Article Text

Abstract
Background Between 1964 and 1996, the 10-year survival of patients having valve replacement surgery for rheumatic heart disease (RHD) in the Northern Territory, Australia, was 68%. As medical care has evolved since then, this study aimed to determine whether there has been a corresponding improvement in survival.
Methods A retrospective study of Aboriginal patients with RHD in the Northern Territory, Australia, having their first valve surgery between 1997 and 2016. Survival was examined using Kaplan-Meier and Cox regression analysis.
Findings The cohort included 281 adults and 61 children. The median (IQR) age at first surgery was 31 (18–42) years; 173/342 (51%) had a valve replacement, 113/342 (33%) had a valve repair and 56/342 (16%) had a commissurotomy. There were 93/342 (27%) deaths during a median (IQR) follow-up of 8 (4–12) years. The overall 10-year survival was 70% (95% CI: 64% to 76%). It was 62% (95% CI: 53% to 70%) in those having valve replacement. There were 204/281 (73%) adults with at least 1 preoperative comorbidity. Preoperative comorbidity was associated with earlier death, the risk of death increasing with each comorbidity (HR: 1.3 (95% CI: 1.2 to 1.5), p<0.001). Preoperative chronic kidney disease (HR 6.5 (95% CI: 3.0 to 14.0) p≤0.001)), coronary artery disease (HR 3.3 (95% CI: 1.3 to 8.4) p=0.012) and pulmonary artery systolic pressure>50 mm Hg before surgery (HR 1.9 (95% CI: 1.2 to 3.1) p=0.007) were independently associated with death.
Interpretation Survival after valve replacement for RHD in this region of Australia has not improved. Although the patients were young, many had multiple comorbidities, which influenced long-term outcomes. The increasing prevalence of complex comorbidity in the region is a barrier to achieving optimal health outcomes.
- Child health
- Public Health
- Thoracic surgery
- Treatment
Data availability statement
Data are not publicly available. Data may be obtained from a third party upon reasonable request. Data cannot be shared publicly because of the Northern Territory Health Services Act 2014. A dataset is available from the Northern Territory Human Research Ethics Committee (contact via email ethics@menzies.edu.au) for researchers who meet the criteria for access to confidential data.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Aboriginal people with rheumatic heart disease (RHD) die, on average, 20 years earlier than Aboriginal people without RHD and over 30 years earlier than non-Aboriginal Australians.
WHAT THIS STUDY ADDS
Despite recent advances in surgical technique, perioperative care and the management of medical comorbidities in Australia’s universal health system, the survival of Aboriginal people requiring RHD valve replacement surgery in the region between 1997 and 2016 has fallen to 62%.
Half of the premature deaths were related to comorbidities; the risk of death increased with each additional comorbidity.
Although the median age of adults at the time of initial RHD surgery was only 35, almost three-quarters already had significant comorbidity, while 40% had multiple comorbidities.
Pulmonary artery systolic pressure≥50 mm Hg was one of three factors that were independently associated with death during long-term follow-up.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The results provide a rationale for integrating RHD care into the prevention and longitudinal management of the other chronic diseases that are common in the Aboriginal population.
The study suggests earlier surgery—before pulmonary artery systolic pressure becomes dangerously elevated—may improve long-term outcomes.
Introduction
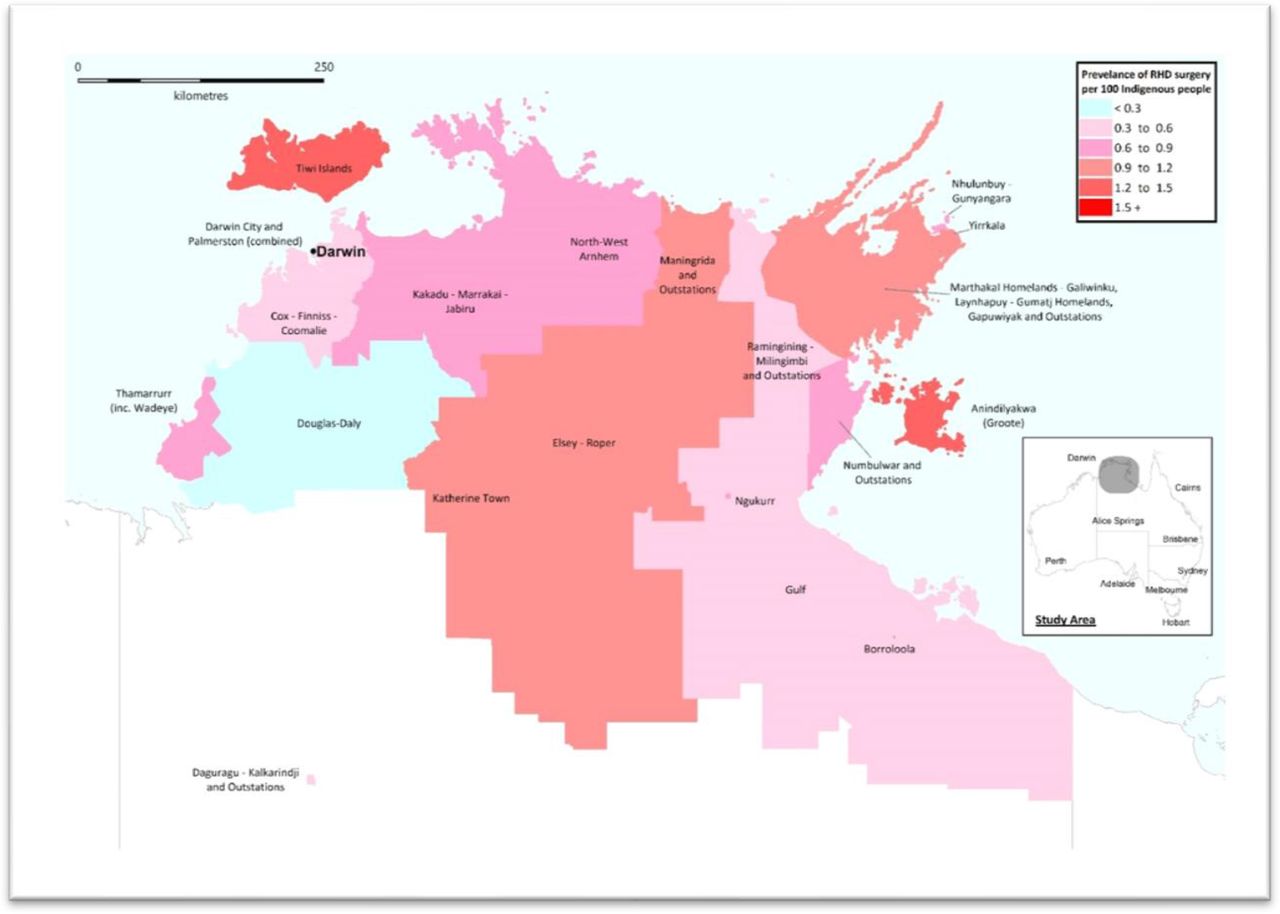
Rheumatic heart disease (RHD) is almost entirely preventable. Yet, the rate of RHD in the Aboriginal (Aboriginal is used throughout this paper to be respectful and inclusive of all peoples who identify as Aboriginal, Torres Strait Islanders, First Nations or Indigenous Australians) population in Australia’s Northern Territory (NT) is as high as anywhere in the world and more than 50 times higher than the general Australian population (figure 1).1 Aboriginal people with RHD die, on average, 20 years earlier than Aboriginal people without RHD and over 30 years earlier than the non-Aboriginal Australian population.2
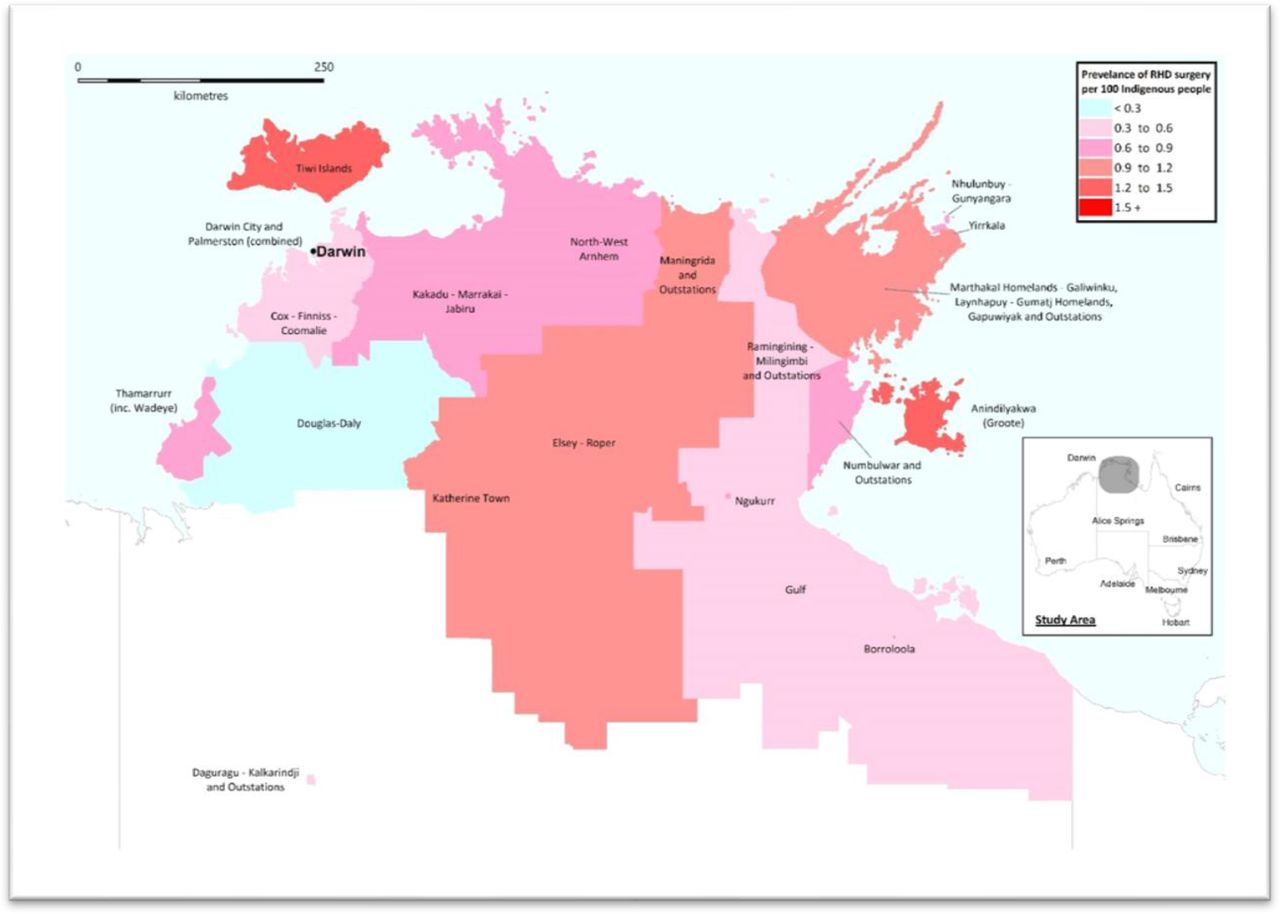
The prevalence of rheumatic heart disease (RHD) surgical patients within Aboriginal regions across the Top End of the Northern Territory. The map was constructed using mapping software (MapInfo Professional V 2019, Connecticut, USA) using Indigenous Locations data provided by the Australian Bureau of Statistics under Creative Commons Attribution 4.0 International licence (https://creativecommons.org/licenses/by/4.0/). It includes all surgical patients at the time of the 2016 census. The regions are presented as they are defined by cardiology services at Royal Darwin Hospital.
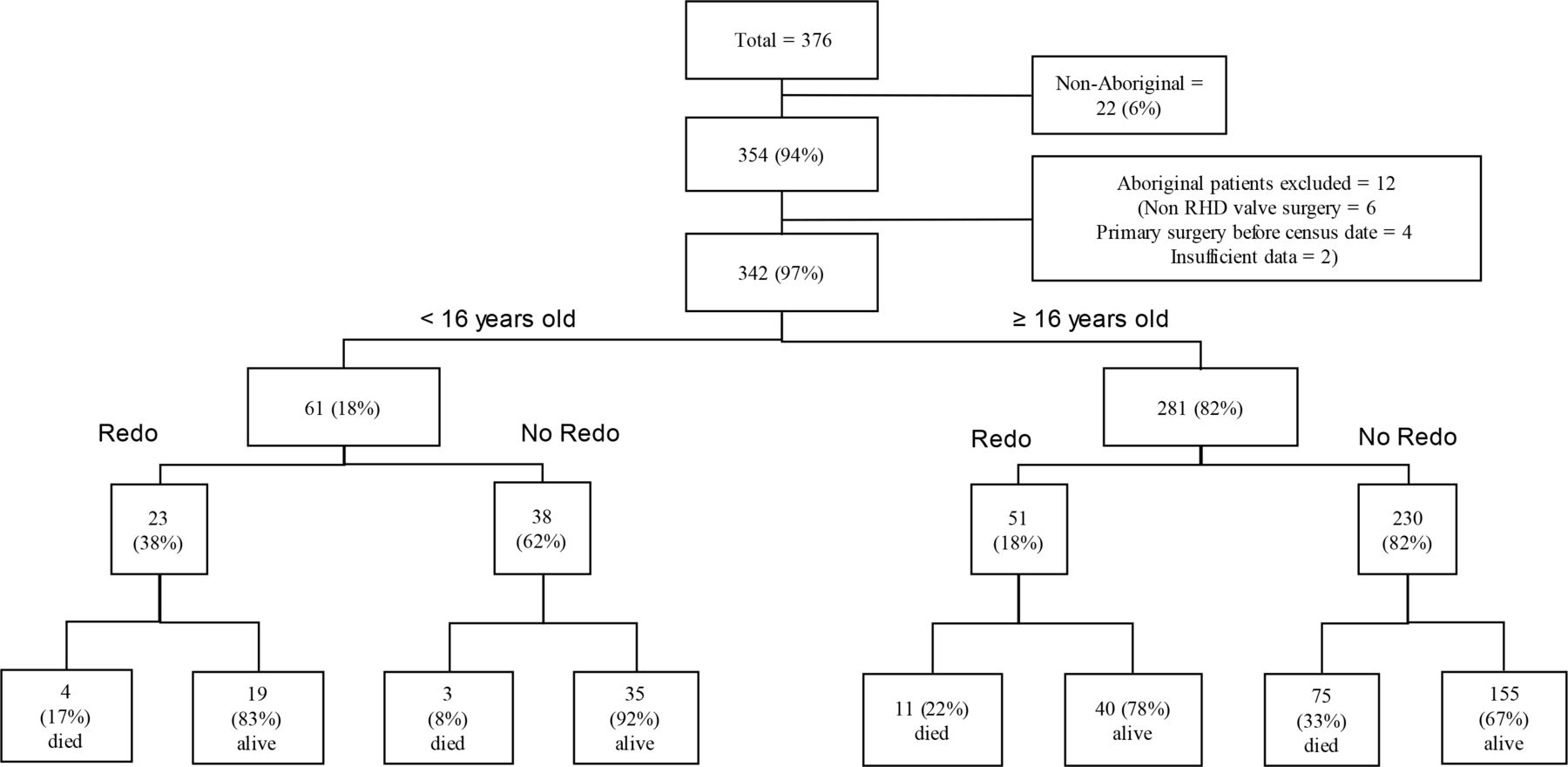
Consort diagram of rheumatic heart disease surgical patients from the Northern Territory, Australia, having their primary surgery between 1997 and 2016. The proportions requiring redo surgery and those who were alive/deceased on 31 July 2016 are presented.
Aboriginal people with RHD in the NT are commonly hospitalised for complications of RHD, and 16% require cardiac surgery within 14 years of their RHD diagnosis.3 For patients in the region with access to surgery, the 10-year survival of all patients with RHD having valve replacement surgery between 1964 and 1996 was 68%. Although 13% of the patients in this cohort were not Aboriginal, Aboriginal patients accounted for all of the cohort’s deaths.4 Since then, the regional health service has developed a model of RHD care that has provided enhanced disease monitoring and has strived to improve adherence to secondary prophylaxis.5 Referral to quaternary surgical centres and advances in operative and perioperative care have resulted in excellent results for selected patients.6
Chronic health conditions are common in the NT population. In response, there has been substantial investment in chronic disease management.7 However, while Australia has a universal health insurance scheme, access is often limited in rural and remote settings, due to health worker shortages in these locations and this is one of the reasons that the burden of many chronic diseases in Aboriginal NT residents is increasing. The prevalence of diabetes mellitus is rising annually by 2.5% and is now among the highest in the world, while the incidence of end-stage kidney disease increased by 67% between 1996 and 2014.8 9 There has also been a 24% increase in Aboriginal NT residents’ hospitalisation for respiratory diseases without an improvement in associated mortality.10 This growing burden of chronic disease is the main contributor to the 15.4 years difference in life expectancy between Aboriginal and non-Aboriginal NT residents.11
Many Aboriginal people continue to experience profound disadvantage, but Government programmes to remedy this have had limited success. In the 2022 Commonwealth Government’s ‘Closing the Gap’ report, Australia was on track to achieve its targets in only 4/17 key socioeconomic and health measures.12 13 The connection among this disadvantage, chronic disease and poor health outcomes is well established. The social determinants of health—the conditions in which people are born, grow, work, live and age—account for about half of the gap between Aboriginal and non-Aboriginal life expectancy.11 RHD and many other chronic health conditions are borne of disadvantage, and many people living with RHD have multiple comorbidities. However, there are limited data about the impact of these conditions on the health outcomes of people with RHD.
This study was conducted to determine whether recent advances in medical and surgical care have produced a corresponding improvement in the survival of NT patients requiring RHD surgery. The study also aimed to examine the burden of chronic health conditions in people requiring RHD surgery and the impact of these comorbidities on long-term outcomes.
Methods
This retrospective study included Aboriginal residents of the Top End of the NT who had their first valve procedure for RHD between 1 January 1997 and 31 July 2016. Patients with inaccessible medical records were excluded (figures 1 and 2).
Patients were identified using the NT RHD register, a database maintained by the NT RHD Control Programme. The register gathers data about individuals diagnosed with acute rheumatic fever (ARF) and RHD in the NT Top End and has been collecting these data since 1997.
Additional data were collected from medical records including demographics, cardiac investigations, comorbidities and the patients’ clinical course. Children were defined as those<16 years at the time of first surgery. Patients who were resident in the Darwin and Palmerston region were defined as having an urban address; those living elsewhere were defined as having a rural or remote address. Individuals accessing the NT health system are routinely asked whether they identify as an Aboriginal Australian.
Researchers reviewed available echocardiography studies that had been reported in accordance with the American Society of Echocardiography guidelines.14 15 Left ventricular (LV) ejection fraction (LVEF) was defined as normal if it was 52%–72% in males, 54%–74% in females or reported as normal during cardiac catheterisation. Mild LV dysfunction was defined as an LVEF of 41%–51% in males and 41%–53% in females, moderate dysfunction as an LVEF 30%–40% and severe dysfunction as an LVEF<30%.15 Recorded complications of RHD included severe pulmonary hypertension (defined as preoperative pulmonary artery systolic pressure≥50 mm Hg measured at cardiac catheterisation or estimated by echocardiography), moderate or severe LV dysfunction, significant dyspnoea (New York Heart Assessment class 3 or 4)16 and atrial fibrillation/flutter.
Individual comorbidities were identified, recorded and categorised into major subgroups to facilitate comparison. Australian guidelines were used to define diabetes mellitus and other cardiovascular risk factors that included smoking, dyslipidaemia and hypertension.17 Coronary artery disease was defined as a history of myocardial infarction or a coronary angiogram, which showed significant disease (>50% stenosis).18 A history of a transient ischaemic attack, ischaemic or haemorrhagic stroke defined cerebrovascular disease.19 Chronic lung disease was defined as the presence of chronic obstructive pulmonary disease, bronchiectasis or obstructive sleep apnoea.17 An estimated glomerular filtration rate<60 mL/min/1.73 m2 defined chronic kidney disease. If a comorbidity was not documented in the medical record, it was presumed to be absent.
The study’s primary endpoint was all-cause mortality. Where possible, the date and cause of death was determined from medical records. Deaths were defined as perioperative if they occurred within 30 days of surgery or prior to hospital discharge. All deaths due to cardiac causes and cerebrovascular accidents were attributed to RHD unless another diagnosis was stated on the death certificate as the primary cause of death. All sudden, unexplained deaths (where patients were found dead in the community) were said to have an unknown cause of death.
Statistics
Data were entered into an electronic database (Microsoft Access V.16.0, Microsoft, Redmond, Washington, USA) and analysed using statistical software (STATA V.15 STATA Corp LP, Texas, USA). Trends over time were determined using an extension of the Wilcoxon rank-sum test. Baseline characteristics of the patients at the time of their surgery were determined and are presented as an absolute number (%) for categorical variables, and as a median (IQR) for continuous variables, as many had a non-parametric distribution. Groups were compared using Fisher’s exact test and the χ2 test, where appropriate. If data were missing, the patients were excluded from analyses of those variables. Unadjusted survival was estimated using Kaplan-Meier curves, with differences between strata tested using the log-rank test. A multivariable Cox proportional hazards model adjusted for age at first surgery (<16 years and ≥16 years) and sex (binary and defined by health workers) was developed to identify independent risk factors associated with death, using a backwards stepwise approach. This was performed initially for the entire cohort and subsequently excluding those who died in the perioperative period. Variables with a p value<0.1 in univariate analysis were selected for the multivariable model and only those with a p value of <0.05 were retained. Incidence rate ratios were used to compare cohorts.
Patient and public involvement
Neither the patients nor the public were involved in the conceptualisation, design, conduct, reporting or dissemination of this study as it was a retrospective audit.
Results
Of the 376 individuals identified, 342 satisfied inclusion criteria and were included in the analysis (figure 2). Of the 34 excluded, 22 were not Aboriginal, 6 had valvular surgery unrelated to RHD and 4 had their initial surgery prior to 1 January 1997. Only two were excluded due to incomplete data. There were 281 (82%) adults and 61 (18%) children; 217 (63%) were female. The median (IQR) age at the time of RHD diagnosis in the 342 patients was 23 (13–35) years. The median (IQR) age at first surgery in children was 11 (9–14) years, in adults it was 35 (26–44) years. The median (IQR) duration of follow-up in the cohort after first surgery was 8 (4–12) years.
The patients’ first surgery involved a single valve on 282 (82%) occasions and multiple valves on 60 (18%) occasions. These 342 surgeries involved procedures on a total of 406 valves; this was the mitral valve in 294/406 (72%), the aortic valve in 96/406 (24%) and the tricuspid valve in 16/406 (4%). The number of surgeries increased annually over the study period (p for trend=0.02). The number of annual multivalve procedures also increased during the study (p for trend=0.02) (online supplemental figure 1).
Supplemental material
Of the 294 mitral valve procedures, 115 (39%) were repairs, 67 (23%) were mechanical valve replacements, 56 (19%) were bioprosthetic valve replacements and 56 (19%) were percutaneous balloon commissurotomies (PCBV). Of the 96 aortic valve procedures, 42 (44%) were bioprosthetic valve replacements, 38 (39%) were mechanical valve replacements and 16 (17%) were repairs. Overall, 173/342 (51%) had mitral and/or aortic valve replacement surgery as their first procedure.
Complications of RHD at the time of first surgery
Complications of RHD were present in 165/281 (59%) adults; 84/281 (30%) had more than 2 complications (table 1). Severe pulmonary hypertension was the most common, followed by atrial fibrillation/flutter, in 99/281 (35%) and 86/281 (31%), respectively.
Characteristics of the patients at the time of their first surgery
Characteristics of the patients at the time of their first surgery
A total of 204/281 adults (73%) had at least one comorbidity at the time of their first surgery, with smoking (164/281 (58%)) and hypertension (82/281 (29%)) the most common (online supplemental table 1). A high proportion (112/281 (40%)) had multiple comorbidities (table 2), particularly adults with chronic kidney disease who had a median (IQR) of 5 (4–6) comorbidities (online supplemental table 2).
Supplemental material
Supplemental material
The proportion of adults with RHD complications and comorbidities at the time of first surgery
Development of comorbidity after the first surgery in the patients having reoperation
Reoperation was required in 74/342 (22%) during the study period (figure 2). Of 55/74 (74%) with a recorded comorbidity at the latest surgery, 42/55 (76%) had developed a new comorbidity during the median (IQR) of 8 (6–10) years since their first surgery; indeed, these 42 patients had developed a median (IQR) of 2 (1–3) new comorbidities.
Cause of death
There were 86 (31%) deaths in the 281 adults. Death occurred at a median (IQR) of 6 (3–9) years after the first surgery at a median (IQR) age of 47 (38–54) years. A cause of death could be determined in 73/86 (85%), with RHD the primary cause in 40/73 (55%). RHD-related deaths occurred at a median (IQR) age of 49 (36–53) years, 7 (3–10) years after first surgery. Of the 40 RHD-related deaths, 8 (20%) occurred in the perioperative period, 5/281 (1.8%) at the first surgery and 3/51 (5.9%) at the second.
Of the 33/73 (45%) non-RHD-related deaths, 12 were due to pneumonia, 7 to malignancy (4 lung cancer, 1 head and neck carcinoma, 1 synovial sarcoma, 1 cancer of unknown primary), 4 to kidney failure, 4 to ischaemic heart disease, 2 to abdominal sepsis, 1 to skin sepsis, 1 to suicide, 1 to trauma and 1 to primary pulmonary hypertension. Non-RHD adult deaths occurred at a median (IQR) age of 47 (40–56) years, 5 (2–8) years after the first surgery.
There were 7 (11%) deaths in the 61 children. Deaths occurred at a median (IQR) of 8 (6–9) years after the first surgery at a median (IQR) age of 20 (IQR 20–21) years. Of the 7 deaths, 6/7 were RHD-related; there were no deaths in the perioperative period of the first surgery, 2/23 (8.7%) children died in the perioperative period of the second surgery. The one non-RHD death was due to pneumonia.
Of the 10 perioperative deaths in adults and children, 7/10 had pulmonary pressure recorded, and 5/7 had severe pulmonary hypertension preoperatively.
Survival
The overall 1-year, 5-year and 10-year survival in the cohort was 96%, 89% and 70%, respectively. For adults, the 1-year, 5-year and 10-year survival was 96%, 88% and 67%, respectively. For children, the 1-year, 5-year and 10-year survival was 100%, 98% and 85%, respectively.
The overall 1-year, 5-year and 10-year survival among individuals having valve replacement surgery in the cohort was 95%, 85% and 62%, respectively. For adults, it was 94%, 86% and 62%. Only 4/61 (7%) children had valve replacement surgery, 2/4 died at 5 and 9 years, respectively, after their first surgery (figure 3).
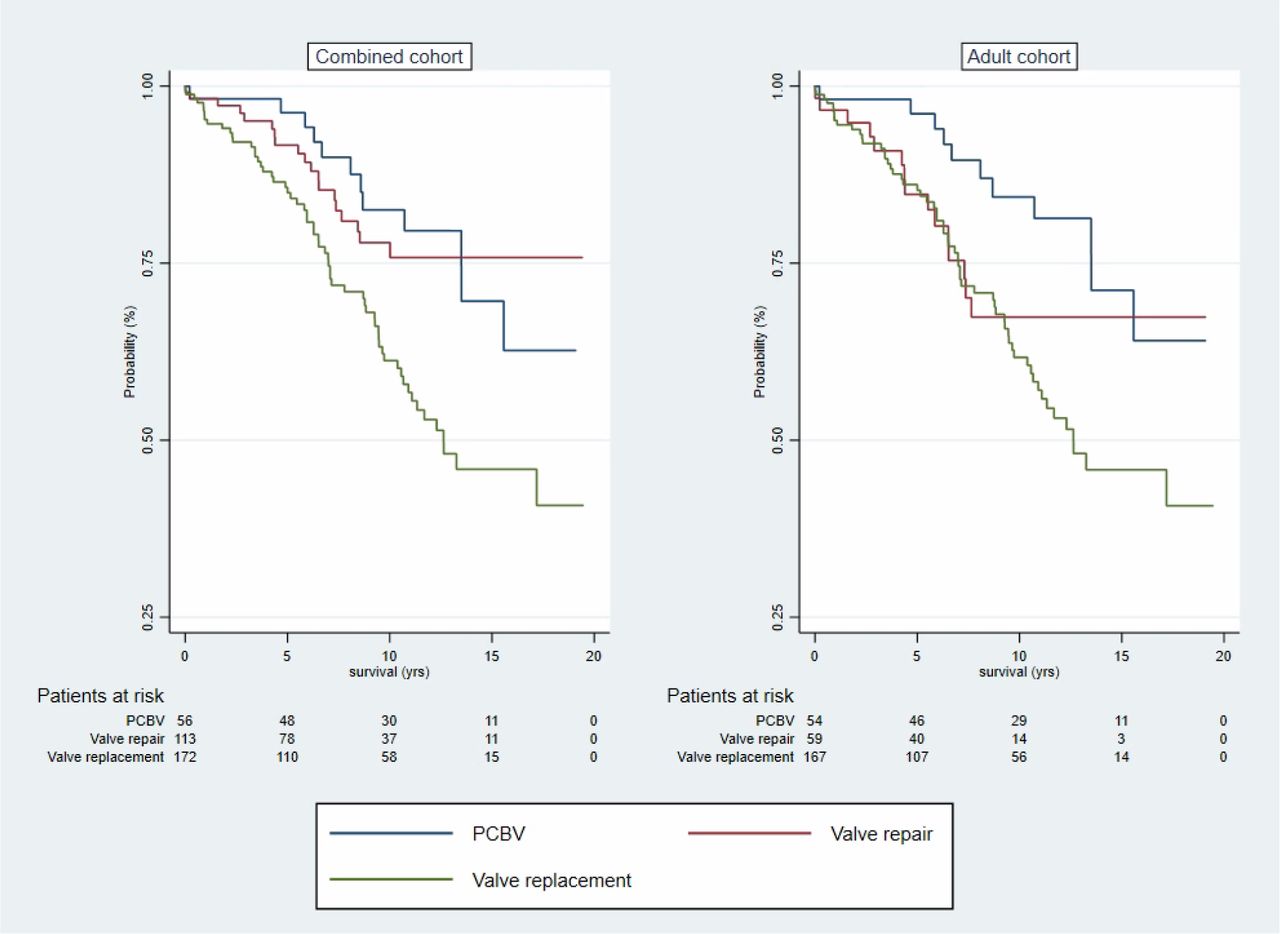
Survival curve comparing patients having any mechanical or bioprosthetic valve replacement and those having valve repair or percutaneous balloon valvuloplasty. One intraoperative death was excluded. Percutaneous balloon valvuloplasty included 56/342 (16%) procedures; 53 PCMC, 3 PCMC+PCTV. Valve repair included 113/342 (33%) procedures; 95 MVRep, 2 AVRep, 12 MVRep+AVRep, 3 MVRep+TVRep, 1 MVRep+AVRep+TVRep. Valve replacement included 173/342 (51%) procedures; 45 bMVR, 41 mMVR, 31 bAVR, 15 mAVR, 23 mMVR+mAVR, 5 bMVR+bAVR, 3MVRep+bAVR, 1 bMVR+AVRep, 3 bMVR+TVRep, 3 mMVR+TVRep, 1 MVRep+bAVR+TVRep, 1 bMVR+bAVR+TVRep, 1 bMVR+bAVR+bTVR. AVRep; aortic valve repair, bAVR; bioprosthetic aortic valve replacement, bMVR; bioprosthetic mitral valve replacement, mAVR; mechanical aortic valve replacement, mMVR; mechanical mitral valve replacement, MVRep; mitral valve repair, PCBV; percutaneous balloon valvuloplasty, PCMC; percutaneous balloon mitral commissurotomy, PCTV; percutaneous balloon tricuspid commissurotomy, TVRep; tricuspid valve repair.
The overall 1-year, 5-year and 10-year survival among individuals having valve repair surgery in the cohort was 98%, 92% and 77%, respectively. For adults, it was 96%, 85% and 65% (figure 3). For children having valve repair surgery, the 1-year, 5-year and 10-year survival was 100%, 100% and 91%, respectively. The overall 1-year, 5-year and 10-year survival among adults having PCBV in the cohort was 98%, 96 and 84%, respectively (figure 3). Only 2/71 children had a PCBV, 1 died 8.6 years after their first procedure.
There was no difference in overall survival between females and males HR 1.1 (95% CI: 0.7 to 1.6) p=0.8. Nor was there any difference in survival between females and males after valve replacement HR 1.5 (95% CI: 0.9 to 2.5) p=0.1 or valve repair HR 0.6 (95% CI: 0.2 to 1.5) p=0.3 Similarly, there was no difference between females and males in the proportion requiring redo surgery (48/217 (22%%) vs 26/125 (21%%), p=0.9) (online supplemental figure 2A–D).
Supplemental material
Contribution of comorbidity to all-cause mortality
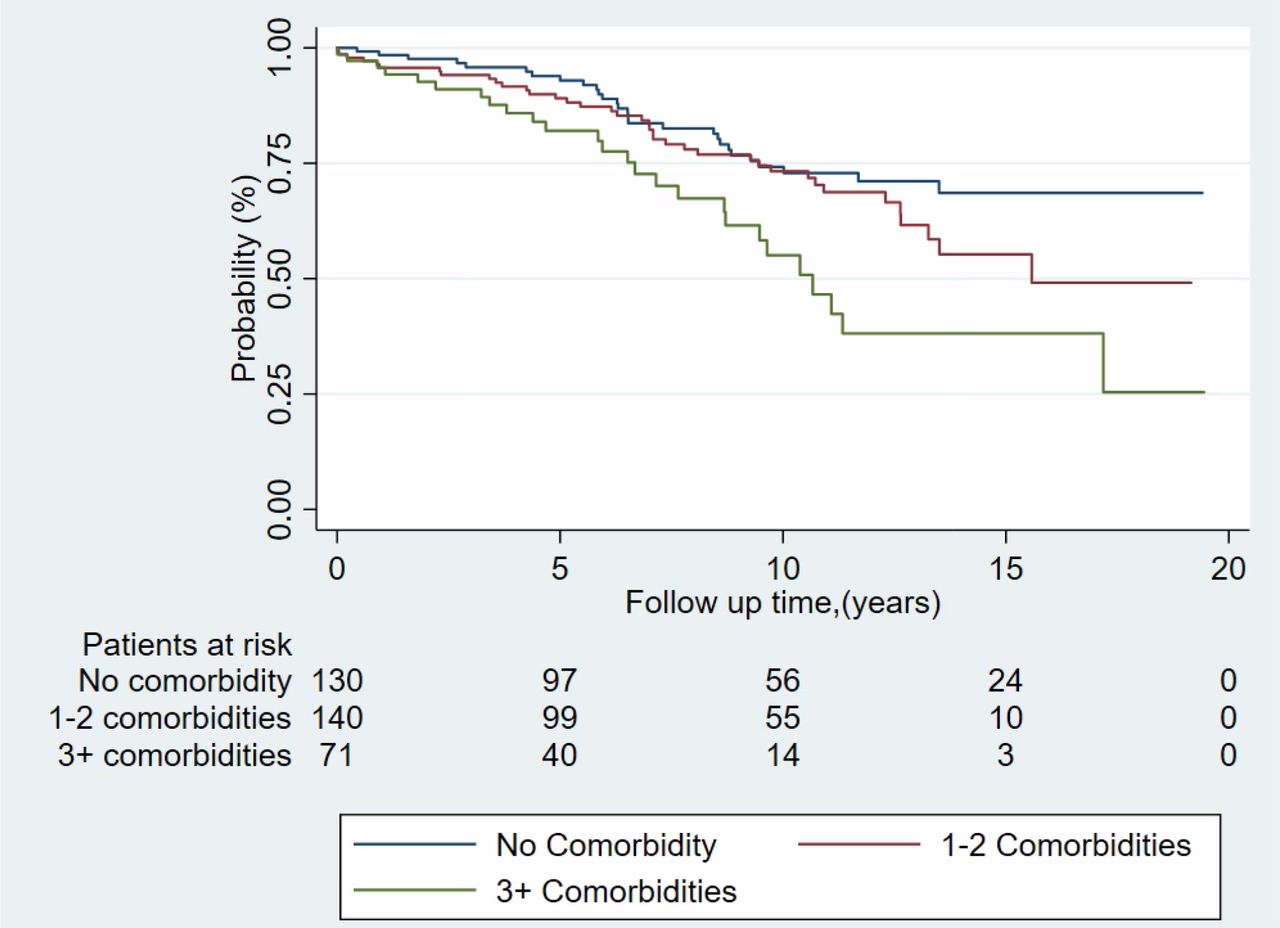
Individuals with comorbidity were more likely to die than those without comorbidity (HR 1.7 (95% CI: 1.1 to 2.6) p=0.02). The risk of death increased with each additional comorbidity, HR 1.3 (95% CI: 1.2 to 1.5) p<0.001. The 1-year, 5-year and 10-year survival for patients with no comorbidities was 98%, 94% and 74%, respectively, it was 95%, 88% and 73%, respectively, for patients with 1–2 comorbidities, and 96%, 82% and 56%, respectively, for patients with ≥3 comorbidities (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Impact of the increasing burden of comorbidity on survival after initial surgery. One intraoperative death was excluded.
Factors independently associated with death
In a multivariable analysis that controlled for age at first surgery and sex, the presence of chronic kidney disease (HR 6.5 (95% CI: 3.0 to 14.0) p=<0.001), coronary artery disease (HR 3.3 (95% CI: 1.3 to 8.4) p=0.012) and severe pulmonary hypertension (HR 1.9 (95% CI: 1.2 to 3.1) p=0.007) were independently associated with subsequent death (table 3). For patients surviving the perioperative period, chronic kidney disease (HR 6.4 (95% CI: 2.9 to 14.3) p=<0.001) and severe pulmonary hypertension (HR 1.9 (95% CI: 1.1 to 3.1) p=0.01) were independently associated with subsequent death; the association between death and coronary artery disease failed to reach statistical significance (HR 2.7 (95% CI: 1.0 to 7.6) p=0.06) (online supplemental table 3).
Supplemental material
Crude and adjusted hazard ratios for mortality in 342 Aboriginal RHD surgical patients
Comparison with historical cohorts
The 10-year survival of the 173 patients who had valve replacement between 1997 and 2016 was compared with that of the 81 patients from the region who had valve replacements between 1964 and 1996 (70/80 (87%) of whom were Aboriginal) (table 4). The 10-year survival of patients in the current series was no different to the previous series (62% (95% CI: 53 to 70) vs 68% (95% CI: 54 to 79), incidence rate ratio 0.9 (95% CI: 0.6 to 1.5) p=0.6).
Study comparison of RHD surgical outcomes across the Top End of the NT between 1964–1996 and 1997–2016
Discussion
Advances in surgical technique, perioperative care and the management of medical comorbidities have not translated into significant improvement in the long-term outcomes of Aboriginal people requiring RHD surgery in this region of Australia. The 10-year survival of the entire cohort requiring valve replacement surgery was only 62%, no better than a figure of 68% between 1964 and 1996. The overall 10-year survival of adults in the cohort was 67% with deaths occurring at a median age of only 47. However, importantly, almost half of the deaths were due to comorbid illness, rather than RHD. Although the median age of adults at the time of initial surgery was only 35, significant comorbidity was already present in almost three-quarters, while 40% had multiple comorbidities. It was also notable that the majority of patients who required reoperation had developed new comorbidities between surgeries.
RHD is the archetypal disease of disadvantage. However, this disadvantage also makes a significant contribution to the burden of comorbidity that many Aboriginal Australians continue to experience, particularly those living in remote communities.20 The ten most disadvantaged local government areas in Australia are all remote Aboriginal communities, with two of the three most disadvantaged communities in the Top End of the NT, the location of this study.21 Current Australian guidelines acknowledge the impact of the social determinants of health on the incidence and course of RHD,5 however, the actual RHD programmes that are delivered to the community have a strong biomedical focus, emphasising disease monitoring and secondary prophylaxis.22 These programmes have had a limited impact on the incidence of ARF and prevalence of RHD across Northern and Central Australia in the last two decades.23 24 There is also limited integration of this RHD care into the prevention and longitudinal management of the comorbidities that—this cohort shows—are common in this population.
Other Australian studies to examine outcomes after RHD surgery have identified similar patterns. A national study comparing outcomes of valve surgery for RHD of 174 Aboriginal and 1210 non-Aboriginal Australians between 2001 and 2012 reported that Aboriginal patients died at a much younger age than non-Aboriginal patients (at a median of 37 vs 65 years), with individuals with diabetes and chronic kidney disease at higher risk of death.25 Meanwhile, between 1992 and 2004, the 10-year valve-related mortality of 30 Aboriginal individuals from Northern Queensland having RHD surgery was 48% despite a median age at surgery of only 38.26
Australia has a universal healthcare system and offers free and open access to surgery for all Australians. In the 21st century, the Australians requiring RHD surgery are almost always Aboriginal people. However, these cohort studies suggest that until there is a fundamental shift in the way the health system cares for Aboriginal people living with—and at risk of—RHD, progress is likely to be limited. Australia ranks fifth on the global Human Development Index; however, this cohort’s long-term survival is worse than the post-RHD surgery survival of the 99th country on this index.27
There is a recognition in the RHD Australia’s ‘RHD Endgame Strategy’ that evolution of the current Australian model of RHD care is necessary, although the crucial elements of a model that improves long-term outcomes remain uncertain.28–30 The RHD Endgame Strategy proposes that Aboriginal leadership of community-based, locally relevant and culturally appropriate programmes is overdue. The strategy argues that these programmes should be holistic and understand Aboriginal concepts of comprehensive healthcare, emphasising that Aboriginal health workers and primary care providers are best placed to deliver this care.30–32 Certainly, community-based approaches that recognise the value of Aboriginal Health workers are effective in the management of chronic diseases, including RHD, in remote NT communities.33 34 The burden of RHD is borne disproportionately by women and it will be essential that the new model of care recognises this. Lessons might be learnt from successful programmes that have had a focus on the health and well-being of Aboriginal women: the ‘Healthy Mums, Healthy Bubs’ programme, for instance, is on target to increase the proportion of Aboriginal babies with a healthy birth weight to 91% by 2031.35 36
However, although Australia has a universal health system, it can be challenging for NT residents—particularly Aboriginal Australians living in rural and remote communities—to access this care. NT residents receive 30% less per-capita health funding than the national average with many Aboriginal residents receiving even less.37 Acknowledging that current programmes are failing to achieve optimal outcomes, the Australian Government has committed US$18 million to the National Aboriginal Community Controlled Health Organisation to support the development and implementation of a new model for RHD care. It is hoped that this funding will assist in identifying the key elements of a programme that delivers improved long-term outcomes for people living with RHD.
It should also be noted that almost 20% of the RHD-related deaths in this cohort occurred in the perioperative period, with perioperative deaths more common in patients with a pulmonary artery systolic pressure≥50 mm Hg. Pulmonary artery systolic pressure≥50 mm Hg was also one of only three factors independently associated with long-term outcome. There were similar findings in a North Queensland study, where all the patients who had valve related deaths and had pulmonary artery systolic pressure recorded had a value>45 mm Hg.26 These studies suggest that earlier surgery, before pulmonary artery systolic pressure becomes dangerously elevated, may reduce RHD-related death. However, this hypothesis would need to be examined prospectively.
Our study has many limitations. Its retrospective design precluded comprehensive data collection. Several important chronic health conditions including mental health disorders, substance use and liver disease were not recorded but are likely to have an impact on long-term outcomes.20 More importantly, information regarding the social determinants of health—which we hypothesise to explain our findings—was also not captured. Other potential health service and system level factors that might have affected outcomes were not recorded including individuals’ access to primary care, to Aboriginal Health workers and to health information in Aboriginal languages; the cultural competence of primary and tertiary care services was also not assessed. Aboriginal people are presented in the cohort as a single homogeneous population but there is a remarkable diversity of individuals and cultural groups across the region and their circumstances differ substantially. Although the study period spanned over two decades, the relatively small sample size could have produced type 2 errors, which may explain the absence of an independent association between diabetes mellitus, heart failure, chronic lung disease and death. Different surgeons performed the procedures at several hospitals over almost two decades; our analysis does not account for differences in surgical approaches and perioperative care. It is also important to consider that the evolution of surgical and perioperative care may have resulted in surgery being offered to patients between 1997 and 2016 who would have been considered too high risk for surgery in the earlier period.
While acknowledging these caveats, it is sobering to see that the overall 10-year survival in this 1997–2016 cohort is no better than those having surgery between 1964 and 1996. It is essential to design a model of care—in partnership with Aboriginal communities—that recognises that RHD does not occur in isolation, and integrates its care into the longitudinal, comprehensive management of other comorbidities.
Conclusion
The 10-year survival of Aboriginal patients having RHD surgery in this region of Australia has not improved despite significant advances in cardiothoracic surgery and perioperative care and improvements in the management of comorbidities. The heavy burden of comorbidities makes a substantial contribution to the premature mortality and this needs to be recognised and incorporated into models of RHD care. However, major improvements in the long-term health outcomes in Aboriginal patients having RHD surgery are only likely to occur when the social determinants of health—that drive the incidence of both RHD and these comorbidities—are also addressed.
Data availability statement
Data are not publicly available. Data may be obtained from a third party upon reasonable request. Data cannot be shared publicly because of the Northern Territory Health Services Act 2014. A dataset is available from the Northern Territory Human Research Ethics Committee (contact via email ethics@menzies.edu.au) for researchers who meet the criteria for access to confidential data.
Ethics statements
Patient consent for publication
Ethics approval
The Human Research Ethics Committees of the Northern Territory Department of Health and Menzies School of Health Research (HREC reference number: 2016-25) and the Australian Institute of Health and Welfare (AIHW reference number: EO2018/5/410) provided ethical approval for the study. The committees waived the requirement for informed consent as the data were retrospective, deidentified at the time of analysis and presented in an aggregated manner.
Acknowledgments
The authors would like to acknowledge the support and expert advice of Peter Horne, Spatial Data Manager, Health Surveillance, Tropical Public Health Services, Cairns and Hinterland Hospital and Health Service during the preparation of the manuscript. The authors would also like to acknowledge the support from the Northern Territory, RHD register, assisting with data related to this surgical cohort. We thank Rheumatic heart disease Australia and James Cook University clinical school for assistance with office space. This project was undertaken in part through Northern Territory general practice education and training as part of the rural generalist fellowship of the Royal Australian College of General Practice. James Doran is supported by the 2017 RACGP Foundation Indigenous Health Award.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Stephanie M Topp
Twitter @Menzies Research @MenziesResearch, @robertsthomson, @RosemaryWyber
Contributors JD, DC, KD, AC, NK, BRemenyi, CR, AR, NG, MS, RF, PR, EH JonathanD and JH conceptualised the study. JD, KD, NK, BRemenyi, ZW and JH contributed to data curation. JD, DC, KD, AC, ZW, CR, AR, JonathanD and JH were responsible for the methods. JD, KD, NK, BRemenyi, GB, JB, RAB, RR-T and AW contributed to data collection. JD, KD and GB verified the raw data. JD, KD, ZW, AW and JH did the formal analysis and validation. DC, KD, AC, NK, BRemenyi, MM, CH, ZW, CR, AR, JM, NG, RF, MI and JH provided supervision. JD, KD, ZW, MM, UD and JH contributed to visualisation. JD, DC, KD, AC, NK, BRemenyi, MM, ZW, CR, AR, UD, JB, MS, SS, BReeves, RJ, MI, RR-T, RW, JonathanD, JK and JH wrote and prepared the original draft. All authors had final responsibility for the decision to submit for publication.
JD accepts full responsibility for the finished work and conduct of the study, had access to the data, and controlled the decision to publish.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Map disclaimer The inclusion of any map (including the depiction of any boundaries therein), or of any geographic or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.