Article Text

Abstract
Introduction Maternity waiting homes (MWHs) link pregnant women to skilled birth attendance at health facilities. Research suggests that some MWH-facility birth interventions are more success at meeting the needs and expectations of their intended users than others. We aimed to develop theory regarding what resources work to support uptake and scale-up of MHW-facility birth interventions, how, for whom, in what contexts and why.
Methods A four-step realist review was conducted which included development of an initial programme theory; searches for evidence; selection, appraisal and extraction of data; and analysis and data synthesis.
Results A programme theory was developed from 106 secondary sources and 12 primary interviews with MWH implementers. The theory demonstrated that uptake and scale-up of the MWH-facility birth intervention depends on complex interactions between three adopter groups: health system stakeholders, community gatekeepers and pregnant women and their families. It describes relationships between 19 contexts, 11 mechanisms and 31 outcomes accross nine context-mechanism-outcome configurations (CMOCs) which were grouped into 3 themes: (1) Engaging stakeholders to develop, integrate, and sustain MWH-facility birth interventions, (2) Promoting and enabling MWH-facility birth utilisation and (3) Creating positive and memorable MWH-facility birth user experiences. Belief, trust, empowerment, health literacy and perceptions of safety, comfort and dignity were mechanisms that supported diffusion and adoption of the intervention within communities and health systems. Examples of resources provided by implementers to trigger mechanisms associated with each CMOC were identified.
Conclusions Implementers of MWHs cannot merely assume that communities will collectively value an MWH-facility birth experience over delivery at home. We posit that MWH-facility birth interventions become vulnerable to under-utilisation when implementers fail to: (1) remove barriers that hinder women’s access to MWH and (2) ensure that conditions and interactions experienced within the MWH and its affiliated health facility support women to feel treated with compassion, dignity and respect.
PROSPERO registration number CRD42020173595.
- Maternal health
- Other study design
- Prevention strategies
- Obstetrics
- Health services research
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Previous reviews have focused on determining maternity waiting home (MWH) effectiveness and assessing user experiences and perceptions of accessibility and feasibility. These reviews did not provide explanations of why the MWH intervention has been successfully taken up and scaled up in some contexts and not in others.
WHAT THIS STUDY ADDS
This article presents a realist programme theory explaining relationships between contexts and mechanisms associated with a greater likelihood of successful MWH adoption by health systems, communities, and women and families in low-income and middle-income countries.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The theories provide transferable lessons that can enhance our ongoing capacity to optimise implementation of MWH-facility birth interventions. They constitute a theoretical foundation on which the contributions of new knowledge on MWH interventions can be understood and applied.
Introduction
Ninety-five per cent of all pregnancy-related deaths occur in low-income and middle-income countries (LMICs).1 Most maternal and neonatal deaths, morbidity and disability are preventable when women have timely access to skilled obstetric care before, during and after childbirth.2 3 Maternity waiting homes (MWHs) are intended to help women and families to overcome delays in reaching care. An MWH is defined as any structure located within or near a health facility that provides (at least) antenatal accommodation for pregnant women and exists to enable women to access (a) skilled health professional(s) during childbirth or earlier if complications arise.3 During their MWH stay, women may also receive education, counselling, and other programming.4 A preliminary conceptual model linking MWHs to maternal and newborn health has been proposed.5
The MWH is a complex intervention and there is no standardised model.4 MWHs vary in size, location in relation to the affiliated facility, included services and amenities, and eligibility criteria for use.3 6 They are established and implemented by government, non-governmental organisations and/or community groups or by partnerships involving these three entities.3 6 The MWH intervention is not a stand-alone intervention, but rather, it links pregnant women to skilled birth attendance at a health facility, a key component of the continuum of care for maternal, neonatal and child health. We use the term ‘MWH-facility birth experience’ to denote the intervention because the quality of both MWH and facility birth services determines the extent to which reductions in maternal and neonatal morbidity and mortality (MNMM) are achieved.5
While recent systematic reviews and meta-analyses report limited, mixed and inconclusive evidence regarding MWH effectiveness,5 7 8 individual studies have associated the MWH-facility birth intervention with increased odds of facility birth9–11; decreased maternal and perinatal mortality12 13; reduced risk of low birth weight14; and increased odds of attendance at all recommended postnatal visits within 6 weeks of birth.15 The intervention remains under-utilised in LMICs,16 which suggests a mismatch between one or more aspects of the implemented MWH-facility birth model and the capacities, expectations, experiences, needs and preferences of its intended beneficiaries. Facilitators and barriers to utilisation include the community’s willingness to participate in implementation17–35; pregnant women and their family’s expectations and preferences in relation to the built environment of an MWH-facility birth model9 16 17 19 30 31 36–50; and their receptivity to the intervention based on the reputation of health service quality.51 The mismatch also suggests that some implementation techniques and contextual adaptations have been more successful than others.
There is a dearth of theory explaining how and why the MWH-facility birth intervention is adopted by health systems, communities and used by women and families in LMICs.5 This gap limits our ongoing capacity to optimise implementation of MWH-facility birth interventions. Developing theories regarding how, why and when this intervention works can support efforts to enhance uptake and scale-up.52 While context and theory have been generally under-recognised in implementation research, they can facilitate examination of implementation problems by drawing on different perspectives, and support optimisation of complex interventions implemented across varied contexts and which may be associated with varied, and potentially inconsistent, outcomes.53–66 The present realist review aimed to develop a programme theory (PT) regarding which MWH-facility birth intervention resources work to support uptake and scale-up of the MWH intervention, how, for whom, in what contexts and why. The guiding research questions were: (1) Which mechanisms support successful uptake and scale-up of MWH services; (2) Which contexts support, or potentially hinder, these mechanisms and (3) Which outcomes are triggered by these mechanisms?
Methods
This study employed a four-step realist review. A realist review is a type of narrative evidence synthesis that focuses on interpretation, critique and deepening understanding of a complex intervention or programme.53 57 67 Realist reviews seek to develop a transferable PT regarding when an intervention or programme is more or less likely to be successful.55 68 A PT expresses generative causation, comprised of statements that link context, mechanism and outcome configurations (CMOCs).4 53 56 69 Context refers to characteristics of systems, settings and individuals that shape how individuals interpret, perceive or respond to an intervention or programme. Mechanisms are context-dependent shifts in reasoning or responses to the resources embedded in an intervention or programme.53 55 58 67 70–72 Outcomes are triggered by explicit or yet to be identified mechanisms. Outcomes are, therefore, the result of an interaction between contexts and mechanisms, and they can involve intended or unintended consequences. Outcomes can be proximal or distal.70 73
Our review timeline was September 2020 to March 2022. We followed a four-step process: (1) development of an initial PT (IPT), (2) search for evidence, (3) selection, appraisal and extraction of data and (4) data analysis and synthesis.4 55 Our reporting is informed by the RAMESES publication standards.74 Consistent with realist review methodology,68 members of an advisory group provided input and feedback at different stages of our review. Our advisory group included MWH implementers who are affiliated with the Mozambique-Canada Maternal Health project (https://www.maternalhealthmozcan.ca/), researchers affiliated with the Maternal Waiting Home Alliance (https://www.maternitywaitinghomes.org/), representatives from the WHO, plus two experienced realist researchers. A glossary list of realist and maternal health terms used within this review can be found in online supplemental appendix A. Aligned to the iterative nature of realist reviews, findings from each stage of the stepwise process informed the methods and tools of the subsequent steps, as reported below.
Supplemental material
Development of an IPT
An IPT is a preliminary attempt to theoretically illuminate the intervention or programme under examination.67 69 74 As this realist review is part of a suite of three reviews aimed at better understanding the effectiveness, acceptability, feasibility and successful implementation of MWH-facility birth interventions,4 our IPT was based on emerging themes and insights generated by a preceding review.5 We also augmented our IPT based on the experiences of several members of the study team. Our IPT involved 31, if-then statements that hypothesised CMOCs across 6 themes (see online supplemental appendix B).
Search for evidence
Thirteen electronic bibliographic, abstract and citation databases were searched for peer-reviewed and grey literature information sources (AMED, CINAHL, Cochrane Library-Pregnancy and Childbirth, EMBASE, Global Health, Google Scholar, LILACS, MASCOT/WOTRO, OVID Medline, ProQuest Dissertations and Theses Global, PsycINFO, PubMed and Web of Science). Information sources dated no earlier than 1990 were sought and search terms included English, Spanish, Portuguese and French phrasing.4 Non-English documents were also requested of colleagues from the Pan American Health Organization. Hand searches of reference lists identified were also performed. The final search was run on 20 July 2020. A more detailed description of the search process and syntax is described within our review protocol.4
Selection, appraisal and extraction of data
Eppi-Reviewer V.4. was used to deduplicate, collate and screen records. Foreign language abstracts were translated to English using Microsoft Translate and DeepL Pro. Two team members (DM and NB) independently screened each record by their title and abstract. Raters demonstrated a high level of agreement during screening (Cohen’s simple estimate of inter-rater reliability, observed kappa=0.94 (0.62 SE), 95% CI (0.82 to 1.00), N=33, one abstract was discussed to reach a decision).
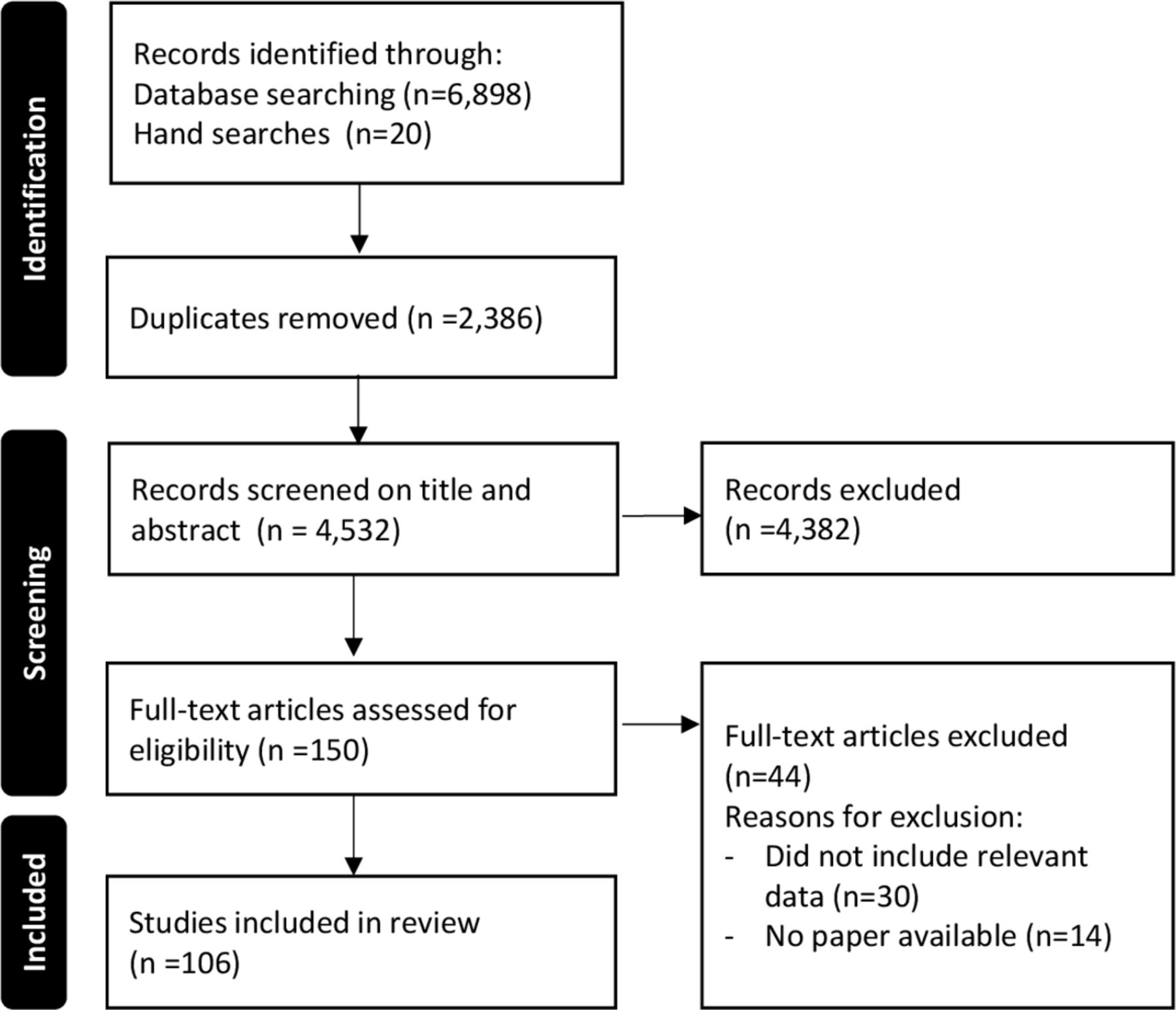
The full texts of selected items were then appraised with Pawson’s criteria of rigour and relevance.55 One hundred and six secondary sources were retained after title and abstract screening and quality appraisal of the initial 4532 secondary sources (Preferred Reporting Items for Systematic Reviews and Meta-Analyses diagram,75 76 figure 1). The majority of these 106 articles were peer-reviewed literature (n=96, 90.6%). Included studies involved qualitative, quantitative or mixed-methods design (see online supplemental appendix C). Sixty-six sources involved one or more countries in Africa (62.3%),9–15 23 25 28–32 34 36 37 39 42–47 49 77–119 25 involved 1 or more countries in South America (23.6%)8 18 19 21 22 24 26 33 35 40 41 48 50 51 81 120–129 and 7 involved one or more countries from Asia (6.6%).38 130–135 Eight sources involved multiple continents (7.5%).16 17 20 136–140

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) diagram.
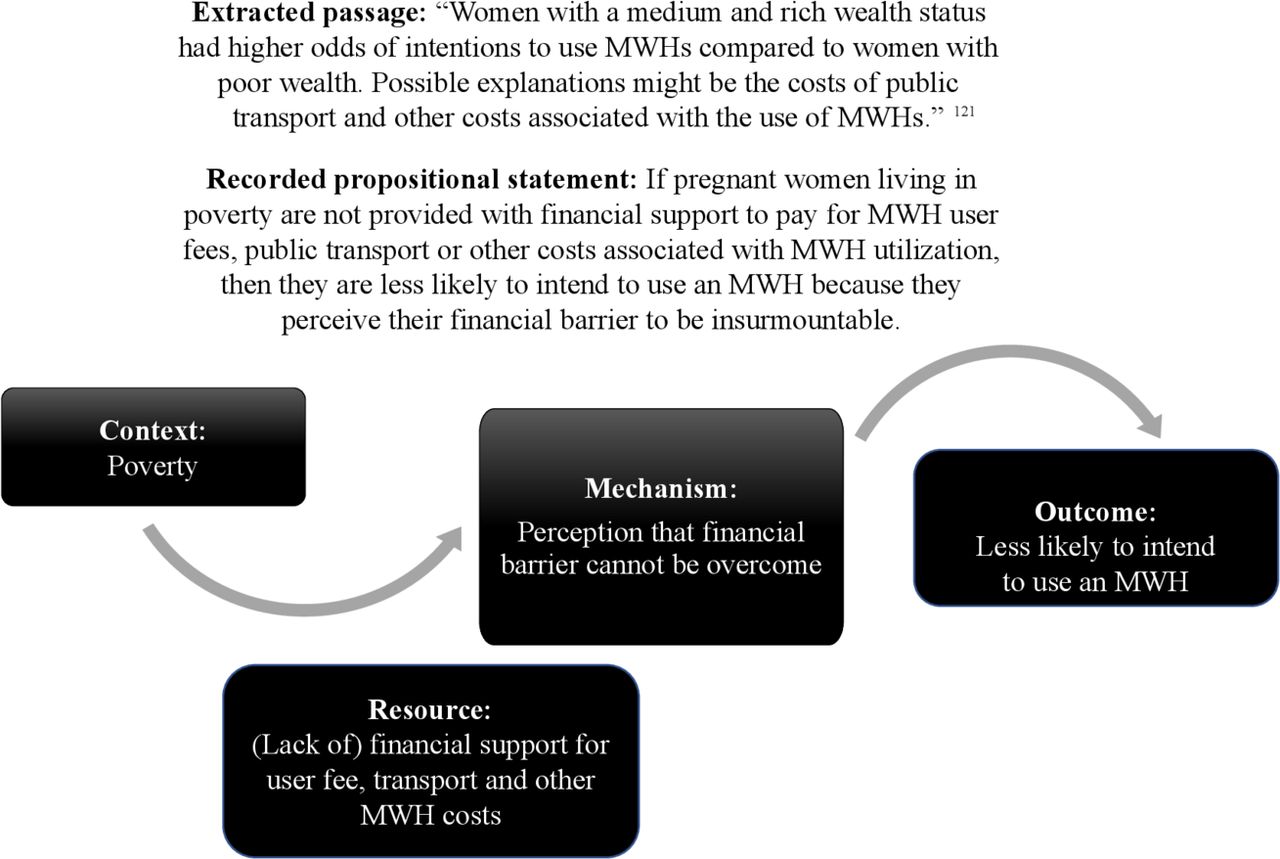
We created an electronic worksheet in Eppi-Reviewer V.4. to capture data extractions from eligible sources. Each eligible source was read line-by-line by one of four members of the team (DM, EZ, IV-U, NSU) who worked collaboratively as analysts. The team of analysts extracted 439 passages of qualitative and quantitative evidence from secondary sources including descriptions of MWH-facility birth intervention design and implementation; user, implementer and provider perspectives; and outcome analyses. As exemplified in figure 2, we used retroductive reasoning to develop CMOCs which identified context(s), resource(s), mechanism(s), and outcome(s) for each extraction.

Data extraction example.
Data analysis and synthesis
As data extraction from secondary sources progressed, the team of analysts repeatedly reviewed and discussed their data extractions and refined the IPT. The refined IPT was then discussed with 12 experienced MWH-facility birth intervention implementers during individual, online, semistructured interviews (see interview guide in online supplemental appendix D). Interviews were conducted from January to February 2021. Implementers were recruited using snowball sampling technique starting with contacts made through existing MWH-facility birth projects that were led by or involved a member of the research team. During their interviews, implementers drew on their MWH-facility birth experiences in Ethiopia (n=2), Liberia (n=1), Mozambique (n=3), Zambia (n=5) and Zimbabwe (n=1). Interviews were recorded with Microsoft Teams (V.1.4.00.16567) with supplemental field notes recorded by hand by a member of the analyst team. Non-English interviews were conducted with the support of a translator. Mean interview time was 72 min (22 min SD). Audiorecordings were transcribed verbatim into electronic files with the use of Sonix.ai, an online transcription service.
Analysis and synthesis of primary interview data followed the same process we used for secondary sources. Further refinements were made to the IPT based on 104 data extractions from the interview transcripts. The refinement process involved integrating similar, individual if-then statements to refine the IPT into a more evidence-based PT consisting of CMOCs phrased as ‘if-then-because’ propositional statements.141 142 The refinement process ended once the analyst team determined that any additional re-examination of our data was unlikely to result in major modifications to our refined PT. At this point, we perceived that theoretical saturation had been reached.54 55 Figure 3 provides an overview of the PT refinement process. We identified two substantive theories, diffusion of innovation143–146 and social convention,147 to support further distillation of our findings.148 These theories have previously been applied in LMIC settings.147 149 150
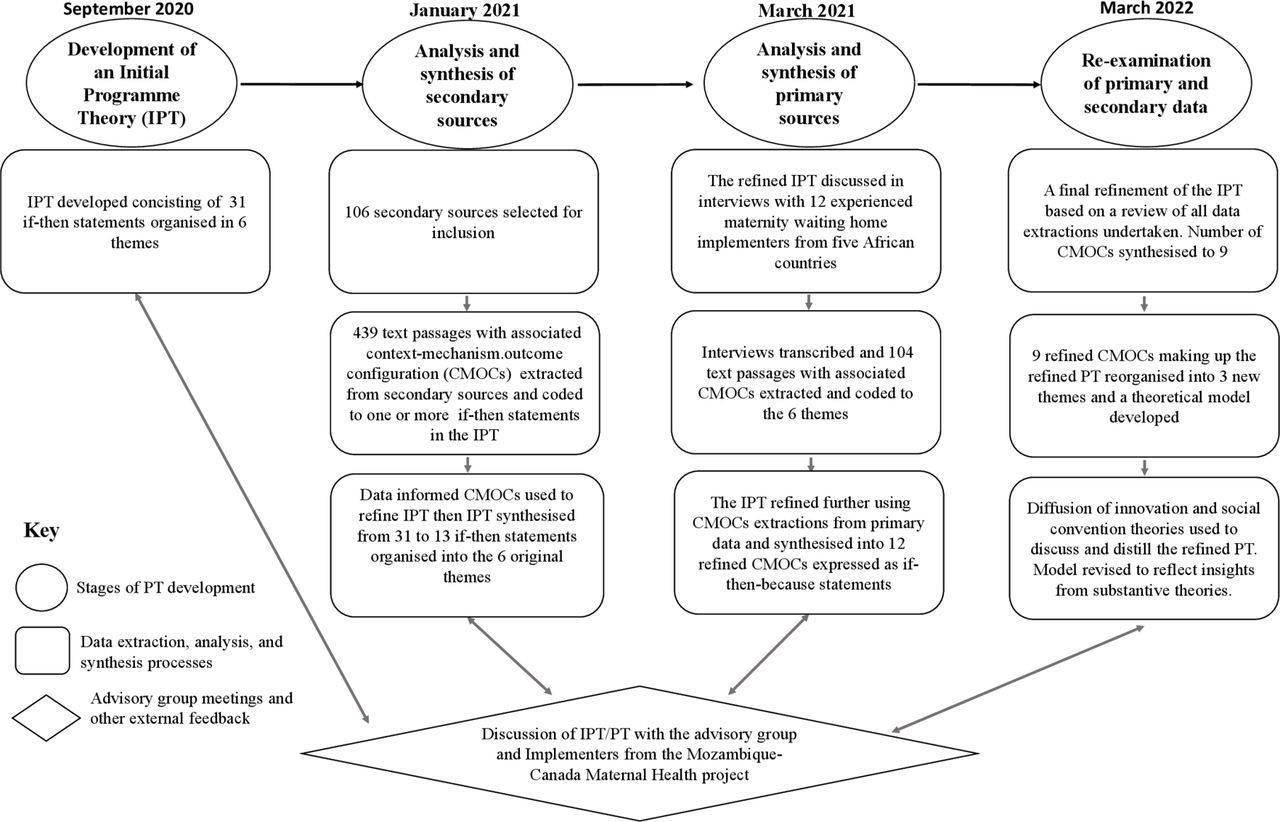
Programme theory (PT) refinement process.
Patient and public involvement
We had initially planned to involve women with experiences of using an MWH in Mozambique and Ethiopia in the design and conduct of the review.4 However, we experienced practical challenges pertaining to recruiting, preparing and supervising women to take on the role during the COVID-19 pandemic. We decided to implement our patient and public involvement plan during a follow-up realist evaluation which is currently at the protocol development stage. The evaluation aims to test our PT in the Mozambican context.
Results
Refined PT
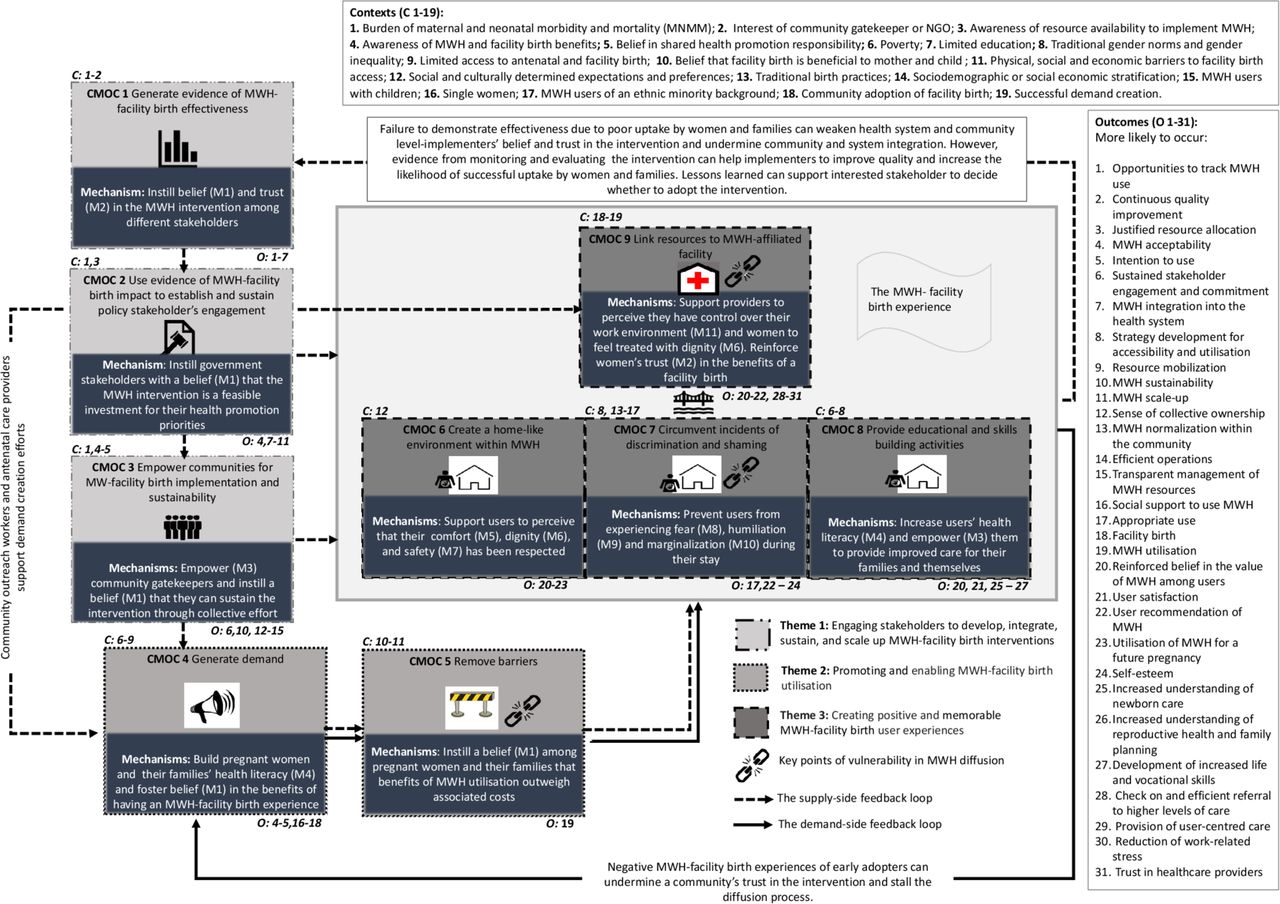
Our findings involve a programme theory presenting relationships between 19 contexts, 11 mechanisms and 31 outcomes. The following sections provide narrative descriptions of the PT which has been grouped into three themes: (1) Engaging stakeholders to develop, integrate and sustain MWH-facility birth interventions, (2) Promoting and enabling MWH-facility birth utilisation and (3) Creating positive and memorable MWH-facility birth user experiences. Box 1 outlines the PT's themes and their associated CMOCs. The online supplemental appendix E details the PT, including its associated IPT statements (CMOCs) and sources of evidence. This online supplemental appendix also provides examples of resources. Figure 4 illustrates a theoretical model and schematic overview of our refined PT. The model represents two feedback loops for supply and demand aspects of the intervention. On the supply-side, evidence of the MWH-facility birth interventions’ success elsewhere influences the adoption of the intervention by implementers in a new country and/or community context (CMOCs 1–3). Stakeholders then adapt the intervention to their context and initiate its implementation. Implementation involves devising and delivering approaches to promoting and enabling utilisation (CMOCs 4–5) and providing positive and memorable user experiences (CMOCs 6–9) that are appropriate for their context. The model suggests that the sustainability of an MWH-facility birth intervention beyond its first implementation circle is dependent on the extent to which the outcomes and impact it delivers reinforce implementation stakeholders’ belief and trust in its effectiveness, feasibility and potential to benefit their country/community. The immediate measure of success is uptake of the intervention by pregnant women and their families. The degree of success determines the extent to which stakeholders remain motivated to provide practical, social, financial and political support for continued quality improvement, including system and/or community integration and scale-up. On the demand-side, users play a critical role in demand creation by sharing their experience of the MWH-facility birth environment within their social network. The CMOCs are not ordered by their relative importance, but according to the process of the MWH-facility birth implementation circle as apparent from the reviewed sources of evidence, as described above.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
An illustrative theoretical model of MWH (maternity waiting home)-facility birth uptake and scale-up within low and middle-income countries.
Refined programme theory of maternity waiting home-facility birth interventions
Theories and examples of resources (or a lack thereof).
Theme 1: Engaging stakeholders to develop, integrate, sustain and scale-up maternity waiting home (MWH)-facility birth interventions.
Context-mechanism-outcome configuration (CMOC)1: Generating evidence of MWH-facility birth intervention effectiveness.
If a community is burdened by maternal and neonatal morbidity (C1) and an MWH has been proposed or introduced by government stakeholders, community gatekeepers or an non-governmental organisation(s) (NGO(s)) (C2) and a system of routine data collection is introduced during its formative implementation phase and is continued through the life cycle of the intervention (R1), and findings are disseminated to stakeholders including community members, health workers and relevant government ministries, departments, agencies (MDAs) (R2) then it is more likely that opportunities for tracking MWH-driven facility birth utilisation will increase (O1), continuous quality improvement of MWH services will increase (O2), resource allocation is more likely to be justified (O3), community members are more likely to accept the MWH (O4) and intend to use it (O5), stakeholder engagement and commitment are more likely to be sustained (O6) and MWH integration into the healthcare system including scale-up is more likely (O7) because the community believes that the intervention is responsive to their needs and preferences (M1), and MDAs continue to trust that the intervention is effective (M2).
CMOC2: Galvanising government buy-in for MWH-facility birth implementation and sustainability
If policy stakeholders from relevant government MDAs in a country that is committed to reducing their burden of maternal and neonatal morbidity and mortality (MNMM) (C1) are aware of resource availability within the system, from an external donor and/or the targeted community to implement the intervention (C3) and they become aware of evidence that an MWH intervention has reduced MNMM in a community within their country or in other settings (R3), then it is more likely that those MDAs will approve (O4) and integrate (O7) this intervention into existing maternal and neonatal health policy, will be more likely to develop a strategy regarding the accessibility, delivery and use of MWHs for affected communities (O8), a government may be more likely to mobilise MWH implementation resources (O9), MWHs are more likely to be sustained (O10) and scale-up of the MWH intervention in a country is more likely (O11) because MDAs believe the MWH is a feasible investment supporting their maternal health promotion priorities (M1).
CMOC3: Empowering communities for MWH-facility birth implementation and sustainability
If a community burdened with maternal and neonatal morbidity and mortality (MNMM) (C1) has members, including individuals who hold gate-keeping power, who are aware of the benefits of MWH and facility birth (C4) and believe they share responsibility for health promotion (C5), and are motivated to mobilise resources towards MWH implementation [with or without support of a government or an NGO(s)] (R4), then the community is more likely to share a sense of collective ownership of the MWH (O12), the MWH is more likely to become normalised within the community (O13), and the MWH is more likely to be operationally sustainable (O10) because community members are empowered to sustain the intervention (M3).
If stakeholders establish a management and/or governance committee(s) to oversee daily operation and/or resource management (R5), then daily operation of the MWH is more likely to become efficient (O14), management of MWH resources is more likely to become transparent (O15) and community engagement is more likely to be sustained (O6), because the stakeholders believe that collective management and governance are important for successful implementation (M1).
Theme 2: Promoting and enabling MWH-facility birth utilisation
CMOC4: Generating demand for MWH
If women and their families who live in poverty (C6) may have limited education (C7) or live within communities that are characterised by traditional gender norms and gender inequality (C8) and have limited accessibility or utilisation of antenatal care and facility births (C9) receive information and education regarding the purpose, importance, benefits and means of accessibility of antenatal care, MWH and facility birth from trusted sources (R6), then families are more likely to approve (O4) and support (O16) women’s utilisation of MWHs, women are more likely to intend to use an MWH (O5), use it appropriately (O17) and have a facility birth (O18) because women and families developed increased health literacy regarding MWH and facility births (M4) and believe in the benefits of using an MWH (M1)
CMOC5: The need to remove roadblocks to MWH-facility birth use
If women and their families believe a facility birth will be beneficial for mother and child (C10) but physical, social or financial barriers exist to their utilisation (C11) that have not been addressed by the MWH (R7), then women are less likely to use an MWH (O19) because they believe that these barriers outweigh the benefits (M1).
Theme 3: Creating positive and memorable MWH-facility birth user experiences
CMOC6: Creating a home-like environment within an MWH
If MWH users and their families have economically, culturally or socially determined expectations and preferences (C12) and the MWH and affiliated health facility are able to match these expectations and preferences (R8) then users’ perceptions of the value of services are more likely to be reinforced (O20), users are more likely to be satisfied (O21), users are more likely to recommend services to others (O22) and use MWH services for a future pregnancy (O23) because users perceive the MWH and affiliated health facility respected their comfort (M5), dignity (M6), and safety (M7).
CMOC7: Circumventing incidents of discrimination and shaming in MWH
If an MWH services a community characterised by traditional gender norms (C8) or traditional birth practices (C13), sociodemographic or socioeconomic stratification (C14) and the MWH does not provide an environment that minimises social comparison among users (R9), then users with children (C15), single women (C16), users of an ethnic minority (C17), or users from the poorest households (C6) are more likely to experience lowered self-esteem (O24), or are less likely to stay at MWH for an appropriate duration (O17), or are less likely to use MWH again for a future pregnancy (O23), or are less likely to recommend MWH to others (O22) because they feel afraid (M8,), humiliated (M9) or marginalised (M10) during their MWH-facility birth experience.
CMOC8: Empowering MWH users through education and skills building
If users have limited education (C7) or are living in a community characterised by traditional gender norms (C8) or are living in poverty (C6), and they are given sexual reproductive maternal and neonatal health education or other skills programming (R10), then it is more likely that they can develop greater understanding of newborn care (O25), or reproductive health and family planning (O26), or have developed increased life and vocational skills (O27). Users’ perceptions of the value of MWH-related services is more likely to be positively reinforced (O20) or MWH user satisfaction increases (O21) because they have developed increased health literacy (M4,) or are empowered to provide better care for their families and themselves (M3).
CMOC9: Linking human and material resources to MWH and MWH affiliated facility
If demand creation is successful for an MWH (C17), but its affiliated health facility has limited human and material resources and MWH implementers do not provide supporting clinical staff to the health facility (R11) and ensure availability of essential obstetric equipment and drugs (R12), then providers may be less likely to check on and efficiently refer MWH users to higher levels of care (O28), are more likely to experience difficulty providing woman-centred, humanised care to their MWH patients (O29), are more likely to experience work-related stress (O30) because these providers perceive they are overburdened and have less control over their work environment (M11). Pregnant women who are patients of these providers are less likely to be satisfied with their facility birth experience (O19), are less likely to recommend an MWH-facility birth experience to members of their community (O20), and they are less likely to trust health provider(s) (O31), because they feel they received undignified care (M6). They do not trust that MWH usage is beneficial (M2).
●(C1-19), contexts; (R1-11), resources; (O1-31), outcomes; (M1-11), mechanisms. Online supplemental appendixes E contains full lists of contributing initial PTs, sources and examples of resources used to trigger mechanisms associated with each PT.
Theme 1: engaging stakeholders to develop, integrate, sustain and scale-up MWH-facility birth interventions
CMOC1: generating evidence of MWH-facility birth intervention effectiveness
Ten articles and six interviews contributed to CMOC1, which illuminated the importance of data generation and reporting in relation to MWH-facility birth uptake and scale-up. Engagement of community members and government stakeholders was likely to be sustained within a given implementation context when routine data regarding MWH-facility birth utilisation, associated birth outcomes, service provision quality and community, and user experiences were regularly collected and shared with stakeholders.20 26 49 81 84 86 Implementers collected data and used it to inform contextual adaptation of the intervention at its inception or continuous quality improvement during its implementation.21 81 Through this approach, implementers cultivated stakeholders’ belief that the intervention was responsive to their needs, preferences, and priorities.99 Continuous data-driven engagement with community members was likely to increase their acceptability of the MWH-facility birth intervention and their intention to support its implementation and use. Maintaining dialogues with national and district level policy stakeholders around performance and impact appeared to sustain their belief in the intervention, which increased the likelihood of these stakeholders’ continued willingness to work towards integration of the intervention into the health system.24 34
CMOC2: galvanising government buy-in for MWH-facility birth implementation and sustainability
Eighteen secondary sources and 10 interviews contributed to CMOC2, which illuminated the relationship between evidence and government stakeholders’ engagement in implementation.
To champion implementation of the MWH-facility birth intervention, government stakeholders needed to believe in the intervention’s potential to contribute to achieving health promotion priorities and commitments to reducing MNMM. This belief was fostered by evidence of the interventions’ success within a setting in the country or from another country.20 21 26 27 30 33 41 80 84 85 101 117 120 121 127 151 Government stakeholders were more likely to support implementation if they had confidence in the intervention’s feasibility. These stakeholders’ commitment was fostered by the availability of resources and technical expertise to implement the intervention within relevant ministries, departments and agencies (MDAs), or through external donor support. Champions were likely to contribute to the mobilisation of resources for MWH implementation (online supplemental appendix E provides examples of resources).41 120 121 Belief in the intervention, especially where it produced local impact, appeared to motivate policymakers to embed the MWH-facility birth intervention into existing health policies and strategies, which in turn, facilitated the integration of the intervention within the healthcare system.20 26 27 30 51 80 84 85 101 151
CMOC3: empowering communities for MWH-facility birth implementation and sustainability
Twenty-one secondary sources and nine interviews contributed to CMOC3 which demonstrated the importance of involving community members in the implementation of an MWH-facility birth intervention.17–27 i Community gatekeepers who believed that the MWH-facility birth intervention aligned with their community’s existing sense of shared responsibility for health promotion were more likely to support the intervention.33 These gatekeepers mobilised resources to establish an MWH close to a health facility, contributed to the management of an MWH intervention, provided oversight and helped generate demand. Implementers established management and governance committees with representation from community members and health facility staff. The committees were more likely to be successful in contexts where members had clear implementation guidelines, and were trained and given the technical and financial capacity to manage, maintain, lead and sustain the intervention.21 23 26 29–31 34 101 102
Theme 2: promoting and enabling MWH-facility birth utilisation
CMOC4: generating demand for MWH-facility birth
Forty-seven secondary sources and 10 interviews informed CMOC4 which associated the intention to have a facility birth with women and families’ understanding of its purpose, importance and benefits for mothers and babies. Context-sensitive health literacy promoting activities were delivered to create awareness and catalyse interest in MWH-facility birth experiences. These activities were delivered in two settings: (1) during antenatal service consultations and (2) in communities. Women at risk of complications and/or who lived a long distance from a birth facility were more likely to be motivated to choose an MWH-facility birth if they received information about their personal risk followed by a recommendation from an antenatal health provider.13 16 17 19 27 30 31 42 44 49 84 92 94 97 103 105 106 111 114–116 118 119 132 134 152 Women who received antenatal care were also more likely to have familiarised themselves with the clinical environment, which increased their self-efficacy in using an MWH and giving birth at an affiliated health facility.119 125 Health facility-affiliated outreach workers visited remote communities whose members had limited access to education and a poor antenatal care and facility birth uptake.29 90 97 152 They conducted education sessions regarding MWH-facility birth during community gatherings.29 107 Outreach workers also engaged influential and trusted members of communities including former traditional birth attendants, tribal leaders and local groups such as a Saving Mothers Action Group to support pregnant women to overcome health literacy related barriers to MWH utilisation.16 17 20 23 26 29 35 78 90 93 107 111 112 115 124 125 134 137 139 152 Conditions of crowding occurred as an unintended consequence where demand exceeded capacity.23 29 87 90 151 152 Improved health literacy supported families to believe in the benefits of an MWH-facility birth experience which, in turn, increased their motivation to intend to have an MWH-facility birth experience.31 83 84 97–99
CMOC5: the need to remove barriers to MWH-facility birth
Thirty-one secondary sources and six interviews informed CMOC5 which relates to families’ ability to overcome barriers impeding their access to MWH-facility birth services. Women and/or families were more likely to have an MWH-birth facility experience if they were able to afford associated costs, such as travel including over long distances or by private vehicle, MWH-facility birth user fees (where applicable) or food and other required supplies.14 91 95 102 104 113 119 125 133 There were instances were women and families reduced their barriers to utilisation by selling assets, borrowing money or incurring debt from the health facility.92 96 114 119 Women and families who were unable to find a way to afford required expenses were not able to have an MWH-facility birth experience.103 108 131 Examples of resources or a lack of resources to remove financial and social barriers are reported in online supplemental appendix E.34 42 51 77 81 84 91 92 97 116 119 125 130 137
Theme 3: creating positive and memorable MWH-facility birth user experiences
CMOC6: creating home-like environments within MWH
Fifty-one secondary sources and eight interviews informed CMOC6 which illuminated optimal MWH environments supporting women and families to feel comfortable, safe and that their dignity was respected during their stay. Women and families had context-specific resource expectations and preferences regarding safety, comfort, and dignified treatment.9 11 12 16 17 19 21 28–31 36–51 84 89 90 93 100 111 115 125 129 131 151 152 Users whose experiences at an MWH were better than those conditions experienced within their own home tended to extend their stay or wished they could have stayed longer.48 92 135 Satisfied users were more likely to utilise an MWH for a future pregnancy,29 85 and were more likely to recommend it to other members of their community.37 40 42 43 92 125 Where an MWH offered a resource, such as electricity, that was not available within women’s homes or their greater community, an MWH attracted unintended users, leading to crowding, and dissatisfaction among MWH users.39
CMOC7: circumventing incidents of discrimination and shaming in MWH
Seventeen secondary sources and five interviews informed CMOC7 which associated several contexts with women’s vulnerability of being discriminated against or shamed during their MWH-facility birth experience. For example, some women living in communities with traditionally-held beliefs regarding gender roles were criticised for being lazy or careless because they left their husbands and children behind to utilise an MWH.119 151 Moreover, women living in communities with limited utilisation of antenatal care and facility birth have been accused of being unfaithful to their husbands because they allowed a male health worker to perform a physical exam.20 23 131 Experiencing an incident of discrimination or shaming evoked negative feelings for women which lowered their self-esteem and made them reluctant to use an MWH for a future pregnancy. Women without previous MWH experience were less likely to use one if they had heard about another woman from her community who had been treated poorly by a staff member or a health provider associated with an MWH.51 93 Examples of resources or a lack of resources to prevent or circumvent incidents of discrimination and shaming are provided in online supplemental appendix E.
CMOC8: empowering MWH users through education and skills building
Twelve secondary sources and five interviews contributed to CMOC8 which illuminated the value of user education and training. Implementers emphasised that MWHs are a place of learning for women. Education and skill-building offered to MWH users included women’s and children’s health,12 17 18 26 41 79 81 88 121 4 10 11 well-being,10 11 73 and skills-related training.30 MWHs tailored their educational programming based on community feedback. Nurses, midwives and community volunteers delivered MWHs’ educational resources via individual counselling and group sessions. Educational sessions were delivered at an MWH or its associated health facility.15 18 41 79 MWH-associated education and training increased women’s health literacy, supported them to feel more independent of their male partners and resulted in women believing that they were worthy of receiving care.10 33 71 89 These perceptions, in turn, appeared to help women to make more informed health-related choices and to recover from painful physical or emotional experiences. Participating in an income-generating activity enabled women to accumulate some personal savings.15 18 41 79 Receiving education and/or training reinforced users’ beliefs in the benefits an MWH-facility birth experience.
CMOC9: linking human and material resources to MWH and its affiliated health facility
Twenty-seven secondary sources and four interviews contributed to CMOC9 which revealed that MWH were often implemented close to health facilities that grappled with human and material resource constraints. Providers were often poorly paid and worked in suboptimal clinical environments.19 51 88 138 Some sources reported that users perceived providers were drawn to the work by the prestige associated with the medical profession rather by their true desire to help others.35 51 140 These contextual constraints were likely to affect the quality of care provided by facility staff, especially when an MWH experienced increased levels of utilisation. While some implementers anticipated that linking an MWH to a birth facility would increase obstetric caseloads, it was believed that this would not place extra burden on the providers.87 Rather, it was believed that providers would be better able to anticipate caseloads and plan for care in advance.87 However, we posit that MWH-driven cases and the responsibility of checking up on women staying at an MWH are likely to exacerbate stress levels for providers working in resource-constrained facilities. Sources indicated that providers practising in these facilities experienced less control over their working environment. Consequently, these providers were less likely to monitor MWH users and efficiently refer users to higher levels of care. They were also less likely to treat pregnant women in a humanised, woman-centred manner. Users were less likely to feel treated with respect and dignity if they experienced verbal or physical abuse at the hands of providers.44 90 107 111 125 Furthermore, their trust in providers and in the benefits of MWH was less likely to be reinforced if they felt neglected by providers.18 39 43 84 114 Consequently, these women were less likely to want an MWH-facility birth experience for a future pregnancy and they were less likely to recommend the experience to other women in their social network.
Discussion
Our PT demonstrates that successful implementation of the MWH-facility birth intervention depends on diffusion of the intervention across three groups of adopters: individuals working within the health system including policy level actors and healthcare providers, members of communities including local gatekeepers, and pregnant women and their families. Rogers’ theory of diffusion describes how innovative ideas, objects and practices are adopted over time, and across individuals and social systems.143 144 Diffusion depends on ongoing communication intended to create awareness of the innovation among targeted individuals and to shape their perceptions so that they decide to make full use of the innovation.144 This communication involves both organised dissemination efforts and passive, opportunistic conversations.144–146
Diffusion occurs both within and between the set of adopter groups. Within each group, individuals’ willingness to adopt will vary, and therefore, it is not necessary to have the support of all members of an individual adopter group at the onset of implementation.146 Rather, a small group of early adopters within each group can be thought of as a critical mass who first decide to adopt the innovation. Ideally, a critical mass should include individuals who are perceived by others as being credible and worthy of respect and who can rally and maintain support for the innovation.153 154 This core group is recruited using organised dissemination, in turn, the critical mass recruits others through passive diffusion, until a large enough proportion of individuals is ready to adopt the innovation. Our PT illuminates mechanisms that enabled or hindered the process of diffusion of the MWH intervention to occur across critical masses at the health system and community levels.
Potential adopters consider whether the innovation is feasible, compatible with their priorities and values, and advantageous relative to what they are already doing to achieve the same goal(s).144–146 The second CMOC shows that belief in the relative advantage of the intervention is likely to be triggered among health system level stakeholders who recognise the fit between their country’s health policy priorities and the MWH intervention. They are then likely to become health system level champions who engage in two levels of dissemination. First, they may seek to further enhance system fit and feasibility by connecting with and advocating for the MWH intervention, and by appealing for support from external partners as well as individuals at the level of local government and targeted communities. Appeals for support may include financial, material and human resources. For example, antenatal care providers and community health workers may support efforts to cultivate awareness and intention to have an MWH-facility birth experience by building health literacy among women and their families. Second, health system level champions may advocate for codification of MWH into national health policies and strategies. These actions can help to legitimise the intervention to health providers and community level adopters. CMOC1 regarding the important role of routine data collection and generating evidence of effectiveness in supporting efforts to engage health system level stakeholders is consistent with literature regarding scaling up complex health interventions in both high and LMICs.149 150 155 Other important contextual determinants of successful scale-up include availability of data regarding cost-effectiveness, consensus among stakeholders regarding approaches to implementation and scale-up, and good leadership within MDAs (ie, leadership that relies on evidence-based rather than politically motivated decisions).144 Health system level stakeholders’ efforts to sustain innovations such as MWHs are likely to be constrained by inadequate resources in LMIC contexts.156
The third CMOC identifies two critical masses at the community level. First, gatekeepers who sense that the intervention fits with the community’s collective values and can provide relative advantage over home births, are likely to become MWH-birth facility champions. These gatekeepers can work to mould the design of an MWH to fit their community’s needs, preferences and expectations. Gatekeeper involvement will help to diffuse the intervention’s credibility within their community. Some community members are then likely to become empowered to also champion the intervention through volunteering their time and donating financial and material resources towards implementation. Community champions may support local demand creation efforts and lead income generating activities. These activities can be used to fund initiatives to alleviate local MWH utilisation barriers and may amplify community champions’ sense of empowerment to sustain the intervention. Community champions may also be empowered to retain oversight of implementation via their representation on MWH management and governance committees. We found that communities with a shared sense of responsibility for health promotion are more likely to be ready to implement the MWH-facility birth intervention. This finding is consistent with community psychology research showing that members of such communities are more willing to engage in collective action and resource mobilisation towards a collective good.157 158
Social convention theory underscores that health practices are social conventions. For the adoption of a new health practice to be successful, members of a community must undergo two processes of social change: collective abandonment of an existing health practice and collective adoption of the new practice that is meant to replace it.153 158 For the process to succeed, the new practice must be integrated into the routine practices and social norms of targeted user groups, which means that they must value the new practice more than the old.143 144 Given that the MWH is linked to an associated health facility, both of these environments need to be considered in the design and implementation of MWH interventions. The concerns of two critical masses, women and families, and the providers they encounter, need to be considered. We identified points of vulnerability that compromise the intervention’s potential to be taken up by these critical masses.
When women and families contemplate the relative advantage of having an MWH-facility birth experience in comparison to a home birth, they consider its potential short-term and long-term financial impacts. Other considerations include whether they can withstand disruption in their daily routines during the woman’s absence and how their community will perceive their involvement with MWH-facility birth services. These concerns can be related to the first-level and second-level delays associated with MWH-facility birth access.2 A point of vulnerability of the adoption-abandonment cycle occurs when implementers fail to deliver context-relevant solutions to women and families facing financial, geographic, social and other barriers to utilisation (CMOC5).150 This failure limits the number of women and families that believe that the cost of an MWH-facility birth experience and any associated negative impact will be outweighed by its benefits.
The women and families who first decide to have an MWH-facility experience constitute another critical mass at the community level. The tipping point of home birth abandonment in favour of MWH-facility birth within a community or group of communities is dependent on how this initial, critical mass of women and families perceive their MWH-facility birth experience. As the MWH-facility birth intervention has limited individual trialability,146 these personal recommendations from early adopters have persuasive power with other members of the community.
Context-mechanism-outcome configurations six to nine highlight that the intervention also becomes vulnerable when an MWH-facility birth environment fails to provide conditions that closely approximate those of a home based birth. Some sources reported incidents where women felt discriminated against, fearful, or humiliated during their stay at an MWH. These experiences were likely to damage their self-esteem and make them reluctant to use the intervention again. Consistent with wider obstetric care literature from LMICs,159–162 our review also illuminated incidents where pregnant women were treated in a disrespectful and abusive manner at the MWH-affiliated facility. Health providers have been shown to prioritise physical health above a woman’s emotional and psychological health and well-being.159 163 The intervention must prioritise women’s emotional health and well-being if they are to perceive its relative advantage.164 While some implementers anticipated MWHs would support obstetric providers to better manage their caseloads, our review found that health facilities affiliated with the intervention often lacked adequate human and material resources. Obstetric providers who practiced in these resource-constrained clinical environments struggled to meet the demands of increased obstetric patients. They were less likely to be able to efficiently refer MWH users to higher levels of care and less likely to treat pregnant women in a humanised, woman-centred manner. Obstetric providers within these facilities are unlikely to perceive that an MWH brings a relative advantage to their work. Consistent with Ezumah et al,165 our findings highlight that it is difficult to develop and sustain users’ trust within a resource-constrained environment. Some sources also reported that MWHs were overcrowded due to high demand,23 29 87 90 151 152 which was likely to make users uncomfortable and create unnecessary workload for obstetric providers. This problem can result from a failure by implementers to balance demand (CMOC4) and bed capacity (CMOC6), which can be accomplished by generating appropriate demand and/or ensuring that bed capacity is aligned with the expected demand.
When women discuss their MWH-facility birth experiences with members of their community, they will include recollection of any negative encounters with provider(s) and staff member(s). These first-hand reports are likely to then diffuse a negative perception of an MWH-facility birth intervention within the greater community. Poor reputation of the facility birth experience can undermine earlier efforts, commitments, trust and belief in the intervention. Diffusion of innovation theory views individuals who delay adoption as being problematic ‘laggards’.143 This perception fails to acknowledge that individuals’ resistance can be borne out of their dehumanising experience(s) with the intervention or learning that others have been subjected to such incidents.166 167 Only by seeking to understand the concerns of non-adopters can implementers design strategies for enhancing uptake.166 167
Strengths, limitations and future directions
Our review drew on a global corpus of evidence involving primary and secondary sources. Secondary sources included qualitative and quantitative research disseminated in peer-reviewed and grey literature. Our review was enriched through interviews with experienced MWH implementers in five African countries. Drawing on substantive theory allowed us to refine our understanding under the lenses of diffusion of innovation and social convention theories. Realist reviews are not intended to identify pathways to achieving all possible outcomes, nor can this methodology exhaustively explain all mechanisms that can generate changes. However, our PT provides a theoretical foundation on which the contributions of new knowledge can be understood and applied. Our review was not able to address all stakeholder questions. Future research should seek to deepen understanding regarding health system and community levels fit with the MWH-facility birth intervention. The human and material resources necessary for the provision of person-centred, humanised maternity care to MWH users during their MWH-facility birth experience requires further examination. The experiences of obstetric providers who practice within MWH-affiliated facilities also warrants attention. Exploration of the material and social conditions that can catalyse opportunities for social comparison and dehumanised care within an MWH and its affiliated health facility is also needed. Finally, there is a need for greater understanding of implementers’ reactions to incidents of dehumanising care that have occurred within MWH or affiliated health facility environments.
Conclusion
This review presents a PT regarding how, why, and in what contexts the MWH-facility birth intervention is more or less likely to be taken up and scaled up within health systems and communities in LMIC. These PT demonstrates that successful implementation of the MWH-facility birth intervention depends on successful diffusion of the intervention across three groups of adopters: individuals working within the health system including policy-level actors and healthcare providers, members of communities including local gatekeepers, and pregnant women and their families. We found that uptake and scale-up of the intervention is less likely to succeed in contexts where implementers fail to support women and families to overcome barriers to their MWH-facility birth utilisation and provide comfort, safety and dignified, humanised, or compassionate care during both women’s stay at an MWH and delivery at the affiliated health facility. Our findings highlight a need to assess intervention-system fit, particularly with regard to the targeted health system’s ability to provide adequate material and human resources to the MWH-affiliated health facility.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Our review received ethics approval from the Behavioural Research Ethics Board (Beh-REB) at the University of Saskatchewan (application ID 2393). Implementers gave informed consent to participate in the study before they were interviewed.
Acknowledgments
We gratefully acknowledge members of the advisory group including Anayda Portela, Denise Kouri, Jessie Forsyth, João Paulo Souza and Tami Waldron. We also extend sincere thanks to the 12 MWH implementers and policy makers who were interviewed during the PT refinement process, including, Abebe Mamo G/tsadik, Bwalya Misheck, Chipo Chimamise, Cristalina Mahumane, Esther Ngaru, Faith Akovi Cooper, Fernanda Andre, Gebeyehu Bulcha and Thandiwe Ngoma.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Seye Abimbola
Twitter @nadege_sandrine, @brynne.gilmore
Contributors NM conceptualised and conceived of the study and is the principal investigator of the Mozambique-Canada Maternal Health Project, which includes MWHs as an intervention component, and through which the funds for this study were procured. NM is responsible for the overall content as guarantor. DM and NSU contributed equally to the research. NM, DM, Tami Waldron, NB and Anayda Portela contributed to the conceptualisation of the study as acknowledged in the protocol.4 DM, NB contributed to literature search and title and abstract screening. DM, EZ, IV-U, NB and NSU contributed to quality screening and data extraction. DM, EZ, NSU and IV-U contributed to data analysis. EZ, IV-U and NSU drafted most of the manuscript. BG provided technical advice throughout the research process and assisted with write up. All authors contributed to substantive content revision and approved the final manuscript. Online supplemental appendix F contains our reflexivity statement with additional information on author contributions and positionality.
Funding This work was supported by Global Affairs Canada (project number D-002085) for the Mozambique-Canada Maternal Health Project, administered by the University of Saskatchewan.
Disclaimer The funder was not involved in any aspect of the research process.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.