- Manisha Nair1,
- Manoj K Choudhury2,
- Saswati S Choudhury3,
- Swapna D Kakoty3,
- Umesh C Sarma2,
- Premila Webster4,
- Marian Knight5
- On behalf of the IndOSS-Assam steering committee
- 1National Perinatal Epidemiology Unit (NPEU), Nuffield Department of Population Health, University of Oxford, Oxford, UK
- 2Srimanta Sankaradeva University of Health Sciences, Guwahati, Assam, India
- 3F.A.A. Medical College, Barpeta, Assam, India
- 4Oxford School of Public Health, Oxford Deanery, Oxford, UK
- 5NPEU, Nuffield Department of Population Health, University of Oxford, Oxford, UK
- Correspondence to Dr Manisha Nair; manisha.nair{at}npeu.ox.ac.uk
- Received 15 December 2015
- Revised 10 March 2016
- Accepted 11 March 2016
Abstract
Objectives To examine the association between maternal anaemia and adverse maternal and infant outcomes, and to assess the feasibility of conducting epidemiological studies through the Indian Obstetric Surveillance System–Assam (IndOSS-Assam).
Design Retrospective cohort study using anonymised hospital records. Exposure: maternal iron deficiency anaemia; outcomes: postpartum haemorrhage (PPH), low birthweight, small-for-gestational age babies, perinatal death.
Setting 5 government medical colleges in Assam.
Study population 1007 pregnant women who delivered in the 5 medical colleges from January to June 2015.
Main outcome measures ORs with 95% CIs to estimate the association between maternal iron deficiency anaemia and the adverse maternal and infant outcomes. Potential interactive roles of infections and induction of labour on the adverse outcomes were explored.
Results 35% (n=351) pregnant women had moderate–severe anaemia. Women with severe anaemia had a higher odds of PPH (adjusted OR (aOR) =9.45; 95% CI 2.62 to 34.05), giving birth to low birthweight (aOR=6.19; 95% CI 1.44 to 26.71) and small-for-gestational age babies (aOR=8.72; 95% CI 1.66 to 45.67), and perinatal death (aOR=16.42; 95% CI 4.38 to 61.55). Odds of PPH increased 17-fold among women with moderate–severe anaemia who underwent induction of labour, and 19-fold among women who had infection and moderate–severe anaemia.
Conclusions Maternal iron deficiency anaemia is a major public health problem in Assam. Maternal anaemia was associated with increased risks of PPH, low birthweight, small-for-gestational age babies and perinatal death. While the best approach is prevention, a large number of women present with severe anaemia late in pregnancy and there is no clear guidance on how these women should be managed during labour and delivery.
Key questions
What is already known about this topic?
Assam, a north-eastern state in India, is reported to have high maternal and infant mortality. It has been hypothesised that iron deficiency anaemia is a major causal factor. However, there is limited research evidence of a causal relationship with maternal and neonatal mortality in Assam.
What are the new findings?
This study was part of a pilot study conducted to assess the feasibility of establishing an Indian obstetric surveillance and research system in the state of Assam (IndOSS-Assam) and demonstrated the feasibility of using routine medical records for future prospective epidemiological studies linked to the surveillance system.
This study showed a high prevalence of iron deficiency anaemia among pregnant women in Assam, which highlights that this is an important public health problem. Maternal anaemia was associated with increased risks of postpartum haemorrhage, low birthweight, small-for-gestational age babies and perinatal death.
The odds of postpartum haemorrhage increased 17-fold, notably among women with moderate–severe anaemia who underwent induction of labour.
Recommendations for policy
Clearly, the best approach is to prevent anaemia or to treat it during the antenatal period, but a large number of pregnant women in India present with severe anaemia either at the point of delivery or in the third trimester. At present, there is no clear guidance with regard to how women with severe anaemia should be managed during labour and delivery, and further studies are required to generate evidence in order to inform policy and practice.
Introduction
Assam, a north-eastern state in India, is reported to have a high maternal mortality ratio (MMR) as well as a high infant mortality rate (IMR). A report published by the Office of the Registrar General, India, estimated the MMR to be 328/100 000 live births for the years 2010–20121 and IMR to be 55/1000 live births for the year 2011.2 It has been hypothesised that iron deficiency anaemia is a major cause of the high maternal and infant mortality in the state. Assam has the highest prevalence of iron deficiency anaemia among pregnant women (73%, Indian National Family Health Survey 2005–2006).3 A study in one tertiary hospital in the state showed that maternal haemoglobin (Hb) levels <8 g/dL were associated with increased risk of low birthweight and small-for-gestational age babies,4 but we did not find any study that examined the effects on maternal and perinatal outcomes.
Iron deficiency anaemia during pregnancy is a known risk factor for preterm birth, low birthweight and small-for-gestational age babies,5 and increases the risk of postpartum haemorrhage (PPH).6 PPH is the leading cause of maternal mortality in India.7 The incidence of PPH is much higher in India compared with the rest of the world and the Registrar General of India attributes this to the high prevalence of anaemia among pregnant women.8 A study investigating the causes of neonatal deaths among the tea garden labourers in Assam reported a high prevalence of low birth weight (43%) and preterm deliveries (34%) in the study population, contributing to >90% of the neonatal deaths.9
While untreated iron deficiency anaemia can itself lead to adverse outcomes, its negative effects may be aggravated by the presence of other risk factors such as infections during pregnancy (malaria,10 urinary tract infection (UTI),11 helminthic infections12). Additionally, studies have suggested that induction of labour is associated with increased risk of PPH.13 ,14 These factors could augment the adverse effects of anaemia on pregnancy outcomes. The objectives of this study were to examine the association between maternal anaemia and PPH, low birthweight, small-for-gestational age babies and perinatal death. In addition, we explored the potential interactive role of infections and induction of labour on the adverse effects of iron deficiency anaemia.
Methods
We conducted a cohort study using anonymised hospital records of pregnant women (>20 weeks of gestation) who underwent delivery in five government medical colleges and hospitals in Assam: Gauhati Medical College and Hospital (GMCH), Guwahati; Assam Medical College and Hospital (AMCH), Dibrugarh; Silchar Medical College and Hospital, Silchar; Fakhruddin Ali Ahmed Medical College and Hospital (FAAMCH), Barpeta; and Jorhat Medical College and Hospital, Jorhat. This study was part of a pilot study conducted to assess the feasibility of establishing an Indian obstetric surveillance and research system in the state of Assam (IndOSS-Assam). Details of the feasibility study are described separately.15 This retrospective study was undertaken to establish the feasibility of using routine medical records for future prospective epidemiological studies linked to the surveillance system.
A data collection form adapted from the Indian Demographic and Health Survey questionnaire and UK Obstetric Surveillance System16 was used to collect anonymous information from the hospital and antenatal records of pregnant women. Data were collected sequentially from the five study sites, for 1 month per site, over a period of 6 months (January–June 2015) to include an average of 200 women per site for an even distribution of the required sample. All women admitted to the postnatal ward of the hospital during the study month were included (until the sample size of 200 was reached) and data were collected from their hospital records by field staff from the Regional Resource Centre, Guwahati, Assam.
The primary exposure for this cohort study was maternal iron deficiency anaemia defined using the WHO criteria for moderate anaemia (pregnant women with an Hb level of 7–9.9 g/dL) and severe anaemia (Hb level <7 g/dL).17 The other exposures, malaria, UTI, helminthic infections and induction of labour, were recorded on the basis of reported diagnoses by clinicians from the women's hospital and antenatal records. The primary outcomes of interest were: (1) primary PPH defined as pregnant women of 20 weeks gestation or more identified as having a blood loss of 500 mL or more from the genital tract within 24 h of birth of a baby18 and (2) low birthweight defined as weight at birth of <2500 g. In addition, we examined two other secondary infant outcomes: small-for-gestational age babies and perinatal death which included stillbirths and neonatal deaths within the first week of life.
The hospital notes did not have information on Hb levels recorded at different gestational periods for each woman. Therefore, we included most recently recorded antenatal Hb concentration and noted the gestational age at which it was recorded. We tested the continuous variable ‘haemoglobin level’ for deviations from linearity. Fitting fractional polynomials showed the presence of a non-linear relationship of Hb level with the outcomes PPH, low birthweight and small-for-gestational age babies. We therefore categorised pregnant women into three groups: mild anaemia/normal Hb, moderate anaemia and severe anaemia.
Gender-specific z-scores and centiles for birthweight-for-gestational age were generated using the INTERGROWTH-21st tool19 for all singleton pregnancies. Infants below the 10th centile or with a z-score <−1.28 were grouped as small-for-gestational age.
We also collected information on known confounders and risk factors for maternal and infant morbidity and mortality including sociodemographic factors such as maternal age, body mass index (BMI), caste (social class), religion, residence, below poverty line status, women's employment status, husband's occupational status and whether he was a tea garden worker; pregnancy-related factors such as parity, previous caesarean section, interpregnancy interval, previous pregnancy problems, pre-existing medical problems, multiple pregnancies, number of antenatal visits, whether folic acid tablets were received and mode of delivery. BMI was calculated from the earliest available information on weight and height of pregnant women measured during the antenatal period, but we do not know the exact time point at which it was measured.
Study power and sample
India is reported to have a high incidence of PPH;8 therefore, a risk of 16% was used for estimating the sample size. For the outcome low birthweight, the reported overall incidence of 37.3% in the state20 was used for the purpose of sample size calculation. Assuming an effect size for the risk ratio to be 1.5, power as 80%, α 5%, and ratio of unexposed to exposed 2, for the above proportions of risk in the unexposed group, we estimated a sample of 230 in the exposed group for the outcome PPH and 70 in the exposed group for low birth weight. These estimates were inflated to account for cluster sampling and possible missing information to give a final estimated sample size of 980.
Statistical analyses
We conducted an initial descriptive analysis to compare the distribution of the confounders and other risk factors across the three exposure groups and univariable analyses to examine the crude ORs for the association between exposure and outcomes. We conducted explanatory multivariable logistic regression analyses using separate models to investigate the associations of maternal anaemia with PPH, low birthweight, small-for-gestational age babies and perinatal death.
We conducted tests for interaction by fitting interaction terms for maternal anaemia and infections during pregnancy for the outcomes PPH, low birthweight and small-for-gestational age babies, and maternal anaemia and induction of labour for PPH followed by likelihood ratio tests. We found significant interaction between these variables; therefore, dummy variables were generated to ascertain the effects of these interactions on the outcomes in separate multivariable logistic regression analyses.
Tests for correlation between the independent variables showed a high correlation between parity and the interpregnancy interval; this variable was therefore not included in the multivariable model. We also found a significant correlation between husbands’ employment status and below poverty line household, as well as between husbands’ employment status and that of the tea garden worker; thus, husbands’ employment status was excluded to improve model parsimony. The final multivariable models therefore adjusted for the following risk factors: caste, religion, residence, below poverty line status, women's employment status, tea garden worker, parity, BMI, maternal age, previous caesarean section, previous pregnancy problems, placental problems in index pregnancy, pre-existing medical problems, multiple pregnancies, number of antenatal visits, whether folic acid tablets were received, and mode of delivery. Mode of delivery was not included in the infant outcomes model as this is not likely to be causally associated.
A substantial proportion of the data was missing for BMI, parity, previous pregnancy problems and below poverty line status. We did not assume the data to be missing at random and generated proxy variables with missing as a separate group for all variables. However, we also conducted complete case analysis for all outcomes and sensitivity analyses by redistributing the missing observations into the different categories of the variables. The results of complete case analyses and sensitivity analyses did not materially differ from that of the main models other than to widen the 95% CI, except for small-for-gestational age for which results could not be obtained as the dependent variable did not vary within the severe anaemia group in complete case analysis (see online supplementary table S1).
Supplementary table
On the basis of the sampling frame, clustering of data was at the level of the tertiary hospital which caters to the population within a definite geographical boundary. We did not consider the intraclass correlation coefficient to be high because the geographical areas that the five tertiary hospitals serve are large with a heterogeneous population. Further, the sampling used a single stage cluster design with five large clusters; thus, we employed the Hubert-White robust SEs method to account for any clustering effect. All associations were considered to be significant at a p value of <0.05 (two tailed) and all analyses were performed using Stata V.13.1, SE (StataCorp, College Station, Texas, USA).
Results
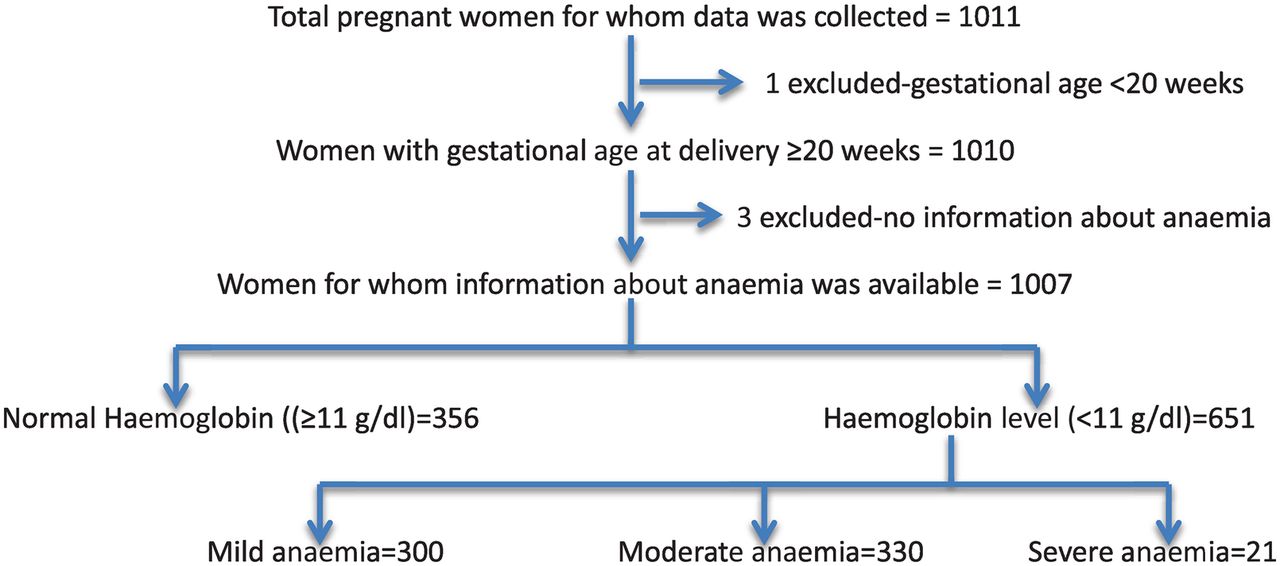
Information was collected for a total of 1011 pregnant women. After excluding one woman who delivered at <20 weeks gestation and three women for whom information on the Hb level was not available, we had a sample of 1007 women (figure 1).
{kind=link}
Flow chart to show the study population.
On the basis of the information available from the hospital records, 33 of the 1007 women (3.3%) had a PPH. Eleven women were reported to have a blood loss of 500–999 mL, 6 between 1000 and 1499 mL, another 6 had >1500 mL of blood loss in the first 24 h after delivery and for the remaining 10, estimates of blood loss were not available. In 73% of the PPH cases, the reported cause was uterine atony (n=24); other causes included placenta praevia (n=2), placental abruption (n=1), uterine infection (n=2), tears/injuries (n=2) and retained placenta (n=2).
We found a high prevalence (n=263 of the 969, 27%) of low birthweight among live-born singleton pregnancies in the study population and a higher prevalence of small-for-gestational age (n=409 of the 969, 42%). There were 33 perinatal deaths of the 989 singleton pregnancies (3.3%), 20 stillbirths and 13 neonatal deaths which occurred either on the day of delivery or within 2 days of birth.
Among the 1007 pregnant women, 28% (n=282) had the most recently recorded Hb in the first trimester (1–12 weeks of gestation), 37% (n=372) in the second trimester (13–27 weeks), 30% (n=302) in the third trimester (28–40 weeks), and for the remaining 5% (n=51) the date of Hb record was not available. Overall, 65.1% had mild anaemia/normal Hb levels (356 women with normal Hb≥11 g/dL, and 300 with mild anaemia 10–10.9 g/dL), 32.8% had moderate anaemia (n=330) and 2.1% (n=21) had severe anaemia during the antenatal period. Just over a quarter of women (n=141) received treatment for anaemia including iron supplementation, blood transfusion or other treatments (such as herbal remedies).
The sociodemographic and pregnancy-related characteristics of the women are shown in table 1. After adjusting for the sociodemographic and pregnancy-related characteristics, we found that compared with women with mild anaemia/normal Hb level, women with severe anaemia had a more than ninefold higher odds of PPH (adjusted OR (aOR) 9.45; 95% CI 2.62 to 34.05), a sixfold higher odds of giving birth to a low birthweight baby (aOR 6.19; 95% CI 1.44 to 26.71), and an almost ninefold higher odds of having a small-for-gestational age baby (aOR 8.72; 95% CI 1.66 to 45.67) (table 2). Women with moderate anaemia also had higher odds of PPH, low birthweight and small-for-gestational age babies compared with women with mild anaemia/normal Hb level, but the association was statistically significant only for the low birthweight outcome (table 2).
Comparison of maternal and infant characteristics across the exposure groups
Association between maternal anaemia and maternal and infant outcomes
The odds of PPH were 17-fold higher among women who had moderate–severe anaemia and underwent induction of labour compared with women who had neither of these exposures. Similarly, the odds of PPH were almost 19-fold higher among women who had moderate–severe anaemia and infection during pregnancy compared with women who had neither of these risk factors (table 2). The associations between moderate–severe anaemia and infant outcomes, low birthweight and small-for-gestational age were observed to not vary according to the presence of maternal infection during the antenatal period. Women with severe anaemia were observed to have a 16-fold higher odds of perinatal mortality compared with women with mild anaemia/normal Hb levels (table 2).
Calculated study power based on estimated prevalence of the outcomes in the study population
The prevalence of the outcomes PPH and low birthweight was found to be lower than the figures available from the literature; therefore, we calculated the study power for each outcome on the basis of the estimated prevalence of the outcomes in the study population and the final sample. For a prevalence of 2.3% PPH in the unexposed population, with 351 participants in the exposed group (ratio of unexposed (mild anaemia/normal Hb) to exposed (moderate–severe anaemia)=1.9), our study had 80% power to detect significantly an OR of 2.28 or greater associated with maternal anaemia at p<0.05 (two-tailed). For the prevalence of 25% low birthweight babies in the unexposed population, with 351 participants in the exposed group (ratio of unexposed to exposed=1.9), our study had 80% power to detect significantly an OR of 1.29 or greater. For a prevalence of 44% small-for-gestational age babies in the unexposed group (351 participants in the exposed group, ratio of unexposed to exposed=1.9), our study had 80% power to detect significantly an OR of 1.19 or greater, and for a prevalence of 2.8% perinatal deaths in the unexposed group (351 participants in the exposed group, ratio of unexposed to exposed=1.9), our study had 80% power to detect significantly an OR of 1.16 or greater.
Discussion
We were able to use the IndOSS-Assam surveillance and research system successfully to conduct this cohort study. The study showed that after adjusting for other risk factors, women with severe anaemia were at a significantly higher risk of PPH, giving birth to low birthweight and small-for-gestational age babies, and having a baby who died in the perinatal period. The odds of these adverse outcomes were also higher among women with moderate anaemia, but only the association with low birth weight was statistically significant. Importantly, the risk of PPH increased 17-fold among women with moderate–severe anaemia who underwent induction of labour.
Limitations of this study
This was a retrospective cohort study based on information collected from the hospital records of pregnant women. There are known issues related to estimation of blood loss in the peripartum period and after delivery through observation alone; therefore, we cannot ignore the possibility of misclassification. We were also not able to grade the severity of PPH. As discussed above, the hospital notes did not have records of the Hb level at different gestational periods; thus, the effects of anaemia in relation to the different gestational periods could not be ascertained. Another inherent limitation of collecting data from hospital records is a high proportion of missing data, which was evident in our study. However, the estimated ORs using complete case analysis and sensitivity analyses were not substantively different from the outputs of the main models.
Findings in relation to other studies
A number of studies in India and in other low and middle income countries (LMICs) have shown that anaemia during pregnancy is associated with increased risk of PPH,6 ,21 low birthweight4 ,5 ,21 and small-for-gestational age babies.4 ,21 Our results, in relation to the adverse neonatal outcomes, are comparable to the other study in Assam conducted in one hospital (n=421).4 Studies from other countries show varying results when examining the association between maternal anaemia on the risk of perinatal death. One study in Pakistan found maternal anaemia to be associated with increased risk of stillbirth,22 but another in China showed that a Hb level <9 g/dL in the third trimester was associated with a reduced risk of stillbirth and maternal anaemia was not associated with neonatal death.23 A study that used National Maternal and Infant Health Survey data in the USA found moderate anaemia to be associated with an increased risk of stillbirth among non-black women, but found no statistically significant association among black women.24
Individual associations of infections during pregnancy and maternal anaemia with adverse maternal and fetal outcomes have been shown by several studies.5 ,6 ,10 ,12 It is known that there is a causal relationship between infections and anaemia during pregnancy.11 We found a significant additive effect of infection and moderate–severe anaemia on increased risk of PPH, but this was not observed for the infant outcomes.
We observed a 17-fold increased risk of PPH among pregnant women with moderate–severe anaemia who underwent induction of labour. A few small studies have suggested that women with severe anaemia are more likely to have uterine atony due to impaired transport of oxygen and Hb to the uterus,6 ,21 but there is no strong evidence. This could be a possible explanation for the increased risk of PPH observed among pregnant women with moderate–severe anaemia who underwent induction of labour in this study, but it is also possible that other mechanisms exist.
Implications and future research
We found a high prevalence of iron deficiency anaemia among pregnant women in Assam which highlights that this is an important public health problem. Maternal anaemia was associated with increased risks of PPH, low birthweight, small-for-gestational age babies and perinatal death. Clearly, the best approach would be to prevent anaemia or to treat it during the antenatal period, but the Annual Health Survey showed that only 23% of the pregnant women in Assam consumed the complete course of iron–folic acid tablets in 2012–2013 (a slight improvement from 15.3% in 2010–2011).25 A large number of pregnant women in India present with severe anaemia either at the point of delivery or in the third trimester.26 ,27 In this study, 62% of the women with severe anaemia had low Hb levels during the third trimester of pregnancy when there is little scope for prevention or iron treatment.
At present, there is no clear guidance with regard to how women with severe anaemia should be managed during labour and delivery. The WHO guidelines on induction of labour do not provide any recommendation with regard to whether induction of labour should be carried out in women with severe anaemia;28 nor do the guidelines on management of anaemia make recommendations for management of women with moderate–severe anaemia during labour and delivery.17 Considering the high prevalence (35%) of moderate–severe anaemia among pregnant women in the study population and in several LMICs (an estimated 42% of pregnant women suffer from anaemia globally29), and its association with PPH and high risk of maternal death, further consideration needs to be given to generating evidence on the appropriate management of pregnant women with moderate–severe anaemia during the peripartum period to prevent maternal morbidity and mortality.
By successfully conducting this pilot study, we were able to demonstrate that the IndOSS-Assam platform can be used to conduct epidemiological research. A number of studies will be undertaken through this platform in the near future to test the hypotheses generated in this study, and to examine the risk factors, management and outcomes of other pregnancy complications in order to improve care.
Footnotes
Handling editor Seye Abimbola
Contributors MN designed the study, trained the field staff, conducted literature searches, planned and carried out the data analysis, interpreted the data, and wrote the first draft of the manuscript. MKC designed the study, trained the field staff, supervised data collection and data entry, and edited the manuscript. SSC designed the study, trained the field staff, supervised data collection and data entry, and edited the manuscript. SDK designed the study, trained the field staff, and edited the manuscript. UCS designed the study, trained the field staff, supervised data collection, and edited the manuscript. PW designed the study, and edited the manuscript. MK designed the study, contributed to the data analysis plan, data interpretation, and to the writing of the manuscript.
Funding This study was funded by the John Fell Oxford University Press (OUP) Research Fund, PRAC/JF/131/124; and by the Srimanta Sankaradeva University of Health Sciences, Assam. MK is funded by a National Institute for Health Research (NIHR) Research Professorship.
Disclaimer The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Competing interests None declared.
Ethics approval The IndOSS-Assam feasibility study, of which this retrospective study was a part, was approved by the Institutional Ethics Committee of Srimanta Sankaradeva University of Health Sciences (No SSUHS/Ethics/2014/1, dated 27 June 2014); the Health Ministry's Screening Committee, Indian Council of Medical Research (No 5/7/12 12/14-RCH, dated 25 September 2014) and the University of Oxford's Oxford Tropical Research Ethics Committee (OxTRTEC Reference 57-14).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/