Article Text

Abstract
Objective The 2016 Global Strategy on Human Resources for Health: Workforce 2030 projected a global shortage of 18 million health workers by 2030. This article provides an assessment of the health workforce stock in 2020 and presents a revised estimate of the projected shortage by 2030.
Methods Latest data reported through WHO’s National Health Workforce Accounts (NHWA) were extracted to assess health workforce stock for 2020. Using a stock and flow model, projections were computed for the year 2030. The global health workforce shortage estimation was revised.
Results In 2020, the global workforce stock was 29.1 million nurses, 12.7 million medical doctors, 3.7 million pharmacists, 2.5 million dentists, 2.2 million midwives and 14.9 million additional occupations, tallying to 65.1 million health workers. It was not equitably distributed with a 6.5-fold difference in density between high-income and low-income countries. The projected health workforce size by 2030 is 84 million health workers. This represents an average growth of 29% from 2020 to 2030 which is faster than the population growth rate (9.7%). This reassessment presents a revised global health workforce shortage of 15 million health workers in 2020 decreasing to 10 million health workers by 2030 (a 33% decrease globally). WHO African and Eastern Mediterranean regions’ shortages are projected to decrease by only 7% and 15%, respectively.
Conclusions The latest NHWA data show progress in the increasing size of the health workforce globally as more jobs are and will continue to be created in the health economy. It however masks considerable inequities, particularly in WHO African and Eastern Mediterranean regions, and alarmingly among the 47 countries on the WHO Support and Safeguards List. Progress should be acknowledged with caution considering the immeasurable impact of COVID-19 pandemic on health workers globally.
- health systems evaluation
- medical demography
- public health
- descriptive study
Data availability statement
Data are available on reasonable request.
Data availability statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request. The NHWA data portal (available here: https://apps.who.int/nhwaportal/) enable access to all health workforce data reported by Member States to WHO and which were used in the present article.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
The Global Strategy on Human Resources for Health: Workforce 2030 highlighted a projected health workforce (HWF) shortage of 18 million health workers by 2030.
Following 5 years of the National Health Workforce Accounts (NHWA) global implementation, data availability has significantly improved which allows for a reassessment of the HWF shortage by 2030.
WHAT THIS STUDY ADDS
The latest NHWA data for the year 2020 show a total stock of 65 million health workers globally, which represents an increase of 14 million net jobs as compared with 2013, and furthermore a potential increase of 19 million net jobs by 2030.
Consequently, the revised estimates of the global HWF shortages indicate a reduction (of the 18 million figure) to 15 million in 2020 and a projected number of 10 million by 2030 based on current trajectories into the future (mostly depicting a pre-COVID-19 situation).
Significant regional disparities remain, and inequities have increased, as the projected 2030 shortage will cluster in the 47 countries included in the WHO support and safeguard list. Those countries alone will bear two-third of the global shortage.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
Given the latest available data, the COVID-19 pandemic has no observable effect on these trends; economic uncertainties however are likely to impose constraints on the employment of newly graduated health workers in some countries and could derail and reverse the progress to date.
The results of this reassessment is a high alert for the need for sustainable investments in the healthcare workforce, particularly in regions and countries highlighted in this analysis.
Introduction
Health workers play a central role in health systems. This is evidenced globally by the COVID-19 pandemic, during which the most common cause of disruptions to essential health services reported was the lack of staffing.1 Health workers are also recognised as central to attaining, sustaining and accelerating progress towards Universal Health Coverage (UHC).2
With the growing global recognition of the role of health workforce, the United Nations Sustainable Development Goals (SDGs) defined a specific target in SDG3.c ‘to increase recruitment of health workforce, especially in least developed countries and small island developing states (SIDS)’. The Global Strategy on Human Resources for Health: Workforce 2030 (GSHRH) sets out the global policy agenda to ensure a health workforce that is fit for purpose to attain the targets of UHC and the SDGs.3 The GSHRH provided estimates of the size of the global health workforce in 2013 and projections to 2030. It estimated a global shortage of 18 million health workers by 2030. This projection was based on data availed by the WHO Global Health Observatory at the time, with some degree of uncertainty related to both the variability in quality and completeness of the underlying data and to the assumptions made. It required the addition of tracer indicators to estimate the median health workforce densities to be used as thresholds for estimating the global shortage.
The decision by the World Health Assembly in 2016 to adopt the progressive implementation of the National Health Workforce Accounts (NHWA)4 and annual reporting to WHO has led to significant improvements in data quality and availability. Partnered activities such as the State of the World’s Nursing 20205 and the State of the World’s Midwifery 20216 have also generated empirical data. In addition, improved data on the number of dentists, pharmacists and other health occupations facilitated their inclusion in the global estimates.
The present article therefore provides an assessment of the health workforce stock for the year 2020 based on latest data reported by Member States and a projection to 2030. The analysis also provides an overview of the trends in the global health workforce shortages between 2013 and 2020, and projections to 2030. An improved data-driven understanding of the global health workforce is quintessentially important for planning, policy and investment decisions. And more critically when those are linked to COVID-19 recovery priorities in job creation and social protection as well as informing global equity priorities, such as the WHO Health Workforce Support and Safeguards list (HWF-SSL) 2020.7
Methods
Health workforce data on the stock, age groupings and the number of graduates were extracted for each country and every year between 2000 and 2020 from the NHWA4 platform on the 4 January 2022. The NHWA online platform is a global repository of countries’ reported health workforce data, and is the central monitoring mechanism of global health workforce indicators and targets articulated in the GSHRH, the UN SDG3.c8 and the subindicators of the WHO 13th Global Programme of Work.9 Aligned with the NHWA definitions and the Organisation for Economic Co-operation and Development (OECD)/EUROSTAT/WHO-EURO joint data collection, the stock in the data extracted and later referred in this paper was defined as ‘the number of practicing health workers’ and was therefore limited to the number of health workers delivering care to the population. When no information on practising health workers was available, the stock of ‘professionally active health workers’ was used instead and when the latter was also not available, the stock of ‘licensed to practice health workers’ was used. Country data were summarised and presented by WHO regions, and the World Bank income group,10 with an extra identification of SIDS.11 Results were also reported for the group of 47 countries in the WHO HWF-SSL7 prioritised in monitoring the implementation of the WHO Global Code of Practice on the International Recruitment of Health Personnel. Occupations were classified according to ILO’s International Standard Classification of Occupation.12
To compute the density of health workers per 10 000 population for each country, year and occupation, the population size data were extracted from the World Population Prospects (2019 release) of the United Nations’ Population Division.13 The baseline density for each occupation was computed for the year 2020. When no data were available for the year 2020, the latest available stock data before 2020 was used instead (see online supplemental appendix 5 for the latest year available by country and the NHWA data portal: https://apps.who.int/nhwaportal/ for further details by year). To compare health workers densities with those used in the time of the GSHRH development, data for the latest year until 2013 were also extracted. These data for year 2013 were mostly retrospectively completed by Member States since the launch of the GSHRH and therefore form a stable baseline to compare with. For the few countries with missing stock data (2 countries for dentists, 22 for midwives, 7 for pharmacists), the average density of countries in the same income group was used.
Supplemental material
For each occupation group, the projection of health workers to year 2030 relied on a simple stock and flow model over 10 years which factors in production and attrition of health workers as follows:
Health workforce stock2030≈(health workforce stock2020 ×(1−% age65+))×(1–0.1×% age55–64)(10−1)+10×0.7×number of graduates annually
The use of the percentage of health workers older than 65+ years was applied in the first projection year (2021) and later the share of those aged 55–64 years in the following years (2022–2030) were used to factor in attrition from 2021 to 2030. This modelling approach was initially applied in the State of the World’s Nursing 2020.5 Because the age of retirement is commonly 65 years in many countries,14 the share of those aged 65+ years was considered as an attrition on an annual basis. One-tenth of those aged 55–64 years were considered as moving to the category 65+ years. Health systems’ absorption capacity of new graduates from health professional education was also factored in the modelling by adding-in a fixed 70% of the annual graduates. This estimated percentage was approximated from OECD Stat15 data by activity level, which shows an average ratio between practising and licensed to practice health workers of around 70% for physicians (74%), nurses (70%), dentists (70%) and pharmacists (66%). The fixed 70% absorption capacity considered across all country income groups comes with assumption that in each country the education market would self-regulate relative to the availability of positions in the health labour market of each country. It could be argued however that the absorption capacity could vary and be somewhat lower in low-income countries. As a sensitivity analysis, a varying absorption capacity of 70%, 60%, 50% and 40% were used for high-income, upper middle-income, lower middle-income and low-income countries, respectively.
The revised shortage of health workers was measured relative to thresholds, which are estimated by the median density of health workers for five occupational groups (medical doctors, nursing personnel, midwifery personnel, dentists and pharmacists) in 2013. The median density of each occupation was used to bring our method as close as possible to that applied in the GSHRH estimation for which the shortage threshold was equivalent to the world’s median density of three of the five occupational groups (medical doctors, nursing personnel, midwifery personnel). For each occupation, the difference between its median (threshold) density and the observed density was converted into a stock count (by multiplying the difference between the two densities by the population size in the specific country) and computed for 2013, 2020 and the projection to 2030. Next, the stock count was summed up across the five occupations and then increased by a region-specific proportion to account for other occupations similar to the approach used in the GSHRH estimation. The proportion of other occupations was determined using data from 82 countries that reported stock data for at least 15 occupations including the 5 occupations mentioned above (online supplemental appendix 2).
Data extraction was conducted from the NHWA data platform (2021 update) and data analysis was conducted with Stata.16
Results
Workforce in 2020
For the five occupation groups, recent stock data were reported by the great majority of countries (online supplemental appendix 1). Aggregating data for the 194 Member States of WHO, the five occupation groups (dentists, medical doctors, midwifery personnel, nursing personnel and pharmacists) represent a total of 50.1 million health workers in 2020 (table 1). Adding the share of other occupations (online supplemental appendix 2) gives an estimated total of 65 million health workers out of which nursing personnel represent one-third (29.1 million). Compared with 2013, this stock has increased by 29% globally, 3 times greater than the population increase over the same period (8.2% growth).
Stock of SDG3.c health workers (medical doctors, nurses, midwives, dentists, pharmacists) in 2020 by WHO region (in millions)
Accounting for the population size and the density of health workers per 10 000 population in 2020 reveals a striking inequity, with high-income countries having a health workers density that is 6.5 times that of low-income countries (figure 1).

Density of health workers per 10 000 population in 2020 by income group. *Includes dentists, medical doctors, midwifery personnel, nursing personnel and pharmacists.
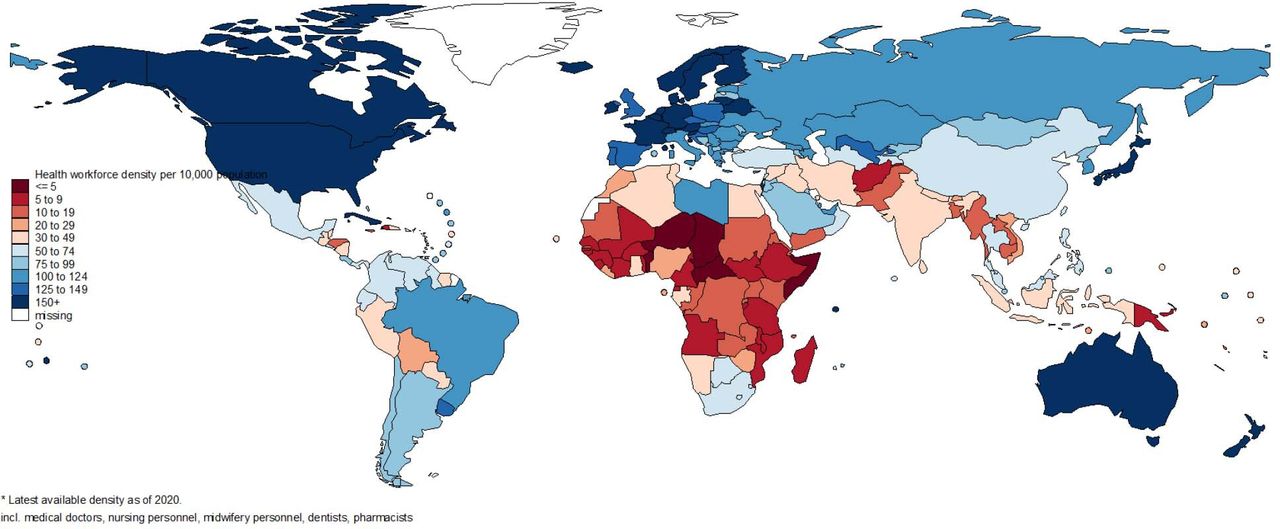
This finding underscores the fact that slightly more than one-fifth (22%) of the world’s population have close to half (47%) of the global health workforce. This inequity has marginally decreased since 2013 when it was 7.6 times greater. Figure 2 depicts the inequitable distribution of health workers at a more granular level and the degree of subregional disparities.
{kind=link}
{kind=link}
Map of health workers (dentists, medical doctors, midwifery personnel, nursing personnel, pharmacists) density per 10 000 population in 2020. Cut-off points used for density per 10 000: 5, 10, 20, 30, 50, 75, 100, 125, 150. The middle cut-off point used is 50 health workers per 10 000 population and is close to the shortage benchmark (see “health workforce shortage section“ below), therefore countries in red colour scale on the map can be considered as having a health workforce shortage.
For the SIDS, the density of the five occupation groups only increased slightly from 57.9 to 59.3 per 10 000 between 2013 and 2020. In 2013, it was higher in SIDS (5.4%) as compared with other countries while in 2020 the density in SIDS became lower (8.4%).
Projection to 2030
The projection of stock (table 2) indicates that the global health workforce could reach 84 million health workers in 2030. This is a projected global increase of 29% which is 3 times faster than the equivalent population increase (a projected increase of 9.5% globally) in the period 2020–2030.
The projected stock of SDG3.c health workers (dentists, medical doctors, midwives, nurses, pharmacists) in 2030 by WHO region (in millions)
Results of the sensitivity analysis (which considers a varying absorption capacity of new graduates by income group) show that the projected stock of the global health workforce is 76 million health workers, which would correspond to a global increase of 17% between 2020 and 2030.
Health workforce shortage
Using the median densities of health workers in 2013 for the five occupations, a combined threshold of 51.2 health workers per 10 000 population was estimated. To compare, including only medical doctors, midwifery personnel and nursing personnel as considered in the GSHRH estimation, the combined threshold becomes 47.6 which is close to the value of 44.5 estimated in 2016.3 Hence, the analysis proceeds with the new threshold (based on the five occupations) to estimate the shortage of health workers for the years 2013, 2020 and for the projected health workforce stock in 2030 (table 3).
Estimation of the global health workforce shortage (in millions) in 2013, 2020 and projected in 2030 by occupation
Results presented in table 3 show that the global shortage estimates to 15.4 million health workers in 2020 globally and is projected to be around 10.2 million in 2030 (a decrease of about 34%). In similar sense, results from the sensitivity analysis show that the projected health workforce shortage for 2030 is 12.9 million health workers, that is, a 16% decrease of shortage since 2020.
Although the overall trend is showing a notable decrease in the shortage for most occupations, regional disparities exist (online supplemental appendix 3). The largest decrease in the shortage was observed for WHO Western Pacific region. In contrast, the changes in shortages remain unclear for WHO African region with an estimated shortage of 5.1 million, 5.7 million and 5.3 million in 2013, 2020 and 2030, respectively. Hence, factoring in the rapid increase in population size, health worker shortages in WHO African region is projected to constitute 52% of the global shortage by 2030 while representing a quarter in 2013. As for the SIDS, the difference in the projected decrease in shortage between 2020 and 2030 is less (−12%) than that estimated for other countries (−34%). The 47 countries in the WHO HWF-SSL represented half of the estimated shortage of health workers in 2020, and it is projected to only slightly decrease (9%) by 2030. Alarmingly, these 47 countries between them will encompass 69% of the global health workforce shortage by 2030.
Discussion
The GSHRH highlighted a projected health workforce shortage of 18 million health workers by 2030.3 It identified gaps in data reporting and triggered dedicated policies and efforts to monitor health workforce through the progressive implementation of the NHWA.17 Five years on, data availability and quality significantly improved allowing the present reassessment to take place. The latest NHWA data for year 2020 measures a total global stock of 65.1 million health workers (dentists, medical doctors, midwives, nurses, pharmacists and other health workers) which indicates an increase of 14 million net jobs (a 27% increase) as compared with 2013. This growth in the size of the health workforce is >3 times faster than the population growth rate over the same period. Although some data improvement could have had a role in the change in reported number, it is important to note that the figure used for 2013 is not the number that was reported in the Global Strategy on Human Resources for Health: workforce 2030, but on a revised estimate that includes the retrospective reporting, hence could be now considered as a solid reference stock.
The analysis to 2030 indicates a projected growth rate of 2.7% annually (as compared with an 0.9% growth of global population), which represents an increase in 19 million net jobs that could reach 84 million health workers in 2030. This increasing stock of employed health workers in the health economy is consistent with the predictions stated in the GSHRH3 and the UN High Level Commission on Health Employment and Economic Growth.18 Both identified strong economic demand—mostly in upper middle-income and high-income countries—that could create up to 40 million additional jobs by 2030. In spite of this consistency, the 2030 estimate of 84 million health workers should be viewed with a degree of caution as it is based on the prevailing graduation rates and cannot as yet factor in the multidimensional impact of the COVID-19 pandemic neither on healthcare workers19 20 nor on the education market.
Unequivocally, the pace of progress has significantly reduced the previously estimated global shortage to 15.4 million in 2020 and is projected to further decline to 10.2 million in 2030: lower than that estimated in the GSHRH3 or through other methods.21 Part of the this can be explained by the availability of better and more recent data allowing for a better assessment of the shortage. For instance, the GSHRH estimates predicted a 17% decrease in shortage between 2013 and 2030, while this reassessment estimates a 49% decline between 2013 and 2030, largely explained by better data on additional health occupations and their collective contributions in expanding access to UHC.
This global progress is however uneven. WHO African and the Eastern Mediterranean regions did not show improvements of their health workforce shortage between 2013 and 2020, which is projected to remain stagnant by 2030. One possible explanation is their notable population growth rate of 28% and 18%, respectively, between 2020 and 2030, compared with about 5% in other WHO regions. Our findings further suggest that at this pace, the projected 2030 shortage will be clustered in 47 countries (mostly in WHO African region), included in the WHO HWF-SSL and between them encompass two-third of the global shortage by 2030. This is an alarming situation for the African region’s heath systems that are facing an increasing demand for health services by a growing population size and the rising demand to accelerate progress towards the SDG health-related targets.22 Despite the clear focus on SIDS articulated in SDG3.c, these countries show less progress in reducing their shortages in comparison with other countries. SIDS countries are facing several challenges, such service delivery as in hard-to-reach areas and limited national education capacity, which may explain the modest reduction of the shortage. This finding underscores the urgency for dedicated actions and support to SIDS countries.
Limitations
While this paper presents an estimate for year 2020 with latest data for almost all countries, it must be noted that in the case of few countries’ data the latest year available was sometimes >3 years earlier than 2020 (online supplemental appendix 5). For most countries, the density used for year 2020 and applied to the population of 2020 came either from 2018, 2019 or 2020 (78% of countries for dentists, 76% for medical doctors, 71% for midwifes, 83% for nurses and 64% for pharmacists). For these countries, the potential change in density between 2018 and 2020 can be considered as negligible. However, for the remaining countries, when latest data dated before 2018, there is a slight possibility of underestimating the stock of 2020 given that density expected to have increased over time. Alternative approaches could be used, such as multiple imputation, to fill empirical data gaps, however those would require specific development to include both the profiling of countries with missing data and the interpolation of missing values in trends by occupation group.
The method used for projecting the global health workforce to 2030 relied on a simple stock and flow model. It has however a few limitations. First, the model assumes a fixed production capacity throughout the period. The model used is therefore conservative and may slightly underestimate or overestimate the production capacity of individual countries over time. Second, no data on health worker migration were used in the modelling. It can be expected that the attrition factor due to outmigration varies by country and might affect the shortage estimate. In particular, the COVID-19 pandemic could have disrupted international mobility and countries most dependent on international migration, such as high-income countries, may experience a slower progression of their overall stock to 2030. On the whole, the impact of attrition due to migration is difficult to estimate, however it can be speculated that the degree of potential variation on our estimation would be equivalent to the average share of foreign-trained nurses from OECD Stat of about of 6.3%.15 It can be expected that countries in African region and South-East Asia region would be affected also by having higher retention of health workers during this period, but this might not necessarily have translated into new jobs. Third, the age distribution used as an attrition factor was considered as fixed. The age at retirement was set at 65 years, which is in line with data from OECD.14 A faster attrition rate might occur because the majority of health workers are women,23 who may retire on average at a slightly younger age than men. Fourth, our reassessment assumed that 70% of new graduates would be constantly employed over the coming years. It implies that 30% of graduates would be trained as health workers but being unemployed or working in other sectors than health such as in public administration, in education, etc. As a consequence, the overall stock of health workers in each country by 2030 would be higher than the estimation of practising health workers considered in the present paper. This fixed 70% share of graduates becoming employed is an uncertain assumption in light of potential fiscal space constraints linked to the social and economic impact of the COVID-19 pandemic.24 A sensitivity analysis was also conducted and considered ‘what if’ only 50% of new graduates were absorbed in the health sector annually in all countries, the projected workforce would be around 75.9 million health workers by 2030 as compared with 84 million with a 70% absorption capacity. If all countries were to experience a major reduction of 30% absorption capacity, the projected health workforce would be 67.5 million health workers by 2030. These sensitivity analyses stipulate the necessity to sustain a high absorption capacity in the years leading to 2030. Beyond the impact of COVID-19, the absorption capacity of new graduates could also vary by income group and by occupation. A sensitivity analysis using a varying absorption capacity relative to income groups showed a projected stock of 76 million health workers and a shortage of 12.9 million by 2030. Fifth, the attraction to and retention of jobs in the health sector (postpandemic) may become a relative unknown given the negative impact of attrition due to concerns over higher risks of infections, risks to mental health and well-being, stigmatisation19 among others. Put together however, these limitations are least problematic for the short-term projection (over 10 years) presented in this analysis.
The shortage estimation also relies on a global comparison of densities of occupation groups and therefore provide a broad indication of the progress that would be required for countries with lowest density to scale-up their workforce relative to the threshold median density. It also suggests that health systems would become better equipped to ensure essential health services provision without necessarily reaching the UHC service coverage index (SCI) of at least 80.
Therefore, the shortage of health workers can be estimated using alternative methods and scenarios (online supplemental appendix 4). For instance, between 2020 and 2030, our analysis showed that 10 million health workers would retire globally, half of those are in high-income countries. Factoring in the population growth, an alternative scenario on the number of health workers required to compensate attrition due to retirements estimates that 13.7 million health workers will be needed by 2030 primarily in high-income countries.
Alternative scenarios can also consider target densities to reach a specific level of essential service coverage under the assumption of a perfectly causal relationship between UHC SCI and health workforce density. Such scenario would produce an estimated shortage as high as 78 million if all countries of the world were to reach a UHC SCI level of 80 in 2030 (online supplemental appendix 4).
Conclusions
Using the latest NHWA data, this paper illustrated progress in the total stock of the global health workforce between 2013 and 2020 and generated revised projections to 2030 that suggest a reasonable pace globally in reducing shortages. However, there are two issues of concern. First, the COVID-19 pandemic continues to entail an unprecedented global public health crisis coupled with economic uncertainties that are bound to affect all sorts of projections to 2030. For instance, the lack of economic activities and revenues may limit public expenditures on health and fall short in covering the recurrent cost of health workers’ wages required. Second, pervasive inequity in health workers distribution remain, with low-income countries and SIDS presenting very low health worker densities in 2020 that are likely to remain stagnant by 2030. This reassessment demonstrated that, while the shortage is projected to rapidly decline in many countries, it is expected to remain high in low-income countries. More drastically, most of the shortage by 2030 (69%) will be found in 47 countries included in the WHO HWF-SSL.7 This is a fundamental threat to equity and the concept of ‘universal’ health coverage. The results of this analysis provide compelling evidence to why governments and global health development partners need to accelerate investments in health worker education, to facilitate the recruitment of new health workers, and to overcome fiscal space constraints that would jeopardise the progress attained in the last decade. Towards that end, mounting evidence and mitigating measures have been explicitly addressed in the Working for Health Action Plan 2022–2030 tabled for endorsement and support by the 75th World Health Assembly.25
Data availability statement
Data are available on reasonable request.
Data availability statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request. The NHWA data portal (available here: https://apps.who.int/nhwaportal/) enable access to all health workforce data reported by Member States to WHO and which were used in the present article.
Ethics statements
Patient consent for publication
Acknowledgments
The authors wish to acknowledge Dr Giorgio Cometto and Dr Pascal Zurn (Health Workforce Department, World Health Organization) for helpful comments on the manuscript.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Seye Abimbola
Contributors MB, guarantor. MB, KD, JC conceptualised the study. MB, TK, TSN conducted data management and statistical analysis. MB drafted the first manuscript. All authors contributed to editing the manuscript. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.