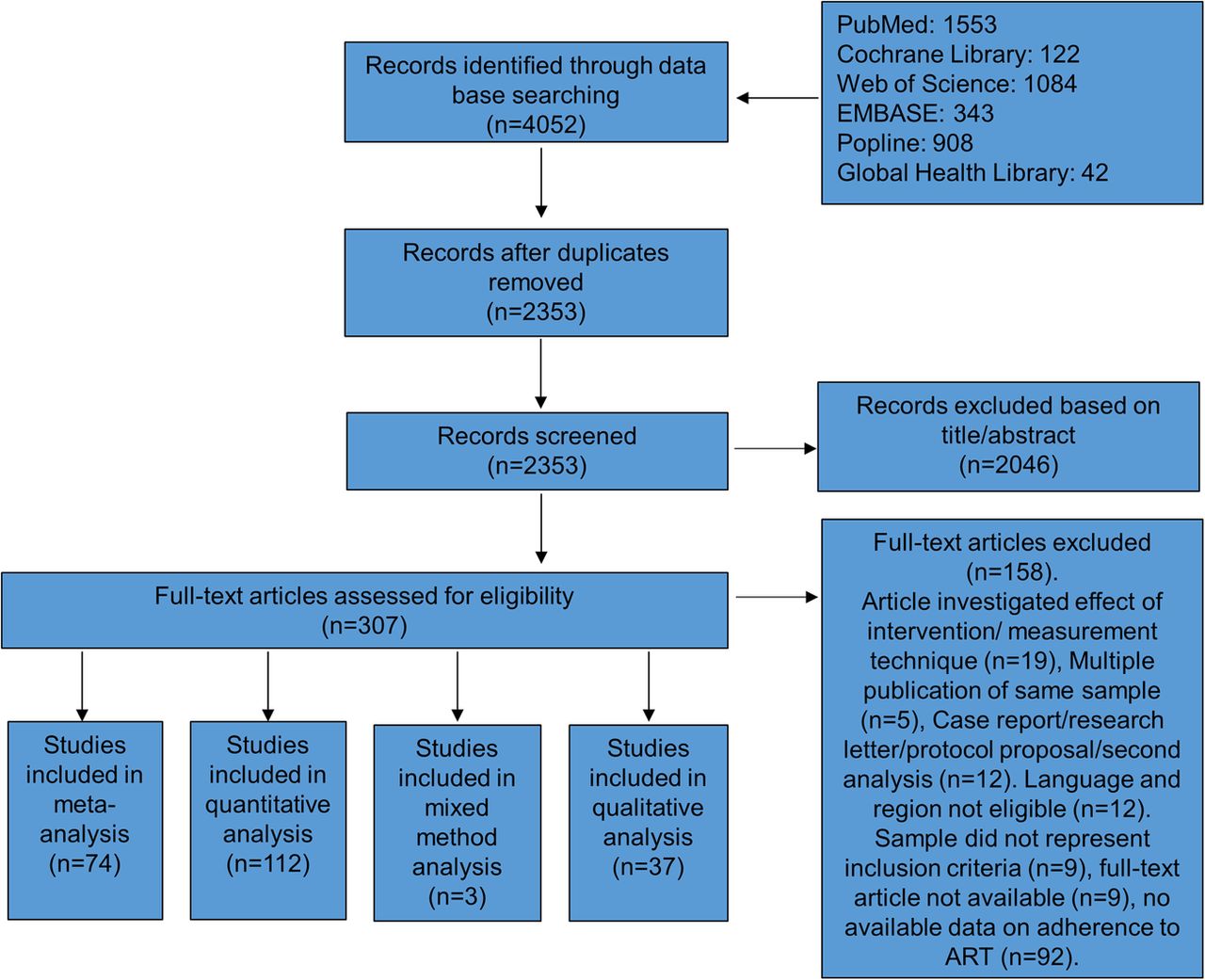
A total of 4052 articles were identified through the systematic literature search (see flow diagram in figure 1). After removing duplicates, 2353 articles were screened on title and abstract, 2046 articles did not meet inclusion criteria and were excluded. After full-text assessment of the remaining 307 articles, a total of 146 articles were included for the final analysis. Of these 146 articles reporting on determinants of (non-)adherence, 112 reported on quantitative and 37 qualitative data, with 3 studies using mixed methods.
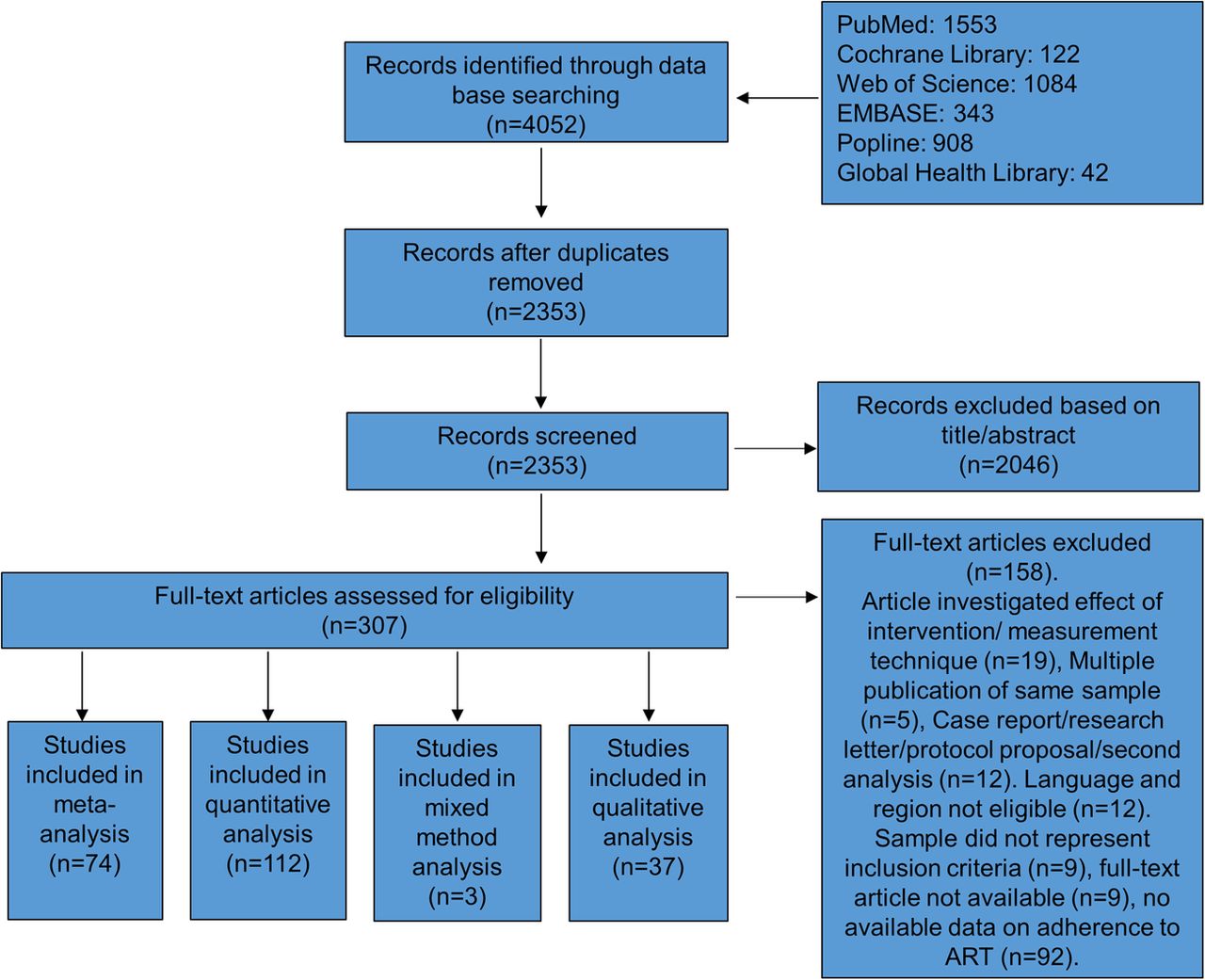
Flow diagram of the study selection for inclusion in the systematic review on determinants of adherence to ART in SSA. ART, antiretroviral treatment; SSA, sub-Saharan Africa.
Study characteristics of these articles are presented in table 1 and online supplementary data 2. Included studies were published between 2003 and 2014, and reported on 161 922 participants. Seventy-four articles reported on Central and East-Africa, 56 on Southern Africa and 36 on West-Africa. The average adherence rate was 52.5% (adherence 100%) and 72.9% (adherence 95%).
Overview of characteristics of studies on adherence of antiretroviral treatment (ART)
supplementary data
Bias assessment
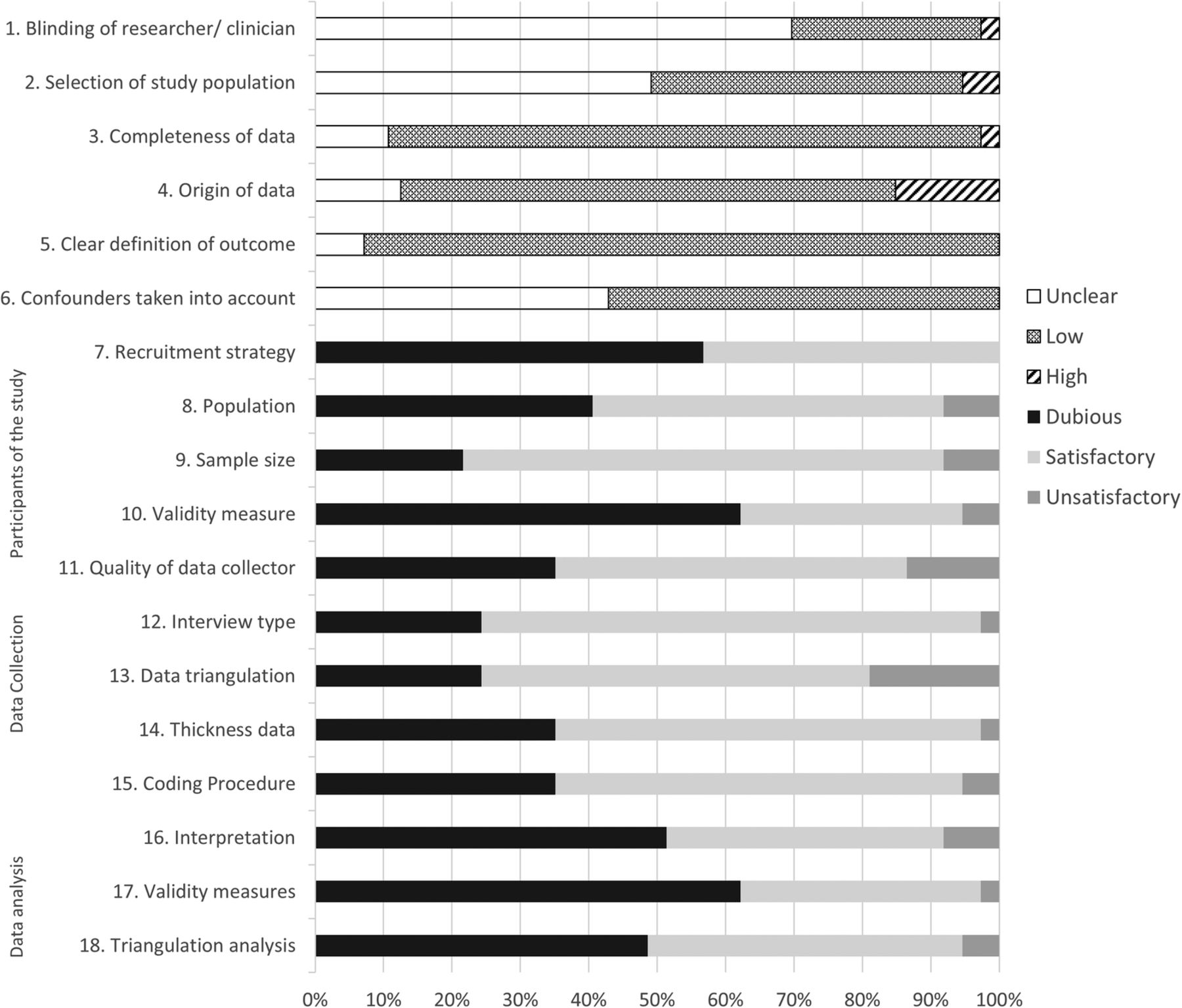
Overall the performance of risk of bias was reasonably well, with only a few studies reporting high risk of bias on one or more of the categories (25% quantitative, 51.3% qualitative). Risk of bias assessment of the quantitative and qualitative studies is summarised in figure 2. Details for bias assessment for individual studies can be found in online supplementary files 3 and 4.

Summary risk of bias assessment for qualitative (items 1–6) and qualitative7–18 studies on adherence to ART. ART, antiretroviral treatment.
supplementary data
supplementary data
For quantitative studies, blinding of researchers and selection of study population was frequently unclear (69.6% and 49.1%). The other categories scored reasonably well, especially completeness of data and clear definitions of outcome (86.6% and 92.9%). For qualitative studies, validity of measurements in data collection and data analysis were least well defined (62.1%). Recruitment strategy was unclear in 56.8%. Other categories scored reasonably well.
The funnel plots, where possible, showed on visual inspection some evidence of publication bias in smaller studies considering younger age, that is, 15–35 years, low or no education, and discrimination (see online supplementary data 4).
Determinants of (non-)adherence
Sociodemographic, socioeconomic and lifestyle factors
Sociodemographic and socioeconomic determinants were reported in 105 studies.
Age was reported by 20 articles to be a determinant for adherence, with better adherence seen in older patients (>35 years) compared with younger patients.22–41
Eighteen studies reported gender influences on adherence. Eleven reported better adherence for women,31 ,42–51 but six reported the opposite.22 ,28 ,41 ,52–54 Among men who had sex with men lower adherence was reported.55
Lower levels of education corresponded with non-adherence,42 ,45 ,52 ,53 ,56 ,57 and higher adherence was observed among patients with formal education.58–60 However, some articles reported the opposite.41 ,61–63
Alcohol use increased the risk of non-adherence.3 ,22 ,23 ,31 ,33 ,39 ,42 ,43 ,46 ,47 ,61 ,64–87 Suggested reasons were that patients may forget to take their medication as a consequence of alcohol use.33 ,67 ,78 Men may use alcohol to deny the reality of being HIV-positive.85
Religion was reported as both a barrier to and a promoter of adherence.33 ,67 ,71 ,74 ,79 ,82–85 ,88–102 Belief and faith that God provided the knowledge to make ART acts was observed to promote adherence,71 ,82 ,92 ,93 whereas studies reporting belief in religious cures for HIV over conventional medical approaches observed increased non-adherence.71 ,82 ,93
Employment showed conflicting outcomes; non-adherence was observed to be higher in unemployed54 ,61 ,64 ,96 and employed31 ,74 ,78 ,96 ,103 people. Similarly, both higher income and poverty were associated with non-adherence.3 ,28 ,42 ,47 ,49 ,51 ,52 ,56 ,59 ,85 ,87 ,96 ,104–107 Financial challenges, including transport costs, health facility costs and financial insecurity were associated with non-adherence.40 ,54 ,59 ,62 ,64 ,69 ,71 ,78 ,83 ,85 ,88 ,94 ,101 ,107–117 Food insecurity resulted in non-adherence through two mechanisms: stopping ART when food was unavailable to avoid aggravated (gastrointestinal) side effects, or because taking ART when insufficient food is available increased hunger.31 ,49 ,53 ,59 ,64 ,65 ,67 ,69 ,71 ,72 ,78 ,82 ,83 ,85 ,95 ,102 ,105 ,107 ,109 ,110 ,115 ,118–120
Other predictors reported to be associated with (non-)adherence were: distance to clinic,29 ,37 ,41 ,52 ,84 ,85 ,111 ,121 having children,88 ,93 ,106 ,110 ,114–116 ,122 geographical area,45 ,58 ,96 ,117 ,123 marital status,41 ,53 ,58 ,61 ,64 ,65 ,68 ,104 number of sexual partners,47 ,124 travelling,33 ,71 ,105 ,109 ,110 forgetting to take medication,59 ,71 ,83 ,84 hospital versus government ART initiative,51 living situation,87 tobacco use,47 unable to maintain healthy lifestyle122 and language barriers.36
Treatment and health facilities
Seventy-five articles reported treatment determinants affecting adherence. The majority of these mentioned the negative influence of side effects on adherence, such as chronic diarrhoea and body shaping effects, giving rise to the fear of involuntary disclosure of HIV status.3 ,23 ,28 ,33 ,42 ,53 ,56 ,57 ,59 ,62 ,67 ,69 ,71 ,79 ,83–85 ,88 ,94 ,95 ,102 ,107 ,110 ,114 ,115 ,120 ,121 ,125–130 The second most reported determinant was the influence of healthcare workers on patient adherence. A confidential and good relationship with healthcare providers resulted in better adherence. Non-adherence was seen when patients encountered unpleasant experiences with clinic staff, including rudeness, condemnation and fatigue.7 ,30 ,33 ,59 ,65–67 ,78 ,79 ,83–85 ,88 ,94 ,101 ,109 ,113 ,116 ,122 ,131
Health facility determinants associated with non-adherence included experiencing no privacy at the facility, due to crowded pharmacies, consultations with multiple patients and lost files. Long waiting times and limited clinic hours were reported to lead to non-adherence, especially for employed people who would need to take time off to collect their medication.3 ,7 ,33 ,65 ,67 ,69 ,78 ,79 ,83–85 ,87 ,88 ,94 ,97 ,101 ,107 ,109
Patients positive perceptions of ART, such as a strong belief in value of treatment and understanding importance of adherence,33 ,83 ,94 ,109 ,114 ,116 ,118 ,122 were associated with adherence, whereas rumours and false beliefs about ART, including that ART can cause harm and is a sexual stimulant, were associated with non-adherence.83 ,84 ,102 ,109 ,114 ,120 ,126
Duration of treatment was observed to be associated with both adherence29 ,56 ,64 ,74 ,124 ,132 ,133 and non-adherence.23 ,38 ,52 ,69 ,72 ,75 ,134 Studies reporting better adherence over time suggested that long-term experience with ART results in better knowledge and strategies to incorporate ART use in daily life, social support, longer exposure to healthcare services, returning of strength and increased ability to manage side effects.29 ,56 ,64 ,124 Reasons for increased non-adherence could be the experience of no instant consequences for non-adherence and risk behaviour like smoking and use of alcohol.69 A proposed concept for adherence support interventions to reduce the consequences of duration of adherence was a shift towards promoting adherence as a means to live, rather than only survive.23 ,75 ,134 Other treatment and healthcare facility-related determinants were: pill burden as a predictor for non-adherence,36 ,38 ,39 ,64 ,84 ,102 ,106 ,110 ,115 ,130 change in medication or treatment,56 ,65 ,74 ,83 ,109 ,114 medication type,7 ,26 ,37 ,42 ,64 ,103 ,135 ,136 missing scheduled visits,30 ,40 ,66 ,137 pharmacy stock out,40 ,42 ,48 ,67 dietary instructions,100 study type136 and unclearly defined ART dosage.3 ,102
Psychosocial
Seventy-three studies found psychosocial determinants affecting adherence. Disclosure, whereby people living with HIV hide or skip their medication to avoid disclosure of HIV status, was described most often in relation to non-adherence.4 ,22 ,26 ,32 ,41 ,50 ,61 ,68 ,69 ,75 ,77 ,84 ,85 ,90 ,91 ,122 ,125 ,131 ,137 ,138 Disclosing one's HIV status to spouse, children and others has been observed to be a predictor of receiving support and was observed to be associated with adherence.33 ,37 ,49 ,62 ,67 ,78 ,83 ,85 ,111 ,115 ,116 ,131 ,139 Similarly, material, emotional and social support was associated with adherence.29 ,33 ,38 ,52 ,64 ,73 ,82–85 ,88 ,94 ,101 ,107 ,109 ,113 ,115 ,119 ,125 ,129 ,131 ,140–143
Fear of discrimination and/or experiencing stigma were determinants of non-adherence. This included being laughed at, exclusion from activities, being fired and alienation.3 ,33 ,43 ,59 ,64 ,65 ,67 ,78 ,83 ,85 ,88 ,97 ,103 ,107 ,109,113–115 ,120 ,122 ,125 ,130 ,144 ,145 Depression was found to be a predictor for non-adherence, and included reasons such as ‘ready to die’ and ‘loss of hope of ever getting better’.25 ,43 ,71 ,73 ,77 ,82 ,87 ,94 ,105 ,113 ,120 ,140 ,142 ,146–149 Further factors strongly influencing adherence include coming to terms and acceptance of illness, for example, people with a desire to live and take care of children, and fear of returning to pre-ART health state.67 ,82 ,84 ,94 ,110 ,116 ,122 ,144 Conversely, difficulty in coming to terms and lack of belief in existence of HIV, and not feeling sick were barriers to adherence.3 ,33 Other determinants affecting both adherence and non-adherence were cognitive impairment,73 ,128 ,143 internalised stigma,43 ,68 ,73 ,82 known use of ART and/or HIV status of others,47 ,49 ,69 ,72 ,134 ,139 psychological distress,72 ,150 trauma,109 ,142 ,151 masculinity,85 ,122 ,152 sharing medication,35 ,94 lack of commitment to therapy,63 ,85 ,105 ,119 ,120 isolation from family,115 caring for family,114 ,121 wanting to return to life before ART,119 being accused of infecting others,102 psychiatric care service126 and stress.83
Health status
The most common health status-related determinant was perceived health status. Experiencing improved health on ART, increased confidence in medication, weight gain and being able to return to work were positively associated with adherence.3 ,33 ,44 ,47 ,82–85 ,88 ,90 ,92 ,101 ,102 ,108–110 ,113 ,115–117 ,119 ,129 ,144 However, some studies noted that improved health could result in non-adherence if people believed to have been cured.33 ,38 ,84 ,105 ,110 ,120 ,122 ,130 ,138 Studies assessing adherence in relation to participant's CD4 cell count were conflicting. Both low and high CD4 counts were reported to increase and decrease adherence to ARTs.23 ,25 ,32 ,37 ,38 ,96 ,137 ,153
Adherence to ART could be decreased when a patient needs to cope with multiple ailments including malaria, diabetes and high blood pressure—especially when asymptomatic for HIV.47 ,94 ,109 ,113 ,122 ,129 The following determinants predicted non-adherence to a lesser extent: body mass index,26 ,95 ,154 TB,50 ,73 ,74 WHO clinical stage,26 ,56 ,75 CDC staging criteria,133 haemoglobin,32 immune reconstitution inflammatory syndrome event81 and viral load.95
Counselling and education interventions
Counselling and education were mentioned by 20 articles to be associated with adherence. Adherence training commonly consisted of strategies to cope with the medication and its side effects. Patients who had poor knowledge of basic HIV concepts due to no or low-quality counselling were at higher risk of non-adherence.25 ,64 ,66 ,78 ,79 ,82 ,84–86 ,88 ,92 ,94 ,101 ,102 ,107 ,109 ,110 ,116 ,131
The use of memory aids like mobile phones, radio alarms, watches, clocks, reminders of children and pill boxes were observed to be associated with adherence,44 ,88 ,109 ,110 ,113 ,114 ,119 ,140 ,155 likewise implementation of ART in daily routines; not being able to do so was associated with non-adherence.3 ,29 ,69 ,85 ,102 ,105 ,109 ,110 ,125 ,144 Having a treatment partner or clinic buddy was observed to be associated with adherence.32 ,85 ,112 ,114 ,139 ,144 ,156 Receiving support by non-governmental organisation/government83–85 and adherence self-efficacy122 were also reported determinants of adherence.
A total of 14 studies found no significant determinants of adherence.157–165
Meta-analysis
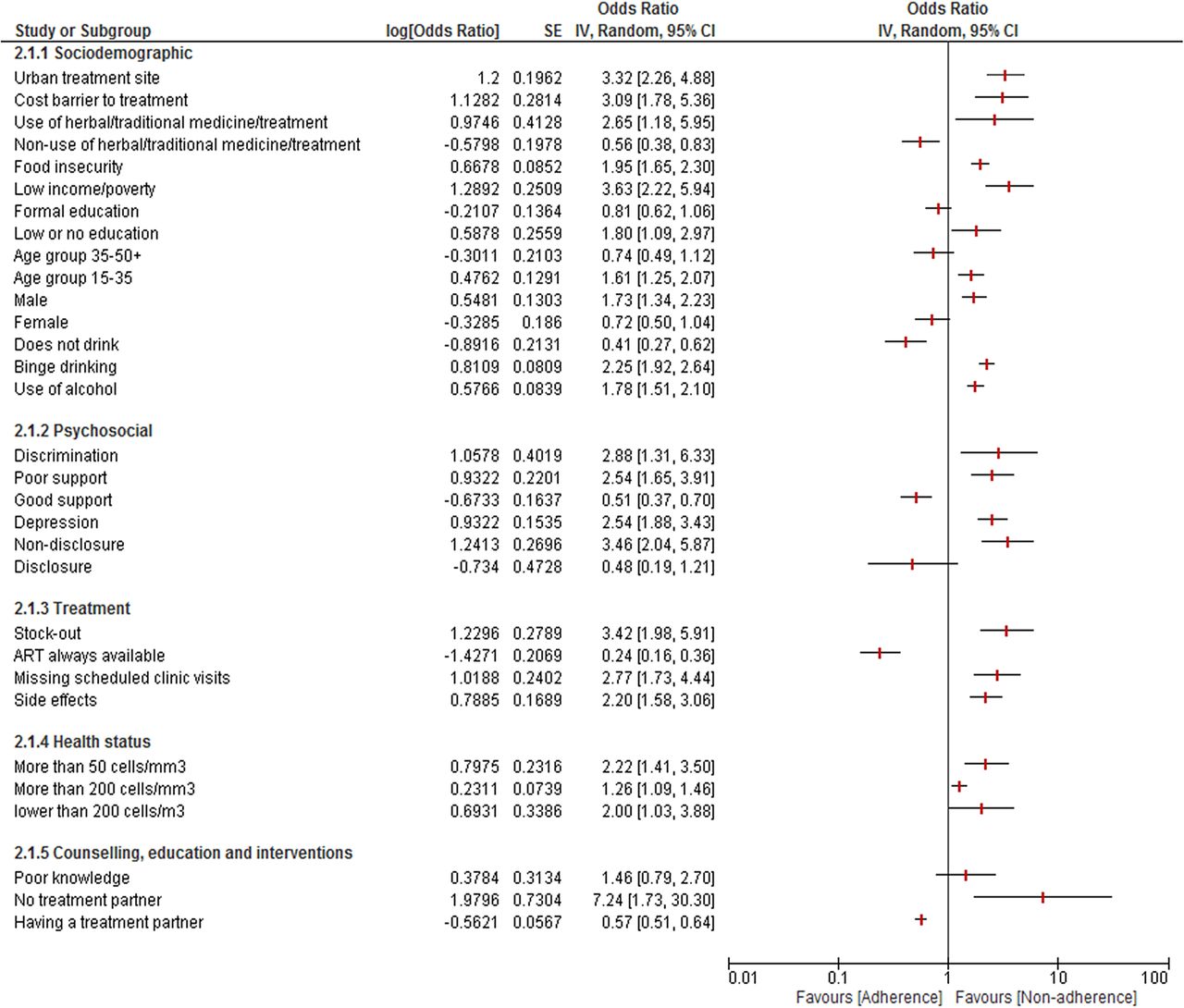
Meta-analysis could be performed for 25 determinants: 12 sociodemographic and socioeconomic factors, 5 psychosocial, 4 treatment-related and 2 health status and intervention-related determinants. Results are summarised in figure 3, sample sizes and number of studies included per determinant are presented in online supplementary data 5.
{kind=link}
{kind=link}
{kind=link}
Forrest plot meta-analysis for determinants of non-adherence to ART. ART, antiretroviral treatment.
supplementary data
Sociodemographic and socioeconomic factors
Determinants associated with a protective effect on adherence were not drinking alcohol (OR=0.41; 95% CI 0.27 to 0.65; I2=38%)22 ,39 and non-use of herbal/traditional medicine/treatment (OR=0.56; 95% CI 0.38 to 0.83).100
Non-adherence was associated with the following determinants: use of alcohol (OR=1.78; 95% CI 1.51 to 2.09; I2=39%),23 ,46 ,61 ,64 ,66 ,72 ,74 ,76 ,86 ,87 binge drinking (OR=2.25; 95% CI 1.92 to 2.65; I2=18%),31 ,42 ,46 ,47 ,65 ,70 ,73 ,75 ,86 male gender (OR=1.73; 95% CI 1.34 to 2.23; I2=60%),22 ,31 ,42 ,47 ,48 ,51 ,61 younger age (15–35 years; OR=1.61; 95% CI 1.25 to 2.06; I2=92%),30 ,32 ,34 ,35 ,37 ,39 ,40 ,61 low or no education (OR=1.80; 95% CI 1.09 to 2.98; I2=81%),30 ,75 ,78 ,93 ,97 ,114 ,118 use of herbal/traditional medicine/treatment (OR=2.65; 95% CI 1.18 to 5.95; I2=78%),90 ,91 ,95 ,96 ,98 low income or living below poverty level (OR=3.36; 95% CI 2.22 to 5.93; I2=66%),28 ,42 ,47 ,52 ,96 ,104 costs forming barriers to treatment (OR=3.09; 95% CI 1.78 to 5.37; I2=59%),40 ,59 ,62 ,111 ,117 urban treatment site or urban residence (OR=3.32; 95% CI 2.26 to 4.87; I2=0%)45 ,58 ,96 and food insecurity (OR=1.95; 95% CI 1.65 to 2.29; I2=13%).31 ,49 ,53 ,65 ,72 ,95
Other determinants were not significantly related to adherence, for example, formal education, (un)employment, high income and marital status. However, female gender and older age (35 to 50+ years) showed trends in favouring adherence (OR=0.72; 95% CI 0.50 to 1.03; I2=79%)26 ,36 ,38 and (OR=0.74; 95% CI 0.49 to 1.11; I2=86%),22 ,23 ,25 ,27 ,28 ,30 respectively.
Treatment and health facilities
Reliable ART availability (OR=0.24; 95% CI 0.16 to 0.37)40 was associated with increased adherence, whereas pharmacy stock-out was associated with non-adherence (OR=3.42; 95% CI 1.98 to 5.90; I2=0%).42 ,48 Other determinants associated with non-adherence were side effects (OR=2.20; 95% CI 1.58 to 3.07; I2=76%)23 ,42 ,53 ,57 ,62 ,121 ,126 ,128 ,129 ,165 and missing scheduled clinic visits (OR=2.77; 95% CI 1.73 to 4.43; I2=55%). Non-significant determinants were: change in regimen and/or treatment, and perceived health status by patients.
Psychosocial
Adherence was associated with good social support (OR=0.51; 95% CI 0.37 to 0.71; I2=0%).129 ,140 ,141 Determinants predictive for non-adherence were: non-disclosure to others (OR=3.46; 95% CI 2.04 to 5.89; I2=66%),49 ,52 ,53 ,64 ,66 ,137 ,138 depression (OR=2.54; 95% CI 1.65 to 3.91; I2=52%),25 ,43 ,73 ,87 ,140 ,147–149 poor social support (OR=2.54; 95% CI 1.65 to 3.91; I2=31%)29 ,64 ,73 ,143 and discrimination (OR=2.88; 95% CI 1.31 to 6.36; I2=73%).43 ,65 ,103 ,145 Psychological distress was not related to ART adherence.72 ,73
Health status
Contrary to the narrative assessment, CD4 count was predictive for non-adherence in the meta-analysis: CD4 ≥200 cells/mm3 (OR=1.26; 95% CI 1.09 to 1.46; I2=40%),25 ,32 ,37 ,96 CD4≤200 cells/mm3 (OR=2.00; 95% CI 1.03 to 3.87; I2=30%)23 ,137 and CD4≤50 cells/mm3 (OR=2.22; 95% CI 1.41 to 3.50).153
Discussion
Our systematic review complements the existing body of literature, and identified numerous determinants influencing adherence to antiretroviral medication in SSA. Significant determinants for quantitative and qualitative studies of non-adherence were the use of alcohol, male gender, use of traditional/herbal medicine, dissatisfaction with healthcare facility and healthcare workers, depression, discrimination and stigmatisation, and poor social support. Promoters of adherence included counselling and education interventions, memory aids, and active disclosure among people with HIV. Determinants of health status had conflicting influence on adherence.
Langebeek et al11 performed a meta-analysis on predictors of adherence globally, and Mills et al12 compared developed and developing countries. A number of comparable determinants were found including substance abuse, concerns about ART or necessity of ART, satisfaction with the healthcare provider, depression, stigma, social support, financial constraints and pill burden.11 Our approach focussed on determinants of adherence for people living with HIV in SSA, who constitute about two-third of HIV patients worldwide, and as such we were able to identify specific determinants relevant for this setting, including, for example, food insecurity, use of traditional herbs and medicine, and stigma. Trust and satisfaction with a healthcare provider may be more important in SSA countries with a low and medium Human Development Index,11 as well as issues of access to healthcare, impact of financial constraints, and disruption of services and medication distribution.12
A strength of this systematic review is our mixed-methods approach, in which we combined a meta-analysis with a narrative review and included both quantitative and qualitative studies and the comprehensive search undertaken including databases that specifically focus on low-income and middle-income country-based research.
A number of limitations should be considered. Importantly, this systematic review and inference of results is limited by the quality of the individual papers underlying the process. For example, a high risk of bias was introduced with the limited consideration of confounders on the association between determinant and exposure. Likewise, if studies did not ask about determinants, this information was not captured in this review, a rather general limitation of studies. As the majority of data extractions were completed by one reviewer, this could have introduced bias; however, all questions related to inclusion/exclusion of a study were discussed with the investigator team.
We observed significant heterogeneity in measurements and definition of optimal adherence and inclusion criteria for participants in the different studies. Various methods were employed to assess adherence: self-report questionnaires, pill count, pharmacy refill, visual analogue scale, viral load, CD4 cell count, Center for Adherence Support Evaluation (CASE), Community Programs for Clinical Research on AIDS (CPCRA), electronic medication monitors and the AIDS clinical trial group adherence scale. Although some have been validated, no consensus exists about the extent of their validity or gold standard. Direct measurement of blood drug level concentration was not used in any of the studies. We considered the heterogeneity in the assessment of risk of bias by assessing all varieties and their appropriateness and applicability within the paper. For example, self-report has been validated for adherence assessment in rural areas, and therefore was considered a low risk of bias method in this review, even though the exact execution will determine its ultimate validation. Future studies should consider seeking consensus for the optimal tool to assess adherence, building on the available assessment of methods166–168 and considering practical limitations for application in SSA settings. For example, the 30-day analogue scale may be a promising approach for its convenient and reliable results.168–172
Clinical implications
Our comprehensive overview of determinants that affect (non-)adherence could be of great use to optimise ART clinical service and adherence support within the current healthcare systems. Identified determinants allow for tailored support and interventions to be developed, evaluated and when effective, implemented in regions with scarce resources.
Interaction/clustering observed between determinants allow clinics to identify high-risk individuals most likely to benefit from targeted interventions. In fact, this is an active area of research and ample examples exist for specific evidence-based interventions.
For people living with HIV receiving ART who struggle with adherence as a result of the burden of monthly visits to crowded clinics, travel costs and/or time off work, a support group of several other persons receiving ART could be helpful whereby the group members take turns collecting medications.173 ,174
For the strongest individual predictor of (non-)adherence, alcohol use, a number of interventions have been identified. These include brief health provider-initiated alcohol interventions for people living with HIV8 ,175 and the WHO-proposed intervention framework with brief consultations focussed on alcohol reduction.176 Interventions focussed on younger patients include personalised, interactive and daily SMS reminders.177 Group-based counselling intervention for depression can potentially increase adherence.178 Other important interventions focus on improving quality of healthcare delivered in a system usually underfunded and overstretched. These include decentralisation of ART services, and task shifting from doctors and nurses to counsellors or community health workers.179 ,180
In conclusion, determinants of (non)-adherence in SSA identified in this review could facilitate the development, evaluation and implementation of targeted interventions. Given the increased accessibility of ART in SSA, optimising adherence will improve the health of millions of people living with HIV.
Acknowledgments
The authors would like to thank Professor Dr Rob Scholten for his advice on the meta-analysis conducted for the current study.
Footnotes
Handling editor Seye Abimbola
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/