Article Text

Abstract
Introduction The private sector accounts for an important share of health services available in South Asia. It is not known to what extent socioeconomic and urban–rural inequalities in maternal, newborn and child health (MNCH) interventions are being affected by the presence of private providers.
Methods Nationally representative surveys carried out from 2009 to 2015 were analysed for seven of the eight countries in South Asia, as data for Sri Lanka were not available. The outcomes studied included antenatal care (four or more visits), institutional delivery, early initiation of breast feeding, postnatal care for babies, and careseeking for diarrhoea and pneumonia. Results were stratified according to quintiles of household wealth and urban–rural residence.
Results At regional level, the public sector played a larger role than the private sector in providing antenatal (24.8% vs 15.6% coverage), delivery (51.9% vs 26.8%) and postnatal care (15.7% vs 8.2%), as well as in the early initiation of breast feeding (26.1% vs 11.1%). The reverse was observed in careseeking for diarrhoea (15.0% and 46.2%) and pneumonia (18.2% and 50.5%). In 28 out of 37 possible analyses of coverage by country, socioeconomic inequalities were significantly wider in the private than in the public sector, and in only four cases the reverse pattern was observed. In 20 of the 37 analyses, the public sector was also more likely to be used by the wealthiest women and children.
Conclusion The private sector plays a substantial role in delivering MNCH interventions in South Asia but is more inequitable than the public sector.
- health equity
- maternal–child health services
- socioeconomic factors
- health status disparities
- Asia
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
The private sector is known to play a major role in the delivery of health services in the South Asia region, yet little is known regarding how it affects inequalities in intervention coverage for women and children.
Earlier analyses of coverage with reproductive and maternal interventions suggest that the distribution of services across wealth quintiles tended to be more equitable in the public than in the private sector. These analyses did not provide formal statistical comparisons of the magnitude of inequalities between the two sectors, nor included the most recent surveys. None of the analyses provided regionally aggregated results.
What are the new findings?
Our analyses of nationally representative surveys from seven of the eight countries in South Asia confirm the important role played by the private sector in providing preventive and curative interventions to women and children in this region.
Our findings on socioeconomic inequalities in coverage show that the private sector tends to be markedly more unequal than the public sector throughout the seven countries and for all interventions under study.
What do the new findings imply?
Our analyses suggest that, unless proactive efforts are made to the contrary, greater involvement of the private sector may exacerbate inequalities in reproductive, maternal, newborn and child health coverage, and if involvement of the private sector is deemed as essential for reaching the health-related Sustainable Development Goals, measures must be put in place to monitor and correct its potential negative impact on health inequalities.
Introduction
During the era of the Millennium Development Goals (MDGs), much progress was achieved in terms of population coverage with key maternal, newborn and child health (MNCH) interventions in South Asia.1 Between 2000 and 2015, maternal mortality fell by 53% and under-five mortality by 47%.2 3 However, progress at the national level does not necessarily mean that within-country inequalities were reduced4 and, despite the clear progress, substantial challenges remain.5 Most notably, South Asia’s neonatal mortality rate is particularly high, and 40% of newborn deaths globally are in South Asia.3 6
The Sustainable Development Goals (SDGs)7 include a comprehensive set of MNCH targets that address the unfinished MDG agenda, while expanding the health agenda to include additional major challenges such as non-communicable diseases, injuries and the environment. The SDG target on universal health coverage (UHC) underpins all health-related targets and provides an opportunity to refocus efforts toward a sustainable approach through system-wide reform. Achieving the SDG targets for MNCH will represent a huge challenge for some South Asian countries. The current annual rates of reduction (ARRs) in maternal mortality, stillbirths and newborn mortality are much lower than the ARRs that are necessary to meet these global targets in countries such as Afghanistan, Bangladesh, India and Pakistan6 (UNICEF. Save Newborns).8
There is growing recognition of the role played by the private sector in providing MNCH interventions in many countries. The 2018 report of the Independent Accountability Panel for Every Woman, Every Child, Every Adolescent9 stated that ‘at this point in the roadmap to 2030, it is essential to get it right regarding the private sector’s accountability for women’s, children’s and adolescents’ well-being, and for public health’. This plea is particularly relevant for South Asia, which is widely known for the strong role played by the private sector in providing health services. According to a recent review, ‘healthcare services in South Asia are characterised by low public investment, dependence on services provided by the private sector, and very high rates of out of pocket expenses as the principal source of health financing’.10 The same authors found that most people in South Asia depend on private providers for healthcare and that public investment in health has stagnated. As shown in WHO and World Bank’s report in 2018, domestic private health expenditure in 2015 was very high in some South Asian countries, corresponding to 78% of total health expenditure in Afghanistan, 74% in Bangladesh, 71% in India and in Nepal and 69% in Pakistan. Furthermore, among domestic private health expenditure, more than 90% are out-of-pocket expenditure which has exposed individuals to financial hardship.11 Although private health expenditure by households is a only a proxy for the size of the private sector, these figures support the major role of the private sector in the region.
The public and private sectors differ in terms of geographic distribution, out-of-pocket costs to families and therefore economic accessibility and likely on quality of care. It is therefore likely that reliance on private or public sector will vary according to wealth and place of residence. Given South Asia’s need to accelerate progress on key MNCH indicators, as well as existing high private sector expenditures, it is important to assess the current role of the private sector in advancing progress toward the equitable achievement of SDG targets for women’s and children’s health.
The aim of the present analyses is to determine the relative importance of the private and public sectors in providing MNCH care in South Asian countries, with particular emphasis on their role in terms of equitable coverage. The objectives are to summarise source of care for key MNCH intervention indicators in South Asian countries with recent data; examine socioeconomic and urban–rural inequalities of key MNCH indicators, within the public and private sectors; and to discuss the policy and programmatic implications of these findings regarding the achievement of UHC for women and children.
Methods
The analyses were carried out using the most recent national survey available for seven of the eight countries in the region, as a recent survey was not available for Sri Lanka. Demographic and Health Surveys (DHS) were available for Afghanistan (2015), Bangladesh (2014), India (2015 National Family Health Survey, based on the DHS methodology), Maldives (2009), Nepal (2016) and Pakistan (2012). Bhutan had data from a Multiple Indicator Cluster Survey (MICS) carried out in 2010. Both types of surveys use multistage sampling to identify women aged 15–49 years and children under the age of 5 years. Their questionnaires and indicator definitions are highly comparable.12 Further information is available elsewhere on DHS13 and MICS.14
The following coverage indicators were selected as proxies of care during the various stages of the continuum of MNCH care: four or more antenatal care visits, place of delivery (home or institution), early initiation of breast feeding, postnatal care for babies, careseeking for suspected pneumonia and careseeking for diarrhoea. Population coverage was expressed as the proportion of those in need of an intervention who received it. For example, the number of births was the denominator for delivery care, and the number of children under the age of 5 years who presented diarrhoea in the 2 weeks preceding the survey was the denominator for the diarrhoea careseeking indicator. Indicator definitions, with their respective denominators, are available in online supplementary Webannex A.
Supplemental material
For each indicator, public and private sector contacts were differentiated. The types of facilities and providers defined as public or private in each country are shown in online supplementary Webannex B. In accordance with WHO definitions (http://apps.who.int/gho/data/node.wrapper.imr?x-id=4737), informal providers such as shops selling drugs, quacks and traditional birth attendants are not included in the analyses. Typically, public facilities include hospitals, clinics and primary care units run by the government, while private facilities include hospitals and clinics run by for-profit or not-for-profit institutions. Online supplementary Webannex C shows how different categories of private providers contributed to coverage in each country. For indicators including multiple contacts—such as antenatal care and careseeking—some women and children who used both types of providers were classified in a combined ‘public and private’ category. Early initiation of breast feeding was also analysed for home births, in addition to the two types of providers involved in delivering the child.
Supplemental material
Supplemental material
Coverage in the public and private sectors was stratified according to household wealth quintiles and urban–rural residence. Wealth indices were calculated through principal component analyses of data on household appliances (such as televisions and refrigerators), characteristics of the dwelling (materials used for the walls, floor and roof), presence of electricity, type of water supply and sanitary facilities and other variables related to economic status (ownership of the house, land or livestock). Because relevant assets may vary in urban and rural households, separate principal component analyses are carried out in each area, which are later combined into a single score using a scaling procedure to allow comparability between urban and rural households.15 The values of wealth index for each household were calculated by the survey analysts and are available in the original databases; these were used to divide the sampled households into quintiles.15 The classification of urban or rural residence was based on criteria defined by each country.
Two summary measures of inequality, based on the frequency of the outcomes in the five wealth groups, were calculated. The slope index of inequality expresses absolute inequalities, being based on a logistic regression approach with coverage as the outcome and wealth as the exposure.16 It is expressed as the difference in percentage points between the fitted values of the coverage indicator for the top and the bottom of the wealth distribution. The concentration index, on the other hand, reflects relative inequalities and is based on a concept similar to the Gini Index for income concentration; for the purpose of easier presentation, we scaled both indices from −100 to +100. Both take a value of zero when there is perfect equality among all socioeconomic groups; positive values indicate higher coverage among the rich than the poor, and negative values indicate the opposite trend. Further information on these indices and their calculation is available elsewhere.16
Regional estimates for South Asia were obtained by weighting the national results by the country’s total number of births; for the careseeking, the weights consisted of the country’s under-five population. Information on births and under-five population for 2016 was obtained from the UNICEF publication State of the World’s Children.17
Statistical tests were initially used for assessing the significance of the associations between wealth quintiles and coverage estimates; p levels for the slope and concentration indices (in the online supplementary materials) show how far the observed distribution is from the line of perfect equality. The inequality measures and respective SEs were obtained from our own reanalyses of the surveys. These were used to test the differences between inequality indices in the public and private sectors, using Z-tests based on a normal distribution approximation and considering inequality in each group independent. The Stata command ztesti was used for this purpose.
All analyses are based on anonymised, publicly available datasets. Stata was used for all analyses (StataCorp. 2017. Stata Statistical Software: Release 15; Stata, College Station, Texas, USA). Ethical clearance for data collection was obtained by the national institutions responsible for the national surveys.
Patient and public involvement statement
There was no involvement of patients as the analyses were based on data from publicly available, population-based surveys carried out in the past.
Results
The numbers of births in the 2 years reported in each survey ranged from 2465 in Bhutan to 259 469 in India, with a median of 5038 (Nepal). The number of women and children included in the analyses, by country, are shown in online supplementary Webannex D. The Bhutan survey did not provide information on antenatal or postnatal care, nor on careseeking for diarrhoea. The Nepal and Maldives surveys did not collect information on postnatal care.
Supplemental material
Regional and national results
On aggregate across South Asia, the population coverage of the interventions studied varies from 27.4% (postnatal care) to 78.7% (institutional delivery) (figure 1). Only three interventions—institutional delivery (the sum of deliveries in the public and private sectors) and careseeking for diarrhoea and pneumonia—had regional coverage greater than 60%. The lowest coverage levels were observed for the newborn indicators: postnatal care and early initiation of breast feeding.

Coverage in the public and private sector for key interventions, aggregated results for the South Asian region.
The data labels in figure 1 show the proportions of the population covered in the public and private sectors. Using all provider contacts as the denominator, the private sector accounted for 30.9% of all antenatal care, 34.1% of institutional deliveries, 30.1% of postnatal care, 29.8% of early breastfeeding initiation, 73.2% of diarrhoea and 75.3% of pneumonia care.
The regional results are heavily driven by the more populous countries, particularly India and to a lesser extent Bangladesh and Pakistan. However, overall coverage—including both public and private sectors—varied markedly from country to country (figure 2). For example, institutional deliveries ranged from 37.6% in Bangladesh to 95.4% in the Maldives and antenatal care from 17.8% in Afghanistan to 85.4% in the Maldives. The Maldives also showed the highest national coverage with early initiation of breast feeding and careseeking for diarrhoea. Of the four countries with available information on postnatal care, the highest coverage was observed in Bangladesh. Variability in pneumonia careseeking was less marked, ranging from 42.0% in Bangladesh to 78.1% in India.

Coverage in the public and private sectors for key interventions, by country. BF, breast feeding.
In addition to variations in overall coverage, there were marked between-country differences in terms of the public/private mix. Figure 2 shows the results for the six coverage indicators, by country. The private sector was seldom used for most interventions in Afghanistan, Bhutan and Maldives, where the public sector was responsible for most contacts. In contrast, the private sector accounted for a large share of contacts—often more than half—in Bangladesh, India and Pakistan. In Nepal, much of the careseeking for diarrhoea and pneumonia relied on the private sector, in contrast for antenatal or delivery care where the public sector predominated.
The types of private providers varied by country and by intervention. Online supplementary Webannex C shows the proportions of contacts with different private providers, among women and children who sought private care; the total may exceed 100% when more than one provider was sought. Non-governmental institutions were most frequently used in Bangladesh—where they accounted for up to 23.6% of private contacts—than in other countries where these represented less than 10% of contacts. For antenatal, delivery and postnatal care, private hospitals or maternity homes accounted for most private contacts, followed by private doctors’ offices. The latter were particularly frequent in Afghanistan. Careseeking for diarrhoea and pneumonia was mainly sought from hospitals in the Maldives and Nepal, and from private doctors’ offices in the remaining countries.
Analyses by wealth quintile
The second part of the analyses was focused on wealth-related and urban/rural within-country inequalities in overall coverage, as well as within the public and private sectors.
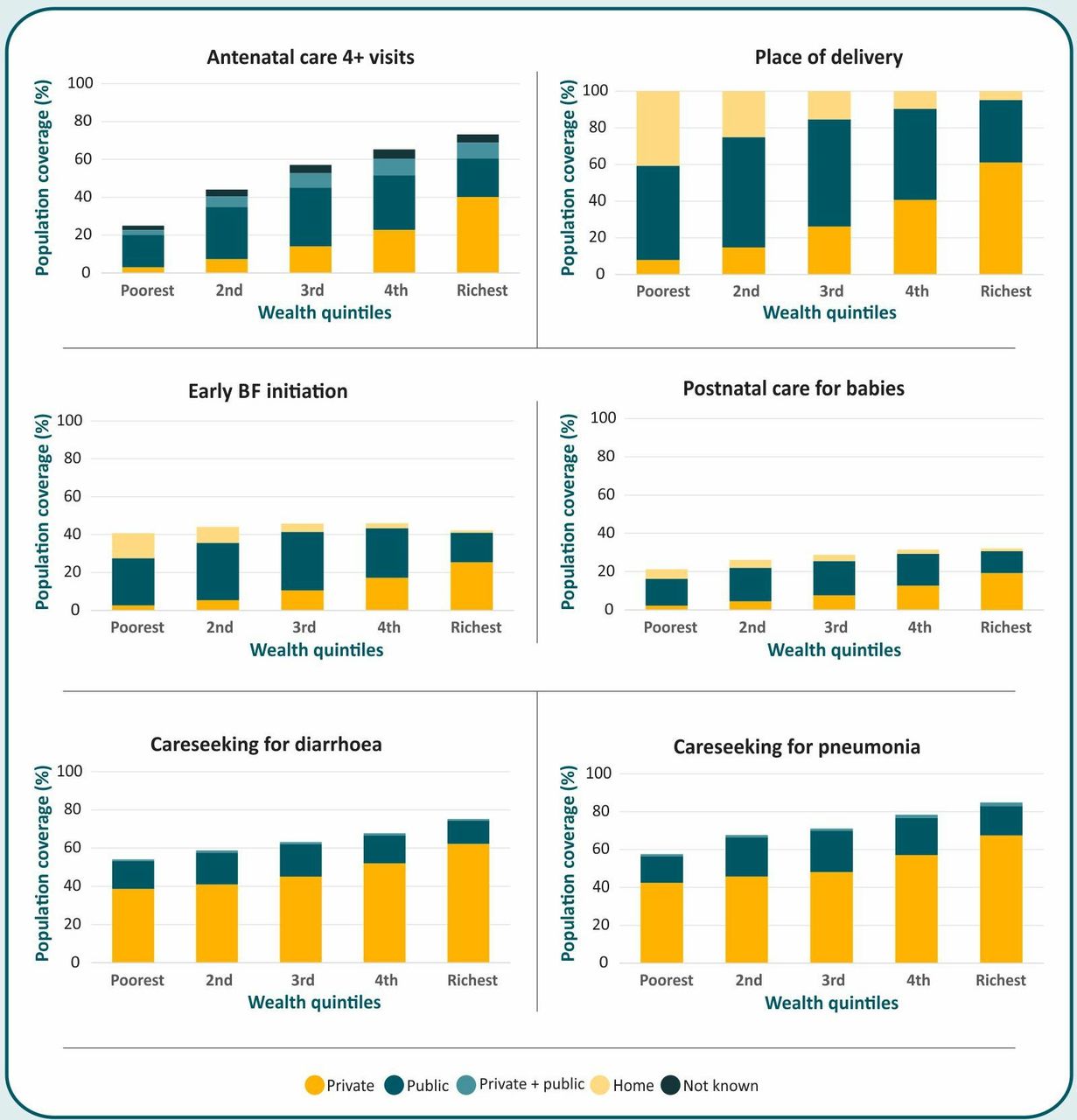
Figure 3 shows wealth-related inequalities in the six coverage outcomes for the whole region, based on the population-weighted indicators. There were very strong direct associations between coverage and wealth for the indicators, with two exceptions: early initiation of breast feeding and postnatal care, both of which had low coverage in all quintiles.

Intervention coverage in the public and private sector by wealth quintile, for the region.
The indicator with the sharpest wealth-related inequalities was the place of delivery (figure 4). In all countries studied, home deliveries were most common in the poorest quintile, and private sector deliveries most common in the wealthiest quintile. In the three countries with the lowest proportion of private-sector deliveries in the whole population—Afghanistan, Bhutan and Nepal—the public sector was most used by wealthy women. The opposite was found in the Maldives and in India, where women in the poorer quintiles were more likely to use the public sector than those in the wealthiest quintile—as most of the latter relied on the private sector as mentioned. In Bangladesh and Pakistan, the proportions of women delivering in public facilities increased only slightly with family wealth. Graphs showing wealth-related inequalities by country and public–private sector for the remaining coverage indicators are shown in online supplementary Webannex E.
Supplemental material

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Place of delivery by wealth quintile, by country.
Summary measures of inequality
We compared the magnitude of wealth-related inequalities in the public and private sectors, by indicator and countries. The results for absolute and relative inequalities were very similar except for Afghanistan and Bhutan, where the private sector is very small and relative ratios may provide different results from absolute differences. To simplify the description of the findings, table 1 presents the results for absolute inequality (slope indices), and online supplementary Webannex F presents the results for relative inequalities (concentration indices). Absolute measures are easier to interpret, as the difference in coverage between the extremes of the wealth scale is expressed in per cent points, and unlike the concentration index, the slope index is not highly sensitive to coverage in the poorest groups.
Supplemental material
Values of the wealth-based slope index for absolute inequality (expressed in per cent points) in the public and private sectors, by intervention and country
The slope index indicates the difference in coverage, expressed in per cent points, between the wealthiest and poorest ends of the socioeconomic scale. Positive values correspond to higher coverage among the rich than the poor, that is, pro-rich inequalities. These are shown in black font (table 1). All indices for the private sector are in black font, indicating pro-rich patterns for every interventions in every country. Pro-rich inequalities are also common in the public sector, except for diarrhoea and pneumonia careseeking.
Negative values of the slope index signal pro-poor inequalities, all of which were found in the public sector, particularly for the careseeking variables. It is also worth noting the presence of pro-poor inequalities in the public sector for all interventions in the Maldives.
Still in table 1, we compared the magnitude of inequalities between the two sectors. Cells that are highlighted in blue indicate that pro-rich inequalities were significantly larger in the private than in the public sector, whereas yellow cells show the opposite. Cells that are not highlighted presented similar levels of inequality in both sectors (p>0.05; exact p values are shown in table 1). Of the 37 cells with data, 28 are blue, thus indicating that the private sector tends to show greater pro-rich inequalities than the public sector. The exceptions are Afghanistan and Bhutan, where the yellow cells show stronger pro-rich inequalities in the private than in the public sector, as the latter is rarely used in these countries.
Analyses by urban/rural residence
There were also differences in coverage levels according to place of residence (table 2), but these patterns varied markedly by country and by intervention. In table 2, cells in black font indicate higher coverage in urban than in rural area within a given sector, and those in red font show the opposite trend. Cells highlighted in yellow show significantly greater urban–rural gaps in the private than in the public sector, while blue cells show the opposite pattern. Patterns varied by country and by intervention. Afghanistan mostly shows higher coverage in the public than in the private sector, particularly in rural areas. The reverse is true for Bangladesh, where the private sector is the most frequent source of care in both areas, but particularly for urban women and children. In Bhutan, the private sector is virtually absent. India shows a complex pattern: for careseeking, the private sector predominates in both urban and rural areas; for antenatal and postnatal care, urban areas had similar reliance on both sectors, but rural areas had greater use of public sector; for delivery care and early initiation of breast feeding, the public sector preference was mostly marked in rural than urban areas. In the Maldives, the public sector led for most indicators, particularly in the rural areas, and it also predominated in Nepal, except for the two careseeking indicators in urban areas. Lastly, in Pakistan both urban and rural areas showed substantially higher use of the private than the public sector, for all interventions.
Table 2Coverage (%) in urban and rural areas, by intervention, country and type of provider
Table 2 also shows urban/rural coverage ratios by intervention and sector. In most countries, private care is more common in urban than in rural areas, whereas public care is more equitably distributed.
Discussion
Given the major interest on how the private sector may contribute to achieving the health-related SDGs,9 disaggregation of coverage statistics by type of provider is essential for understanding the magnitude of inequalities in health and for proposing policy and programmatic interventions to address such inequalities. Our analyses contribute to a comprehensive examination of MNCH coverage disparities in the public and private sector in South Asia and globally.
Earlier analyses have assessed the role of private and public sector providers in delivering a limited number of interventions in several countries in South Asia and elsewhere,18–22 but there was limited overlap with the present analyses. In particular, we update and expand on the findings from a 57-country analysis of DHS carried out up to 2012, which included six South Asian countries; we relied on more recent surveys for five of these countries and were able to also include Bhutan.23 We report on standardised results for seven of the eight countries in South Asia, which jointly account for more than 95% of all children under the age of 5 years in the region. The existing literature suggests that the private sector tends to be less equitable than the public sector. None of these earlier analyses included formal statistical comparisons of the magnitude of inequalities by sector.
At regional level, three interventions—institutional delivery and careseeking for diarrhoea and pneumonia—had coverage between 60% and 80%, whereas the other three—four or more antenatal care visits, postnatal care and early breastfeeding initiation—failed to reach most women and children. The very low coverage with the last two interventions is noteworthy. It is important to note that these were introduced more recently than the other four, which may explain their low coverage.24
Our analyses confirm the major role played by the private sector in delivering maternal and child healthcare in the region.10 25 Yet, we show that the public–private mix varied substantially by country and type of intervention. For the region as a whole, the public sector accounted for most of the coverage with maternal and newborn interventions, but the private sector is responsible for most of the careseeking for childhood diarrhoea and pneumonia. Child immunisations were not included in the present analyses, but a 2011 review showed that private sector provision accounted for a very small fraction of all vaccines provided to children in Bangladesh, Pakistan and Sri Lanka, and possibly a higher proportion (17% in the 1990s) in India.26
The analyses by wealth quintile are revealing. Except for the two more recent interventions—postnatal care and early initiation—all other indicators show substantial socioeconomic gradients not only in terms of overall coverage but also according to the type of provider. Our analyses of the magnitude of inequalities by sector (table 1) show that the private sector is more inequitable than the public sector in all countries except in Afghanistan and Bhutan, where the private sector shows very low coverage.
Both public and private providers contribute to inequalities. Women and children from wealthier families tend to rely both on the private and public sectors, while those from poorer families rely primarily on the public sector, except for careseeking for children.
Urban–rural differences in the public–private patterns were less marked than those associated with wealth. Either private providers predominated both in urban and rural areas (as was the case for Bangladesh and Pakistan) or the public sector led in both areas (as in Afghanistan, Bhutan and Maldives). A mixed pattern was observed in India and Nepal, where the public sector led for all interventions in urban and rural areas, except for careseeking for diarrhoea and pneumonia, where the private sector predominated; in Nepal, this was only observed in urban areas.
In Bangladesh, Pakistan and India, the greater share of the private sector in providing child healthcare is consistent with the findings from the literature—namely, that out-of-pocket expenditures in these countries account for more than 50% of health spending.27 It is also noteworthy that in several countries even the poorest families rely mostly on the private sector, particularly for case management of childhood illnesses.
Care for diarrhoea or respiratory symptoms sought from pharmacies and drugstores was not included in the present analyses, which were limited to appropriate healthcare providers as defined by DHS in conjunction with national governments, and in agreement with the WHO definition of appropriate care (http://apps.who.int/gho/data/node.wrapper.imr?x-id=4737). Nevertheless, two of the original DHS reports provide detailed breakdowns on use of pharmacies or drugstores for pneumonia, by wealth quintile. In Bangladesh,28 the percentages of children taken to such shops were 27.3, 28.3, 26.8, 25.6 and 16.5 in wealth quintiles 1–5, showing lesser use by children from the wealthiest families. In Bhutan,29 no children with pneumonia symptoms were taken to a pharmacy or drugstore in the four poorer quintiles, and only 0.9% of those in the wealthiest quintile sought such care. Therefore, these shops may account for a substantial proportion of care sought in countries such as Bangladesh, but are seldom used in others such as Bhutan.
Our analyses have some limitations. First, there were no data for Sri Lanka, and for the Maldives the most recent publicly available survey is from 2009 and for Pakistan from 2012; however, inequalities in coverage tend to change slowly, so that this is unlikely to have substantially affected the comparisons. Second, the classification of private sector providers included both for-profit and not-for-profit clinics, such as non-governmental organisations (NGOs), of which latter might well be more equitable. Given that NGOs accounted for less than 10% of private contacts (except for antenatal, delivery and postnatal care in Bangladesh), it was not possible to further investigate this possibility. Third, the information on coverage is obtained by recall, usually by the women who were interviewed about their pregnancies and their children. Fourth, we used household asset indices for estimating socioeconomic position; such indices only reflect relative position within the survey sample in each country, and not absolute wealth. Indices were calculated separately for rural and urban areas, and then merged into a national index.15 The marked differences in coverage by socioeconomic position suggests that the wealth index was able to identify subgroups of the population with different access to services in each country. The regionally aggregated results must be interpreted while bearing in mind that the quintiles represent within-country relative wealth distributions, and that the actual cut-offs in terms of absolute wealth may vary from country to country.
Our analyses do not address effective coverage, that is, the adequacy and quality of the care provided during the contacts with health workers. For some countries, particularly the Maldives and Nepal, sample sizes for pneumonia careseeking were small due to low numbers of children with this condition in the 2 weeks preceding the survey (see online supplementary Webannex D). Our population-weighted results are heavily influenced by the large Indian population, yet provide a detailed overview of the region as a whole; country-specific results are also provided in the tables and online supplementary Webannexes.
Policy and programmatic interventions must reflect the public–private mix in each country, and in particular the different cadres of private providers, which were classified into four categories by McPake and Hanson: ‘the low-quality, underqualified sector that serves poor people in many countries; not-for-profit providers that operate on a range of scales; formally registered small-to-medium private practices; and the corporate commercial hospital sector, which is growing rapidly and about which little is known’.30 For example, in countries with strong presence of the low-quality private sector, such as Bangladesh, India and Pakistan, strategies must be designed to boost the public sector, which is generally more equitable as the above results show. Recognising that expansion of the public sector may require long-term investments in most countries, immediate strategies must be put in place to promote the use of appropriate private providers by poor and rural women and children, and to overcome the monetary, geographic and cultural barriers that hamper their access to the private sector. The India’s Janani Suraksha Yojana scheme of providing cash transfers to vulnerable women who deliver in public or in a selected number of accredited private facilities is an important step in this direction.31 32 In addition to vouchers, other options such as contracting-out may be explored.33 34 The recent launch of National Health Protection Scheme in India—Prime Minister’s Jan Arogya Yojna or PMJAY—offers a huge opportunity to tap the potential of private sector for providing healthcare services (https://mera.pmjay.co.in/). A detailed review of such schemes is beyond the scope of the present article, but readers are referred to a recent publication-reviewed initiatives aimed at reaching equitable coverage in South Asia, with special attention to those involving the private sector.25 The impact of such initiatives must be closely monitored with an equity lens.
In parallel with efforts to increase access to providers, it is essential to invest in improving quality of care in both public and private sectors and build a responsive regulatory system; poor quality of care in low/middle-income countries is pervasive and has been hampering effects to reduce maternal, newborn and child mortality.35 The high rates of caesarean sections in the private sector in countries such as Bangladesh and India36 highlight the need for regulatory measures.
Training of public and private sector practitioners may also play a role, but it may be affected by turnover and by commercial interests, the latter by private providers. Our results on early initiation of breastfeeding coverage, which was substantially lower than coverage with institutional delivery, suggest the existence of missed opportunities that could be avoided by proper promotion. Health worker training, supportive supervision and innovative quality improvement approaches are necessary to ensure that children brought to facilities effectively get the recommended interventions. Such initiatives must be thoroughly evaluated not only in terms of their overall impact on coverage but also on equity.
Lastly, there is an urgent need to focus on newborn health, as deaths in the neonatal period are becoming more and more important in relative terms as postneonatal deaths are being reduced at a much faster rate than newborn deaths. The leading causes of newborn deaths in the region are prematurity, intrapartum deaths and sepsis.37 Our results included two indicators directly related to newborn health—postnatal visits38 and early initiation of breast feeding39—both of which systematically showed the lowest coverage in all country studies. To address the high mortality rate among newborns, UNICEF is currently promoting the uptake of these interventions in the South Asian region.8
Earlier analyses suggested that interventions delivered at community level by the public sector—such as immunisations or vitamin A supplementation—are more equitably distributed in the population than interventions that require contact with a health provider in a hospital or clinic.36 The present analyses are focused on the latter, more inequitable interventions. The main lessons arising learned are that the private sector is an important source of care in most countries, and that access to private services is more inequitable than access to public services, even when for-profit and not-for-profit private services are jointly analysed. Richer women and children are more likely to use both the private and the public sector in most countries, whereas urban–rural differences are not as marked. Family wealth is a driver of inequalities, and use of the private sector may be seen as a strategy used by the wealthy to achieve higher coverage in light of the limited availability or perceived lack of quality of public services. Yet, success in meeting UHC and the SDG goals for maternal, newborn and child mortality will be largely driven by the ability to reach the poorest women and children with high-quality interventions.
The public–private mix varies markedly by intervention, from country to country, and according to family wealth and residence. Effective programme and policies must be supported by regular monitoring of coverage with an equity lens. It is also likely that for large countries such as India and Pakistan, subnational patterns may vary, requiring efforts to be tailored to the local conditions.
From a whole-population perspective, one may argue that the ultimate goal is to reach universal coverage and that a combination of greater use of private providers by the wealthy and of public services by the poor would be acceptable. Our results, however, show that this is far from being the case in most South Asian countries, where substantial proportions of poor and rural women and children are not being reached by either sector.
The next step is to disseminate the present analyses to policy-makers in the region and to promote data-driven, country-specific policy discussions regarding on how to integrate the public and private sectors in the effort toward reaching high and equitable coverage.
References
Footnotes
Handling editor Sanni Yaya
Contributors SG, LC-A, CGV, PR and AJDB conceived the idea of manuscript. CGV, AJDB, FCW and LPV carried out data analysis with inputs from other researchers involved. CGV, FCW, GG, MZM, SG and LC-A drafted the first version of the manuscript. All authors provided inputs to the interpretation of findings and approved the final version of manuscript.
Funding The analyses were funded by the UNICEF Regional Office for South Asia. UNICEF staff members are included among the authors of the manuscript.
Disclaimer The results presented here are descriptive and do not reflect the results of any program or initiative being implemented by UNICEF.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available.