Article Text

Abstract
Introduction Worldwide, the 33 recognised megacities comprise approximately 7% of the global population, yet account for 20% COVID-19 deaths. The specific inequities and other factors within megacities that affect vulnerability to COVID-19 mortality remain poorly defined. We assessed individual, community-level and healthcare factors associated with COVID-19-related mortality in a megacity of Jakarta, Indonesia, during two epidemic waves spanning 2 March 2020 to 31 August 2021.
Methods This retrospective cohort included residents of Jakarta, Indonesia, with PCR-confirmed COVID-19. We extracted demographic, clinical, outcome (recovered or died), vaccine coverage data and disease prevalence from Jakarta Health Office surveillance records, and collected subdistrict level sociodemographics data from various official sources. We used multilevel logistic regression to examine individual, community and subdistrict-level healthcare factors and their associations with COVID-19 mortality.
Results Of 705 503 cases with a definitive outcome by 31 August 2021, 694 706 (98.5%) recovered and 10 797 (1.5%) died. The median age was 36 years (IQR 24–50), 13.2% (93 459) were <18 years and 51.6% were female. The subdistrict level accounted for 1.5% of variance in mortality (p<0.0001). Mortality ranged from 0.9 to 1.8% by subdistrict. Individual-level factors associated with death were older age, male sex, comorbidities and age <5 years during the first wave (adjusted OR (aOR)) 1.56, 95% CI 1.04 to 2.35; reference: age 20–29 years). Community-level factors associated with death were poverty (aOR for the poorer quarter 1.35, 95% CI 1.17 to 1.55; reference: wealthiest quarter) and high population density (aOR for the highest density 1.34, 95% CI 1.14 to 2.58; reference: the lowest). Healthcare factor associated with death was low vaccine coverage (aOR for the lowest coverage 1.25, 95% CI 1.13 to 1.38; reference: the highest).
Conclusion In addition to individual risk factors, living in areas with high poverty and density, and low healthcare performance further increase the vulnerability of communities to COVID-19-associated death in urban low-resource settings.
- COVID-19
- epidemiology
- health systems
- public health
Data availability statement
Data are available on reasonable request. After publication, the datasets used for this study will be made available to others on reasonable requests to the corresponding author, including a detailed research proposal, study objectives and statistical analysis plan. Deidentified participant data will be provided after written approval from the corresponding author and the DKI Jakarta Health Office.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
In addition to individual risk factors such as older age and comorbidities, few studies from North America and South America have reported the association between lower community-level socioeconomic status and healthcare performance with increased risk of COVID-19-related death.
However, the specific inequities and other factors within megacities that affect vulnerability to COVID-19 mortality remain poorly defined.
WHAT THIS STUDY ADDS
This study affirmed that in addition to well-known individual risk factors, community-level poverty and density, and lower COVID-19 vaccine coverage further increase the vulnerability of communities to die from COVID-19 in urban low-resource settings.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
This study highlights the need for accelerated vaccine roll-out and additional preventive interventions to protect the urban poor who are most vulnerable to dying from COVID-19.
In the context of a heavily decentralised health system such as in Indonesia, coordination and prioritisation of available resources and public health intervention will be critical to ensure optimal health outcomes for vulnerable communities, especially for those areas with high poverty, population density and low vaccine coverage.
Background
There are currently 33 megacities, defined by the United Nations Department of Economic and Social Affairs as cities with a population of at least 10 million persons.1 Worldwide, megacities comprise 7% of the global population, yet account for approximately 20% of all COVID-19 deaths.2 Megacities often contain high levels of inequity with regard to income, housing, sanitation, transportation, population density, basic healthcare and other factors. The important role of health inequity in the spread and mortality of epidemics has been known from influenza in 1918 to Ebola in 2014.3–7 The severity of illness and clinical outcomes can be affected by the concentration of comorbidities in susceptible groups in communities,3 4 8 and through disparities of access to healthcare for preventive measures or prompt diagnosis and treatment. Ensuring health equity, especially in megacities experiencing massive urbanisation and mobility is essential for the current and future global health threats.
In the context of the ongoing pandemic, understanding community-level and healthcare risk factors associated with the mortality is very important to guide policymaking and target public health and clinical interventions, particularly in the context of fragile public health systems. At individual level, older age and pre-existing chronic comorbidities have been consistently reported as the main risk factors of COVID-19-related mortality across different settings.9–13 At the community level, recent findings in USA, Chile and Brazil suggested that COVID-19 mortality was concentrated in groups with higher sociodemographic vulnerability.14–18 At the health system level, a recent study from Brazil reported that higher COVID-19 deaths rate was associated with lower intensive care unit beds per 100 000 people.19 However, there is a general scarcity of data in lower-middle-income country (LMIC) assessing the influence of community-level sociodemographics and healthcare factors on COVID-19-related mortality.
Indonesia, the world’s fourth most populous country (population 274 million), is an LMIC featuring great geographical, cultural and socioeconomic diversity across the archipelago. For example, the 2019 Human Development Index (HDI) ranged from 0.32 in Nduga District, Papua to 0.87 in Yogyakarta city, Yogyakarta.20 Indonesia has suffered the highest number of COVID-19 confirmed cases and deaths in Southeast Asia, second only to India in all of Asia,21 at 6 023 924 cases and 155 421 deaths (2.6% case fatality rate (CFR)) up to 5 April 2022,22 of which 21% (1 240 678) of cases and 9.8% (15 205) of deaths occurred in its capital Jakarta, a megacity (7659 km2, and estimated population 10.6 million) that features stark health inequalities and sociodemographic heterogeneity. The first SARS-CoV-2 epidemic wave occurred from 2 March 2020 to 30 April 2021, and a more intense second wave dominated by Delta variant peaked in July 2021.23 24
As in many LMICs, accessing quality healthcare services is challenging to substantial proportions of the Indonesian population, due to under-resourced and fragile health systems.25 The 2018 Public Health Development Index (PHDI)26 ranges from 35% in Paniai district, Papua province to 75% in Gianyar district, Bali province. Within the province-level administration area called the Special Capital City Area Jakarta (Daerah Khusus Ibukota, DKI Jakarta), the PHDI ranged from 64% in North Jakarta to 68% in East Jakarta districts. However, the five districts of DKI Jakarta (North, East, West, South and Central) are highly heterogeneous sociodemographically and little is known regarding the capacity and performance of public health systems at subdistrict level. That heterogeneity and the large number of COVID-19 cases and deaths during the first and second wave of the epidemic in DKI Jakarta provides insights directly relevant to the national public health response to the COVID-19 crisis, as well as other LMIC settings. In this study, we assessed individual, community-level and healthcare vulnerability among the 44 subdistricts of DKI Jakarta and how those factors were associated with COVID-19-related mortality during the first 18 months of the epidemic in that province (March 2020 through August 2021).
Methods
Study design and participants
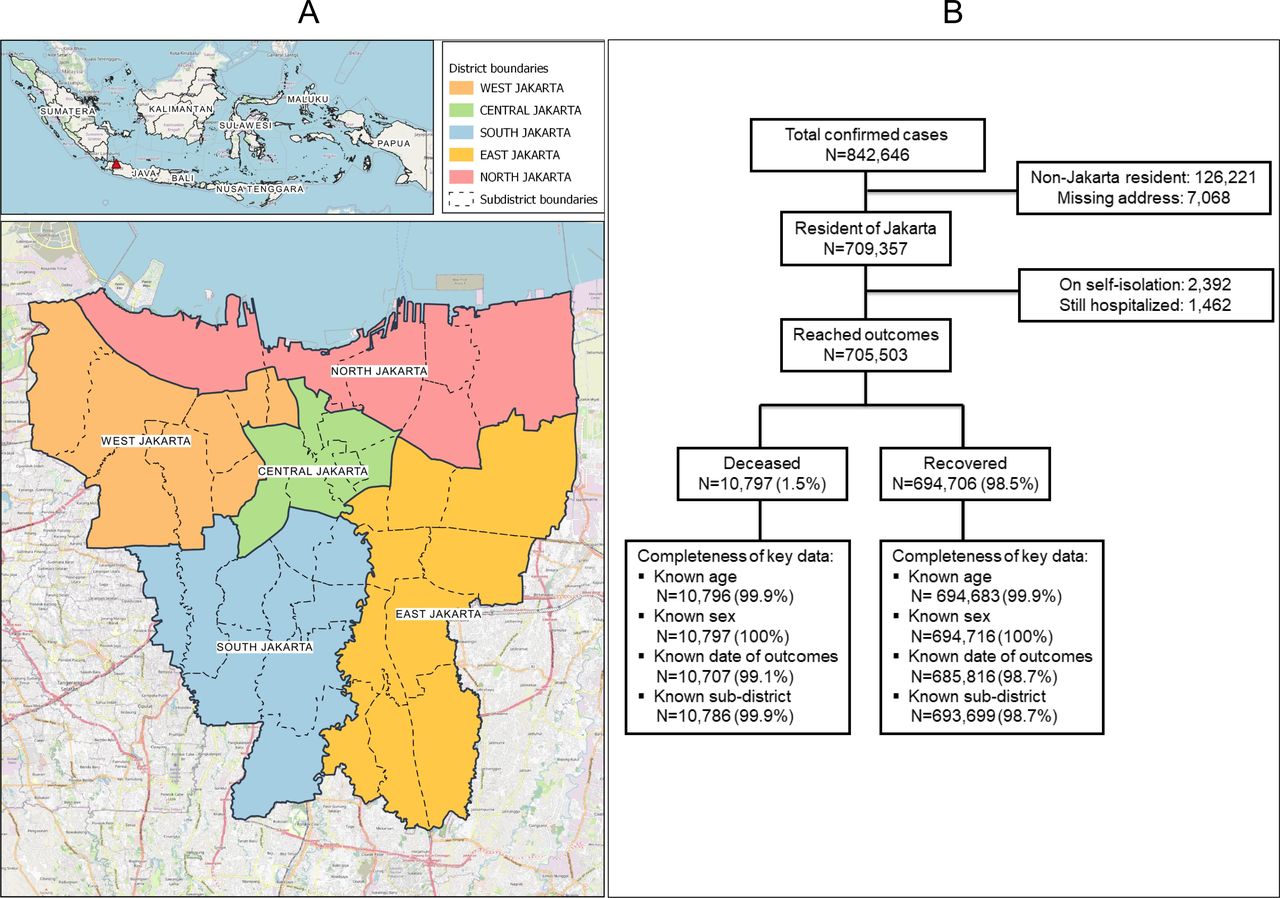
This was a retrospective cohort study of all adults and children diagnosed with PCR-confirmed SARS-CoV-2 infection (COVID-19 cases) in DKI Jakarta, Indonesia, recorded by the DKI Jakarta Health Office, who either died or recovered between 2 March 2020 and 31 August 2021. We restricted the analysis to DKI Jakarta residents to enable robust estimations of community-level risk factors and individual outcomes (deceased vs recovered) of cases living in the corresponding subdistrict (figure 1A). In accordance with Indonesia’s national COVID-19 guidelines,27 confirmatory SARS-CoV-2 PCR testing was conducted on naso-and/or oropharyngeal swab specimens in COVID-19 reference laboratories.

Study sites (A) and flow chart and completeness of key variables (B).
Patient and public involvement
This study did not include patients and public in the design, or conduct, or reporting, or dissemination plans. This study was a secondary analysis of anonymised routine surveillance data conducted as part of a formal collaboration between the Jakarta Health Office and Eijkman-Oxford Clinical Research Unit, Jakarta.
Data collection and operational definitions
Individual-level data were collected from all cases who lived in any of 44 subdistricts in DKI Jakarta. Each subdistrict public health facility had designated epidemiologists and surveillance officers responsible for epidemiological investigations using an official COVID-19 case investigation form capturing demographical and clinical data of each confirmed case. The epidemiological investigations were done by visiting each individual cases. Completed forms were submitted to the DKI Jakarta Health Office for cleaning and verification (checking for completeness, inconsistency, error and duplication) and entered into a surveillance database. We extracted individual data regarding SARS-CoV-2 PCR testing, hospital admission and outcomes (recovered or deceased), along with age, sex and pre-existing comorbidities (based on clinical assessment or cases self-report).27
Community-level risk factors data (subdistrict level) were obtained from official government websites. Data on number of populations, population density (number of residents per square kilometre (km2, number of neighbourhoods with poor sanitation were collected from the DKI Jakarta Government Integrated Data Portal).28 Data on the number of individuals categorised as poorest (the lowest tenth of the national level of poverty) were obtained from the National Team for the Acceleration of Poverty Reduction, and used to calculate proportion of poorest individuals by subdistrict.29 Population density, poverty and proportion of poor sanitation areas were used to describe sociodemographic vulnerability.
Health care-related data on number of nurses, and number of medical doctors were obtained from the DKI Jakarta Government Integrated Data Portal.28 Data on COVID-19 vaccine coverage, universal child immunisation coverage, all-cause mortality among under 5 years population, prevalence of hypertension, diabetes and tuberculosis were collected from the DKI Jakarta Health Office surveillance records. The following variables were calculated to describe the healthcare vulnerability at subdistrict-level: doctor–population ratio (number of doctors per 10 000 population in 2020), nurse–population ratio (number of nurses per 10 000 population in 2020), COVID-19 vaccine coverage (proportion of individuals received two doses of COVID-19 vaccine per 31 August 2021), universal child immunisation coverage (proportion of children received complete dosage of government mandatory vaccination), all-cause mortality among under 5 years population (proportion of all of deaths per 1000 under 5 years population), prevalence of hypertension in 2019 (proportion of cases per 100 population), prevalence of diabetes in 2019 (proportion of cases per 100 population), and prevalence of tuberculosis in 2019 (proportion of cases per 100 population).
Statistical analysis
Numeric values of each community-level risk factors were categorised into quarters, that is, below 25th percentile (quarter 1), 25–50th percentile (quarter 2), 50–75th percentile (quarter 3) and above 75th percentile (quarter 4). Descriptive statistics included proportions for categorical variables and medians and IQRs for continuous variables. We used the Mann-Whitney U test, χ² test or Fisher’s exact test to compare characteristics between deceased and recovered cases. We set statistical significance at 0.05, and all tests were two sided.
We used bivariable and multivariable multilevel logistic regression models to determine the risk of death, expressed as odds ratio (OR) with 95% confidence intervals (CIs). Subdistrict was treated as the random effect variable to adjust for clustering of observations within subdistricts. We did null model analysis (no predictor was added) and the result justified the use of the multilevel models. We excluded cases from two subdistricts with insufficient sample size (Kepulauan Seribu Selatan and Utara). All independent variables with p<0.10 in bivariable analysis were included in the multivariable models. Final model selection was informed by intraclass correlation postestimation test. We used interaction terms to examine potential effect modification by age, sex and time. In the presence of interaction, the stratum-specific OR and 95% CI were calculated, adjusting for other variables with p <0.10 in bivariable analysis. Additionally, we used a restricted cubic spline mixed effect regression to model the OR of death over time.
There was a substantial proportion of missing data for chronic comorbidities (58%). Missing-indicator analysis by risk factor stratification and by regression analysis identified bias of missing data with respect to mortality, thus, we additionally conducted analysis to assess sensitivity of risk factor identification due to missing data. We performed multilevel logistic regression analysis with multiple imputations (100 imputed datasets), treating subdistrict as random effect variable. Age, sex and outcome were included as independent variables in imputing the comorbidities variable. All statistical analyses were done in Stata/MP V.17.1 (StataCorp). This study is reported as per Strengthening the Reporting of Observational Studies in Epidemiology guidelines.21 30
Results
Between 2 March 2021 and 31 August 2021, a total of 842 646 PCR-confirmed COVID-19 cases were recorded by the DKI Jakarta Health Office (figure 1). Of those, 709 357 (84.2%) lived in DKI Jakarta and 705 503 (99.5%) had reached a definitive outcome before 1 September 2021, that is, those deceased or recovered and were included in this analysis. The 2392 (0.3%) individuals who were still hospitalised, and 1462 (0.2%) who were in self-isolation were not included in analysis. The study flow chart and completeness of key data are presented in figure 1B.
Table 1 presents the characteristics of the 7 05 503 cases included in the analysis. The median age was 36 years (IQR 24–50, range 0.1–121), with 93 459 (13.2%) under 18 years, and 364 133 (51.6%) were women, and 233 025 (33.0%) had been hospitalised due to COVD-19. The second wave of the pandemic comprised 372 688 (53.7%) cases, with 288 228 (40.9%) having no chronic comorbidities, 4974 (0.7%) with at least one comorbidity and 412 301 (58.4%) with unknown status of comorbidities.
Individual, community, healthcare characteristics and outcomes of COVID-19 cases in DKI Jakarta, 2 March 2020 to 31 August 2021
Regarding sociodemographics, 150 028 (21.6%) cases lived in subdistricts with the highest population density (22 578–50 829 people/km2, and 175 249 (24.9%) with the highest proportion of poor population (3.6–8.8%). Regarding healthcare, 190 502 (27.0%) lived in the lowest COVID-19 vaccine coverage (33.0–36.1%), 181 890 (25.8%) lived in the highest hypertension prevalence (13.6–33.0%), 184 111 (26.1%) in the highest diabetes prevalence (3.2–5.4%), 163 400 (23.2%) in the highest tuberculosis prevalence (0.5–2.4%) and 173 999 (25.1%) in the highest childhood vaccine coverage (98.9–100.0%) (see table 1 for details).
Of the 705 503 cases with a known outcome, 694 706 (98.5%) had recovered, 10 797 (1.5%) had died and 105 (1.0%) had been declared dead at home and without hospitalisation. The highest numbers of cases (39% of 705 503), and deaths (25% of 10 797) were observed in July 2021 (online supplemental figure 1A). Although a large majority of deaths (76%, 8203) was 50 years or older, death occurred across all age groups. Age-specific CFRs were 0.2% (47/21 793) for <5 years; 0.1% (16/23 070) for 5–9 years; 0.1% (72/66 514) for 10–19 years; 0.2% (311/149 267) for 20–29 years; 0.5% (692/146 900) for 30–39 years; 1.2% (1455/121 454) for 40–49 years; 3.2% (3115/98 934) for 50–59 years; 5.4% (2827/52 776) for 60–69 years and 9.1% (2261/24 761) for ≥70 years (online supplemental table 1 and figure 1B).
Supplemental material
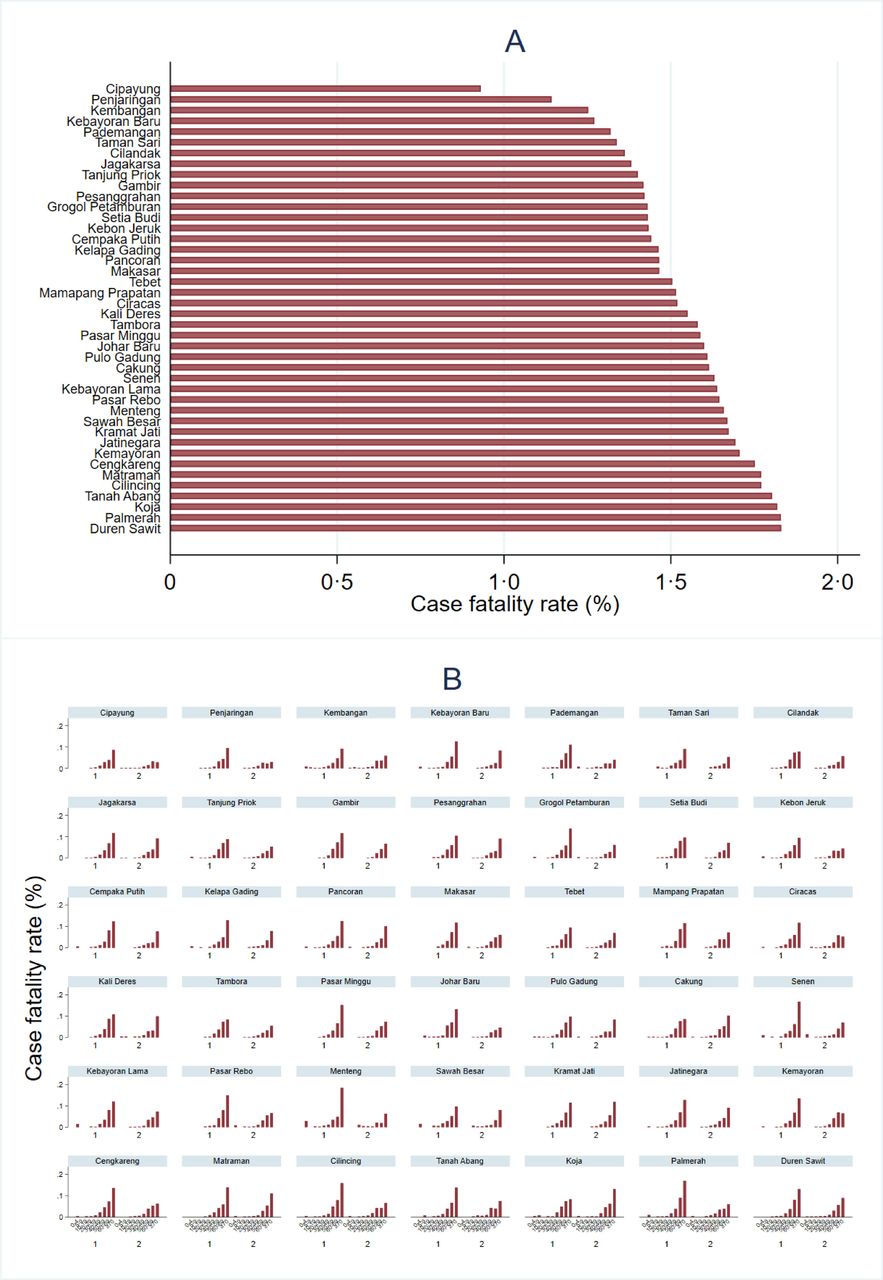
Compared with recovered cases, deceased cases were older (median 59 vs 35 years); more likely to be males (1.8% vs 1.3%), to have one or more comorbidities (9.4% vs 1.0%), to be infected in the first wave (1.9% vs 1.2%), and to live in subdistricts with higher population density (highest density: 1.7% vs lowest density: 1.4%), higher poverty (highest: 1.6% vs lowest: 1.4%); higher nurse–population ratio (lowest: 1.6% vs highest: 1.5%); and lower vaccine coverage (lowest: 1.7% vs highest: 1.4%) (table 1). The CFR ranged from 0.9–1.8% by subdistrict (figure 2A). Compared with the first wave, there was a notable decrease in CFRs across subdistricts during the second wave of the epidemic (figures 2B, 3E,F). Moreover, the subdistricts with higher population density, poverty and lower vaccine coverage tended to be the subdistricts with higher CFR (figure 3A–D), with persistent correlation over time (online supplemental figure 1C).

Overall case fatality rate (CFR) by subdistrict (A) and age-specific CFR per subdistrict and by pandemic wave (B). Age was categorised as 0-4, 5-9, 10-19, 20-29, 30-39, 40-49, 50-59, 60-69, and ≥70 years old.

Characteristics of study sites. Sites categorised based on subdistrict population density (A) poverty level (B) COVID-19 vaccine coverage per 31 August 2021 (C) overall case fatality rate (D) case fatality rate during the first wave (E) and case fatality rate during the second wave (F). Black lines represent the subdistrict administrative border. Detailed summary of characteristic by subdistrict can be found in online supplemental table S7.
In bivariable analysis (table 2), the risk of death was significantly associated with older age, male sex, comorbidities, first wave and higher subdistrict population density, poverty, higher prevalence of tuberculosis, all-cause mortality among under 5 years and lower COVID-19 vaccine coverage.
Bivariable analysis of individual, community and healthcare risk factors associated with COVID-19 mortality in DKI Jakarta, 2 March 2020 to 31 August 2021
In the final multivariable multilevel logistic regression model (figure 4A), the risk of death was increased for age groups 30–39 years (adjusted OR, aOR 1.94, 95% CI 1.62 to 2.33), 40–49 years (aOR 4.51, 95% CI 3.82 to 5.33), 50–59 years (aOR 12.65, 95% CI 10.80 to 14.81), 60–69 years (aOR 18.64, 95% CI 15.87 to 21.89), ≥70 years (aOR 32.91, 95% CI 27.97 to 38.72) compared with 20–29 years; for males (aOR 1.29, 95% CI 1.24 to 1.34); for individuals with at least one comorbidity (aOR 3.96, 95% CI 3.56 to 4.41); for residents of subdistricts with highest population density (aOR 1.34, 95% CI 1.14 to 1.58, reference: lowest density), higher poverty (Q3) (aOR 1.35, 95% CI 1.17 to 1.55, reference: lowest poverty) and with lowest vaccine coverage (aOR 1.25, 95% CI 1.13 to 1.38, reference: highest coverage). We found no associations with proportion of poor sanitation areas, doctor–population ratio, nurse–opulation ratio, prevalence of hypertension, diabetes and tuberculosis (p>0.05 each). The sensitivity analysis revealed similar findings, suggesting there was no significant bias introduced by missing data in our dataset; it also suggested that the risk of death was increased for cases who had at least one comorbidity (aOR 4.25, 95% CI 3.81 to 4.75) compared with those who had no comorbidity (online supplemental table 2).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Final multilevel logistic regression model showing individual, community and healthcare factors associated with COVID-19 mortality (A) and age-specific COVID-19 mortality risk over time (B) in DKI Jakarta, Indonesia, 2 March 2020 to 31 August 2021. Subdistrict was treated as the random effect variable in both models. For analysis presented in (A), first wave=March 2020 to April 2021. Second wave=May 2021 to August 2021. Numeric values were categorised into quartiles (Q) that is, below 25th percentile (lowest), 25th–50th percentile (Q2), 50th–75th percentile (Q3) and above 75th percentile (Highest) for each subdistrict level variable. For (B), each line represents age-specific OR estimates obtained from restricted cubic spline multilevel logistic regression model.
We found that the effect of age was modified by time (first wave), and poverty was modified by population density (p<0.0001). Although higher age was associated with increased risk of death, we found that the risk of death was higher for children 0–4 years (aOR 1.56 95% CI 1.04 to 2.35) compared with adult age 20–29 years in the first pandemic wave, but not in the second wave (online supplemental table 3). We found that mortality risk significantly decreased over time especially for children 0–9 years (figure 4B). In addition, we found that the risk of death was higher for subdistricts with highest level of poverty and density compared with subdistricts with lowest poverty and density (aOR 1.27, 95% CI 1.10 to 1.47) (online supplemental table 4). Sex was not found to be an effect modifier in the final model.
Discussion
This retrospective study described the complete epidemiological surveillance data of PCR-confirmed COVID-19 cases in DKI Jakarta, including 705 503 adults and children living in 44 subdistricts, during two epidemic waves spanning the first 18 months of the SARS-CoV-2 transmission in Indonesia. This analysis represents one of the largest reported case series from any LMIC to date. The overall CFR was 1.5% (10 797/705 503), and deaths occurred across all ages. People aged less than 50 accounted for 75% of cases and 81% of the population, while those older than 50 accounted for 76% of deaths but only 19% of the population. Mortality increased with age, from 1.2% in cases aged 40–49 years to 9.1% in patients aged ≥70 years. In line with previous reports from various settings, the strongest independent risk factors of deaths were older age, male sex and the presence of one or more chronic comorbidities. Important novel findings were that subdistrict-level sociodemographic factors, especially high population density and poverty, and healthcare factors, especially low COVID-19 vaccine coverage, further increased the risk of COVID-19-related death in metropolitan Jakarta.
A previous US study conducted in the early phase of the pandemic showed a significant association between household crowding and COVID-19 outcomes18; counties with the highest household crowding had a nearly twofold higher COVID-19 mortality rate than counties with the lowest crowding. Concordant with that study, we found that residents in subdistricts with the highest population density had a 34% higher risk of death than those residing in subdistricts with the lowest density. This finding typically relates to crowded urban communities who have the lowest standards of sanitation and waste management, and housing along flood-prone riverbanks. These subdistricts are also known to have relatively higher prevalence of non-communicable diseases such as hypertension and diabetes, and poverty-related infectious disease such as tuberculosis (online supplemental table 5), which are well-established risk factors for worse COVID-19-associated clinical outcomes.31 Reducing mortality in these areas may require comprehensive interventions such as improving diagnosis and case management of those known non-communicable and infectious diseases, as well as ensuring high COVID-19 vaccine coverage, and a sustainable social security network that may reduce vulnerability of these communities.
Socioeconomic status including poverty has been associated with COVID-19 mortality in previous studies from South America.15–17 In Chile, living in municipalities with lower socioeconomic status was associated with increased risk of COVID-19-related mortality among general population.15 In Brazil, living in a region with lower socioeconomic status was associated with higher mortality risk among children hospitalised with COVID-19.16 17 Similar to those studies, we found that the risk of death was 40% higher for resident of subdistricts with higher poverty (quarter 3) relative to those of lowest poverty. The interaction between poverty and population density also revealed that the risk of death was 30% higher for subdistricts with highest level of poverty and density compared with subdistricts with lowest poverty and density. Urban crowding and poverty impose very many disadvantages to health, here shown to include elevated risk of death as a consequence of SARS-CoV-2 infection.
The risk of COVID-19-related death in DKI Jakarta was 25% higher for resident of subdistricts with the lowest vaccine coverage (33%–36%), compared with resident of subdistricts with the highest COVID-19 vaccine coverage (41%–51%) as of 31 August 2021. This finding indicates that subdistricts with higher vaccine coverage can significantly reduce risk of mortality compared with those subdistricts with lower vaccine coverage. A previous study from Brazil reported that rapid scaling up of vaccination coverage among elderly Brazilians was associated with significant declines in relative mortality compared with younger individuals, in a setting where the gamma variant predominated.32 Moreover, a recent modelling study estimated that the US states of Florida and Texas could have averted more than 95 000 hospital admissions and 22 000 deaths, if they had reached the vaccination coverage achieved by the top five states and continued at the same pace until 31 August 2021.33 Those observations, corroborated in DKI Jakarta by this study, highlight the health dividend of reduced mortality with rapid vaccination roll outs targeting the most vulnerable in reducing COVID-19-related deaths. As per 5 April 2022, two-dose COVID-19 vaccination coverage was 75.9% (7 648 797/10 083 716 targeted population) in DKI Jakarta,22 and 76.9% (160 182 529/208 265 720 targeted population) in Indonesia.23
Consistent with evidence from previous studies across various settings, our findings affirm that older age, male sex and presence of underlying comorbidities were associated with higher risk of COVID-19-related mortality in the general population of DKI Jakarta, Indonesia.11–13 15 17 The finding that children aged under 5 years old were 60% more likely to die during the first wave but not during the second, especially for those living in vulnerable districts, indicates that the youngest populations have been suffering most from gaps in access to health services, clinical management and community support during the early epidemic response. Similar findings were reported from Brazil, where the risk of in-hospital death was 1.4-fold higher for children aged <2 years compared with those aged 2–11 years, those with comorbidities and living in areas with lower socioeconomics status.16 Hypertension and diabetes have each been associated with elevated risk of COVID-19 death in this setting.13
Findings from this study revealed the extent of pandemic inequity in Indonesia’s capital city of Jakarta, a megacity that has a better health systems capacity (PHDI=66%, ranked 4th of 34th provinces) compared with other areas in Indonesia, except for Bali (PHDI=69%, ranked 1st of 34th provinces), Yogyakarta (PHDI=68%, ranked 2nd of 34th provinces), and Kepulauan Riau (PHDI=66%, ranked 3rd of 34th provinces).26 Our findings could suggest that pandemic inequity may also impact on other areas with lower health systems capacity than Jakarta, equally putting vulnerable groups living in such areas at higher risk of dying with COVID-19. In the context of a heavily decentralised health system such as in Indonesia,25 coordination and prioritisation of available resources and public health intervention will be critical to ensure optimal health outcomes for vulnerable communities, especially for those areas with high poverty, population density and low vaccine coverage.
This study had some limitations. The retrospective design and reliance on routine surveillance data meant that, for some key baseline variables, data were incomplete or uniformly unavailable (eg, type of comorbidities and disease severity classification). The imperfect contact tracing, testing and reporting activities could result in underreporting of cases, especially those asymptomatic and mild cases, therefore, could result in overestimation of CFR in this study. As in many other settings, the individual-level sociodemographics data were not recorded in the current Indonesia’s national database.22 Comorbidities were often self-reported or could be underdiagnosed, potentially resulting in underreporting and hence underestimation of effect sizes. Details on supportive care and treatment received were also not available for this analysis. There are several other relevant sociodemographics variables such as HDI and PHDI that may represent population and health system vulnerability24 but were only available at the district level, and were not included in our analysis. However, our analysis included all available key variables that compose those indicators (prevalence of infectious and non-communicable diseases, healthcare workers–population ratio, universal child immunisation and all-cause mortality among under 5 years old population), therefore, enhancing credibility of our findings.
In conclusion, individual-level risk factors associated with COVID-19 mortality in DKI Jakarta, Indonesia are broadly similar to those in more developed settings, dominated by advanced age and comorbidities. At the community and healthcare level, our analysis suggested that COVID-19 disproportionately affected people living in areas of high population density, poverty and lower vaccination coverage. These findings indicate that vulnerability to death associated with COVID-19 includes not only the elderly and comorbid, but also the urban poor. This finding may inform decisions on health resource allocation against COVID-19 delivering the greatest possible health dividends by prioritising interventions, including vaccination, fort the most vulnerable communities. Future nationwide studies assessing individual, community and healthcare capacity vulnerability associated with COVID-19-related mortality are needed to better understand the COVID-19 impact and to better tailor interventions to prioritise the most vulnerable communities.
Supplemental material
Data availability statement
Data are available on reasonable request. After publication, the datasets used for this study will be made available to others on reasonable requests to the corresponding author, including a detailed research proposal, study objectives and statistical analysis plan. Deidentified participant data will be provided after written approval from the corresponding author and the DKI Jakarta Health Office.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the Health Research Ethics Committee of the National Institute of Health Research and Development, Ministry of Health Indonesia (LB.02.01/2/KE.643/2021). The requirement for patient consent was waived as this was a secondary analysis of anonymised routine surveillance data.
Acknowledgments
This work was funded by the Wellcome (UK) Africa Asia Programme Vietnam (106680/Z/14/Z). We acknowledge all health care workers involved in the care for the COVID-19 patients, as well as those involved in the field data collection. Data cleaning was supported by funding from the Open Society Foundations.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Seye Abimbola
Twitter @henryonce, @lenny_zanri
Contributors HS was the principal investigator of this study. HS designed the study, did the analysis, accepted full responsibility for the work and/or the conduct of the study, had full access to the data, and controlled the decision to publish. NS, VA, WW and DO did data collection and verification. KDL did the data cleaning. HS, AHS, RLH, JKB and IRFE contributed to the analysis and drafted the paper. All authors critically revised the manuscript for important intellectual content and all authors gave final approval for the version to be published.
Funding Wellcome Africa Asia Programme Vietnam (106680/Z/14/Z).
Disclaimer The funder of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report. The corresponding author had full access to all of the data and the final responsibility to submit for publication. All authors were not precluded from accessing data in the study, and accepted responsibility to submit for publication.
Map disclaimer The inclusion of any map (including the depiction of any boundaries therein), or of any geographic or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.