Article Text

Abstract
The COVID-19 pandemic is a devastating reminder that mitigating the threat of emerging zoonotic outbreaks relies on our collective capacity to work across human health, animal health and environment sectors. Despite the critical need for shared approaches, collaborative benchmarks in the International Health Regulations (IHR) Monitoring and Evaluation Framework and more specifically the Joint External Evaluation (JEE) often reveal low levels of performance in collaborative technical areas (TAs), thus identifying a real need to work on the human–animal–environment interface to improve health security. The National Bridging Workshops (NBWs) proposed jointly by the World Organisation of Animal Health and World Health Organization (WHO) provide opportunity for national human health, animal health, environment and other relevant sectors in countries to explore the efficiency and gaps in their coordination for the management of zoonotic diseases. The results, gathered in a prioritised roadmap, support the operationalisation of the recommendations made during JEE for TAs where a multisectoral One Health approach is beneficial. For those collaborative TAs (12 out of 19 in the JEE), more than two-thirds of the recommendations can be implemented through one or multiple activities jointly agreed during NBW. Interestingly, when associated with the WHO Benchmark Tool for IHR, it appears that NBW activities are often associated with lower level of performance than anticipated during the JEE missions, revealing that countries often overestimate their capacities at the human–animal–environment interface. Deeper, more focused and more widely shared discussions between professionals highlight the need for concrete foundations of multisectoral coordination to meet goals for One Health and improved global health security through IHR.
- COVID-19
- health policy
- health systems
- public health
- infections
- diseases
- disorders
- injuries
Data availability statement
Data are available in a public, open access repository.
This is an open access article distributed under the terms of the Creative Commons Attribution IGO License (CC BY NC 3.0 IGO), which permits use, distribution,and reproduction in any medium, provided the original work is properly cited. In any reproduction of this article there should not be any suggestion that WHO or this article endorse any specific organization or products. The use of the WHO logo is not permitted. This notice should be preserved along with the article’s original URL.Disclaimer: The author is a staff member of the World Health Organization. The author alone is responsible for the views expressed in this publication and they do not necessarily represent the views, decisions or policies of the World Health Organization.
Statistics from Altmetric.com
Summary box
The COVID-19 pandemic is a devastating reminder that mitigating the threat of emerging zoonotic outbreaks relies on our collective effort and capacity to work across human health, animal health and environment sectors.
Coordination between human health, animal health and environment sectors in countries can be improved when the International Health Regulations (IHR) and World Organisation of Animal Health’s Performance of Veterinary Services (PVS) frameworks are viewed in tandem, as accomplished through the IHR-PVS National Bridging Workshops (NBWs).
An analysis of NBW activities and collaborative indicators reported by countries in the Joint External Evaluation reveals that countries tend to overestimate their capacities at the human–animal–environment interface.
A deeper, more nuanced discussion between professionals highlights the need for concrete foundations of multisectoral coordination in international frameworks for evaluation, ultimately supporting improved global health security through the implementation of the IHR.
Introduction
While the world is actively fighting against COVID-19, we must acknowledge that in the past two decades, experts have predicted increased frequency of animal–human contacts and the likelihood of emergence of zoonotic pathogens, suggesting that ‘pandemics will become more frequent and more devastating in the future (and) face all countries because once diseases emerge, they travel rapidly and freely through our global networks of travel and trade’.1 Controlling potential emerging pathogens in animals is challenging, if not unrealistic, in particular in wildlife populations.2 Limiting the impact of such emergences relies on the capacity of countries to rapidly detect and respond to outbreaks as soon as they become apparent in animals, in humans or both. Therefore, an efficient early warning and response system for zoonotic events requires routine collaboration between human health services, animal health services and environment services to cover both domestic and wild animals, possibly further informed by the monitoring of environmental factors known to drive emergence or amplification of zoonotic diseases.3 When used to support operational coordination, a multisectoral or One Health approach to collaboration allows for improved performance in surveillance, real-time sharing of information, joint risk assessment, field investigation and riposte across sectors and between multiple actors.4 5
The tripartite (Food and Agriculture Organization (FAO), World Organisation of Animal Health (OIE) and WHO) defines One Health as ‘an approach to address a health threat at the human-animal-environment interface based on collaboration, communication, and coordination across all relevant sectors and disciplines, with the ultimate goal of achieving optimal health outcomes for both people and animals’.5 In this definition, a One Health approach is applicable at the subnational, national, regional and global levels. Benefits of sharing information, joint planning and coordinating actions between human health, animal health and environment sectors have been documented in several papers including by Zinsstag et al,6 with concrete examples of the advantage of One Health for the prevention and control of zoonotic diseases provided.6 However, the author recognises that ‘communication on zoonoses is often totally lacking between public-health and veterinary authorities (and) interactions should be better institutionalised and responsibilities clarified’ (p2143). The need for institutionalisation and clarification of respective roles and mandates in the management of zoonotic events had been critically experienced and successfully overcome during the H5N1 highly pathogenic avian influenza crisis. While the epidemic was instrumental in catalysing multisectoral action, the attention was often difficult to maintain once the crisis was over and other priorities asserted demands and resources.7 It is precisely in ‘peace time’ that joint mechanisms and collaborations between sectors should be organised to improve preparedness for similar challenges to come. Maintaining the momentum on One Health is a daunting task and needs a driving force enabling the institutionalisation of the approach, national ownership and the political support to implement it at national and international levels.8 9
The International Health Regulation (2005) as a driving force
Large-scale transboundary infectious events of zoonotic nature, including the 2009 H1N1 influenza pandemic, the Ebola outbreak in West Africa in 2014–2016 and more recently the COVID-19 pandemic, brought renewed attention to the multidimension of such events, the imperious necessity to engage multiple sectors in the response, the risk posed to global health security by a country’s deficient detection and response capacities and the urgent need to increase preparedness and readiness, and to ensure comprehensive and immediate interventions. This highlights the importance of complying with the International Health Regulations (IHR).10
The IHR was adopted by all WHO member states in 1969 and was initially focusing on a limited number of diseases with the potential to disseminate internationally. In consideration of the increase in international travel and trade, and the emergence, re-emergence and international dissemination of diseases and other health threats, the World Health Assembly (WHA) called for a significant revision in 2005 with the objectives to ‘prevent, protect against, control and provide a public health response to the international spread of disease in ways that are commensurate with and restricted to public health risks, and which avoid unnecessary interference with international traffic and trade’.
As a legally binding framework, the IHR provides rights and obligations to both WHO and state parties (all WHO members and few other countries). In particular, state parties have committed to have or develop minimum core public health capacities to implement the IHR (2005) effectively and to report their level of compliance to the WHA on a yearly basis. This commitment is transposed at their behest into their legislative and regulatory framework, for implementation as appropriate in their specific context. Because the IHR (2005) is a commitment at the highest levels of the governments, is not restricted to the public health sector and encourages a whole-of-government response to health risks, it can be used as a driving force to encourage the previously mentioned institutionalisation of interactions between sectors and constitutes a privileged platform to operationalise the One Health approach towards the prevention, detection and control of public health events.11
The opportunity to use the supportive framework and legally binding environment offered by the regulations to support collaborative efforts at the human–animal–environment interface was initially challenged by the limited knowledge about the IHR (2005) in sectors other than human health.12 The contribution of the veterinary sector in each of the core capacities included in the IHR (2005) was explored, including their links with international standards for animal health, such as the OIE Aquatic and Terrestrial Animal Health Codes.13 With respect to respective mandates and prerogatives, efforts were made to highlight complementarities and to inform the veterinary sector about the IHR (2005) and the relevance of its involvement to increase the visibility and consideration of its deliveries. Similar efforts crossing from the animal health sector to the public health sector have allowed for an improved understanding of the missions and activities of the veterinary services and possible synergies for improved performance.
More concrete connections were possible when the OIE’s Performance of Veterinary Services (PVS) pathway was confronted to the IHR assessment tools and PVS indicators (called critical competencies) linked to IHR core capacities.13 The PVS pathway is the framework for assessing compliance of the veterinary services with internationally adopted standards and for providing support for improvement.14 The bridging between the two frameworks was explored and put into practice rapidly after international communities called for more concrete actions to improve compliance with the IHR (2005), particularly regarding capacities at the human−animal−environment interface. Using legal and regulatory frameworks as foundation was a deliberate decision, since national professionals are familiar with and have experience with working under the IHR (2005) and the OIE frameworks in the public health and animal health sectors, respectively. This knowledge was an asset to ensure both sectors take ownership of results of the bridging exercise and make the necessary adjustments at the human−animal−environment interface.
Linking evaluation frameworks across human and animal health sectors
After the West African Ebola outbreak in 2014, the IHR Review Committee recommended WHO to develop the IHR Monitoring and Evaluation Framework (MEF) to support countries in monitoring and enhancing their capacities and complying with the IHR (2005).15 This framework comprises various components, including the State Party Annual Report (SPAR), which facilitate the mandatory annual reporting of countries of their level of compliance with IHR (2005) and the Joint External Evaluation (JEE) tool, which is a voluntary review of IHR core capacities conducted jointly by national and external experts.16 The contribution of the veterinary sector in each of these components has been summarised elsewhere.11 In 2017, WHO and OIE published a handbook aiming to facilitate the review of JEE technical areas (TAs) by highlighting the role of the Veterinary Services in 16 of the 19 JEE TAs (see table 1) and, out of these TAs, identifying synergies between 35 JEE indicators and the PVS critical competencies.17 These obviously include TAs focusing more specifically on (1) zoonotic diseases, (2) food safety and (3) antimicrobial resistance, but also other TAs such as surveillance, laboratory and response for which multisectoral aspects are usually more neglected in the discussion.18 This effort to improve collaboration during the JEE missions, including through more veterinarians and animal health professionals joining the panel of external experts, was well recognised and contributed to a wider consideration of One Health perspectives in the revision of the JEE tool conducted in 2019.19 The chronology of all these events is illustrated in figure 1.
Association between recommendations made during the JEE missions and joint activities identified during NBW

Illustrates the chronology of events that informed the development of tools to support the implementation of IHR.
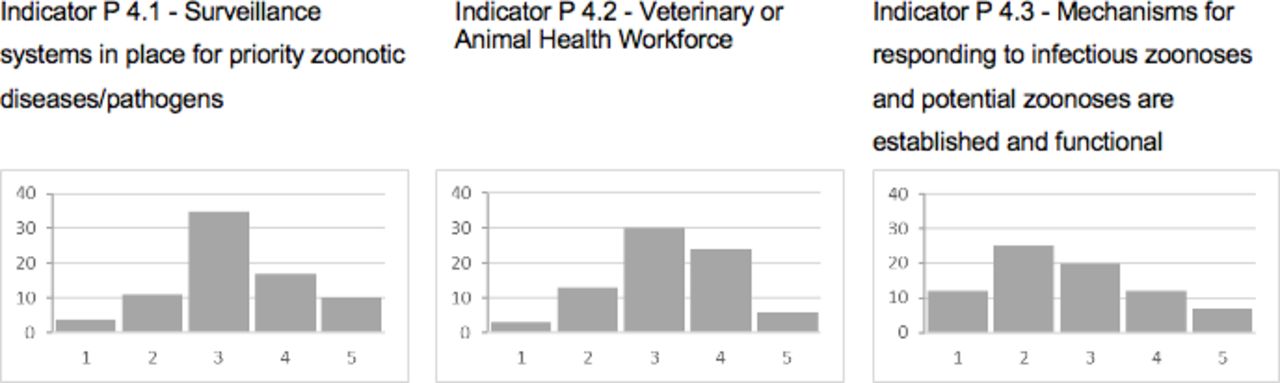
As of November 2020, JEEs have been conducted in a total of 113 countries. During these JEE missions, TAs are discussed using indicators and level of performance scored from 1 (indicating no implementation or very limited implementation) to 5 (performing implementation). As an illustration, the scores for the three indicators of TA zoonotic diseases, all countries included, are summarised in figure 2 and indicate that most countries consider having a surveillance system in place for zoonotic diseases of greatest concern (indicator P 4.1, scores 2–4) and adequate veterinary health forces at national and (most of) subnational levels (indicator P 4.2, scores 3 and 4). The level of performance of their response mechanism to zoonotic diseases is scored lower (indicator P 4.3, scores 2 and 3), mainly because of limited coordination institutionalised between human, animal and wildlife sectors.
{kind=link}
{kind=link}
Illustrates the mean scores for three indicators of JEE TA zoonotic diseases, all countries included.
One Health roadmaps to operationalise the recommendations of JEEs
Beginning in 2014, the effort to use the IHR (2005) as a driving force for the implementation of the One Health approach for health security also resulted in the implementation of IHR-PVS National Bridging Workshops (NBWs) jointly developed by WHO and OIE.20 These events conducted in countries provide the opportunity for the two sectors to jointly review the results of the IHR MEF (JEE and/or SPAR) and PVS pathway and to agree on concrete and operational activities to fill the gaps in their coordination between the two sectors for the core functions of the IHR (2005).13 The exercise, conducted with professionals from multiple sectors and operating at various level in the national system, used a methodology ensuring full engagement and appropriation of the results by the participants. One of the outputs of a NBW is a jointly developed, detailed, practical, realistic and consensual roadmap prioritising activities to improve coordination at the human–animal–environment interface. Jointly agreed activities included in this roadmap are later used to inform multisectoral One Health action planning.21
The need for more interactions between the human health, animal health and environment sectors was widely recognised and almost systematically mentioned in the JEE recommendations (Zinsstag, in press). Given that the NBWs focus on zoonotic diseases and food safety issues, they do not extensively cover four JEE TAs: Antimicrobial resistance, biosafety and biosecurity, immunisation, and linking public health and security authorities. However, biosafety and biosecurity issues are usually addressed in the discussion on laboratories, and despite possible misuse of zoonotic pathogens, no particular priority is being given to the dimension on security.
From the 16 previously mentioned JEE TAs, a total of 180 standardised recommendations were identified, 129 recommendations if the four TAs less extensively covered during the NBWs are removed. In parallel, the database summarising the NBW activities from 22 countries covered from 2017 to 2019 includes 66 standardised activities, grouped in 13 categories. The mapping exercise between the two databases revealed that out of the 129 recommendations, 89 (69%) have one or multiple NBW activities associated (table 1).
Some TAs (identified with an asterisk in table 1: IHR coordination, communication and advocacy, zoonotic diseases, real-time surveillance, preparedness, emergency response operations, medical countermeasures and personnel deployment) have NBW activities associated with more than 70% of their recommendations, confirming the contribution of these activities in their operationalisation. Workforce development is also a TA for which concrete activities such as strengthening of curriculum or specific continuing education programmes are frequently proposed during the NBWs. Interestingly, only half of the recommendations made for the food safety TA are associated with NBW activities, possibly because most of its recommendations target a wider scope than the zoonotic component discussed during the NBWs (eg, food safety national plan, guidelines, specific legislation and regulation, control at points of entry and international networks). Most of the JEE recommendations (64%) are associated with a unique activity proposed during NBWs; 30% are associated with two; and 6% with three or more. The five most informed JEE recommendations, with four NBW activities or more, are reported in table 2, reflecting the needs identified during the NBWs to conduct complementary actions for their implementation.
JEE recommendations for which four or more activities are included in the NBW roadmaps
Benchmarking performance against expected IHR core capacities
The WHO Benchmark Tool for IHR capacities (IHR Benchmark Tool, hereby referred to as BT) developed in 2019 proposes a set of actions that can be applied to increase the performance of countries in TAs, thus strengthening their IHR capacities.22 The BT covers all 13 IHR capacities delineated in the SPAR and 19 TAs delineated in the JEE tool, slightly differently organised. For example, the JEE has three indicators for zoonotic diseases but this TA is covered by only two benchmarks, the actions related to veterinary workforce being included in the benchmark on human resources instead.
Similar to the JEE, NBW activities can be associated with 12 BT TAs, in which 30 out of 32 benchmark actions are further informed and operationalised by a total of 58 different NBW activities (table 3). Benchmarks on zoonosis and food safety logically gather the highest number of associations and the widest diversity of NBW activities (respectively 74% and 52% of the NBW activities listed are associated with these TAs). In comparison, a large number of NBW activities can be associated with human resources, but with a lower diversity (31%), meaning that most of the NBW activities associated with its four benchmarks are the same.
Benchmarks and associated NBW activities
Interestingly, NBW activities are often associated with improvement at a low level of performance in the BT. A global review indicates that 36% of NBW activities are associated with an improvement from level 1 to level 2, and 35% from level 2 to level 3, all TAs considered together. In more details for the TA on zoonotic diseases, 19% of NBW activities support the improvement from level (L) 1 to L2 of benchmark 4.1 (Coordinated surveillance system for priority zoonotic diseases) and 47% from L2 to L3. For benchmark 4.2 (Mechanism to respond to priority diseases), 19% of NBW activities support progress from L1 to L2, and 54% from L2 to L3. Similarly, for the TA on human resources, which includes the veterinary workforce, frequencies are 40% from L1 to L2, and 40% from L2 to L3. These results contrast with those of the JEE, when performances were ranked higher, for surveillance and workforce development (figure 2), revealing that countries often overestimate their capacities at the human–animal–environment interface during JEE. Deeper, more focused and nuanced discussions between professionals during NBWs highlight the need to strengthen foundations of multisectoral coordination for most of the TAs.
Conclusion
Operationalising One Health, multisectoral approaches remain challenging, even when the need for collaboration seems obvious as it is the case at the human–animal–environment interface for the management of zoonotic diseases. A number of institutional and administrative problems hamper collaboration across various ministries.8 There may simply be legal or other structural and functional barriers to cooperation between sectors like public health, animal health, wildlife, environment and other relevant partners, such as diverging mandates or rivalries over budget allocations. There may also be cultural and perception issues to overcome, requiring cultural shifts and behavioural changes among professionals within agencies.12 Joint review of capacities and resulting evaluation frameworks is an effective and efficient exercise to improve dialogue. This allows for the shared exploration of synergies between sectors, allowing them to act jointly, using One Heath tools developed for strengthening specific or more transversal TAs.23 Deeper follow-up discussions and the engagement of a wider professional audience and relevant authorities, including those working at the subnational levels in countries, help to complement the recommendations with more concrete and operational inputs. In particular, detailed planning of activities jointly developed for critical TAs such as surveillance, human resources and workforce development, field investigation, laboratory functions and joint response to emergencies is instrumental in building partnerships and coordination between sectors, which strengthen almost all the IHR core capacities reviewed in the IHR MEF. Even more productive is to build on this coordination with concrete activities such as joint risk assessments, after-action reviews or simulation exercises, which create the opportunity to test the reported performance.5 24
There is currently a concerted effort to ensure that IHR core capacities are an integral part of broader health systems to achieve both goals of health security and universal health coverage.25 This approach and associated principles are fully endorsed by the international community as a way forward to help countries build back better after COVID-19, and were already reinforced years ago by the tripartite—FAO, OIE and WHO—in their first tripartite concept note.26 It can be expected that the implementation of the NBW roadmaps can contribute to this integrative effort for a more coordinated approach, ultimately strengthening collaborative capacity at the human–animal–environment interface.
Data availability statement
Data are available in a public, open access repository.
Ethics statements
Patient consent for publication
References
Footnotes
Handling editor Seye Abimbola
Contributors This article has been informed by the authors’ research, practice and evaluation of the use of Joint External Evaluation (JEE), WHO Benchmark Tool and National Bridging Workshops (NBWs) to support improved coordination between human health and animal health sectors in countries. SdlR, GB, AS, TS, TT, NI, GG, FC and MC supported the development and piloting of the NBW methodology, including a cross analysis of International Health Regulations (IHR) and Performance of Veterinary Services. SdlR, GB, KMME, RS, DS, AT, NK, JX and SC contributed their expertise in IHR and JEE, as well as related tools and approaches for strengthening collaborative health security. All authors were involved in developing, writing and revising the article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.