Article Text

Abstract
Objective In a pandemic, government assistance is essential to support the most vulnerable households as they face health and economic challenges. However, government assistance is effective only when it reaches vulnerable households in time. In this paper, we estimated the timeliness of government assistance for the most vulnerable households (ie, the poor households) in Ethiopia during its COVID-19 response of 2020. In particular, we conducted a time-to-event analysis to compare the time to receive government assistance between poor and non-poor households in Ethiopia.
Methods We used a semiparametric Cox proportional model to evaluate whether the time to first receipt of government assistance during the COVID-19 response in 2020 differed between poor and non-poor Ethiopian households. We used the Schoenfeld test to check the proportionality assumption and conducted the stratified Cox regression analysis to adjust for non-proportional variables. The data from World Bank’s High-Frequency Phone Surveys on COVID-19 and the 2019 Ethiopian Socioeconomic Survey were used for this analysis.
Results We found that the poor households in rural areas were 88% (HR: 1.88; 95% CI: 1.19 to 2.98) more likely to receive government assistance than non-poor households at any point within 10 months after the start of the pandemic. However, there was no significant difference between urban poor and non-poor households’ likelihood of receiving government assistance during this timeframe.
Conclusion The Ethiopian government has leveraged its existing social protection network to quickly reach poor households in rural areas during the COVID-19 response of 2020. The country will need to continue strengthening and scaling the existing social protection systems to accurately target the wider vulnerable population in urban areas.
- COVID-19
- Health policy
Data availability statement
Data may be obtained from a third party and are not publicly available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
In a pandemic, government assistance is crucial to enable low-income families to cope with health and economic challenges. Ethiopian government prioritised vulnerable population groups such as the poor, informal sector workers and female-headed households as key populations to receive social protection in the early COVID-19 response of 2020. However, little is known about how successful the government was in reaching its target population. The data collected from the surveys such as the Building Resilience in Ethiopia programme and the World Bank High-Frequency Phone Surveys provide an insight into the coverage of government assistance during the COVID-19 response of 2020.
WHAT THIS STUDY ADDS
Along with assessing whether the government social assistance went to those who needed it the most in the COVID-19 pandemic, it is essential to investigate how quickly the vulnerable groups received the assistance. Government assistance is effective only when it reaches the most affected in time. We used the World Bank’s High-Frequency Phone Surveys on COVID-19 to estimate the timeliness of government assistance for the most vulnerable households (ie, the poor households) in Ethiopia during its COVID-19 response of 2020. We found that the poor households in rural areas were more likely to receive government assistance than non-poor households at any point in time during Ethiopia’s COVID-19 response of 2020. However, there was no significant difference between urban poor and non-poor households’ likelihood of receiving government assistance.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The Ethiopian government has leveraged its existing safety net programmes to quickly reach poor households in rural areas during the COVID-19 response of 2020. However, the Ethiopian government will have to continue its efforts to scale up the current distribution of social assistance to reach a wider vulnerable population in urban areas if the COVID-19 cases surge again.
Introduction
In crises situations such as the COVID-19 pandemic, government assistance is crucial to enable low-income families to cope with health and economic challenges. This assistance cushions poor households from income and food shocks by replacing lost income, providing food security and slowing the downward economic pull of the pandemic. Within 3 months of the start of the COVID-19 pandemic (by May 2020), around 190 countries introduced social protection measures; about 60% of these were social assistance, while cash transfers represented 30%.1 However, there were disparities in access to these social protection measures across countries and regions. For example, cash transfers covered around 22% of the total population in North America but reached only 2% of the population in Africa.1 Access to social protection measures is important because the COVID-19 pandemic has given rise to what the World Bank calls the ‘new poor’, defined as those who were expected to be non-poor prior to the COVID-19 outbreak but were pushed into poverty in 2020 by the pandemic.2 Globally, around 97 million people were pushed into poverty by COVID-19 in 2020. The new poor are more likely to come from households in low-income and middle-income countries (LMICs) with incomes near the poverty threshold before the COVID-19 pandemic, as the adverse economic effects of the pandemic are concentrated in this group.3
Previous studies indicate that poor households have a higher incidence of chronic comorbidities, increasing their risk of COVID-19 infection and catastrophic health expenditure.4 In addition, these households are more likely to adopt extreme coping strategies, such as selling assets or reducing food expenditure, which could have adverse long-term consequences. Furthermore, poor households tend to reduce spending on their children’s education during a crisis. Therefore, their children are more likely to discontinue schooling, permanently reducing their potential future earnings.5
Ethiopia, the second-most populous country in Africa, confirmed its first case of COVID-19 on 13 March 2020. By January 2021, 10 months later, the cumulative number of confirmed cases had reached 137 650, and about 2093 people had died from COVID-19. Within 7 months of the start of the pandemic in Ethiopia, 8% of Ethiopian households reported that at least one household member had experienced a job loss, and 75% of households reported a reduction or total loss of income due to COVID-19.6 7 A third of these households reduced food expenditure or sold their assets to cope with the income loss. This COVID-related income loss was more prevalent among poor households than non-poor households.8
COVID-19 social assistance in Ethiopia
The Ethiopian government’s response to pandemic-related food and income shocks came primarily from its existing social protection network, the Productive Safety Net Programme (PSNP).8 Since 2005, the PSNP programme has provided food and cash assistance to the poorest rural households in exchange for labour. In addition, the Urban Productive Safety Net Programme (UPSNP) programme was launched in 2017 to cover food-insecure households in a few urban areas. After the COVID-19 outbreak, the Ethiopian government waived PSNP’s work requirement for 3 months and provided unconditional benefits to its beneficiaries.
Although the Ethiopian government’s COVID-19 response considered vulnerable groups such as the poor, informal sector workers and female-headed households as key populations to receive social protection, little is known about how successful the government was in reaching those it targeted.7 9 10 Two important questions are whether the government social assistance went to those who needed it the most to cope with the COVID-19 pandemic and how fast they received it. Furthermore, the government’s assistance is effective only if it quickly reaches the most affected families to provide much-needed support. Although a few studies have assessed which groups benefited the most from the government assistance during the initial months of COVID-19 response,11 none has evaluated how fast government assistance reached vulnerable groups. We fill this gap by estimating the timeliness of government assistance for the most vulnerable households (ie, the poor households) in Ethiopia during its COVID-19 response of 2020. In particular, we conducted a time-to-event analysis to compare the time to receive government assistance between poor and non-poor households in 2020.
Methods
Study setting
Ethiopia confirmed its first case of COVID-19 on 13 March 2020, in Addis Ababa. Since then, it has spread to all regions in Ethiopia. As of 30 November 2020, Addis Ababa city was the most affected (58 457 cases representing 53% of all cases), followed by Oromia (18 509 cases), Tigray (6662 cases) and Amhara (6383 cases).12 The Ethiopian Federal government implemented several public health measures to slow the spread of COVID-19 early in the pandemic. These included shelter-in-place orders, bans on large gatherings and overcrowded public transport, school and college closures and mandatory quarantine for infected persons. The government also disseminated information on preventive measures through media, cell phones and the Ministry of Health website.13 On 8 April 2020, the government declared a state of emergency to curb the spread of the COVID-19.14 To alleviate the economic impacts of COVID-19, the government made essential modifications to the PSNP programme. For example, the government waived the public work requirement for 3 months from the start of the pandemic and made advance payments to all the beneficiaries to cover April through June 2020.15 On 3 April 2020, the Prime Minister’s office announced a COVID-19 Multi-Sectoral Preparedness and Response Plan, with prospective costing of interventions of US$1.64 billion.16 The interventions included food provision to vulnerable people not covered under urban and rural PSNP, provision of shelter and non-food items, agriculture sector support and refugee support, among others.
Data
We analysed data from the World Bank’s High-Frequency Phone Surveys (HFPS) on COVID-19, implemented in Ethiopia from April 2020 to June 2021.7 HFPS includes a sample of 3249 households drawn from the household sample interviewed during the 2018/2019 Ethiopia Socioeconomic Survey (ESS).17 Like 2018/2019 ESS, the HFPS sample is representative at the national, rural and urban levels. The HFPS sample was tracked over 12 survey rounds between April 2020 and June 2021 through monthly phone interviews. The number of households followed up in each of the survey rounds is described in table 1. HFPS collected information on whether the households received assistance during COVID-19, including the type of assistance, the amount received and the types of institutions providing the assistance. We merged the HFPS sample with the 2019 ESS sample to construct a prepandemic sociodemographic profile of Ethiopian households. The information on each household’s structure, economic status and location (rural/urban) was obtained from the ESS 2019 data, while the experience of COVID-19 social assistance was obtained from the HFPS data.
Summary of COVID-19 high-frequency phone surveys (HFPS), Ethiopia
Study variables
The primary outcome variable was the time to first receipt government assistance, defined as the number of days until the household received assistance from the government for the first time since the start of the pandemic. For households who received government assistance multiple times between April 2020 and January 2021, we only counted days until the household received the first government assistance. Households received multiple forms of government assistance (eg, food, cash and cash for work) through the PSNP or other social support channels. We included all forms of government assistance received through PSNP or non-PSNP in constructing the primary outcome variable. HFPS did not specify the exact dates when the households received their first government assistance. Instead, households were asked to elicit a binary response (yes/no) to the question on whether they received any government assistance during the recall period (ie, the time since the last interview for the first three survey rounds and 4 weeks preceding the survey for all other rounds). If the household responded ‘yes’ to the question on receiving government assistance, we assumed the mid-date of the recall period as the date of receiving the first government assistance. We then counted the number of days from 13 March 2020 (ie, the date of the first reported COVID-19 case in Ethiopia) to the estimated date of receiving the first government assistance for each household to construct the primary outcome.
To explore potential differences in the administration of food assistance and cash assistance, we conducted a separate analysis using two secondary outcome variables: (1) receipt of the first food assistance from the government and (2) receipt of the first cash assistance from the government. Each secondary outcome variable was defined as the number of days until the household received the relevant assistance from the government for the first time during the COVID-19 response of 2020.
The primary independent variable was the household’s prepandemic economic status captured by the spatially adjusted adult-equivalent consumption expenditure variable from 2019 ESS data. We first divided the consumption expenditure into deciles. We then created a binary variable with the bottom-most four deciles indicating poor households and the top-most six deciles indicating non-poor households. Most recent data on poverty in Ethiopia suggested that 30.8% of the population live below the global poverty threshold of $1.90 per day, 68.9% live below the global threshold of $3.20 per day and 23.5% live below the national poverty threshold.18 We took an approximate average of these estimates to capture a representative group of households living in poverty.
We controlled for other variables, which identified vulnerable groups that needed government assistance the most in the pandemic. Previous studies indicated that the households in densely populated urban areas were more likely to lose their labour incomes in the early phase of the pandemic.19 Moreover, women were disproportionately affected, with women’s employment experiencing a most significant drop within 3 months after the start of the pandemic in Ethiopia.20 In addition, households with a higher number of non-earning members (elderly above 64 years and children below 15 years) were more likely to absorb income shocks by resorting to extreme coping measures such as selling assets during the pandemic.21 We, therefore, controlled for household location (rural/urban), gender of household head (male/female), schooling status of household head (attended school/did not attend school) and the ratio of the number of dependents to the total number of household members.
Statistical analysis
We conducted a time-to-event analysis using a semiparametric Cox proportional model to evaluate whether the time to first receipt of government assistance during the COVID-19 response in 2020 differed between poor and non-poor Ethiopian households.22 The analytical sample included households who received government assistance between April 2020 and January 2021 (uncensored observations) and households for which information on time to first receiving the government assistance was not available due to loss to follow-up or non-occurrence of the outcome before January 2021 (censored events).
We first plotted Kaplan-Meier failure function curves for poor and non-poor households to indicate the probability of receiving government assistance for the two groups at any point in time between March 2020 and January 2021. We then used a multivariable Cox proportional hazard (PH) regression model to test whether the hazard rates were statistically different for poor and non-poor households, controlling for other factors. We applied probability weights to the Cox PH regression to obtain nationally representative HRs. The resultant HR from the Cox PH model was interpreted as the ratio of hazard rate in the poor to non-poor households. We then repeated the statistical analysis process on secondary outcome variables to evaluate whether the time to receive the first government food or cash assistance during the COVID-19 response of 2020 differed between poor and non-poor Ethiopian households.
Model validation
Cox PH regression assumes that the hazard functions for the different strata of the variables in the model are proportional over time. We tested this proportionality assumption using the Schoenfeld test and found that it held for all but one covariate, household location (rural/urban) (see table 3).23 Therefore, in line with recommended practice, we stratified the Cox PH model by the variable that did not meet the proportionality assumption. While the stratified Cox PH model computes separate baseline hazards for each level of stratification, it assumes the same regression coefficients for remaining covariates across the strata. We tested this assumption of the stratified Cox PH model by allowing interaction between the stratified variable and other covariates. Finally, we used the Wald test to check whether adding interaction terms in the stratified Cox model improved the model’s overall fit.
Results
The analytical sample included 3247 households. These households were weighted to represent approximately 19 million Ethiopian households (table 2). In 2019, a third of these households were located in urban areas, around a fourth were female-headed and nearly half of the households had a household head with no prior schooling. On average, 40% of all household members were dependents. The average annual consumption expenditure of the poor households and non-poor households was Birr 7135 (about US$245) and Birr 24 423 (about US$840), respectively. The poor households were more likely to be in rural areas (84.5%), have a male household head (78.0%) and have a head that did not attend the school (63.5%) (online supplemental appendix table 1).
Supplemental material
Percentage of households who received some form of assistance from the government at least once between March 2020 and January 2021, by household location
Around 14.0% of households in Ethiopia received some form of government assistance at least once by January 2021, that is, within 10 months from the start of the COVID-19 pandemic (table 2). In this 10-month timeframe, government assistance had reached a higher proportion of poor households (18.8%) than non-poor households (10.6%). Similarly, the Ethiopian government reached a higher proportion of other vulnerable households by January 2021. For example, 16.0% of rural households, 23.8% of female-headed households and 16.9% of households with uneducated heads received government assistance vis-a-vis 9.9% of households in urban areas, 10.8% of with male-headed households and 11.0% of households with educated heads.
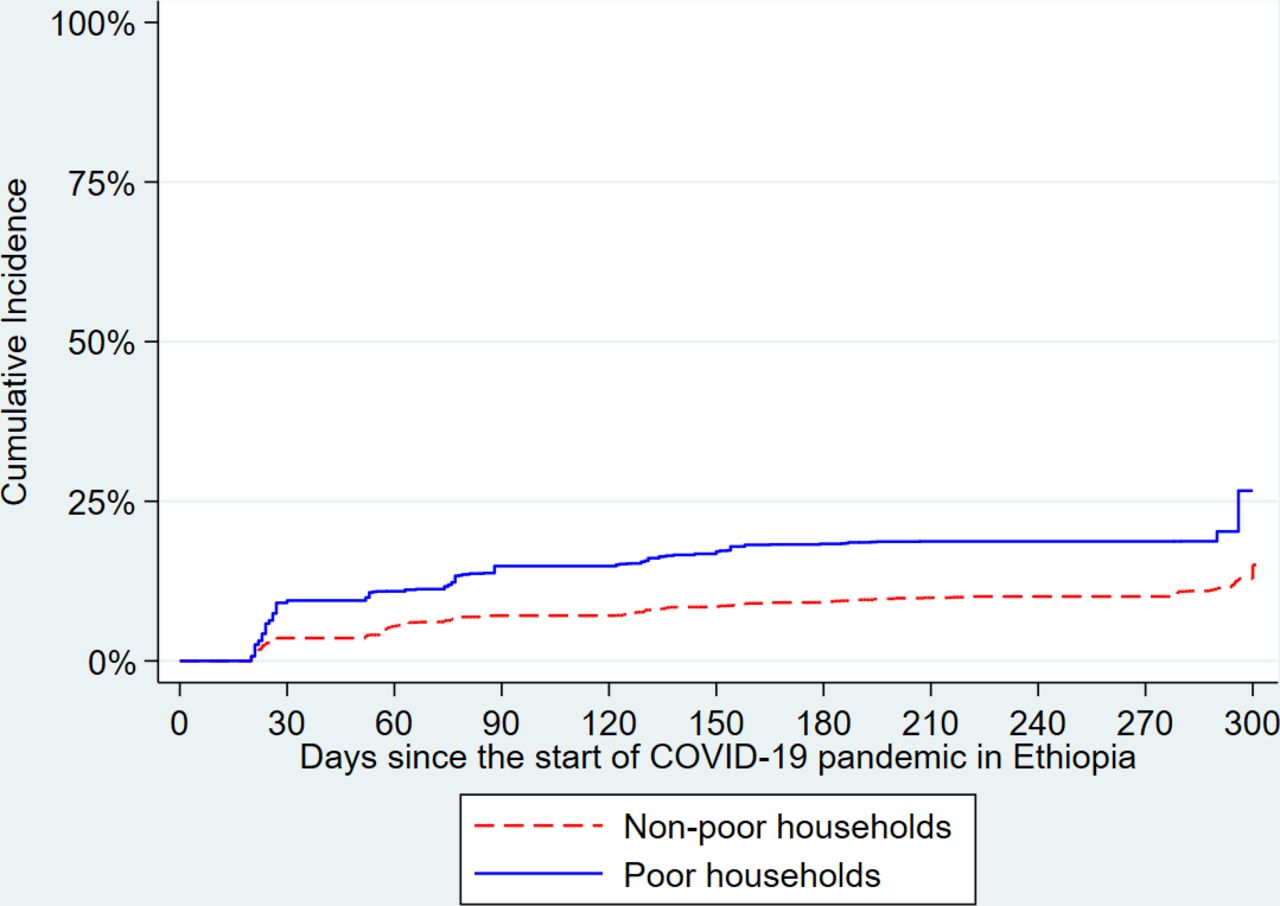
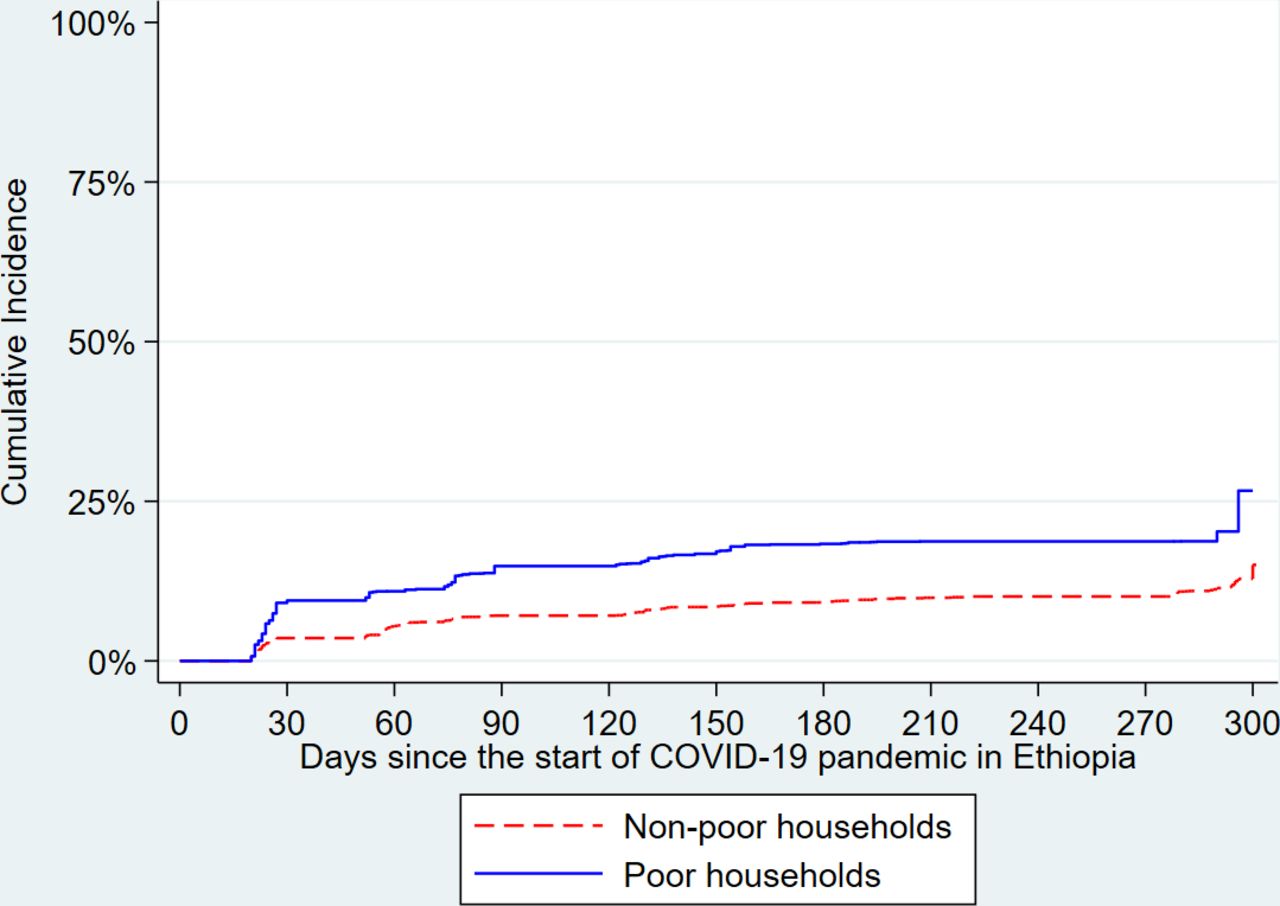
The Kaplan-Meier failure function for poor and non-poor households plotted in figure 1 indicates that the probability of the first receipt of government assistance was higher for poor households than non-poor households at all points in time between March 2020 and January 2021. Two months after the start of the pandemic (ie, day 60), the likelihood that a poor household had received the first government assistance (10.9%) was twice that of the non-poor households (5.5%). By the 10th month (day 300), the likelihood that a poor household had received government assistance for the first time (26.7%) continued to be almost twice that of the non-poor households (15.0%).
{kind=link}
Kaplan-Meier failure function for poor and non-poor households. Kaplan-Meier failure function for poor and non-poor households indicates the probability of receiving the first government assistance for the two groups at any point in time between 13 March 2020 (start date of the pandemic in Ethiopia) and January 2021.
Even after holding all other variables constant, the adjusted HR from the Cox PH regression for poor compared with non-poor households was 1.72 (HR: 1.72; 95% CI: 1.18 to 2.49) (table 3, column 1). In other words, poor households were 72% more likely to receive their first instance of government assistance than non-poor households at any point in time during the first 10 months of the pandemic; this implies that the Ethiopian government’s approach to providing the assistance was pro-poor. Similarly, the adjusted HR for female-headed households compared with male-headed households was 2.89 (HR: 2.89; 95% CI: 1.95 to 4.28). Urban households were significantly less likely to receive their first instance of government assistance than rural households (HR: 0.58; CI: 0.41 to 0.83) at any point in time during the first 10 months of the pandemic.
Cox proportional hazards regression model, scaled Schoenfeld test and stratified Cox proportional regression model for the outcome variable ‘time to first receipt government assistance’
We tested the proportionality assumption of the Cox PH model using the Schoenfeld statistical test (table 3, column 2). We found that all variables except the household location (rural/urban) variable met the proportionality assumption. Therefore, we ran a stratified Cox regression model where we stratified the model by the household location (rural/urban) categories (table 3, column 3). The stratified model indicated that the expected adjusted hazard was 1.71 times (HR: 1.71; 95% CI: 1.18 to 2.47) higher in poor than non-poor households. Moreover, the female-headed households were significantly more likely to receive their first government assistance than male-headed households at any point in time between March 2020 and January 2021.
We allowed the HRs to vary across rural and urban locations by including an interaction between household location and other variables in the regression (table 3, column 4). We found a significant effect of poverty and gender of household head in rural areas, while schooling status and gender of household head were significant in urban areas (table 4). Among rural households, the poor households were significantly more likely to receive their first government assistance than non-poor households (HR: 1.88; 95% CI: 1.19 to 2.98) at any time during the first 10 months after the start of the pandemic. However, the expected hazard was not significantly different for poor and non-poor households in urban areas (HR: 1.04; 95% CI: 0.62 to 1.76). The HR for households with educated versus uneducated heads differed among rural and urban households. In rural areas, there was no significant difference in the likelihood of receiving first government assistance between households with educated and uneducated heads (HR: 0.88; 95% CI: 0.55 to 1.40). However, households with uneducated heads were 99% more likely (HR: 1.99 ; 95% CI: 1.30 to 3.04) to receive government assistance than educated heads in urban areas. On the other hand, female-headed households had a significantly higher likelihood of receiving government assistance than male-headed households at any time during the survey period in both rural (HR: 3.00; 95% CI: 1.84 to 4.90) and urban areas (HR: 2.43; 95% CI: 1.61 to 3.69).
Cox proportional hazards regression model fitted to rural and urban households for the outcome variable ‘time to first receipt government assistance’
We ran the Wald test to check whether adding interaction terms in the model creates a statistically significant improvement in the model’s fit. Based on the Wald test, we were able to reject the null hypothesis that the coefficients of interaction terms are simultaneously equal to zero, indicating that the stratified model with interaction terms improves the fit of the model.
In the subgroup analysis, we found that the time to receive food assistance for the first time from the government did not differ significantly between poor and non-poor households at any point in time between March 2020 and January 2021 (online supplemental appendix table 2, column 3). However, poor households were more likely to receive their first government cash assistance than non-poor households at any point in time during the COVID-19 response of 2020 (online supplemental appendix table 3, column 3).
Discussion
Little is known about how effective governments are in reaching the people they aim to protect during emergencies such as the COVID-19 pandemic. Our study helps to fill one aspect of this knowledge gap by investigating whether government support reached those most likely to need it and how quickly they received it. We found that the Ethiopian government’s delivery of social assistance was pro-poor during the 2020 COVID-19 response. In particular, poor households in rural areas had a higher likelihood of receiving government assistance than non-poor households during this timeframe. However, within urban areas, there was no significant difference between poor and non-poor households’ likelihood of receiving government assistance. Moreover, government assistance was more likely to reach female-headed households than male-headed households in both rural and urban areas at any point in time during the first 10 months of the pandemic.
One reason why government assistance reached a higher proportion of poorer households in rural areas may be the strong presence of PSNP networks in rural Ethiopia since 2005. Most households who received government assistance at least once reported that their first government assistance came through a PSNP programme. A study evaluating the effectiveness of the PSNP programme during the COVID-19 pandemic found that participation in PSNP offset all of the adverse effects of the COVID-19 pandemic on food insecurity.14 PSNP households were less likely to adopt extreme coping measures such as reducing expenditures on education, health and agricultural inputs. The protective effect of PSNP was higher for poorer households and those living in remote, rural areas.
Although the Ethiopian government mainly considered targeting the urban poor in its 2020 COVID-19 response, we did not find a significant difference between urban poor and non-poor households’ likelihood of receiving government assistance at any point in time.9 This might be because the UPSNP pilot is relatively new. It was launched only in 2017 in 11 cities.24 The Ethiopian government’s ability to achieve a pro-poor approach in rural areas and not as much in urban areas highlights the importance of having a robust social protection infrastructure to enable quick distribution of benefits to the most vulnerable groups in crises. In September 2020, Ethiopia received a grant to launch the Urban Productive Safety Nets and Jobs Project (UPSNJP) to extend economic support to the urban poor in 83 cities and promote the inclusion of disadvantaged urban youth in labour market.
Despite the pro-poor findings, the Ethiopian government still has room for improvement. The government assistance only reached a small proportion of poor households during the initial COVID-19 response of 2020. Around 57% of the poor households who received some form of government assistance reported receiving assistance only once, as of October 2020.25 HFPS also collected information on the value of assistance received. The respondents were asked to report cash equivalent for food and in-kind assistance along with the value of cash assistance. In the first HFPS round, poor households reported receiving US$23.5 on average from the government (range: US$0.9 to US$81.6, median: US$17.2). In HFPS round 5 (ie, September 2021), the average government assistance reported by the poor households was US$37.1 (range: US$0.9 to US$257.7, median: US$25.8). Given that most households received assistance only once between March and October 2020, the median assistance reported received by most households was below the monthly minimum wage of US$34.7 in Ethiopia.26 The coverage and value of government assistance need to be increased with a special focus on those most affected by poverty. Moreover, the government can improve its targeting in the urban areas to achieve the kinds of results in the rural area. The UPSNJP launched by the Ethiopian government is a step in the right direction.
The main strength of our study lies in conducting a time-to-event analysis. In time-to-event analysis, we are able to assess whether the event had occurred and also assess when the event occurred. In a public health emergency like the COVID-19, it is crucial to investigate whether the most vulnerable groups received the assistance. However, it is equally important to ask how quickly they receive assistance because in the absence of timely assistance, households are pushed to adopt extreme coping strategies that are likely to have long-lasting negative consequences. Our findings are similar to a previous study by Josephson and colleagues that used HFPS data and a linear probability model to estimate the likelihood of different vulnerable groups to receive assistance during the COVID-19 pandemic.11 Josephson and colleagues found that female-headed households were more likely to receive social assistance than male-headed households in four African countries, including Ethiopia. However, the linear regression methods used in their study are not suited to evaluate the time-to-event aspects of social assistance.
There are limitations to our study. First, the HFPS sample represents only those households with access to phones.27 While 90% of households in urban Ethiopia have access to phones, only 40% of rural households own a phone. There is a systematic difference between the households who own phones and those who do not own phones in terms of total consumption expenditure. Therefore, it is likely that impoverished households who do not have access to phones are not captured in the HFPS. Nevertheless, we still found a pro-poor effect in rural households among those with phones which is a positive outcome by itself. Second, the length of the recall period for the question on government assistance receipt differed among survey rounds. For example, in rounds 2 and 3, the households were asked if they had received any government assistance since the previous interview call. From round 4 onwards, the households were asked if they had received government assistance in the 4 weeks preceding the survey date. The changes in the recall period and framing of the question over the survey rounds might lead to the inconsistent recording of the government assistance receipt. The information on the receipt of government assistance is not available for round 8. Therefore, the instances of government assistance receipt may be underestimated in our analysis. Third, we used a relative measure of poverty in our analysis to identify poor households, which is different from geographical and community-based targeting used by Ethiopian social assistance programmes to reach poor and food-insecure households. In our analysis, all households with an annual consumption expenditure in the bottom-most four deciles of the HFPS sample were considered poor. This different approach to measuring poverty might explain why we found that 10% of non-poor households received government assistance during the COVID-19 response of 2020.
While targeting those in need and providing timely assistance during the pandemic is crucial, it is also important to investigate whether the assistance received was adequate. One-time assistance or scant assistance per capita might not be enough for poor households to cope with the downward economic pull of the pandemic. Therefore, future research should investigate whether those in need received adequate COVID-19 assistance from the Ethiopian government. Moreover, researchers can use the HFPS data collected for other countries to evaluate their response to the pandemic and identify strategies that worked or could be strengthened to reach a broader swath of the vulnerable population.
In summary, our study highlights how Ethiopia was able to leverage its existing social protection system during a public health emergency to help reach its most vulnerable population groups. However, countries need to be mindful of pre-existing structural gaps in the existing social protection system. The COVID-19 pandemic provides an opportunity to fix some of the pre-existing bottlenecks in the social protection system. Therefore, investing in strengthening and scaling the existing social protection systems will help countries reduce impoverishments, reduce catastrophic spending and build resilience to future crises.
Conclusion
In a public health emergency, government assistance is crucial to cushion vulnerable households from health, food and income shocks. However, government assistance is effective only when it reaches the most vulnerable people on time. We show that the government social assistance in Ethiopia was more likely to reach the poor than non-poor in rural areas at any point in time in the 10 months timeframe from the start of the pandemic. However, the Ethiopian government will have to continue its efforts to scale up the current distribution of social assistance to reach a larger proportion of the vulnerable population in urban areas if the COVID-19 cases surge again.
Supplemental material
Data availability statement
Data may be obtained from a third party and are not publicly available.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by Duke University's institutional review board (2021-0349) on 26 February 2021.
Acknowledgments
We want to thank Dr Gavin Yamey (MD, MPH, MA), the Director of the Centre for Policy Impact in Global Health, Duke Global Health Institute, for providing helpful comments on the draft paper.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Lei Si
Twitter @KassahunAddis
Contributors OO led the overall design of the study with inputs from all authors. ASD collected the data and performed the analysis with support from OO. ASD drafted the initial manuscript. All authors contributed to the revision of the manuscript and approved the final version. ASD act as the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests OO, WM, MMD and ASD report grants from Bill & Melinda Gates Foundation outside the submitted work.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Author note The reflexivity statement for this paper is linked as an online supplemental material 1.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.