Article Text

Abstract
Background Maternal mortality remains a public health problem despite several global efforts. Globally, about 830 women die of pregnancy-related death per day, with more than two-third of these cases occurring in Africa. We examined the spatial distribution of maternal mortality in Africa and explored the influence of SDoH on the spatial distribution.
Methods We used country-level secondary data of 54 African countries collected between 2006 and 2018 from three databases namely, World Development Indicator, WHO’s Global Health Observatory Data and Human Development Report. We performed descriptive analyses, presented in tables and maps. The spatial analysis involved local indicator of spatial autocorrelation maps and spatial regression. Finally, we built Bayesian networks to determine and show the strength of social determinants associated with maternal mortality.
Results We found that the average prevalence of maternal mortality ratio (MMR) in Africa was 415 per 100 000 live births. Findings from the spatial analyses showed clusters (hotspots) of MMR with seven countries (Guinea-Bissau, Guinea, Sierra Leone, Cote d’Ivoire, Chad and Cameroon, Mauritania), all within the Middle and West Africa. On the other hand, the cold spot clusters were formed by two countries; South Africa and Namibia; eight countries (Algeria, Tunisia, Libya, Ghana, Gabon and Congo, Equatorial Guinea and Cape Verde) formed low–high clusters; thus, indicating that these countries have significantly low MMR but within the neighbourhood of countries with significantly high MMR. The findings from the regression and Bayesian network analysis showed that gender inequities and the proportion of skilled birth attendant are strongest social determinants that drive the variations in maternal mortality across Africa.
Conclusion Maternal mortality is very high in Africa especially in countries in the middle and western African subregions. To achieve the target 3.1 of the sustainable development goal on maternal health, there is a need to design effective strategies that will address gender inequalities and the shortage of health professionals.
- child health
- health policy
- health services research
- maternal health
- epidemiology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Maternal mortality is a global health issue; however, Africa bears more than 90% of the burden. Hypertension during pregnancy and post-partum haemorrhage have been identified as key risk factors in most maternal deaths in Africa.
However, the spatial distribution of maternal mortality using analytical approach in multicountry studies, and conditioning for multiple socioeconomic determinants is scanty.
What are the new findings?
The spatial distribution of maternal mortality ratio showed that hotspots for maternal mortality are made up of seven countries (Guinea-Bissau, Guinea, Sierra Leone and Cote d’Ivoire, Chad and Cameroon, Mauritania).
Gender inequality, low use of skilled birth attendant at birth and shortage of skilled health professionals are key social determinants that expose women to high risks of maternal mortality in Africa.
What do the new findings imply?
In order to achieve the SDG target 3.1 of 70 per 100,000 live births by 2030, countries that formed the hotspot clusters need to increase health care investments towards building a stronger and better health care personnel. Brain drain problem facing the African health sector must also be urgently addressed.
There is need for a concerted plan to address the problem of gender inequality in Africa. These strategies should be part of intervention efforts aimed at addressing high maternal mortality in Africa.
Background
Maternal mortality is the death of women during pregnancy or within 42 days of pregnancy.1 2 Every maternal death that occurred is a huge tragedy as its consequence is beyond the woman, it has been shown to have adverse social and economic impact on immediate family and community at large and, in some cases, generational impacts are huge.3 4 Evidence has shown that larger percentage of maternal death is preventable,5 6 however, it remains a global health concern because of its persistently high prevalence, especially in low-income and middle-income countries. It is now used as a sentinel event to track progress in reproductive health and other relevant development goals globally.
To aid international comparison, the term maternal mortality ratio (MMR) was coined, and it is defined as the number of maternal mortalities per 100 000 live births.1 5 At the end of the millennium development goal (MDG) era in 2015, the global prevalence of MMR dropped by 44%, from 385 MMR in 1990 to 216 MMR at 2015.5 7 8 Except for the USA with MMR of 14 per 100 000 live birth, most high-income countries have lowered their MMR below 7 per 100 000 live birth but more than 90% of the burden of maternal mortality remains in Africa and South Asia.5 9 The recent global health priority on MMR as encapsulated in the sustainable development goals (SDGs), is to reduce the global MMR to 70 per 100 000 livebirths and maximum of 140 per 100 000 livebirths in countries known for high incidence.10 11 For countries such as Sierra Leone, Chad and Nigeria with very high MMR, above 1100 per 100 000, it is going to be a herculean task that will require evidence and implementation of effective policies.
Determinants of maternal mortality are well-researched subject within health research in Africa; it has always received international attention since the International Conference on Population and Development Programme of Action till the current SDG. However, like other global health problems, more attention has been given to medically related determinants over the years. Determinants, such as postpartum haemorrhage and hypertension during pregnancy, are well emphasised in literature as the common cause of maternal mortality.5 6 Some family-level characteristics such as economic status and marital relationships, social–cultural factors such as religion, gender norms and health belief have also been identified as key determinants.12 13 While this showed that causes of maternal mortality are multifaceted, most interventions designed to tackle this major public health problem relate to the medical causes.
It is apparent that if the SDG will be met on MMR unlike the previous MDGs, there is need to apply pragmatic approaches in generating evidence and designing government policies to effectively tackle this problem. In this era of limited resources in most LMICs, foreign donor and funding agencies continue to play important roles in their healthcare system. Therefore, the need for these agencies and regional organisations, such as the WHO African regional office and West African Health Organisation, to prioritise health spending and funding is more important now than ever. Also, to reduce the incidence of maternal mortality, there will be needs to examine more critically, factors that expose women to some of the risk factors instead of focusing on individual-level or medical causes alone.14
With aggregated country-level data of MMR available for the African countries, coupled with availability of other social determinant of health (SDH) variables, first we statistically examined the spatial distribution of MMR in Africa to identify its hotspot/clusters within the continent as against the descriptive analysis we have in most studies. Taking a cue from Adeyinka and colleagues work on health equity of stillbirth rate in 194 countries,15 spatial regression was used to examine the factors associated with MMR in the continent based on adapted SDH approaches. Finally, we employed Bayesian artificial intelligence techniques to compute belief network based on the result of the regression to inform policy and intervention focus to effectively tackle maternal mortality and achieve relevant SDG goals for MMR in Africa.
Methods
Study design and data source
This is an ecological study based on aggregated country-level data extracted from three publicly available databases: World Development Indicator, WHO’s Global Health Observatory Data and Human Development Report (see online supplemental file 1). Data from 54 African countries were included in the study, the data were majorly based on nationally representative cross-sectional surveys such as Demographic and Health Surveys, Household Income and Expenditure Surveys, House Living Standard and Socioeconomic Surveys. The study year for the variables differs, ranging from 2006 to 2018; detailed description of data collection and survey designed are published elsewhere.16–18
Supplemental material
Study variables
Dependent variable
MMR was defined and computed as the number of women per 100 000 live births who died from pregnancy-related causes during pregnancy or within 42 days of pregnancy termination. This is computed by dividing recorded or estimated maternal death (non-AIDS women aged 15–49 years) by the total record or estimated live birth within the same period. The data were extracted from the World Bank Development Indicator, which is based on estimations from raw data collection in national representative cross-sectional surveys such as household income and expenditure surveys, house living standard and socioeconomic surveys.
Independent variables
Twenty-three independent variables measured at country-level were involved in the study. They were selected based on previous research on maternal mortality in Africa, and to cover the different aspects of SDH framework (see figure 1). As demonstrated in figure 1, we operationalised the selected independent variables using the social determinant models to highlight the possible relationships between MMR and the selected variables. The country-level demographic, socioeconomic and sociocultural factors examined include income inequality, Gross National Income (GNI) per capita, Gender Inequality Index (GII), urban residence, poverty rate, crude birth rate and female educational status. Behavioural factors involved are the prevalence of adult female currently smoking and total alcohol per capita consumption in female adult. We included prevalence of anaemia during pregnancy, the prevalence of obesity among female adults (age-standardised); underweight among female adults (as a proxy for maternal nutrition), the prevalence of hypertension among adult females (age-adjusted) and prevalence of diabetes mellitus in female adults (age-adjusted). Finally, we included factors associated with healthcare service coverage; the percentage of deliveries by caesarean section (CS, as a proxy for access to emergency healthcare during childbirth), antenatal care (ANC) coverage—at least four visits, skilled birth attendants during delivery, and proportion of women of reproductive age who have their need satisfied for family planning, adolescent birth rate and prevalence of child marriage—proxies for sexual and reproductive health. We hypothesised that the overarching determinants in the outermost box of the framework adapted from the WHO will influence factors in inner boxes, and this will further modify MMR in Africa. We conducted multicollinearity test and removed highly correlated variable by picking most relevant one maternal mortality research.
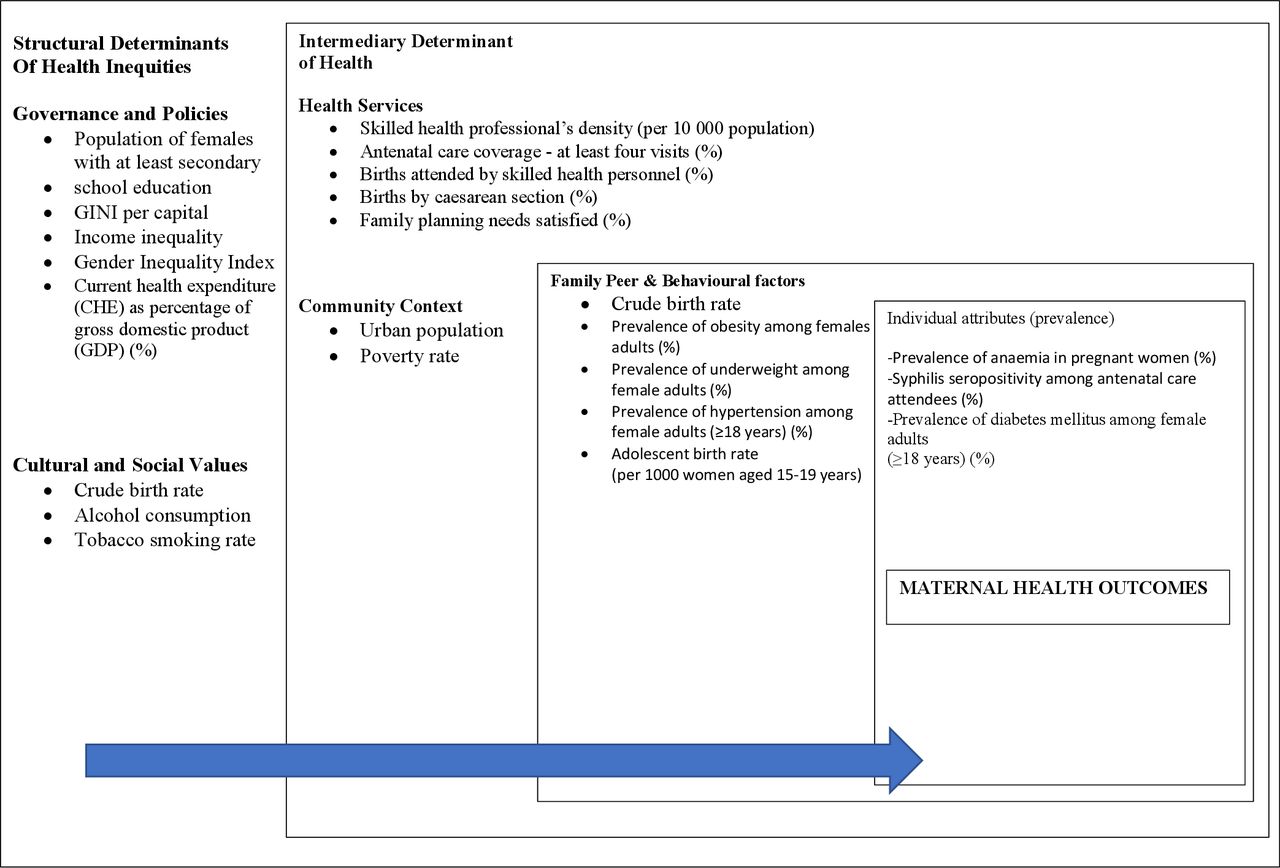
Social determinants framework for maternal death.
Statistical analysis
We conducted a descriptive analysis to explore the distribution of the dependent and independent factors examined in the social determinants of health (SDoH) framework. We adapted the WHO framework to build our models in three main domains (socioeconomic/cultural, healthcare resources and maternal conditions) for easy interpretations and policy implications. The values were expressed as mean with SD or median with IQR.
We used GeoDa v. 1.14 software to perform the spatial analysis, it is more suitable because it explicitly handles spatial data and allows statistical test findings as desired in this study.19 Country was used as a unit scale for spatial analysis, the distance-based threshold of 4272 km (Arc distance) was generated with X and Y coordinates from shapefile downloaded from Intergovernmental Action on Development Climate Prediction and Application Centre (ICPAC) GeoPortal (http://geoportal.icpac.net/). The appropriateness of this spatial weight was confirmed by assessing the symmetry of the connectivity histogram. The connectivity map also showed that all the 54 countries interlinked which is necessary to ascertain spatial dependency. We generated quantile cluster map to show the spatial distribution of the MMR in Africa descriptively. We also performed Global Moran’s I analysis to examine if spatial autocorrelation occurs at local level. Local indicator of spatial autocorrelation (LISA) cluster maps was also generated to statistically show the hot and cold spots spatial clusters of neighbouring countries with high and low MMR, respectively. Local spatial autocorrelation was measured with Local Moran’s I index which ranges from −1 to +1; with positive (+) values indicating strong clustering and negative (–) values indicating dispersion. Finally, we conducted spatial regression based on approaches developed by Anselin20 to investigate the association between MMR and independent variables. Six models were built with the first five covering a different aspect of SDoH framework and the final model only contained significant variables from each model. A pair-wise correlation was used to deal with missing data which were <2%. Ordinary least square (OLS) diagnostic was examined for each model, where spatial dependency was indicated, the model was fitted with spatial error or spatial lag regression as appropriate; best-fit model was determined using R-squared, Log likelihood and Akaike information criterion. We also tested for multicollinearity of independent variables, value <30 was used;20 999 Monte Carlo permutation was used for randomisation to ensure p-value<0.05.
We used the Bayesian network analysis to examine the strength of the relationship between MMR and the determinants. A machine learning R package called ‘bnlearn’ was used for the Bayesian network modelling;21 22 it is based on GeNie software. By using the variables that showed significant association in the final model of the spatial regression, we built the structure of the network from the domain knowledge of the authors on temporal precedence of the variables, using score-based structure algorithms. We introduced geographical regions based on the United Nation’s categorisation as a variable to deal with possible residual cofounding and accounted for missing values by using the expectation–maximisation algorithm. All the variables were continuous data, we discretised them by their median values to show the diagnostic conditional probability distribution. We used supervised machine learning techniques to predict the joint conditional probability of significant independent variables from the Bayesian network when countries with higher MMR are reduced to 70 MMR per 100 000; the target for the 2030 SDG for MMR. Finally, we used k-fold cross-validation (at k=10) to compare and examine the Bayesian model’s goodness of fit; log-likelihood loss was used as the loss function, therefore, the lower the value, the better the fit.23
Patient and public involvement
No patients or the public were directly involved in the design, conduct, reporting or dissemination plans of this research.
Results
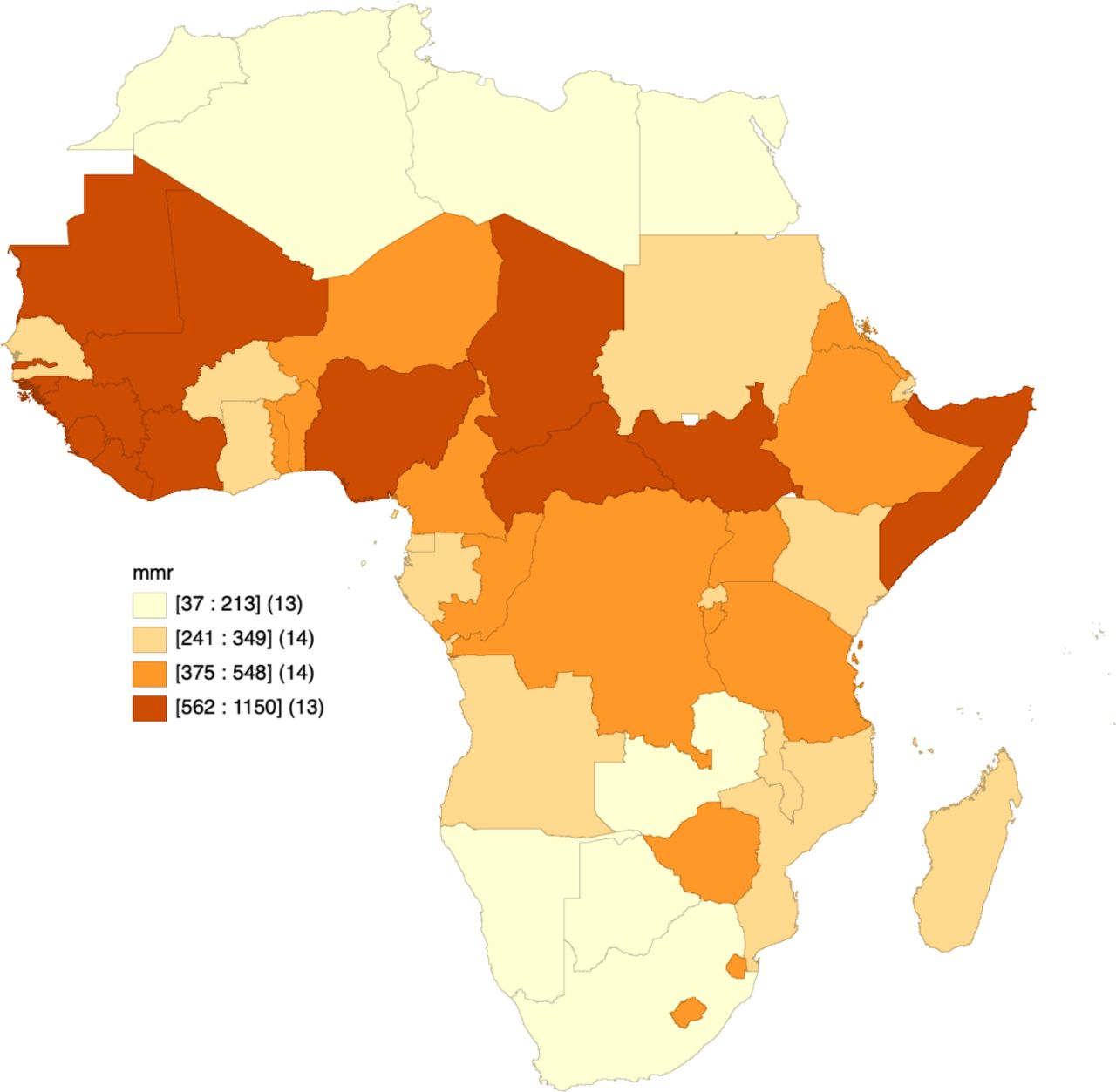
Table 1 and figure 2 show the findings from the descriptive analyses, both showing that the MMR varies across the 54 African countries involved in this analysis. As shown in table 1, the average MMR is 415 (SD: 277.8) per 100 000 total live birth, it ranges from 37 per 100 000 live birth in Egypt to 1150 per 100 000 live birth in South Sudan. The West African region has the highest mean of MMR 549 (SD: 257) per 100 000 live birth ranging from 58 per 100 000 live birth In Cape Verde to 1120 per 100 000 live birth in Sierra Leone. Middle African countries have the second highest with average MMR of 474 (SD: 322) per 100 000 live birth, followed by Southern and Eastern Africa. The lowest MMR was found in Northern Africa with 254 MMR (SD: 404) per 100 000 live birth. The SD indicates the presence of wide dispersion and variability between countries within that region of Africa; countries with the highest and lowest MMR as reported above are from the region.

Quartile map for descriptive distribution maternal mortality ratio in Africa.
Descriptive analysis of maternal mortality ratio (MMR) and independent variables arranged by domain of social health determinants
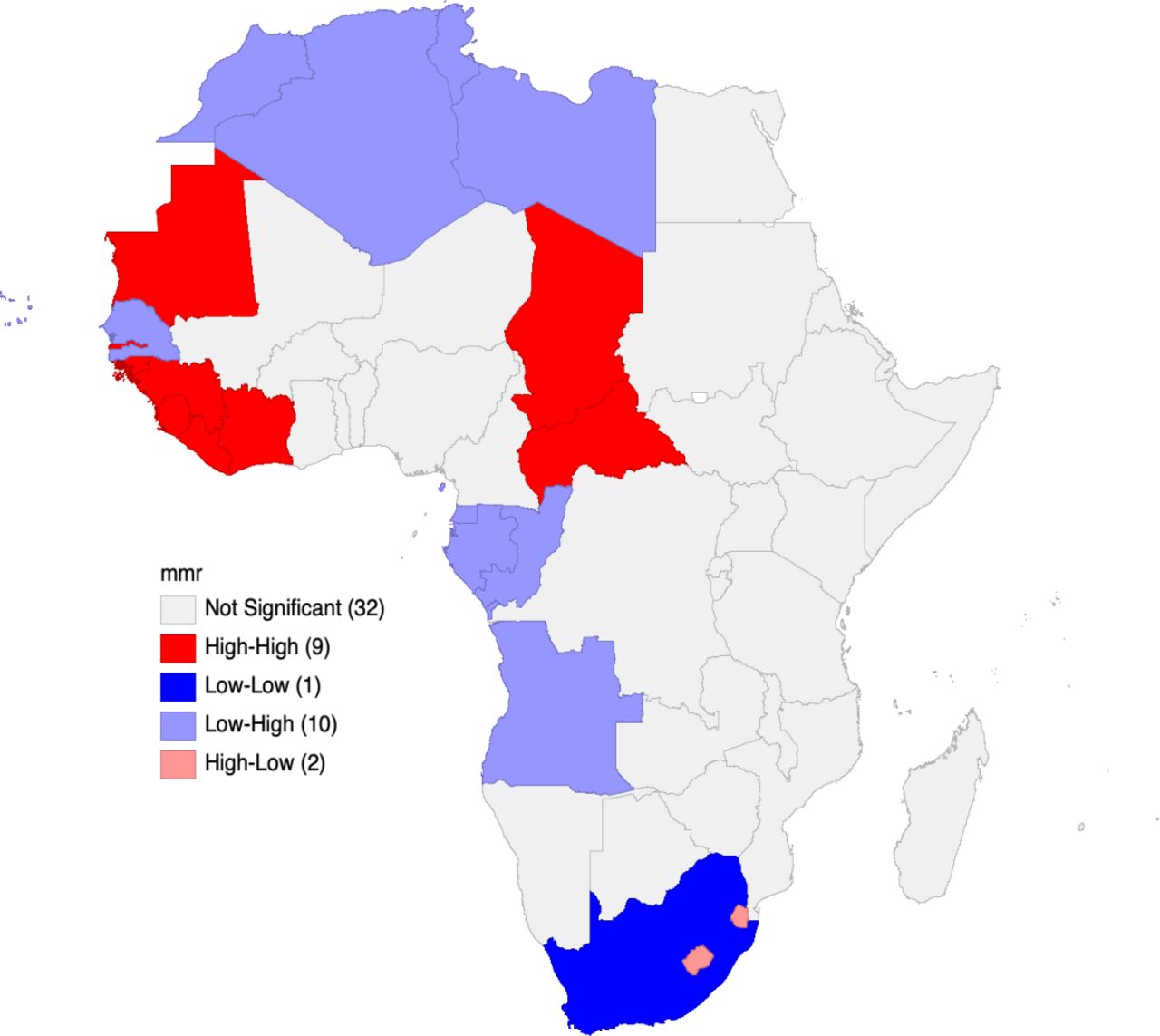
We observed a positively significant spatial autocorrelation with Moran’s I index 0.01 (p<0.05). Therefore, suggesting the aggregation of neighbourhood countries with similar values of MMR across geographical space than an expected random distribution. The LISA map was generated (figure 3) and showed the presence of high–high clusters (meaning countries with significantly high MMR forming hot spots) in 7 (13%) of the 54 countries. The hotspots for MMR in Africa were found in Western (Guinea-Bissau, Guinea, Sierra Leone and Cote d’Ivoire and Liberia) and Middle (Chad and Central Africa Republic) African countries. Mauritania, which is boundary country between Northern and Western part of Africa also form part of the hot-spot clusters. On the other hand, the cold spot cluster was observed in South Africa only. Outside these two extremes, 10 countries (Morocco, Angola, Algeria, Tunisia, Libya, Gabon, Congo, Equatorial Guinea, Cape Verde and Senegal) formed low–high clusters. This indicated that these countries have significantly low MMR within the neighbourhood of countries with significantly high MMR. Also, two countries from the south (Lesotho and Eswatini) appeared in the high-low clusters, indicating to have significantly high MMR within the neighbourhood with significantly low MMR.

LISA map for maternal mortality ratio (MMR) in Africa. LISA, local indicator of spatial autocorrelation.
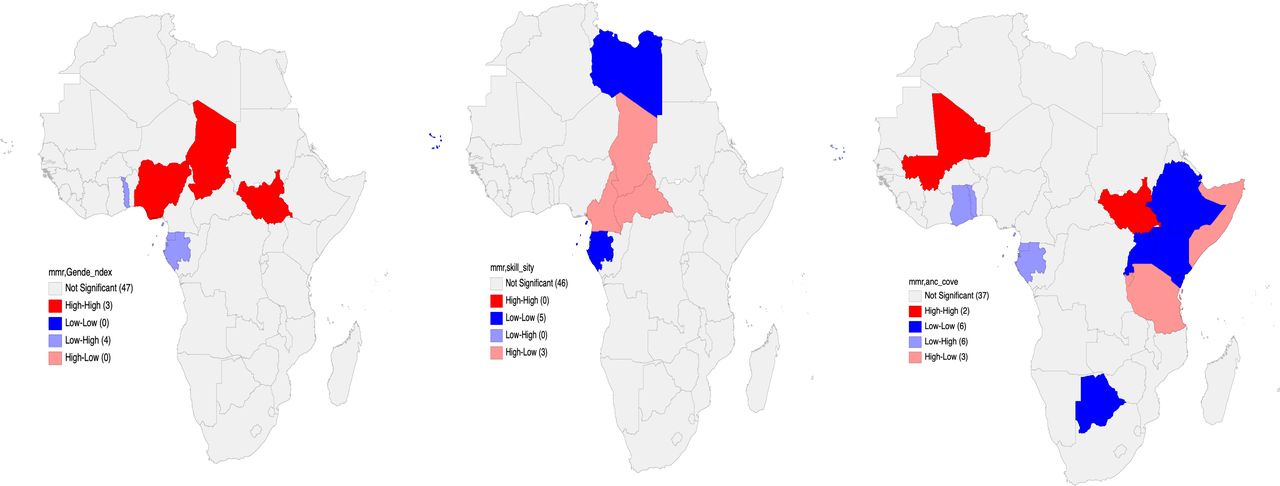
As shown in table 2, the findings from the bivariate spatial regression revealed that geographical variation in country-level percentages of urban population, poverty rate, crude birth rate, current health expenditure as percentage of GDP, prevalence of birth by CS, anaemia, ANC coverage, skilled birth attendance during birth and GII were significantly associated with MMR (see online supplemental file 2). However, finding from the adjusted models built based on the SDoH framework (in table 2) showed the following were significantly associated with MMR; GII (2207.69 (0.001)), Current health expenditure as a percentage of GDP (46.093 (0.02)), the density of skilled health professional (−9.22 (0.001)), Anaemia (9.21 (0.07)), Obesity among female adult (−27.46 (0.01)), deliveries by CS (−28.95 (0.057)) and ANC coverage (9.59991 (0.03)). These findings showed that GII has the biggest positive impact on MMR with obesity among female adult having negative impact. However, in the final model where we only included the significant variables from models I–V, Anaemia, Obesity and ANC coverage became statistically insignificant after we removed CHE, Obesity among female adult and delivery by CS to for best fit model with multicollinearity <30. Also, our findings showed that Gender index has the strongest association with MMR; every 1% increase in Gender index will increase MMR by more than 100% and every 1% increase in the percentage density of skill health personal will reduce MMR by 19%. The variables in our final model explain 56% of the variance in MMR (adjusted R2=0.556). The adjusted LISA maps in figure 4 corroborate finding from the spatial regression.
Supplemental material
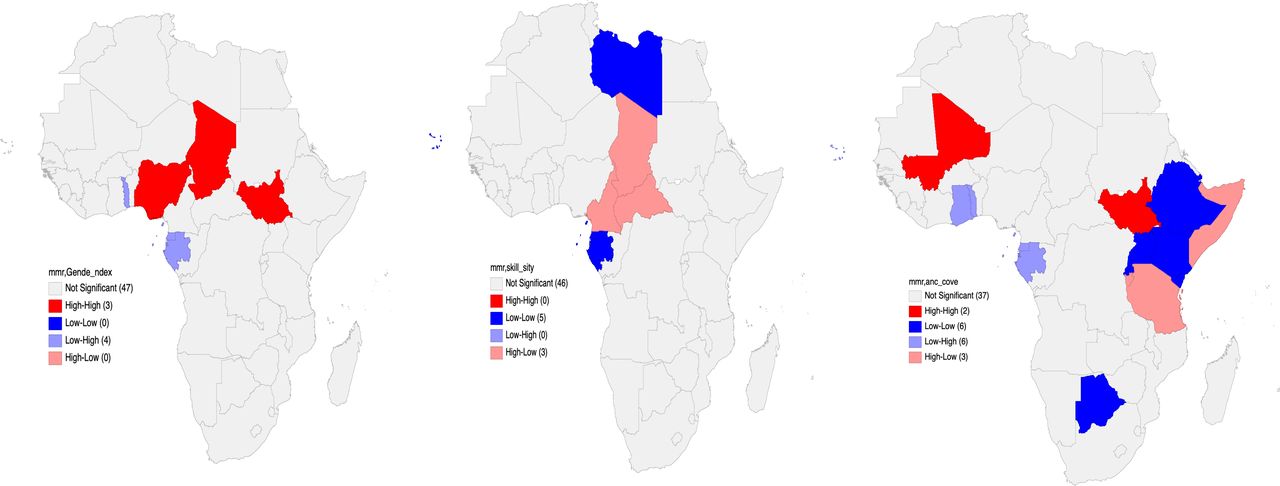
Adjusted LISA map of MMR with significant variables in final mode. LISA, local indicator of spatial autocorrelation; MMR, maternal mortality ratio
Multivariable spatial regression model for maternal mortality ratio (MMR)
Figure 5A presents the joint probability distribution from the network developed based on expert and previous research finding; it shows the local distribution corresponding to each variable in the network. Each arc (arrow) from one variable to another means the latter (variable at the head of the arrow) is dependent on the former (variable at the tail end of the arrow). Region is the only variable with no parent, meaning it is not dependent on any other variable while MMR was designed to be dependent on other variables. However, figure 5B showed that GII has the strongest influence on MMR as indicated by the width of the arc. Interestingly, skill attendant at birth has the second-highest impact on MMR while it also influences coverage of at least four ANC visits, and finally, in the network, the density of skilled health professional has influences proportion of births by CS. Finally, the Bayesian network reveals that the joint probability for low MMR increases from 29.8% to 100% when the percentage of GII reduces from 52% to 25.2% and skilled birth attendants increases from 48.1% to 80% (online supplemental file 2). The log-likelihood loss (6.01) and classification error (0.27) from the cross-validation analysis showed some levels of good fit and prediction accuracy of the Bayesian model built, showing about 74% accuracy.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Bayesian network of probabilistic inference of African regions, gender inequality, ANC coverage, skilled birth attendants at delivery (skill attendant), anaemia in pregnancy, current, health expenditure as percentage of GDP (CHE), birth by caesarean section (CS) and underweight. (B) Bayesian network of probabilistic inference (%) of the key determinants of MMR; the strength of influence was illustrated by weighted normalized width of arcs (arrows).
Discussion
Evidence from previous studies and global monitoring mechanism have consistently shown that maternal mortality is high in Africa, especially in sub-Saharan Africa.6 24 25 However, the statistical spatial distribution and variability of maternal mortality across Africa is not well documented. The few studies that have examined this aspect of maternal mortality are single-country studies, descriptive and sometimes, broad SDoH framework is not covered.26–28 Up-to-date multicounty evidence on spatial distribution and variability of maternal mortality is needed for monitoring progress on the 2030 SDG target 3.1, and for designing appropriate intervention across countries.
In this study, we observed that the mean MMR in Africa is 415 per 100 000 live birth (table 1). This highlights the high prevalence of MMR on the continent and more importantly, the enormous work that needs to be done within the next decade to achieve the SDG goal of reducing MMR to 70 per 100 000 live birth by 2030.10 11 Reducing the incidence of maternal mortality in Africa has been the cornerstone of most global health movements since the 1978s Alma Ata declaration on Primary health care (PHC), to the MDG and the current SDGs. There is also the Universal Health Coverage (UHC) movement, which has become a global health priority, especially for developing countries, with huge support from the WHO and the World Bank. In addition, the African Union’s (AU) recent initiative—Campaign for Accelerated Reduction of Maternal Mortality is an ambitious plan that aims to expand availability and uptake of universally accessible quality maternal mortality to reduce pregnancy-related deaths in Africa. As countries design strategies to achieve the UHC agenda, which is to increase coverage to essential health services to 80% and reduce the out-of-pocket payment to 15%–20%, this could be leveraged on to also reduce MMR in the continent. With evidence from countries like Ghana, provision of special or separate insurance schemes for pregnant women has proven to be effective. They can either be free or at discounted premium payment, especially for those from disadvantaged backgrounds and will enhance service utilisation and prevention of maternal mortality.29–31
The findings from our study revealed the presence of statistically significant spatial disparity in maternal mortality in Africa. Neighbouring countries with a high record of MMR formed statistically significant clusters of hotspots in the west and middle region of Africa. Previous studies that explored national and regional estimates have confirmed similar trends even though they are largely descriptive especially of high prevalence in Middle Africa.24 This region of the continent should probably receive more support, technical and funds, as strategies to combat maternal mortality in Africa. We also highlighted the countries that formed the hotspot/clusters for high MMR within the continent. In the western part, we had Guinea-Bissau, Guinea, Sierra Leone and Cote d’Ivoire, and middle Africa, we also had Chad and Central Africa Republic in middle Africa, and Mauritania, which is boundary country between Northern and Western part of Africa. International effort to tackle MMR in Africa is very high and more focused on Nigeria,32 obviously because of its population and very high incidence of maternal mortality. It recorded about 40% decrease at the end of the MDGs in 2015. However, none of the hotspot countries from our analysis recorded a minimum of 40% decrease, rather, some countries such as Cameroon and Chad had a slight increase in MMR. As efforts are being made to achieve the SDG goal for maternal mortality in the continent, these MMR hotspots in Africa should also receive more supports—technical, human capacity development and funding—from the international and donor agencies.
We investigated the factors using the social determinants framework with spatial regression and Bayesian network. Our results showed that the increased spatial pattern of GII is strongly associated with an increase in MMR. On the other hand, decrease in MMR is closely associated with an increase in the spatial pattern of skilled health personnel, while proportion of birth attended by skilled health professional showed to be strong determinant in the Bayesian network analysis. Findings from this study suggest that maternal mortality continues to be a serious health concern in Africa due to the adverse socioeconomic and inequitable social injustice women are exposed to. These results accord well with previous studies that show how poor health outcomes among disadvantaged population is driven by the social system and support they live in.15 33
In both the spatial regression analysis and the Bayesian network analysis, three factors, GII, percentage of skilled health professional and birth attended by skilled health professionals were associated with the spatial distribution and probability of increased MMR in Africa. As against the focus on medically related risk factors for maternal mortality over the years, the focus must be shifted on adequate human resources in the healthcare sectors in the continent. Inadequacy of health professional has been the bane of most healthcare systems in Africa for long and the pathway through which impact on MMR is obvious.34–36 It is well established that larger percentage of maternal death occurs in rural communities. The same rural communities are usually in shortage of healthcare professionals largely due to poor remuneration, lack of basic amenities in many of these rural areas couple with lack of incentives to encourage the retention of health workers as being practised in many high-come countries.37–40 Therefore, as complications due to hypertensive disorder and postpartum haemorrhage ensue during pregnancy or birth, lack of health professionals to manage this are probably the real cause of maternal mortality.
In consistence with other similar studies,15 27 28 one of the most profound findings from our analysis is the strength of association between the spatial distribution of MMR in Africa and GII; the Bayesian network generated also showed that it has the strongest impact of MMR in Africa. This highly suggests the potential role of women’s empowerment in tackling maternal mortality. Focusing on eradication of gender inequality in the African region is crucial because of its well-established links with the utilisation of reproductive, maternal, child and new-born health services. We found in our study that GII is also highly correlated with social and economic factors considered in this study such as poverty rate, GNI per capita, crude birth-rate and female educational attainment. This alone reinforced the ideology that GII is an important determinant of MMR which also drive socioeconomic and impact sociocultural developments in the continent. Over the years, research has shown and established that smart empowerment of women through education in any country is critical to achieving global health priorities, including the current SDGs.41–43 Interventions aimed at improving girl’s education in Africa should be given a new drive with long-term policy and funding backing under the lens of its amplifying effect on many other areas of health and socioeconomic development. Also, government agencies in Africa, with their foreign sponsors, should develop effective national and regional policies that will strengthen the adequacy of human resources and their retention in the healthcare system.
Finally, in contrast to general trends, findings from our analyses did not show significant associations between MMR, urban residence and lifestyle factors examined (smoking and alcohol consumption). This study has some areas of strengths: it is the first study to examine the social determinants of maternal mortality in Africa using spatial and Bayesian network analyses. Using these analytic approaches, we were able to examine the hot and cold spot for MMR statistically and the strengths of influence ranges of SDoH have on MMR in Africa. On the other hand, the ecological nature of the data set used placed some restriction on the interpretation of the findings. Therefore, the only association at country level do not confer association at individual levels. Also, some factors such as GII and GNI per capital were concurrently measured with the outcome variable; multicollinearity cannot be totally ruled out in our analyses. There were potential confounding factors such as intimate partner violence and the prevalence of polygamy not considered in the analysis because they were not available. Although the data sets were collected in the selected countries at different points in time between 2006 and 2018, similar standardised methodology was used to permit comparability across time and space. In addition, effort was made to minimise heterogeneity in our data by extracting and merging same year data point for each country involved in our analysis.
Conclusion
The findings from this study showed the distribution and disparity in maternal mortality in Africa; the hotspots were found in the middle and western parts of the continent. The proportion of skilled health professional, birth attended by skilled professional in each country and gender inequalities were the main contributors to the variations of maternal mortality. There are needs for the continent to refocus its strategies in combating the high prevalence of MMR with more core attention on drivers of social inequities. Finally, future individual or multicountry studies should focus more on the context at local levels and identify the most-deprived population especially in the countries that made up the hotspots within the continent.
Acknowledgments
The authors thank the MEASURE DHS project for their support and for free access to the original data.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Seye Abimbola
Twitter @SannietYaya, @aosanjorin
Contributors SY contributed to the study design and conceptualisation. SY and SSA reviewed the literature performed the analysis and drafted the first draft of this manuscript. SAA provided technical support and critically reviewed the manuscript for its intellectual content. SY had final responsibility to submit for publication. All authors read and amended drafts of the paper and approved the final version.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Map disclaimer The depiction of boundaries on this map does not imply the expression of any opinion whatsoever on the part of BMJ (or any member of its group) concerning the legal status of any country, territory, jurisdiction or area or of its authorities. This map is provided without any warranty of any kind, either express or implied.
Competing interests SY is editorial board member of this journal.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data for this study were sourced from World Development Indicator (https://databank.worldbank.org/source/world-development-indicators), WHO’s Global Health Observatory Data (https://www.who.int/data/gho) and Human Development Report (http://hdr.undp.org/en/data).
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.