Article Text

Abstract
Introduction Fatalistic cancer beliefs may contribute to delayed diagnosis and poor outcomes, including treatment abandonment, for children with cancer. This study explored Guatemalan parents’ cancer beliefs during initial paediatric cancer communication, and the sociocultural and contextual factors that influence these beliefs.
Methods Twenty families of children with cancer were included in this study. We audio-recorded psychosocial conversations with psychologists and diagnostic conversations with oncologists, then conducted semi-structured interviews with parents to explore the evolution of their cancer beliefs. Audio-recordings were transcribed and translated from Spanish into English, with additional review in both languages by bilingual team members. All 60 transcripts were thematically analysed using a priori and novel codes.
Results Guatemalan parents’ beliefs evolve as they learn about cancer through various sources. Sources of information external to the cancer centre, including prior experiences with cancer, media exposure, community discussion and clinical encounters, contribute to pre-existing beliefs. Many parents’ pre-existing cancer beliefs are fatalistic; some are influenced by Mayan spirituality. Sources internal to the cancer centre include psychologists and oncologists, other providers, other patients and families. Psychologists acknowledge pre-existing beliefs and deliver cancer education using verbal explanations and hand-drawings. Oncologists provide diagnostic information and outline treatment plans. Both support hope by providing a path toward cure. Parents’ lived experience is a culmination of sources and simultaneously independent. Ultimately most parents arrive at an understanding of cancer that is consistent with an allopathic medical model and offers optimism about outcomes.
Conclusion An interdisciplinary communication process that includes cancer education, is attentive to pre-existing beliefs, and supports hope may encourage acceptance of the allopathic medical model and need for treatment. Providers in settings of all resource levels may be able to use these techniques to support cross-cultural cancer communication, reduce treatment abandonment and improve therapy adherence.
- child health
- paediatrics
- cancer
- qualitative study
Data availability statement
Data are available upon request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Fatalistic cancer beliefs contribute to poor outcomes for children with cancer, particularly in low-income and middle-income countries where >90% of children diagnosed with cancer live.
Cancer beliefs may be shaped by various sources including personal experiences, community perspectives, spirituality and experiences with healthcare providers.
What are the new findings?
Some Guatemalan parents hold pre-existing cancer beliefs that are fatalistic, while others may be influenced by Mayan spirituality.
Interdisciplinary providers at a comprehensive cancer centre deliver cancer education and provide information regarding diagnoses and treatment in a manner that acknowledges pre-existing beliefs and supports hope.
Ultimately most parents arrive at an understanding of cancer that is consistent with an allopathic medical model and optimistic about outcomes.
What do the new findings imply?
An interdisciplinary communication process that is attentive to pre-existing beliefs and supports hope may encourage parents of children with cancer to accept the need for treatment.
Providers may be able to use these techniques to support cross-cultural cancer communication, reduce treatment abandonment and improve therapy adherence for families of children with cancer.
Introduction
Individuals with cancer often come to the diagnosis with pre-existing beliefs, including ideas about why it happened, how it can be treated and its expected outcomes. These beliefs can be shaped by many different forces, including personal experiences, spiritual beliefs and community perspectives on cancer. Unfortunately, hopelessness, pessimism, and deterministic thoughts around cancer are associated with delayed diagnoses1 and poorer outcomes.2 Negative cancer beliefs among marginalised populations contribute to disparities by decreasing early intervention.3 Indigenous people’s cancer beliefs have been identified as a barrier to seeking care,4 as well as to participation in cancer communication.5 Healthcare providers in low-income and middle-income countries (LMICs), where 90% of children with cancer live, have identified cancer beliefs, in addition to cost of therapy and distance to a cancer centre, as important factors in refusal and treatment abandonment.6 Treatment abandonment disproportionately affects children in LMICs7 and negatively impacts treatment outcomes. However, cancer beliefs of parents of children with cancer in LMICs have received limited attention in the medical literature. Understanding how beliefs are shaped through encounters with the medical system has potential to reduce treatment abandonment and improve outcomes for children with cancer.
The purpose of this study was to qualitatively explore the evolution of parents’ cancer related beliefs during initial paediatric cancer communication, including the sociocultural and contextual factors that influence these beliefs. This study was conducted in Guatemala, a small but diverse country, with 24 principal ethnic groups, speaking 24 distinct languages and making up 40% of the population.8 While Guatemala is a predominantly Christian country, aspects of traditional Mayan spirituality persist and have been incorporated into many Catholic and Evangelical practices.9 Childhood cancer providers in Guatemala have previously investigated socioeconomic factors affecting treatment abandonment and demonstrated the impact of an interdisciplinary communication intervention.10 This care model includes early involvement of psychosocial support to ensure attention to identified barriers to care, and consists of a two-step process integrating emotional support with basic cancer information. Within this clinical context, we audiotaped conversations at diagnosis between parents of children with cancer, psychologists and oncologists, in order to examine the ways in which parents and clinicians discussed the cancer diagnosis. We then interviewed parents about their current cancer beliefs as well as the evolution of their beliefs from before the child’s cancer diagnosis to the present. In keeping with work on the importance of understanding an individual’s explanatory model of illness,11 we hypothesised that a communication process that recognised pre-existing beliefs would support parents in accepting an allopathic, or biomedical, model and a need for treatment.
Methods
Setting and participants
This study was conducted at Unidad Nacional de Oncología Pediátrica (UNOP) in Guatemala City, Guatemala. Guatemala is an upper-middle income country with a childhood cancer survival rate of approximately 65%. UNOP, founded in 2000 and supported through a public–private partnership, is Guatemala’s national paediatric cancer centre. Approximately 500 new cases of childhood cancer are diagnosed at UNOP each year.
Participants eligible for the study included Spanish speaking parents of children (less than 18 years of age) with a new or probable diagnosis of any form of paediatric cancer. Parents were approached sequentially and offered participation in the study, with additional purposive sampling as necessary to include a range of paediatric ages and diagnoses, as well as parents representing diverse socioeconomic situations. Twenty families participated in all parts of the qualitative study at which point thematic saturation12 was reached and no further participants were enrolled. Twelve families were approached prior to saturation and declined participation in the study. Written informed consent was obtained for all parent and provider participants. This study was performed in compliance with international regulations for protection of human research subjects and approved by the respective oversight boards at St. Jude and UNOP.
Patient and public involvement
Neither patients, parents nor the public were involved in the design, conduct or reporting of this research. We plan to partner with parents as we disseminate these results and consider next steps for potential interventional work.
Study design and data collection
For each family, we audio-recorded psychosocial conversations with psychologists and diagnostic conversations with oncologists. As part of a standard intake process, parents of newly diagnosed patients at UNOP first meet with a social worker and then a psychologist who elicits intake information and provides initial cancer education. Approximately 1 to 5 days following this encounter, families meet with an oncologist who discusses the child’s diagnosis and outlines a treatment plan. The psychologist responsible for intake is always present for the subsequent diagnostic conversation with the oncologist. Children are not present for either conversation, as the practice at UNOP is to have the child meet separately with a child life specialist about their diagnosis. For this study, both conversations with parents were audio-recorded given the role of each conversation in education about the diagnosis, including one or both parents as available and any additional extended family or social support as requested. The recording device was activated by the psychologist and placed to side to enable conversations to occur naturally.
Semi-structured interviews were then conducted within 14 days of diagnosis with one parent per child who was present for both conversations. These interviews explored parents’ experiences and perspectives on the diagnostic process including the evolution of their cancer beliefs. The interview script (online supplemental file 1) was first developed in English, translated into Spanish and back-translated into English with iterative review by bilingual members of the study team. Audio-recorded interviews were conducted in Spanish by a Guatemalan psychologist who was trained in qualitative methods and not involved in initial intake conversations. Data collection occurred from April–August of 2019. All audio recordings were professionally transcribed and translated into English. Bilingual members of the research team reviewed texts and compared them with Spanish audio recordings to ensure translations adequately captured conversations. Caregiver quotations from conversations with providers are noted as such; all other quotations come from study interviews.
Supplemental material
Data analysis
We used thematic content analysis,13 including a combination of a priori and novel codes. A priori codes included codes used to identify the speaker and direction of speech in naturally occurring conversations, codes from the Roter Interaction Analysis Scale,14 as well as codes previously used to analyse patient participation in medical encounters.15 Novel codes included various sources of information (eg, ‘prior experiences with cancer’) and concepts including ‘Mayan spirituality’, a complex notion referring to the Mayan value system and way of living, as well as cosmological beliefs impacting a person’s health and well-being in relation to the equilibrium of the natural world. Two authors (DG and GF) iteratively read transcripts and identified codes based on recurrent themes. Codes were conceptually defined and refined through use on 12 transcripts. Two researchers (DG and GF) independently coded each transcript using the final codebook (online supplemental file 1) and MAXQDA software (VERBI, Berlin, Germany). Inter-rater reliability was calculated for each set of transcripts and ranged from 0.72 to 0.88. Consolidated Criteria for Reporting Qualitative Studies guidelines were followed to ensure rigour.16
Results
Twenty families were included in this study. Demographic information for included families is shown in table 1. The majority of included patients (80%) had haematological malignancies. There were about equal numbers of male and female patients, and the study included all age ranges. While fathers were present for over 50% of diagnostic conversations, more mothers were interviewed (65%).
Participant demographics n (%)
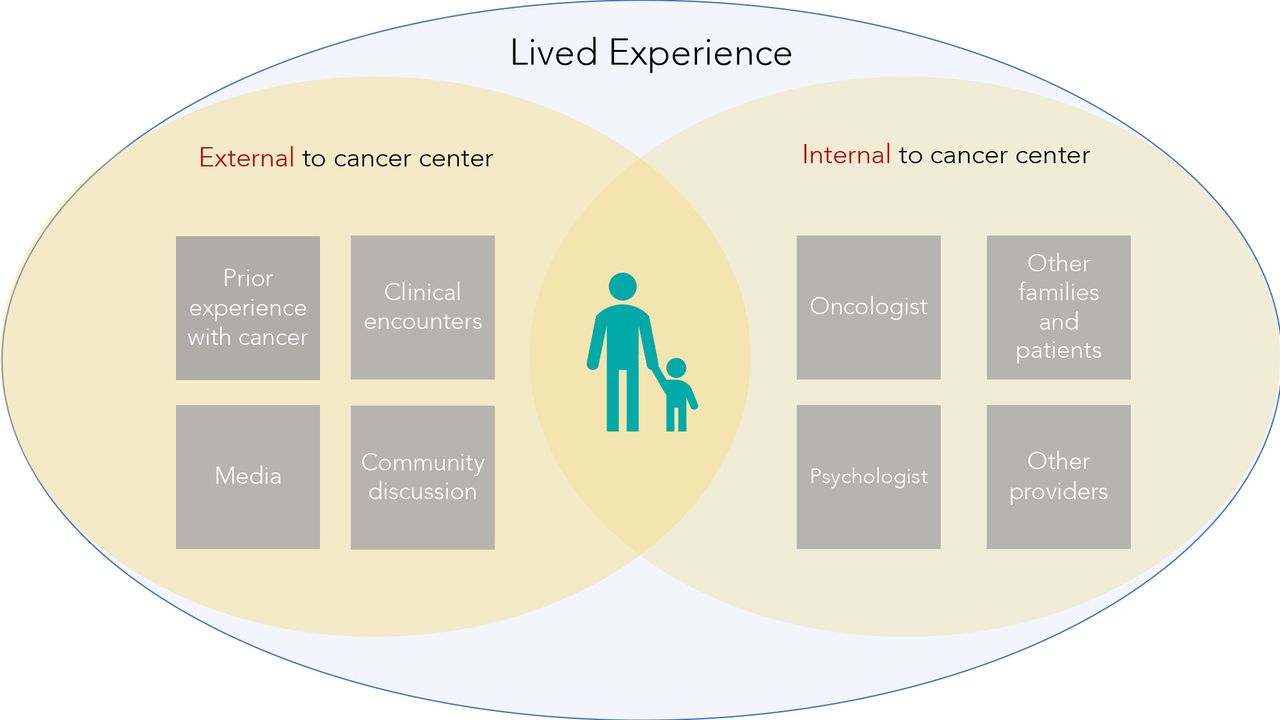
Families learnt about cancer through a variety of sources (figure 1). Some informants were external to the cancer centre, while others were within the cancer centre. External sources of information contributed to parents’ pre-existing beliefs, while sources internal to the cancer centre helped parents through the arc of their child’s diagnosis. All of these information sources influenced parents’ eventual understanding of cancer.

{kind=link}
Sources of information contributing to parents’ understanding of cancer. Guatemalan parents of children with cancer learn about their child’s diagnosis through a variety of sources. Some of these sources of information are external to the cancer centre, including prior experiences with cancer, media exposure, community discussion and clinical encounters prior to reaching Unidad Nacional de Oncología Pediátrica. Other sources of information are internal to the cancer centre and include the psychologist, oncologist, other providers and other patients and their families. A family’s lived experience is a unique source of information that is simultaneously a culmination of all other sources and contributes to the family’s ultimate understanding of cancer.
Pre-existing cancer beliefs
Information sources external to the cancer centre, including prior experiences with cancer and media exposure, contributed to beliefs parents held about cancer before their child’s diagnosis (table 2). Parents often first learnt about cancer through the experiences of family members or people in their community. Fundraising campaigns, news stories and advertisements, many produced by AYUVI (‘help me live’), the foundation supporting UNOP, also exposed families to childhood cancer.
Sources of information external to the cancer centre
For many families, previous experiences taught them cancer was incurable; “I heard about it; I saw a man who died of cancer” (provider conversation); “We got worried because in the news I’ve heard that once you have cancer you don’t have a good future”. Parents mentioned other hardships as well, including disfigurement and financial strains. There were fewer positive descriptions, however some parents did know of people who survived cancer: “I had a chance to see two old people that fought cancer and got cured” and others learnt about the potential for cure from the media. While informative, parents suggested that these sources were distant from their own experience “I don’t know where he was treated, I just met her once and she told me the story”; “When you are not living it, you don’t pay attention to it, I used to see commercials about cancer, but we never searched for information”.
Additional sources external to the cancer centre
After their child fell ill, but prior to arriving at the cancer centre, parents encountered additional sources of information that influenced their cancer beliefs. Community discussion was a powerful source of information for parents. As with prior experience and media exposure, parents received both discouraging and helpful information from their community. One parent said, “many people got me scared because they said for this there was no cure and no medicines” (provider conversation). Another explained how the community helped them reach UNOP: “a friend of my husband’s boss who is a doctor recommended this hospital… that’s how we brought him here”.
In this time of need, some families consulted religious leaders who recommended prayer, and others sought out traditional healers. Mayan spirituality influenced interactions within the community and contributed to parents’ pre-existing cancer beliefs. Specifically, parents discussed ‘the evil eye’ and ‘susto’, loosely translated as fear or surprise. Some parents discussed these beliefs generally but said they did not ‘believe in that stuff’. In other circumstances, belief in Mayan spirituality directly influenced care: “she was very down, so people started saying it was evil eye and susto, so we took her to the healer…they take some plants and rub her with them to cure the susto and the evil eye” (provider conversation); “One person told us he was suffering from fear…and she told us ‘let’s cure him before you get to the hospital’, so they bathed him, they did all the ritual required in cases like these” (provider conversation). In some instances, parents reported traditional healers cured their child of susto, and in others they did not: “we took her to a witchdoctor and at the end it didn’t work” (provider conversation).
With or without community support, most families had at least one clinical encounter prior to reaching UNOP. Some of these encounters were at hospitals; others were with traditional healers, “he started with a fever…so she took him to a healer…they rubbed his stomach” (provider conversation). While many families learnt of their child’s diagnosis prior to reaching UNOP, some did not. Of the families that were given diagnoses, not all were able to understand or absorb the information: “they told us everything, but I just can’t remember anything” (provider conversation). Similarly, not all providers capable of making the diagnoses were able to help: “He said, here we treat that, but we don’t have the specialty or the equipment” (provider conversation).
Information obtained at the cancer centre
Once at UNOP, parents continued to learn about cancer. Primary sources included the psychologist and the oncologist, however other providers including nurses, as well as other patient families, contributed to parents’ understanding of their child’s illness. Quotations from interviews with parents illustrate how they viewed interactions within the cancer centre and examples are included in table 3. Table 4 contains excerpts from parents along their journey through psychosocial and diagnostic conversations, with corresponding reflections during interviews.
Sources of information within the cancer centre
Interactions
Psychologist
Psychologists consistently started conversations with parents by introducing themselves and outlining a plan to discuss the sensitive subject of the child’s illness. Throughout the sessions psychologists provided reassurance, telling parents “you are not alone, we are a team”, and explained to parents they were not at fault. At times, parents cried or expressed strong emotions. During these moments, psychologists paused and comforted families. In addition, psychologists provided hope by explaining that cancer is treatable and curable: “nowadays we have treatment, there are possibilities for cure”. Psychologists at UNOP often drew pictures to supplement their verbal explanations, and frequently used metaphors to explain things to parents using familiar language (eg, using seeds as a metaphor for tumour cells when talking to parents who worked in agriculture). Psychologists also directly asked families about their beliefs in Mayan spirituality and experiences with traditional healers. They did not dismiss these beliefs, but rather acknowledged the evil eye and susto as separate conditions, unrelated to cancer or its treatment: “something important is that we know this is not a result of evil eye or fear, because those are completely different illnesses and they are treated in different ways”.
Parents recognised this support and in interviews described that psychologists “have time to talk” and explained things “in a very nice way that was easy for me to understand…so we can feel less sad or lonely”. They described psychologists providing them with hope for cure; “like she said, nothing is impossible; with treatment they try to cure the children” and said their explanations “gave me strength and confidence”.
Oncologist
Oncologists focused on the diagnosis, location of disease, prognosis and treatment plan for the child’s cancer. Like psychologists, oncologists often used a white board to draw anatomical pictures or pulled up the child’s diagnostic imaging scans on a computer. Oncologists used biomedical rather than metaphorical descriptions of cancer: “what happens with leukemia is that when the cell is formed…there’s a moment when it suffers a damage and it starts reproducing more and more. That’s leukemia”. Oncologists did not discuss Mayan spirituality with parents.
When describing their interactions with oncologists, some parents noted positive interactions: “when the doctor talked to us and he gave us the diagnosis he explained very well”; while others acknowledged a hierarchy or sentiment that they were not worth the doctor’s time, “I feel like I can’t go and talk to them…I see them busy or in a hurry, I feel like I am making them waste their time”. In interviews, parents described oncologists providing hope: “they told me not to worry, that we are going to make it, that he will receive the right treatment” and said, “they treat us kindly, and they don’t make us feel less important”.
Other providers
During interviews, parents referenced providers other than the psychologist or oncologist, and at times categorised UNOP providers generally as a source of information. Parents mentioned social workers, nutritionists, child life specialists and nurses as sources of information. One parent said “nurses, like I said, they help you a lot with the burden”, and another described, “the lady from nutrition is very kind, I can ask her anything”. Parents illustrated how these providers helped them understand their child’s diagnosis, providing reassurance, emotional support and hope (table 3).
Other patients and families
In addition to providers at UNOP, parents learnt about childhood cancer from other patients and families (table 3). By observing other children, families learnt about the physical consequences of treatment including temporary side effects such as hair loss, as well as permanent outcomes including enucleation and amputation. While many parents described initial fear associated with these observations, they also explained the supportive network of families as “a comfort chain that keeps growing”.
Lived experience and current cancer understanding
Throughout conversations with providers, as well as in subsequent interviews, parents described their own lived experience as a source of information. This source emerged as both a culmination of previously outlined sources and simultaneously independent. It was mentioned by parents who had pre-existing beliefs about cancer: “But it’s so different to live this”, as well as those who had never heard of cancer before: “I never heard about blood cancer, until now” (provider conversation). One mother commented on how the experience of having a child diagnosed with cancer separated her from other members of her community, “The ones that have lived this they understand, the others that haven’t lived this don’t understand”. Another described the difference between hearing about cancer and experiencing her child’s diagnosis: “Yes, we heard about it, we heard about tumors, but hearing is different than saying face to face, this is what your child has”.
In interviews, parents reflected on how little they knew when they started their journey, “we didn’t know about anything…we didn’t know what to do because of his disease”. They described worrying that they might have done something to cause their child’s cancer, or that they failed to recognise early symptoms. Parents also explained how their experiences at UNOP shaped their understanding of cancer, one saying “it’s like a 360-degree turn”. They talked about coming to terms with their child’s diagnosis: “they gave us the news…it’s hard to accept it, it takes days, you have to breathe”.
When asked in interviews about how their understanding of cancer had changed, parents often used allopathic descriptions: “She said cancer is a bunch of bad cells, but chemo will destroy the cells”. Some parents expressed understanding that their child’s illness was ‘aggressive’ and described learning about aetiology “we asked where that disease came from, she said even they didn’t know that. The disease just comes”. As parents discussed the allopathic model for cancer, some explained how their understanding differed from what they had previously thought or what their community believed about cancer, “once you have cancer you don’t have a good future…that’s what I heard until they started to explain to me here what type of cancer it was”. One father used allopathic explanations to talk to his family and community about his child’s cancer: “I explained it to them the way they explained it to me. I told them cancer is an active bad cell”. Parents also described accepting treatment saying, “the medicine has helped a lot”, and “chemo will destroy the cells”.
Almost all parents described feeling more hopeful based on experiences at UNOP. One parent described explicitly how providers at UNOP ‘motivate us and give us hope’. Parents hoped for cure, but also that their children would return to school or work, ‘recover soon’, ‘feel better’ and ‘grow, play and have happy life’. As parents expressed hope, many described a dual belief in God and medicine “Maybe He will send a miracle through the doctors” (provider conversation); “I think God gives the doctor his wisdom” (provider conversation). They prayed to God to provide a miracle, to work through or with the doctors to cure their children, and to give them patience and strength. Faith in God was expressed by parents who had referenced Mayan spirituality as well as those who had not and was acknowledged by providers throughout the diagnostic process.
Ultimately, parents described an evolution from fear or incredulity to acceptance of their child’s diagnosis (table 4). One mother explained that she previously equated cancer with death. While she never imagined it would happen in her family, she said she would not have pursued treatment without UNOP “I didn’t know this hospital”. When she was given the diagnosis, she felt sad but asked God for strength and learnt from the providers at UNOP, “I thought there was no medicine, but the doctor told me there is medicine”. She and her husband talked and decided that accepting care was best for their son, “if there is a solution for the disease, we thank God…I feel he is better with the medicine”.
Discussion
Similar to families everywhere, Guatemalan parents included in this study learnt about cancer, and their children’s diagnoses, from a variety of sources. Some of these sources, including prior experiences, media exposure and discussions within their communities, contributed to pre-existing cancer beliefs. While some of these beliefs were aligned with an allopathic medical model, others were not. In Guatemala, Mayan spirituality contributed to beliefs that a child’s cancer may be related to supernatural causes such as susto or the evil eye. In addition, many of the parents in this study had negative or fatalistic beliefs about cancer. Prior to arriving at UNOP, parents equated cancer with death, disfigurement and financial strain.
Nevertheless, parents’ cancer beliefs were not stagnant. As families went through the process of receiving a cancer diagnosis, they were exposed to new sources of information that reflected the culture of their cancer centre. At UNOP, this two-step process included extensive time with the psychosocial team. Psychologists used illustrations and metaphors to educate parents regarding cancer, techniques which have been shown to be effective for cross-cultural communication.17 18 Psychologists were also attentive to families’ pre-existing cancer beliefs, and specifically inquired about Mayan spirituality, even when it was not brought up by the family. As a part of their training, the psychosocial team at UNOP regularly reviews anthropological topics including Mayan beliefs and spirituality which help them provide culturally relevant care. Previous research has demonstrated that cultural differences in explanatory models can contribute to breakdowns of communication between patients and providers.19 In addition, an earlier study at UNOP indicated that up to 90% of families use traditional and complementary complementary medicine while receiving cancer treatment.20 By acknowledging and exploring family beliefs in Mayan spiritualty, the team at UNOP allowed families to openly discuss pre-existing concerns regarding cancer causation and treatment. This communication process enabled honest discussion of traditional beliefs and therapies, while simultaneously supporting acceptance of the allopathic medical model and need for treatment as subsequently described by the oncologist.
During diagnostic conversations, oncologists provided extensive information regarding the child’s diagnosis, location of disease, prognosis and treatment plan. Like the psychologists, oncologists often used images (either drawings or anatomical scans) to convey information. Oncologists focused on allopathic rather than metaphorical descriptions of cancer, and interviews with parents demonstrated their understanding and acceptance of this model.
Along with information, parents described receiving support from providers, patients and families at UNOP. Parents specifically identified how psychologists and oncologists gave them hope for cure, treatment and improved quality of life. As they expressed hope, parents often returned to their faith, integrating deep religious beliefs with a newer acceptance of the medical model. Some parents who expressed faith in God also alluded to traditional Mayan beliefs as they wrestled with aetiology and sought out traditional healers en route to UNOP. This suggests that for many parents in Guatemala spirituality is a complex combination of Mayan and Christian beliefs. In this study, Mayan spirituality was discussed in relation to cancer aetiology and traditional remedies, while God was associated with perseverance and hope. It is possible that this complex interplay set the stage for parents integrating new information as they received it from UNOP providers.
The combination of hope and education allowed parents to transition from fatalistic pre-existing notions of cancer, to a more positive narrative that absolved them from blame and included potential for cure. Prior work in high-income countries has explored the importance of hope throughout the cancer continuum,21–23 and ‘supporting hope’ was recently identified as an additional function of cancer communication for the paediatric population.24 While previous studies have focused on centres in the USA and other high-income countries, our results provide evidence for the importance of supporting hope in LMICs.
This study focused in depth on the diagnostic experience of 20 families at the only paediatric cancer centre in Guatemala. As with all qualitative research, the results may be limited in their generalisability. Further studies are necessary to explore the relevance of these themes to populations in other LMICs, as well as to the communication process at other stages of cancer care. In addition, given the large proportion of families included with haematological malignancies, our study may have over-represented the perspective of this population; additional studies may be necessary to further explore the beliefs of families with solid malignancies. Interview scripts were developed in English, and all analyses were conducted in English, while data were collected in Spanish. A bilingual research team reviewed scripts and transcriptions in both languages, however it is possible that translation of qualitative data may have affected content. In addition, we were unable to conduct interviews in traditional Mayan dialects which may have limited participation from certain communities, or the ability for some families to fully express themselves. To our knowledge, only one family declined participation in the study due to language. Overall, we had a participation rate of 62.5%. The primary reason caregivers declined participation in the study was hesitancy with the audio recordings, and the participation rate for this study is similar to that found in previous paediatric oncology work involving audiotaping.25 However, it is unclear what if any effect on our results this selection bias may have had. Finally, although this study focused on paediatric cancer, paediatric patients were not included. A child life team at UNOP separately discusses diagnoses with paediatric patients and thus they were not included in recorded conversations or interviews. Future studies are necessary to explore diagnostic communication at UNOP from the perspective of paediatric patients.
At the time of diagnosis, parents in Guatemala hold pre-existing cancer beliefs that may diverge from the medical model and are instead influenced by sociocultural and contextual factors. The findings from this study demonstrate that a communication process that is attentive to these beliefs and overarching social concerns supports acceptance of a medical model and need for treatment, without fully supplanting pre-existing beliefs. In Guatemala, an interdisciplinary care model that includes psychosocial involvement from diagnosis has been demonstrated to reduce treatment abandonment rates, and similar models have been applied to other LMICs.10 Our findings suggest that there are important pieces of this model in addition to an interdisciplinary approach, including verbal, written and pictorial education, attention to pre-existing beliefs, and supporting hope, which contribute to its success. Providers in settings of all resource levels may be able to use these techniques to support cross-cultural cancer communication, reduce treatment abandonment and improve therapy adherence. Additional studies should be conducted to validate these findings in other settings and develop targeted interventions.
Data availability statement
Data are available upon request.
Ethics statements
Ethics approval
St Jude Children’s Research Hospital: IRB Number: 19–0162; Reference Number: 005883, and Unidad Nacional Oncologia Pediatrica (no reference number).
Acknowledgments
The authors would like to thank Pilar Alvarado, Inés Ordoñez, Paulina Salazar and Debby Velleman for their efforts assisting in data collection, and the entire medicina integral team at Unidad Nacional de Oncología Pediátrica for supporting this work. We would also like to thank the parent participants of this study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Soumitra S Bhuyan
Twitter @DylanGraetzMD
Contributors DG, CR-G and JWM developed the idea. SR, LF, AC-S and DG were responsible for overseeing and completing data collection. DG and GF analysed the data. DG drafted the initial manuscript. DG and JWM prepared the tables and figures. All authors contributed to interpretation of the findings, editing of the article and approval of the final submitted version.
Funding This work was funded by American Syrian Associated Charities of St Jude Children’s Research Hospital and a Conquer Cancer Young Investigator Award. Any opinions, findings and conclusions expressed in this material are those of the authors and do not necessarily reflect those of the American Society of Clinical Oncology or Conquer Cancer.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.