Article Text

Abstract
Introduction Measles vaccine (MV) may improve health beyond measles protection. To avoid wastage from multi-dose vials, children in Guinea-Bissau are only measles vaccinated when aged 9–11 months and when six or more children are present. We assessed health impacts of providing MV to all measles-unvaccinated children 9–35 months.
Methods We cluster-randomised 182 village clusters under demographic surveillance in rural Guinea-Bissau to an ‘MV-for-all-policy’ arm where we offered MV regardless of age and number of children present at our bi-annual village visits, or a ‘Restrictive-MV-policy’ arm where we followed national policy. Measles-unvaccinated children aged 9–35 months were eligible for enrolment and followed to 5 years of age. In intention-to-treat analyses, we compared mortality using Cox regression analyses with age as underlying timescale. The primary analysis was for children aged 12–35 months at eligibility assessment. Interactions with several background factors were explored.
Results Between 2011 and 2016, we followed 2778 children in the primary analysis. MV coverage by 3 years was 97% among children eligible for enrolment under the MV-for-all-policy, and 48% under the Restrictive-MV-policy. Mortality was 59% lower than anticipated and did not differ by trial arm (MV-for-all-policy: 45/1405: Restrictive-MV-policy: 44/1373; HR: 0.95 (95% CI 0.64 to 1.43)). The effect of MV-for-all changed over time: The HR was 0.53 (95% CI 0.27 to 1.07) during the first 1½ years of enrolment but 1.47 (95% CI 0.87 to 2.50) later (p=0.02, test of interaction). Explorative analyses indicated that the temporal change may be related to interactions with other childhood interventions.
Conclusion The MV-for-all-policy increased MV coverage but had no overall effect on overall mortality.
Trial registration number NCT01306006.
- child health
- epidemiology
- immunisation
- public health
- vaccines
Data availability statement
Data are available upon request. Requests for access to the data should be addressed to the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Two randomised trials and several observational studies indicate that measles vaccination lowers mortality.
A policy of only vaccinating children aged less than 12 months and only vaccinating if more than six children were due to be vaccinated was practiced in Guinea-Bissau.
What are the new findings?
Making measles vaccine (MV) available at biannual village visits increased the coverage by 3 years of age to 97% compared with 48% in the control arm.
Providing MV for all had no overall effect on mortality (HR: 0.95 (95% CI 0.64 to 1.43)) but the effect changed during the trial period from an HR of 0.53 (95% CI 0.27 to 1.07) during the first 1½ years of enrolment to 1.47 (95% CI 0.87 to 2.50) among children enrolled later (p=0.02, test of interaction).
Explorative analyses indicated that the change in effect over time may be explained by differential exposure to other vaccines.
What do the new findings imply?
The restrictive measles vaccination policy left many children unvaccinated and disregarding it (in line with recommendations by WHO) increases coverage and presumably improves measles control.
Beneficial effects of MV may be contingent on the number and sequence of other vaccines.
Introduction
In many low-income countries, measles vaccines (MV) are provided at 9 months of age according to the schedule outlined by the WHO.1 A second dose is recommended during the second year of life, either through a scheduled second MV or through campaigns.2
In Guinea-Bissau in West Africa, the official country estimate for MV coverage in 2011 was 78%,3 and thus far from the recommended coverage target of ≥90% necessary to obtain measles control.2 Although childhood vaccines are provided free of charge at health centres and through outreach services, there are significant barriers to measles vaccination. Among others, we have identified the focus on vaccine wastage as a major barrier. Vaccination coverage for vaccines scheduled during infancy is assessed by 12 months of age. Providing vaccines to children older than 12 months of age does not count in the statistics and is considered wastage.4 Furthermore, since MV is a live vaccine typically provided in 10-dose vials, which has to be discarded 6 hours after opening, the focus on wastage has entailed that children in Guinea-Bissau are only measles vaccinated if at least six children aged 9–11 months are present at the same time. Hence, this ‘restrictive vial opening policy’ results in missed opportunities, and fewer measles vaccinated children.4
Several observational studies5–7 and two randomised trials8 9 from Guinea-Bissau indicate that measles vaccination reduces childhood mortality and morbidity to a much larger extent than can be expected by preventing measles infection. These potential ‘non-specific effects’ (NSEs) of MV were recently examined in a WHO-sponsored literature review which concluded that the marked benefits observed in both randomised trials and observational studies could not be explained by prevention of measles.10 Thus, the restrictive vial opening policy both deprives children of protection against measles infection and of the beneficial NSEs of MV.
To assess the consequences of the restrictive vial policy, we conducted a cluster-randomised trial in rural villages under health and demographic surveillance. We randomised villages to either follow or disregard the national measles vaccination policy during the surveillance visits. In the national measles vaccination policy arm, the ‘Restrictive-MV-policy’-arm, we only vaccinated children 9–11 months of age and only if six or more children were present at the same time. In the ‘MV-for-all-policy’-arm, we provided MV to all measles-unvaccinated children between 9 and 35 months of age, regardless of age and number of children present at a vaccination session. We hypothesised that among measles unvaccinated children aged 12–35 months, mortality before 5 years of age would be 30% lower in the ‘MV-for-all-policy’-arm.
Methods
Setting
The cluster-randomised trial ‘MVEPI’ was conducted in Bandim Health Project’s (BHP) health and demographic surveillance system (HDSS) in rural Guinea-Bissau. The BHP follows 182 clusters of approximately 100 women of fertile age and their children under 5 years of age in the nine rural health regions of Guinea-Bissau.11 The clusters are routinely visited every 6 months by BHP mobile teams registering new pregnancies and children; for all children information on vaccination status is collected (online supplemental material).
Supplemental material
Trial design and randomisation
The 182 rural clusters were randomised 1:1 to either ‘MV-for-all-policy’ or ‘Restrictive-MV-policy’ stratified by region and pretrial mortality rates (online supplemental material). The implications of the randomisation differed for 9–11-month-old children and older children. Among older children, all unvaccinated children in the MV-for-all-policy clusters received MV, and no child in the Restrictive-MV-policy clusters received MV. Among the 9–11-month-old children, children in the MV-for-all-policy clusters received MV irrespective of the number of measles-unvaccinated children in the cluster, whereas in Restrictive-MV-policy clusters, only 9–11-month-old children in clusters with at least six 9–11 months old measles-unvaccinated children present, received MV.
We planned the following analyses: first, an intention-to-treat analysis among all measles-unvaccinated children aged 12–35 months (main analysis) as well as all children aged 9–35 months (the population of 12–35 months old children was the basis for our sample size calculation). Second, a per-protocol analysis, including only children presenting at the vaccination post and deemed eligible for vaccination. Furthermore, in a third analysis, we aimed to assess the community level impact of MV-for-all among all children living in the HDSS villages from the first day they could potentially have been enrolled.
We based our initial sample size calculations on a hypothesised halving of mortality8 but based on emerging evidence updated it to a 30% reduction (online supplemental material). Assuming that providing MV-for-all would lower overall mortality by 30% between enrolment and 5 years of age, that 8% of follow-up time would be censured due to migration, a cluster size of 17, interclass correlation coefficient of 0.5% and a registered pre-trial mortality of 8.3%, we had planned to enrol 3676 children in the age group 12–35 months.
Enrolment
The trial was initiated in February 2011 and enrolment ended in December 2015 when a national measles vaccination campaign was conducted. Measles-unvaccinated children aged 9–35 months of age were eligible for the trial. During the bi-annual visits to the clusters by the BHP mobile teams, mothers/guardians of measles-unvaccinated children between 9 and 35 months of age were identified by trained BHP fieldworkers and interviewed on experiences with seeking MV. The study design and purpose of the MVEPI study was explained to the mother/guardian. If they were interested in participating in the study, the mother/guardian and child were sent to the health post, where the BHP nurse performed a health check of the child (online supplemental material). Children in the Restrictive-MV-policy clusters were vaccinated at the health post if six or more measles-unvaccinated children aged 9–11 months were present at the same time. In the MV-for-all clusters, all measles-unvaccinated children aged 9–35 months at the time of the visit were measles vaccinated by the BHP regardless of number of children present. Only children who were not acutely ill, had a mid upper-arm circumference (MUAC) >110 mm and had not received a live vaccine within the last 28 days were vaccinated. Written consent was sought from the mother/guardian of children older than 12 months who were vaccinated, as this is not standard practice in Guinea-Bissau. The MV (Edmonston-Zagreb, Serum Institute of India) was administered as a deep subcutaneous injection in the subscapular region.
Until July 2012, we enrolled children aged 9–35 months in all villages of the rural Bandim HDSS. In 2012, we initiated a randomised trial of an additional early MV in three of the regions12 and paused enrolments for the MVEPI trial in these regions for 14 months (online supplemental material).
Follow-up
All children followed in the MVEPI trial, were surveyed through the routine BHP surveillance system bi-annually until their fifth birthday, migration or death. At every bi-annual follow-up visit, information on vital status and admissions to hospital was collected and MUAC measured. The reason for loss to follow-up and date of the event was noted by the BHP field workers. Registered hospital admissions and deaths were followed by an interview on the circumstances, symptoms, possible diagnosis and dates.
Statistical analyses
To assess the impact of an MV-for-all-policy, all analyses were based on measles-unvaccinated children eligible for enrolment in the MVEPI study (intention-to-treat-analyses). Since the implication of the policy differed for children above and below 12 months of age, the primary analysis was based on the intention-to-treat population of children aged ≥12 months of age. Children aged 9–11 months were analysed combined with ≥12 months old children in secondary analyses. We compared sociodemographic and baseline health variables for children eligible for enrolment in the MV-for-all-policy arm with children eligible for enrolment in the Restrictive-MV-policy arm.
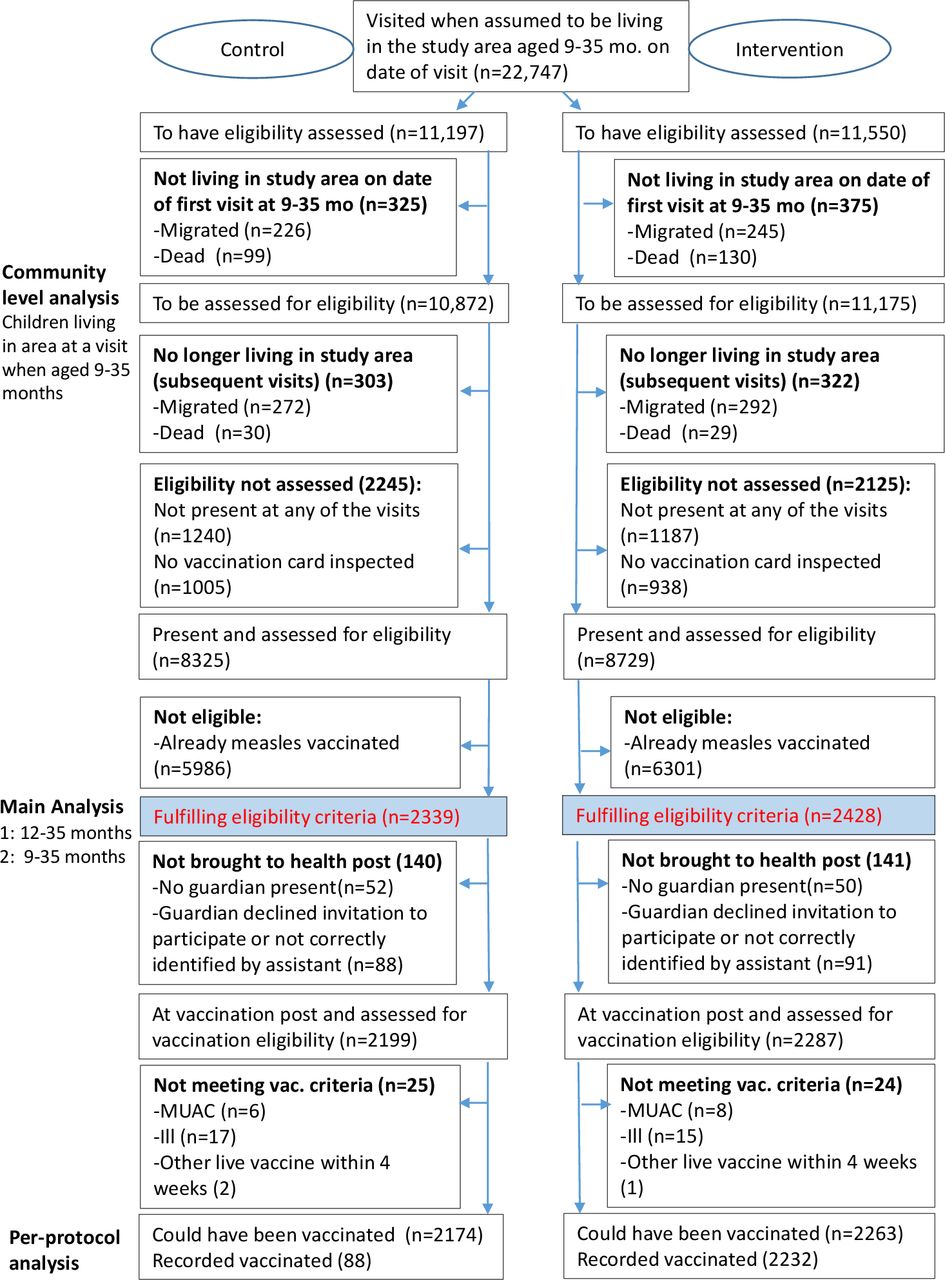
We assessed the impact of living in MV-for-all-policy clusters on mortality from the date of eligibility assessment. We censored the observation time for children at the date of the first event of either: their fifth birthday, death (or first hospital admission, see below), migration or first visit after a new MV-campaign trial initiated by the BHP in November 2016.13 HRs were estimated in Cox proportional hazards models with age as the underlying timescale, stratified by randomisation strata (region and high/low pretrial mortality) and used robust SE to account for village cluster. Proportional hazards assumptions were tested using Schoenfeld residuals. In the supplementary results, we show a per-protocol analysis, including only children who were enrolled in the MVEPI trial and the results on the community level, including all children who were visited at 9–35 months of age (figure 1).
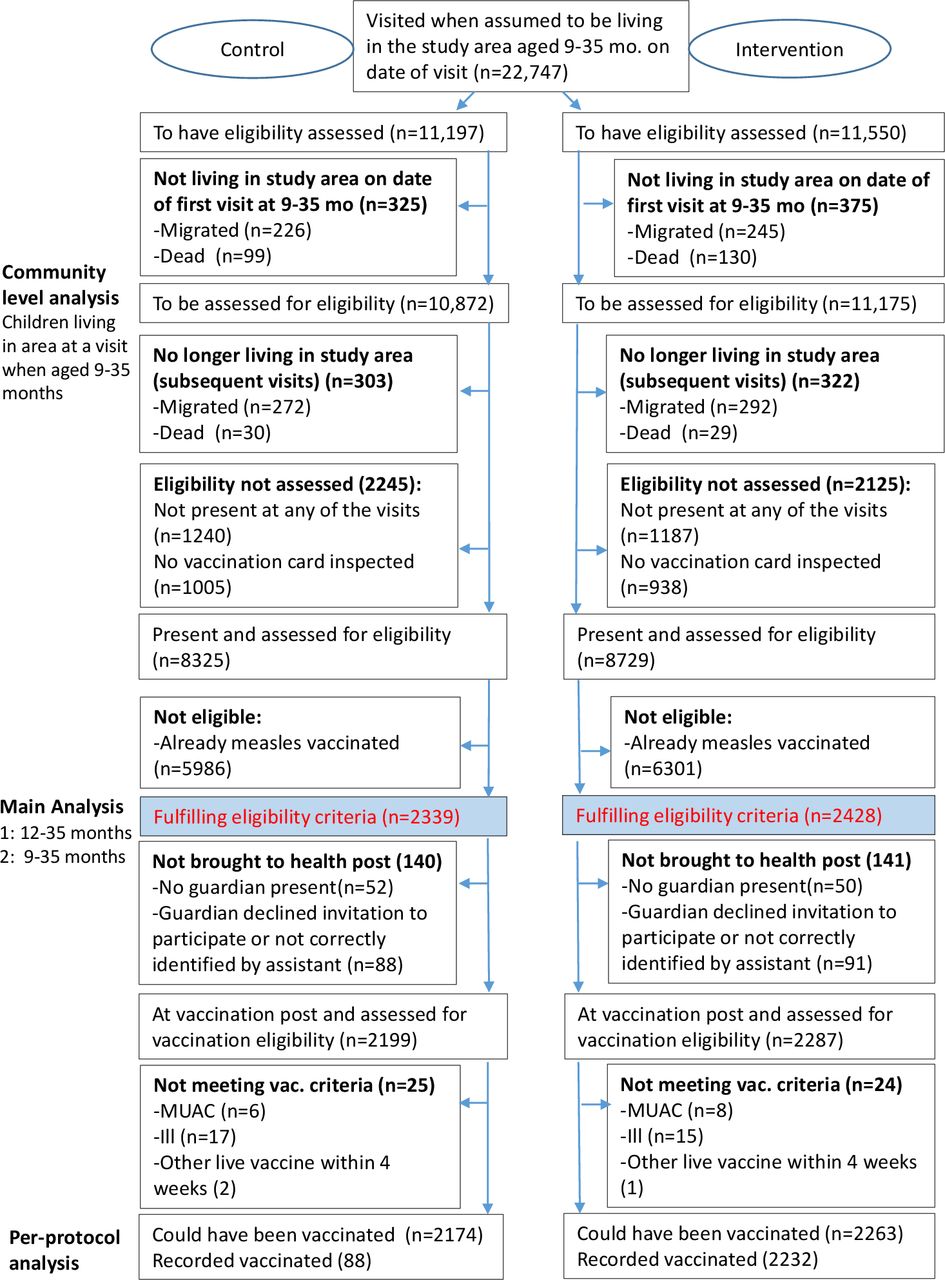
Children screened for eligibility and included in the MVEPI trial. MUAC, mid upper-arm circumference.
In addition, we assessed the impact of the MV-for-all-policy on the risk of hospital admission and MUAC measured at the first visit after enrolment (online supplemental material). Main results are presented overall and separately for girls and boys since prior analyses have indicated that the beneficial effect of MV is stronger in girls than boys.5 8 14–16
To assess the effect of the MV-for-all-policy on MV coverage and to investigate whether children in the Restrictive-MV-policy arm were vaccinated elsewhere after 4 enrolment, we assessed MV coverage by 36 months of age. We did so among all children with a seen vaccination card after 36 months and among children fulfilling the eligibility criteria. We report coverage by study arm and age at enrolment.
For the mortality outcome, we conducted several analyses to investigate determinants of the effect. Vaccination campaigns during follow-up may change the effect of the trial-intervention as a new vaccine becomes the most recent vaccine in both intervention and control arm.17 In prespecified analyses, we therefore examined whether campaigns affected the mortality rate and modified the effect of living in MV-for-all villages. To do so, we split the follow-up time at the date of eligibility to vaccination campaigns during follow-up. A resulting dummy variable (before/after the time-split) was investigated as a potential effect modifier. Two national MV campaigns, several oral polio vaccination (OPV) campaigns and one campaign with the meningitis A vaccine (MenAfriVac) took place while children were followed in the trial (online supplemental table 1 and figure 1).
In explorative analyses, we stratified the analyses for factors that in prior studies have been associated with a differential effect of MV. The assessed background factors were: season of vaccination,18 eligibility for (likely received) campaign-MV before enrolment19 20 and administration of pentavalent vaccine (Penta) at the time of enrolment.21 Since almost all children had been eligible for OPV campaigns prior to enrolment, we performed stratified analyses by number of OPV campaigns rather than by yes/no to campaign exposure.22 We furthermore explored whether the effect differed by number of doses of Penta and whether effects changed before and after initiating the early MV trial, where all children below 12 months of age were offered MV regardless of the number of children present.12 For the potential effect modifiers, we investigated interactions by including a trial-arm*potential effect modifier-term in the Cox model, and report the p value from the corresponding Wald test. Unless a stratification criterion applies only to limited age group, these analyses are presented for all children. All analyses were performed in STATA V.16.1 (StataCorp).
Patient and public involvement statement
Patients and the public were not involved in the design and conduct of this research.
Results
Study cohorts
A total of 22 749 children 9–35 months of age, were recorded in the BHP databases and sought visited between 2011 and 2015. Four thousand seven hundred and sixty-seven were eligible for inclusion in the MVEPI trial at date of visit to the villages (2339 in the Restrictive-MV-policy arm and 2428 in the MV-for-all-policy arm) (the main (intention-to-treat) analysis) and 4437 (93%) were seen at the enrolment post and fulfilled the criteria for vaccination (per-protocol analysis). In the Restrictive-MV-policy arm, 88 of 2174 children (4%) seen at the vaccination post were measles vaccinated at the date of enrolment according to national policy, as they were between 9 and 11 months old and six and more children were present. In the MV-for-all-policy arm, this was 2232 of 2263 (99%; figure 1).
Background characteristics
Table 1 displays the characteristics of children eligible for inclusion. More than half (2778, 58%) were aged 12–35 months on eligibility assessment. Our randomisation achieved balanced groups for most of the assessed factors including age, sex, maternal age, maternal schooling, indicators of socioeconomic status and prior vaccinations both among children aged 12–35 months and among all children. Children in the MV-for-all-policy clusters were more likely to receive a missed dose of Penta at eligibility assessment (table 1). Region of residence and ethnicity of the mother also differed by trial arm. For children who were not enrolled as they had already received MV, there were no marked differences in mortality between the MV-for-all clusters and the Restrictive-MV-policy clusters during the same period of follow-up (online supplemental material).
Characteristics of the measles-unvaccinated children followed in the MVEPI trial
Intervention results
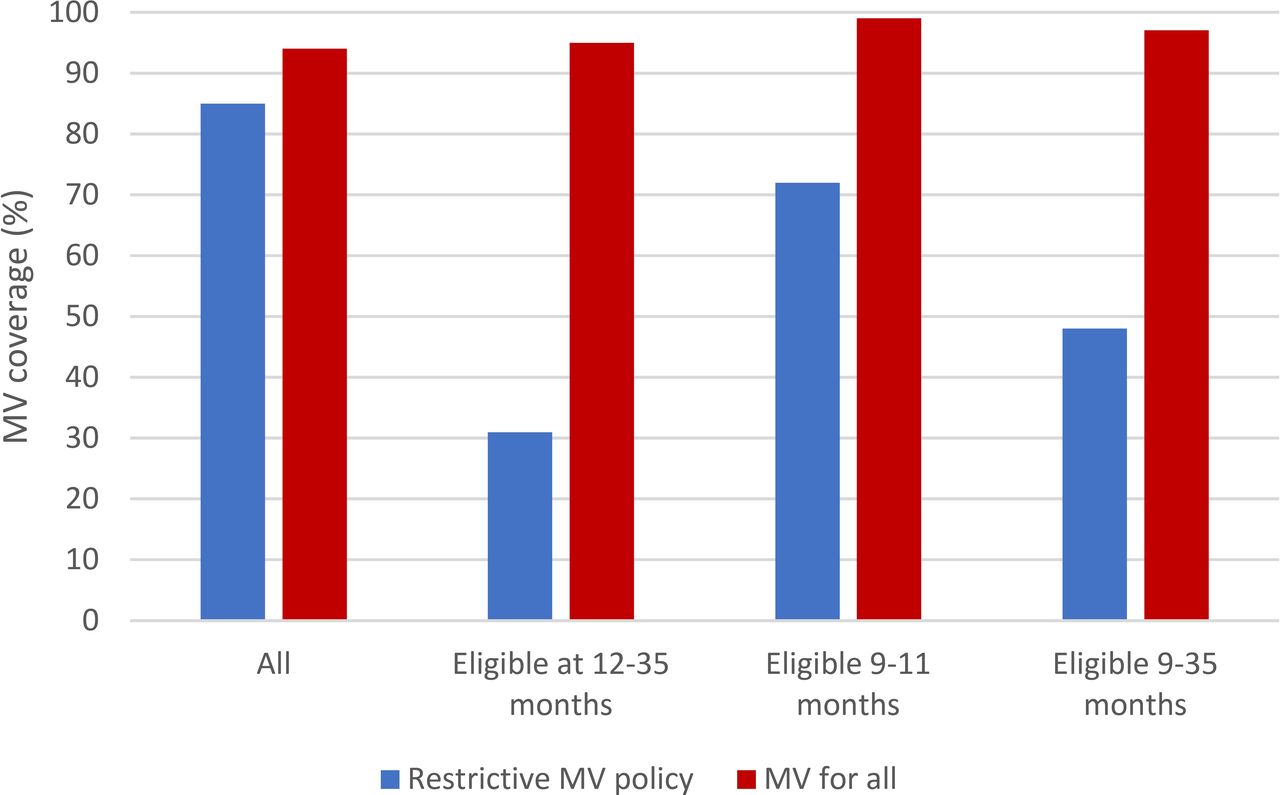
The intervention had a marked effect on MV coverage. Among children with a vaccination card inspected after 3 years of age, the vaccination coverage for MV was 85% (6185/7284) for children living in the Restrictive-MV-policy clusters while it was 96% (7269/7568) in the MV-for-all clusters. Among the initially measles-unvaccinated children, less than a third of the children 12 months or older in the Restrictive-MV-policy arm, had received a routine MV by 3 years of age (figure 2).
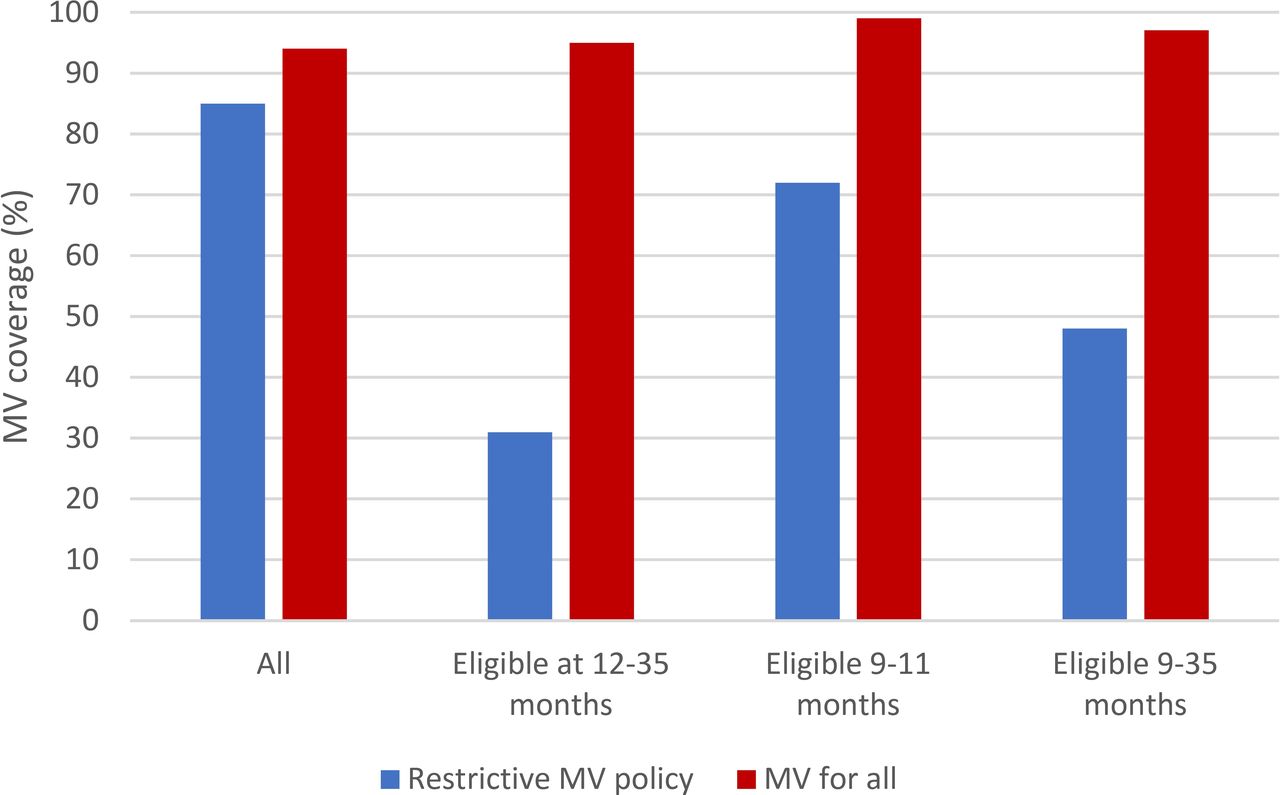
Measles vaccination (MV) coverage by 36 months of age among children with a vaccination card seen after 36 months.MV coverage assessed among: all (all children with eligibility assessment) 14 852 (69%); eligible at 12–35 months: 1923 (69%); eligible at 9–11 months: 1424 (72%); eligible at 9–35 months: 3347 (70%).
Among the 2778 children aged 12–35 months when eligible for enrolment, we registered 89 deaths before 5 years of age during a median follow-up of 2.8 years (IQR: 2.0–3.6 years). This corresponded to a mortality of 3.4% or 12/1000 person years, which was less than half of the anticipated rate based on prior data on which we had based our sample size calculation. There were no differences in mortality for children living in the MV-for-all versus Restrictive-MV-policy clusters (HR: 0.95 (95% CI 0.64 to 1.43)) (figure 3, table 2). This was also seen among all children (HR of 1.06 (95% CI 0.78 to 1.44)) (table 2), in the per-protocol analyses (online supplemental table 2) and the community level analysis (online supplemental material).

{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier survival estimates by trial arm. All children aged 12–35 months.MV, measles vaccine.
Mortality and HRs for death among children eligible for enrolment in the MVEPI trial. Overall and stratified by sex of eligibility assessment
The effects tended to differ for boys and girls (table 2). Among 12–35 months old girls, living in the MV-for-all clusters was associated with a tendency towards higher mortality compared with living in the Restrictive-MV-policy clusters (HR: 1.20 (95% CI 0.63 to 2.27), while the HR was 0.78 (95% CI 0.42 to 1.45) for boys aged 12–35 months (p=0.39 for interaction). The same pattern was observed among children aged 9–11 months. Hence, though not statistically significant the sex-differential effects became more pronounced in the combined analysis of all children (boys: HR=0.79 (95% CI 0.49 to 1.25); girls: HR=1.43 (95% CI 0.87 to 2.35); p=0.10 for interaction). Repeating the analyses with time since eligibility assessment as underlying timescale, resolved a potential problem of non-proportional hazards and did not alter conclusions (online supplemental material).
Other outcomes: hospital admissions, nutritional status and MV coverage
There were fewer hospital admissions than deaths both among children aged ≥12 months (n=61) and among all children (n=133). We observed no difference in the hospital admission rates between the two trial arms for children aged 12–35 months (HR=1.09 (95% CI 0.66 to 1.79)). Nor was there any difference among all children and no marked differences by sex (online supplemental table 3).
No differences in MUAC at the first visit after assessment for eligibility were seen between the two groups, except for boys aged 9–11 months living in MV-for-all-policy villages, where there was a slight but statistically significant lower MUAC (143 mm) than among boys living in Restrictive-MV-policy villages (145 mm) (online supplemental table 4).
Prespecified stratified analyses of mortality effects: interactions with other interventions
Vaccination campaigns during follow-up may change the effect of the trial-intervention as a new vaccine becomes the most recent vaccine in both intervention and control arm.17 We examined whether campaigns affected the mortality rate and modified the effect of living in MV-for-all villages. When splitting the follow-up time into before and after MV campaigns, the mortality rate among children aged 12–35 months differed, the HR for after versus before MV campaigns being 0.45 (95% CI 0.28 to 0.75). The HR for after versus before OPV campaigns was 0.81 (95% CI 0.45 to 1.45) and the HR for after versus before the MenAfriVac campaign was 1.11 (95% CI 0.48 to 2.58).
Splitting the follow-up time of children eligible for enrolment into before and after the MV or OPV campaigns, showed no marked differences between the two trial arms. However, among all children, the HR for MV-for-all was 0.97 (95% CI 0.70 to 1.34) prior to the MenAfriVac campaign but 2.42 (95% CI 0.89 to 6.60) after the campaign (p=0.09 for interaction) (online supplemental table 5). The potential negative effect tended to be more pronounced in girls (HR=5.77 (95% CI 0.68 to 48.39)) than boys (1.58 (95% CI 0.43 to 5.79)).
Explorative analyses
In explorative analyses, we assessed if the effect varied over time and by factors which in prior trials have proved important for the effect of MV. Among children with eligibility assessment in the rainy season, living in the MV-for-all clusters tended to be associated with higher mortality compared with living in the Restrictive-MV-policy clusters (HR=1.35 (95% CI 0.72 to 2.53)), whereas children with eligibility assessment in the dry season tended to benefit from living in the MV-for all clusters, HR=0.69 (95% CI 0.40 to 1.21), p=0.13 for a differential effect. The tendencies were similar when the analysis was extended to all children (online supplemental table 6) and for hospital admissions (online supplemental table 3).
When analysed by enrolment period, the effect differed significantly before and after the initiation of the concurrent early MV trial. Among children aged 12–35 months, living in the MV-for-all villages tended to be beneficial (HR=0.53 (95% CI 0.27 to 1.07)) if they were assessed for eligibility before 18 July 2012 (period 1), but not after (period 2): HR=1.47 (95% CI 0.87 to 2.50) (p=0.02 for interaction) (figure 2). Extending the analysis to all children, the HR was 0.70 (95% CI 0.43 to 1.15) in period 1 and 1.46 (95% CI 0.99 to 2.14) in period, p=0.03 for interaction. The differential effect was strongest for girls, where the HR changed from 0.38 (95% CI 0.10 to 1.49) to 2.15 (95% CI 0.93 to 4.97) (p=0.04) while the HRs for boys were 0.63 (95% CI 0.27 to 1.49) and 0.98 (95% CI 0.42 to 2.30) (online supplemental figure 2). Changing the cut-off date did not alter conclusions (online supplemental material). Since effects differed over time, we furthermore assessed if potentially explanatory factors changed over time.
First, previous studies have shown that OPV-campaigns may affect the effect of MV.22 23 99% (2765/2778) of children aged 12–35 months had been exposed to one or more OPV campaigns prior to eligibility assessment (median number: 3 (IQR: 2–4)). For the younger children aged 9–11 months, 91% (1816/1989) had been exposed (median number: 2 (IQR 1–2)) (online supplemental table 7). Children who had been exposed to two or fewer campaigns prior to enrolment, tended to have higher mortality if they lived in the MV-for-all clusters than if they lived in the restrictive MV clusters, HR=1.69 (95% CI 0.97 to 2.95). In contrast, children who had been exposed to three or more OPV campaigns benefitted from living in the MV-for-all clusters, HR=0.54 (95% CI 0.31 to 0.97) (p=0.005 for interaction). The pattern was similar for all children (table 3). Finer subdivisions of number of doses of campaign OPV indicated beneficial effects among children exposed to 3 or 4+ doses, negative effects in children exposed to 0–1 dose (online supplemental figure 3). The differential effect was observed in both boys and girls (online supplemental figure 3) and may have been stronger after exposure to OPV campaigns after enrolment (online supplemental table 8).
Mortality and HRs for death of children eligible for enrolment in the MVEPI trial, according to number of doses of oral polio vaccine in campaigns prior to assessment of eligibility
In the first period, more children were exposed to several OPV campaigns before eligibility assessment (online supplemental figures 4 and 5). The median number among 12–35 months old children was 4 (IQR: 3–5), while it was 2 (IQR: 2–3) in the second period. The pattern of lower HR for children exposed to ≥3 campaigns was observed in both periods (online supplemental figure 5).
As indicated in table 1, Penta administered at enrolment differed between the two arms of the study. We therefore explored how effects varied by Penta status. Reception of Penta at eligibility assessment did not modify effects (online supplemental table 9). Among children who had not received Penta3 at enrolment, living in the MV-for-all-policy villages tended to be beneficial, HR: 0.59 (95% CI 0.31 to 1.14) while it was not among children who had received Penta3: HR: 1.33 (95% CI 0.77 to 2.31) (p=0.06 for interaction) (table 4). The differential effect was similar in all children (p=0.008 for interaction). Stratifying by doses of Penta indicated a dose–response relationship (online supplemental figure 6).
Mortality and HRs for death of children eligible for enrolment in the MVEPI trial, according to number of doses of pentavalent vaccines (Penta) prior to assessment of eligibility
The Penta3 coverage in children aged 12–35 months was higher during period 2 (61%, 941/1551) than period 1 (54% (667/1226)) (relative risk adjusted for randomisation strata=1.09 (1.02–1.17)). Higher HR with increasing number of Pentas was observed throughout the trial (online supplemental figure 7).
Discussion
Providing MV-for-all at our biannual visits resulted in a marked increase in MV coverage. More than half of the children in the Restrictive-MV-policy arm were still measles-unvaccinated by 3 years of age. Therefore, from a measles preventive point of view, it is imperative that MV is provided to all children regardless of age and number of children present. This way the target coverage for MV of ≥90%, set forth by the WHO, may be reached.2 We have previously shown that the Restrictive-MV-policy entails that mothers take their children several times to seek MV—on average 1.4 times, conferring considerable costs and time spent on taking the child to the healthcare facility for MV.24 The average cost of one MV dose in a 10-dose vial was US$0.279 in 2017 and it is thus one of the cheapest vaccines in the national immunisation programmes.25 In comparison, one dose of Penta had a price of US$2.25 in 2017. Thus, providing MV for all children is a cheap childhood intervention which is key in the strive for measles elimination.
We found no overall effect on mortality, hospital admissions and MUAC for children living in clusters randomised to MV-for-all-policy compared with children living in clusters randomised to Restrictive-MV-policy. Though the effect tended to differ by exposure to routine and campaign vaccines, the lower than expected mortality may have limited the power of these analyses. Most remarkable, the mortality effect changed from being beneficial in the beginning to have negative effects in the last part of the trial.
Strengths and limitations
Nesting the trial into the HDSS with bi-annual household visits, allowed for better registration and more precision of child age as well as the date of death and migrations. Thanks to the HDSS we also had full follow-up and prior data available and could perform stratification of clusters based on pretrial mortality levels prior to randomisation. Background factors were generally evenly distributed among the two trial arms and we observed similar mortality by trial arm among the group of previously measles vaccinated children who were not eligible for trial participation. The clusters under surveillance in the rural HDSS have been sampled with a probability of sampling proportional to population size, but do not include the capital area, where the likelihood that having a low number of children present for vaccination would be lower. Thus, estimates cannot be extrapolated to the whole country.
Our main outcome was mortality. Due to the regular follow-up of the children, we consider the information on this hard end-point very valid. Even when children are travelling, other informants than the mother usually provide valid information on the vital status of the child. Our secondary outcome, hospital admissions, was based on statements made by the mother or another relative, but as hospital admissions are rare and major health events, we still consider the information reliable (online supplemental material).
The lower than expected mortality during the follow-up period, meant that we did not have the planned power to detect a significant difference in mortality if the real effect had been as hypothesised (online supplemental material). Additionally, there were potentially important effect modifiers that we did not have sufficient power to examine. Furthermore, the policy was not implemented strictly: though children older than 12 months were not vaccinated by our teams, 31% of the children aged 12–35 months in the Restrictive-MV-policy clusters had received MV during follow-up. This may have diminished our ability to detect a potential effect of the MV-for-all-policy.
We have performed many stratified analyses, and though the stratification variables are informed by prior studies, their number increases the risk of chance findings. No correction has been made for multiple comparisons and the results of our stratified analyses should be interpreted with caution.
Consistency with other studies
Among children who were eligible for enrolment in MVEPI in the dry season, both mortality and hospital admissions tended to be lower in the MV-for-all villages than in the Restrictive-MV-policy clusters, while it tended to be higher in the rainy season. Stronger beneficial effects in the dry season have previously been observed in a randomised trial of early MV for both mortality8 and admissions.18
Almost all children in the present trial were exposed to OPV campaigns prior to enrolment. These campaigns may have beneficial effects on overall child mortality26 27 and in a recent trial of two-dose MV versus one dose MV, OPV campaign was associated with a lower mortality, particularly among children in the one-dose MV group28 and with stronger effects for girls.23 28 Our findings that the effects of MV differed by the number of OPV doses, with negative effects in children exposed to 1–2 doses, but beneficial effects in children exposed to 3+ doses, has not been examined previously. In prior studies, we have assessed the effect in young children in early MV trials who have been exposed to 0, 1 or 2 campaigns, and in these observed that the HR increased across additional doses of OPV before MV.22 28 However, the children in these trials were much younger and therefore given OPV (rather than OPV+vitamin A) and exposed to 2 versus 1 dose of MV.
We have previously observed that children receiving additional doses of DTP after MV during follow-up did not benefit from MV.20 29 In the present trial, we observed that children fully vaccinated with the DTP-containing Penta had a negative effect, while children still missing doses of Penta benefitted. This has not been examined previously.
MV has been associated with beneficial effects primarily for girls.8 20 However, in this trial, girls in MV-for-all-policy clusters had higher mortality than girls in Restrictive-MV-policy clusters. Our stratified analyses indicate that subsequent exposure to MenAfriVac and potentially prior exposure to OPV could offer explanations for the contrast. Negative effects of vaccination with other non-live vaccines after MV have been observed previously30 31 and negative interactions between OPV and MV may be stronger for girls than boys.23
Interpretation and implications
We observed an inversion in the effect of the intervention over time, with the effect shifting from an almost 50% lower mortality during the first period of the trial to an almost 50% higher mortality during the second period of the trial. This change in effect was particularly marked for girls. We speculate that part of the change in effect might be explained by the exposure to the MenAfriVac campaign, which could potentially have increased mortality in period 2, particularly in the MV-for-all-policy clusters and particularly for girls. This presupposes that the increased mortality associated with receiving non-live vaccines after MV is generalisable to MenAfriVac. However, the NSEs of MenAfriVac have not been investigated yet. Our exploratory analyses also identified the increase in Penta coverage and differential exposure to several OPV campaigns prior to enrolment as potential explanations. Both exposure to 0–2 doses of campaigns OPV and Penta3 which appeared to cause a negative effect of MV-for-all, were more common in period 2 than period 1 and the patterns were consistent within period 1 and period 2. Similar patterns were observed for both sexes, but the potential negative effects appeared stronger in girls than boys (online supplemental figure 5). The observations were unplanned, and though the internal consistency supports causality, we cannot rule out that other factors correlated with the identified effect modifiers may have played a role.
Numerous studies have demonstrated that non-live vaccines after MV have a negative effect particularly for girls.14 17 29 31 We speculate that this might explain the observed pattern after MenAfriVac. We have argued elsewhere that providing a live vaccine after non-live vaccines reverses a potential detrimental effect of the non-live vaccine.17 However, the present data suggest that MV after Penta3 may not always be sufficient. Despite no measurable overall benefit on health, it was clear that the MV-for-all-policy had a marked effect on MV coverage.
Conclusion
The MV-for-all-policy facilitated vaccination opportunities for children who would otherwise be unlikely to receive measles vaccination. We found no overall effect on child health but detected differential mortality patterns indicating that both prior and subsequent vaccine exposures affect the response to MV.
Data availability statement
Data are available upon request. Requests for access to the data should be addressed to the corresponding author.
Ethics statements
Ethics approval
The protocol was approved by the National Ethics Committee in Guinea-Bissau and the Central Ethical Committee in Denmark gave consultative approval.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Seye Abimbola
Twitter @AneFisker
Contributors PA, AR, CSB and ABF designed the trial. SB and ABF supervised enrolments, follow-up, data entry and data cleaning. SB and ABF analysed the data. SB wrote the first draft of the paper. ABF has primary responsibility for the final content. All authors contributed to and approved the final version of the paper.
Funding The Danish National Research Foundation (grant: DNRF108) funded the data collection. Odense University Hospital (grant: A70) co-funded the salary of SB. Independent Research Fund Denmark (Sapere Aude Research Leader grant: 9060-00018B) and Lundbeck Foundation (Ascending Investigator grant: R313-2019-635) support ABF’s work.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.