Article Text

Abstract
Introduction Optimal breastfeeding practices have far-reaching health and economic benefits. Evidence suggests disparities in breastfeeding practices by maternal age-groups, with younger mothers often having lower rates of breastfeeding initiation, continuation and exclusivity compared with older mothers. There is limited knowledge of trends and factors associated with breastfeeding practices, particularly among adolescent and younger mothers in Nigeria. We examine key breastfeeding practices in Nigeria over a 15-year period, comparing adolescent mothers to young women.
Methods We used four Nigeria Demographic and Health Surveys collected between 2003 and 2018. We constructed six key breastfeeding indicators to cover the time period of breastfeeding from initiation to child age 24 months in women of three maternal age groups at the time of birth: young adolescents (<18 years), older adolescents (18–19.9 years) and young women (20–24.9 years). We used logistic regression to examine the association between maternal age group and select breastfeeding behaviours on the 2018 survey.
Results Analysis showed an increase in optimal breastfeeding practices across the four surveys and among all maternal age groups examined. Adolescent mothers had consistently lower prevalence for three of the six key breastfeeding indicators: early initiation of breastfeeding, exclusive breastfeeding <6 months and no prelacteal feed. Compared with young women, adolescent mothers had a higher prevalence of continued breastfeeding at 1 and 2 years. In multivariate analysis, we found that maternal age group was not associated with early breastfeeding initiation or with exclusive breastfeeding <6 months. However, several sociodemographic (ethnicity, region of residence) and healthcare-related (mode of delivery, antenatal care, postnatal breastfeeding counselling) factors were strongly associated with these two practices.
Conclusions In Nigeria, there is need to better support breastfeeding and nutritional practices in adolescents and young women focusing on ethnic groups (Hausa, Fulani, Kanuri/Beriberi) and geographic regions (South East) that are lagging behind.
- child health
- maternal health
- nutrition
- public health
- cross-sectional survey
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
The percentage of children ever breastfed in Nigeria in 2018 is high.
Children born to adolescent mothers have poorer survival and health outcomes, partly due to suboptimal (breast)feeding practices.
What are the new findings?
The prevalence of optimal breastfeeding practices among children <6 months of age has increased over time among all maternal age groups examined (<18, 18–19.9, 20–24.9).
We found narrowing of gaps between maternal age groups in the percentage of children exclusively breastfed and receiving no prelacteal feed, between 2003 and 2018.
Maternal age group was not associated with early initiation of breastfeeding or with exclusive breastfeeding of infants <6 months of age in multivariable analyses.
What do the new findings imply?
Our findings suggest the feasibility of improving optimal breastfeeding practices among adolescent girls and young women.
Evidence and action on breastfeeding requires contextualised understanding especially as it concerns subpopulations of adolescent girls and young women, predominantly identified by ethnicity and region of residence.
Introduction
Breastfeeding lays an important foundation for child survival and health by providing essential nutrition and protection necessary for early growth and development.1–4 When optimal, breastfeeding can prevent 823 000 child deaths every year, making it arguably the most effective child mortality prevention intervention, while also offering longer-term benefits including reduced risk for obesity, diabetes, asthma and dermatological diseases in children.5 6 Breastfeeding is also important to maternal reproductive health, improving uterine contractions immediately after childbirth,7 protecting against breast and ovarian cancers,5 8 and providing highly effective postpartum contraceptive protection through lactational amenorrhea.9 10 Given these benefits, breastfeeding is becoming increasingly recognised as crucial to health and development goals. Breastfeeding is directly linked to two of the UN Sustainable Development Goals (SDGs)—SDG 2 and SDG 3, which focus on improved nutrition, and maternal and child health, respectively. Additionally, improving breastfeeding drives progress towards other SDGs including: SDGs 4, 5 and 6 (breastfeeding impacts on intelligence, enhancing economic and human capital development)11–14 as well as SDG 10 by reducing inequality between the rich and poor.5 To optimise these benefits, the WHO currently recommends breastfeeding initiation within 1 hour of birth, exclusive breastfeeding for 6 months and continued breastfeeding for up to 2 years combined with complementary foods.
Despite evidence of its benefits, suboptimal breastfeeding practices continue to undermine the achievement of global maternal and child health goals. At current rates, many countries will fall short of the World Health Assembly target to increase the percentage of children under 6 months of age who are exclusively breastfed to at least 50% by 2025.15 This has grave health and economic consequences. For example, even though suboptimal breastfeeding fell from being the 8th to the 22nd leading risk factor of global mortality between 1990 and 2015,16 non-exclusive and discontinued breastfeeding remained the leading causes of death in most of sub-Saharan Africa,17–20 accounting for 45% of neonatal infectious deaths, 30% of diarrhoeal and 18% of acute respiratory mortality among children under 5 years.17 In China, India, Nigeria, Mexico and Indonesia alone, suboptimal breastfeeding accounted for over 236 000 annual child deaths, with future economic cost and cognitive losses estimated at $119 billion per year.21 22
Factors known to be associated with breastfeeding practices include economic status,23–28 maternal education,29 30 employment status,31 type of residence,32 mode and place of delivery,33–36 infant feeding counselling, sex and age of child.32 34 37 38 Although these factors affect women of all reproductive ages, evidence suggests that adolescent mothers are more physiologically and socioeconomically disadvantaged, and these disadvantages may lead to higher prevalence of suboptimal breastfeeding practices and worse health outcomes among their children. Compared with older mothers, adolescent and young mothers are less likely to initiate breastfeeding,39 40 more likely to prematurely discontinue exclusive breastfeeding41–43 and have a shorter overall duration of breastfeeding.44–47 Correspondingly, the health outcomes of their children are comparably worse than children born to older mothers.48 These issues explain why adolescents have become an important population group in global efforts to achieve equitable health and leaving no one behind.49 50
Several issues highlight the importance of exploring and understanding breastfeeding practices among adolescents. First, adolescent fertility rates, although declining globally, remain high in many low-income and middle-income countries (LMICs). In 2016 alone, adolescent mothers aged 15–19 years had more than 11 million live births,51 and a considerable number of these infants were affected by suboptimal breastfeeding practices. Second, as breastmilk can potentially mitigate or offset some of the social and economic disadvantages faced by adolescents and their infants, research and interventions tailored to the specific needs and concerns of this population are critically needed. This is more so given that adolescents have unique challenges and vulnerabilities that make them substantially different from older mothers, resulting in specific concerns about breastfeeding practices.52–60 Considering that these maternal-age differences are further amplified by contextual and population differences in breastfeeding practices, a contextualised understanding of facilitators and barriers of breastfeeding is critical to guide interventions aiming to establish and improve optimal breastfeeding especially in adolescents.
Nigeria is a west African country with an estimated population in 2018 of 195 million ethnically diverse people61 representing over 250 ethnic groups.62 63 The country is administratively divided into 36 states which are further subdivided into local government areas. Healthcare services are delivered through a mix of public (at all three levels of government) and private sector (ie, private for-profit, not-for-profit, religious and traditional and community-based outlets) providers. Nigeria’s most recent Demographic and Health Survey (DHS) in 2018 showed that the average duration of exclusive breastfeeding was 2.8 months and only 29% of children under 6 months of age were exclusively breastfed.64 Suboptimal breastfeeding in Nigeria is estimated to account for 103 742 child deaths annually, translating to almost $12 billion in future economic losses, rising higher to $21 billion per year (4.1% of gross national income) if cognitive losses and health costs are factored in 22. In 2016 alone, suboptimal breastfeeding accounted for over 50% of neonatal, infant and child deaths caused by diarrhoea and a disability-adjusted life years of 1.9 million among children under 5 years. Children born to adolescent mothers in Nigeria are disproportionately affected64 and this has been the pattern since 1990.65 While factors known to be associated with breastfeeding practices in Nigeria include normative and cultural expectations around breastfeeding, networks of support, place of delivery, and the activity of traditional birth attendants,65 66 the evidence on breastfeeding practices among adolescents is scarce.67–70
The objective of this paper is twofold. First, we sought to examine differences between adolescents (<20 years) and young women (20–24.9 years) with respect to trends in key breastfeeding indicators over a 15-year period in Nigeria. Second, we used the most recent survey data from 2018 to examine the association between maternal age group (adolescents versus young women) and two key breastfeeding indicators (early initiation of breastfeeding and exclusive breastfeeding of infants<6 months of age). This analysis was conducted adjusting for important confounders, including region of residence and mode of delivery.
Methods
Data
This is a repeat cross-sectional study using four DHS collected in Nigeria in 2003, 2008, 2013 and 2018. The DHS are cross-sectional, nationally representative household surveys using model questionnaires which are adapted by each country. The surveys collect information on a range of sociodemographic and health issues, including details of live births for all women of reproductive age (15–49 years) living in sampled households. Information collected about the mother and child dyad was based on the women’s self-report, while household characteristics were provided by the head of household in a separate questionnaire.
Population
The unit of analysis was children born in the 24-month period preceding each survey. We restricted the sample to children whose mothers were younger than 25 years at the time of the birth.
Definitions
Maternal age group: Our analysis focuses on a population of ‘young people’, which according to the WHO refers to individuals between ages 10 and 24. Further, the WHO defines an adolescent as any person between ages 10 and 19 years. We categorised maternal age groups at the time of birth as <18 (young adolescents), 18–19.9 (older adolescents) and 20–24.9 years (young women). The reason we did not include children of mothers older than 25 years at time of birth was that the parity profile in older maternal age groups does not overlap with adolescents and young women where the median age at first childbirth is in the age group 20–24.
Breastfeeding indicators: Using and adapting indicator definitions from WHO and DHS,64 71 we constructed six key breastfeeding indicators to cover the time period of breastfeeding from initiation to child age 24 months (table 1). These include: (1) ever being breastfed, (2) early initiation of breastfeeding, (3) no prelacteal feeding, (4) exclusive breastfeeding among children<6 months, (5) continued breastfeeding of children at 1 year and (6) continued breastfeeding at 2 years. To maintain consistency in denominators across all six indicators, we included only the most recently born child of each mother.
Definitions of breastfeeding indicators
The denominator for Indicator 1 (percentage ever breastfed) was estimated among most recently born children, to be consistent with the denominators for the other five indicators. We conducted sensitivity analysis on Indicator 1 among all children born <24 months before the survey versus only those most recently born (online supplementary material 1). Second, given the importance of birth order in breastfeeding practices and the predominance of children of first birth order among children born to adolescents and young women, we conducted additional analyses to estimate all six indicators restricting analysis to most recently born children who were birth order 1 (ie, first live birth to their mother) or the most recently born twin if the first birth reported resulted in multiples (online supplementary material 2). Third, in the population of indicators 4, 5 and 6, we excluded children not living with their mothers at the time of survey, consistent with the definition of these indicators in the DHS. The percentage of most recently born children (of all birth orders) not living with their mother at the time of survey, disaggregated by maternal age group is shown in online supplementary material 3. Last, the extent of missingness in the variables used to construct the six breastfeeding indicators was very low. Online supplementary material 4 provides details of how missing data were handled.
Supplemental material
Supplemental material
Supplemental material
Supplemental material
For the second objective, the age groups of mothers (<18, 18–19.9, 20–24.9) were the primary exposure of interest, and we considered indicators 2 and 4 to be the main outcomes. Initiation of breastfeeding within 1 hour was chosen as a reflection of intrapartum/early postpartum/neonatal care and support, and feeding practices in early infancy. Exclusive breastfeeding among infants younger than 6 months is a WHO and UNICEF recommendation based on well-established evidence and is related to education, knowledge, awareness, and support of exclusive breastfeeding in infancy.
Potential confounders of the association between maternal age group and early initiation of breastfeeding included: birth order (first or higher), sex of infant (male or female), pregnancy wantedness (wanted at the time or unwanted/mistimed), region (North- Central, North East, North West, South East, South South, South West), residence (urban, rural), ethnicity (broadly defined by four categories: Igbo, Ijaw/Izon, Ibibio, Ekoi; Hausa, Fulani, Kanuri/Beriberi; Yoruba, Igala, Tiv and Others), religion (Muslim; Christian and others), marital status at time of birth (married or cohabiting or neither), maternal education level (no education, primary, secondary and higher education), household wealth quintile, utilisation of antenatal care (ANC) during pregnancy (no antenatal care, 1–3 visits during pregnancy, 4+ visits during pregnancy), location of childbirth (home or other domestic environment, primary level health facility, hospital) and mode of delivery (vaginal or caesarean section).
Factors relevant to exclusive breastfeeding of children under 6 months of age which were the same as those for early initiation of breastfeeding include: birth order, sex of infant, pregnancy wantedness, region, residence, ethnicity, religion, education level, maternal education, household wealth quintile, utilisation of antenatal care during pregnancy, location of childbirth and mode of delivery. Additional variables included infant age in months at time of survey (0–1, 2–3, 4–5), maternal marital status at time of survey (married/cohabiting or not), whether the mother worked in the 7 days preceding the survey or not, whether the mother partly or fully controlled decisions about her own healthcare or not, whether breastfeeding was initiated early (Indicator 2) and whether the mother reported having received breastfeeding support from a health provider in the first 2 days after birth or not.
Analysis
All analysis was conducted in Stata SE v.15. For Objective 1, we ran descriptive analysis of levels reported for all six indicators across the three age groups and associated 95% CIs. We produced estimates if sample of children available was >50. For objective 2, we used logistic regression to examine the association between maternal age group and two key breastfeeding behaviours. Bivariate analysis examined the association between each variable and the outcome. All variables were retained in multivariable analysis regardless of significance, except in the analysis of exclusive breastfeeding where the sample size did not support the model with all variables. In this case, we removed variables not associated with the outcome at the p<0.1 level in either bivariate or multivariate models. We present crude and adjusted ORs (aORs) with associated 95% CIs and Wald test p values. The DHS use a multilevel cluster sampling survey design; individual women’s survey weights are needed in analysis to adjust for this and for non-response. Therefore, in all analyses, we adjusted for sampling weights, clustering and stratification. We did not pool the four surveys.
Ethical approval
The DHS receive government permission, use informed consent and assure respondents of confidentiality. We did not require an ethics approval for this study since it involved secondary data analysis.
Patient and public involvement
No patient or public involvement took place in the design or conduct of this analysis. The results are intended for wide dissemination, including to researchers, programme implementers and governmental agencies, all of whom reach the public and the key population of this study.
Results
We included 992 (2003), 4437 (2008), 4810 (2013) and 4844 (2018) most recently born children of mothers age <25 years at the time of birth, who were under the age of 24 months at the time of each survey in analysis.
Levels of breastfeeding indicators by age group and survey
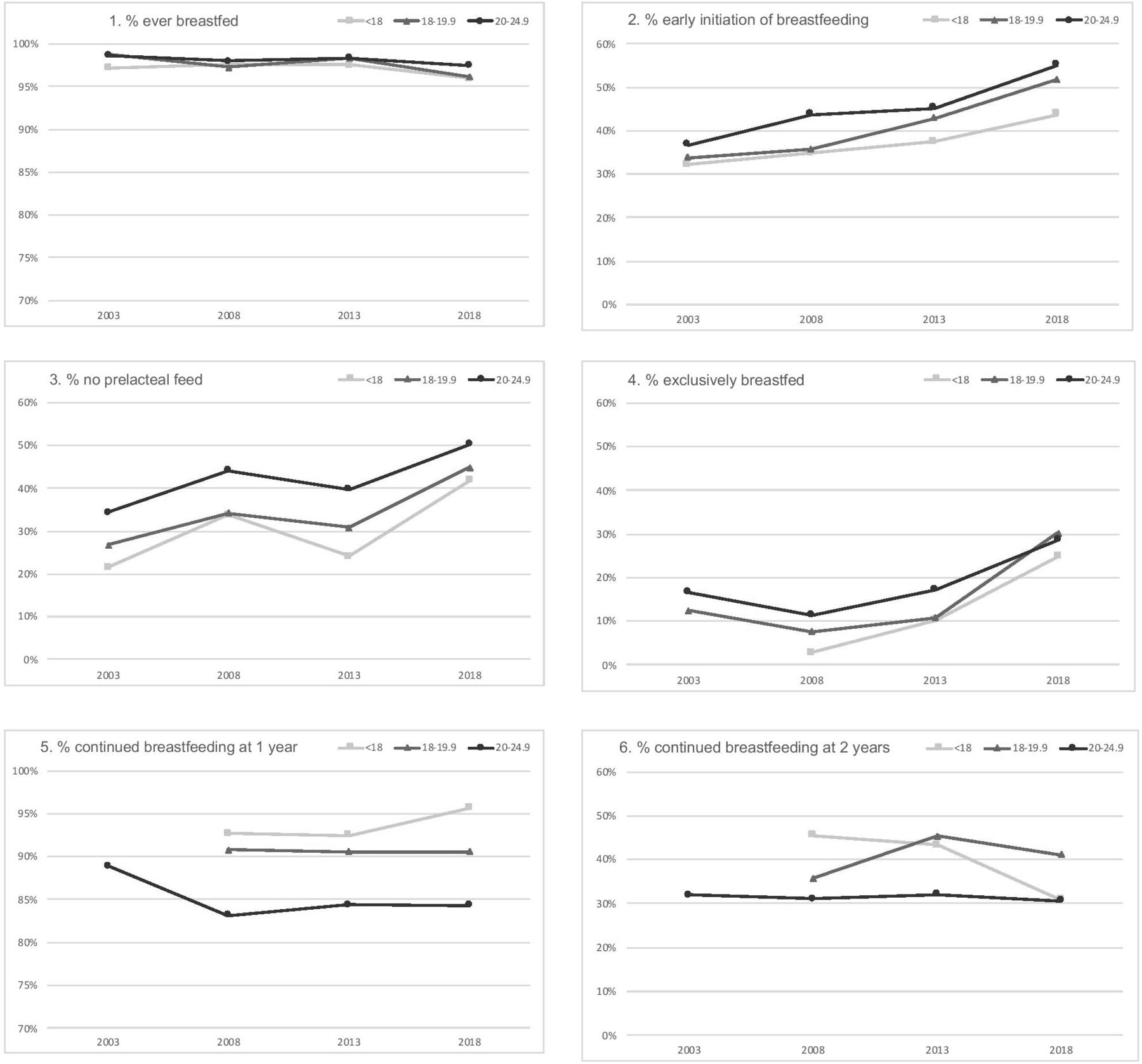
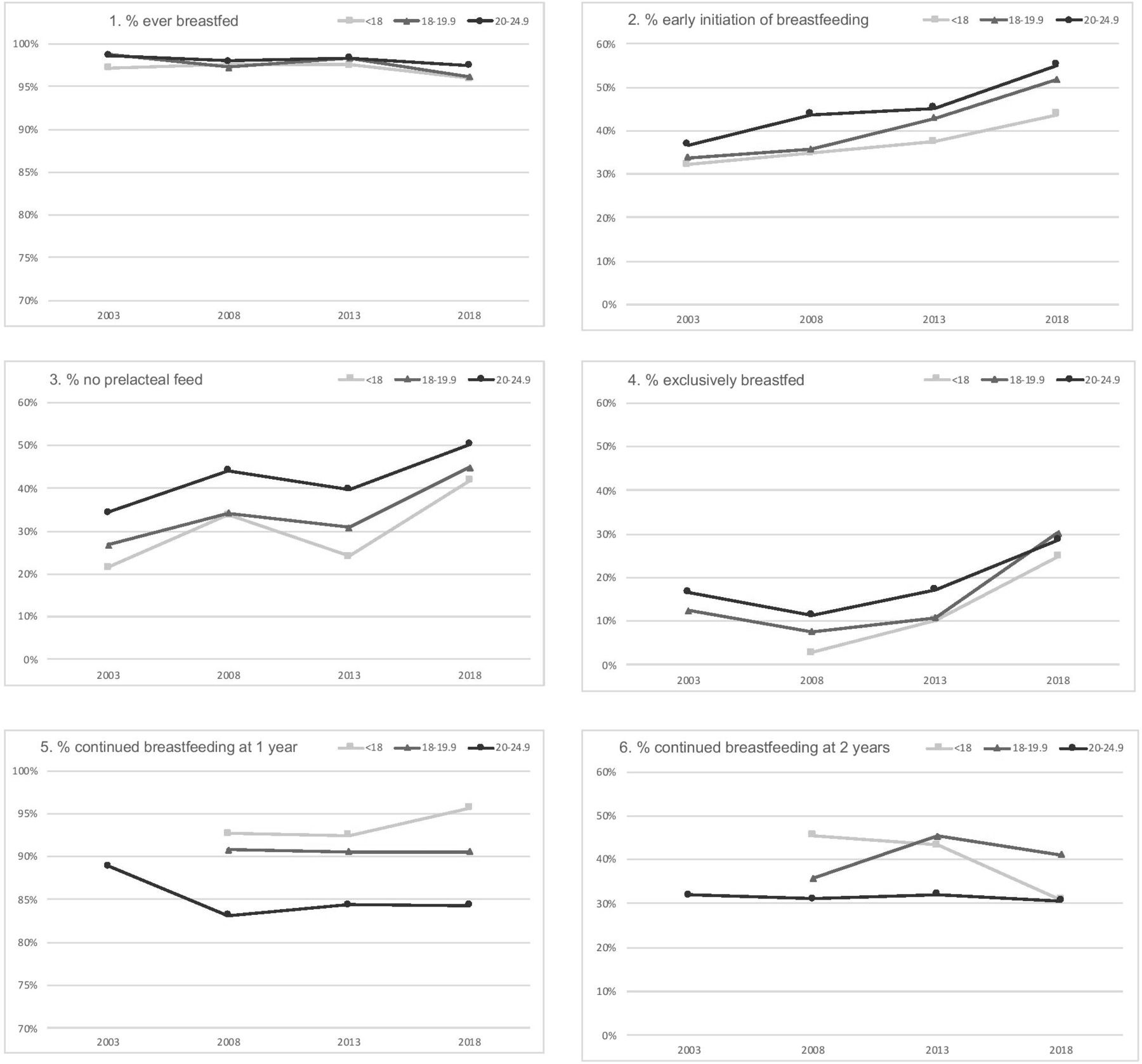
We report the main results of analysis for objective 1 in table 2 and figure 1. The percentages of children who were reported to have been ever breastfed (Indicator 1) were near universal (>96%) across all age groups examined and over the entire time period covered by the four surveys. Sensitivity analysis using all children (rather than just most recently born children) showed similar results (online supplementary material 1). The levels of early initiation of breastfeeding (Indicator 2) were relatively low—at around one third—in 2003, having increased steadily over time in all three age groups to reach levels of around 50% on the 2018 survey. Levels of early initiation were highest among young women (20–24 years), followed by the older adolescents (18–19.9) and young adolescents (<18) on all surveys. The percentage of infants receiving no prelacteal feed (Indicator 3) showed similar patterns as Indicator 2—starting from low levels and rising consistently over time, with lower levels among adolescent mothers compared with young women at each survey. This gap between maternal age groups was particularly wide in 2013.
Comparison of breastfeeding indicators by age of mother and survey
{kind=link}
Time trends in the six breastfeeding indicators, by maternal age group. Estimates are not available for certain age groups on the earliest survey due to small sample sizes (n<50).
Since the 2003 survey included small sample sizes of children (<50), we were not able to produce all age-disaggregated estimates for Indicators 4–6. In 2008, the percentage of infants<6 months of age who were exclusively breastfed (Indicator 4) was extremely low at around 10%. This percentage rose consistently over time to reach levels of around 30% in 2018, which were similar across the three age groups examined. The percentage of children who continued to breastfeed at 1 year of age (Indicator 5) was high at around 85%–95%, with no substantial changes in these levels over the period of time under examination. On the most recent survey, children of mothers<18 years at the time of birth appeared more likely to continue breastfeeding at 1 year compared with children of young women (95.7% compared with 84.3%). Last, the percentage of children continuing to breastfeed to 2 years of age (Indicator 6) have remained at around 30%–40% across time and age groups.
Given the importance of birth order in the comparisons between these young age groups, we conducted a sensitivity analysis of children of birth order 1 only (online supplementary material 2). This showed that in 2018, the levels of early initiation of breastfeeding were approximately the same within each maternal age group as for all birth orders combined, meaning that infants of young adolescents remained less likely to be put to breast within 1 hour of birth compared with those of young women. However, among first birth order infants, the differences between levels of exclusive breastfeeding <6 months (higher among children of young women) and continued breastfeeding at 1 year (higher among young adolescents) between young adolescents and young women widened.
Determinants of early initiation of breastfeeding (2018 DHS)
Next, we examined the crude and adjusted associations of age group with two key breastfeeding practices, early initiation of breastfeeding and exclusive breastfeeding of infants<6 months of age, on the 2018 survey. In crude analysis, compared with young women (20–24 years), young adolescents had 36% lower odds of initiating breastfeeding early (p<0.001) (table 3). There was no difference in early initiation of breastfeeding between young women and older adolescents (18–20 years). Among other factors examined, the crude association between region, urban/rural residence, ethnicity, religion, maternal education, household wealth quintile, antenatal care, location of childbirth and mode of delivery were significant at p<0.05.
Crude and adjusted association between maternal age group and early initiation of breastfeeding (n=4844)
In multivariable analysis, the effect of maternal age group was no longer significant; this occurred predominantly as a result of adjustment for ethnicity and to a smaller extent also for region and residence (these three variables were correlated to some extent). Mode of delivery was the factor with the strongest association with initiation of breastfeeding in the adjusted model; infants born by caesarean section had 87% lower odds of early initiation of breastfeeding compared with those born vaginally (p<0.001). In the adjusted model, the effect of two factors which were not associated with early initiation of breastfeeding in bivariate analysis became significant—birth order and wantedness of pregnancy. Infants of first birth order were 25% less likely to be breastfed compared with second and higher birth orders (p=0.001). Infants from pregnancies which were reported as mistimed or unwanted were 30% less likely to have been breastfed early (p=0.007). Compared with the North West region, infants from North Central and South West had more than twice the odds of early initiation of breastfeeding (both p<0.001). Ethnicity and household wealth quintile remained significant predictors of early initiation of breastfeeding. The adjusted association between receipt of antenatal care and early initiation of breastfeeding was in an unexpected direction; compared with infants whose mothers received no antenatal care, those who received 1–3 visits were 27% less likely to be breastfed early (p=0.013). The OR was also lower (aOR=0.83) among infants whose mothers received four or more antenatal care visits (p=0.085).
Determinants of exclusive breastfeeding under 6 months (2018 DHS)
We found that maternal age group was not associated with exclusive breastfeeding of infants under 6 months of age in crude or adjusted analysis (table 4). Compared with infants of second or higher birth order, first-born infants had 1.52 times the odds of being exclusively breastfed (p=0.027) in crude analysis; this association was no longer significant in adjusted analysis. The age group of infant was a strong predictor of exclusive breastfeeding. Compared with infants 5–6 months of age, those 0–1 month old were more than three times more likely to be exclusively breastfed (aOR 3.16, p<0.001) and those 2–3 month more than twice as likely (aOR 2.63, p<0.001). Region was not significantly associated with exclusive breastfeeding at the p<0.05 level, but adjusted ORs ranged from 0.50 (South East) to 1.27 (North East), compared with the North West region. It is possible that the lack of significance is related to sample size limitation rather than absence of effect. Compared with the ethnicity category combining Hausa, Fulani and Kanuri/Beriberi, all three other ethnic groups had higher odds of exclusive breastfeeding; this effect was significant among the Yoruba, Igala, Tiv category only (aOR 3.13, p=0.013). Compared with infants whose mothers reported no antenatal care, those whose mothers received 1–3 or 4+ visits were approximately 60% more likely to have been exclusively breastfed. Early initiation of breastfeeding was not associated with exclusive breastfeeding in adjusted analysis (p=0.845). Delivering in health facilities, and particularly primary health facilities (compared with home birth) and receiving postnatal breastfeeding counselling (compared with not receiving it) carried higher ORs of exclusive breastfeeding, although the p values were greater than >0.05. Notably, variables capturing household wealth, maternal education and maternal empowerment (work, decision-making) were not significantly associated with exclusive breastfeeding in the adjusted model.
Crude and adjusted association between maternal age group and exclusive breastfeeding among children under 6 months (n=1018)
Discussion
In this in-depth analysis of breastfeeding practices in adolescent girls and young women in Nigeria over a 15-year period, we found that adolescent mothers had consistently lower prevalence for three of the six key breastfeeding indicators compared to young women: early initiation of breastfeeding, exclusive breastfeeding <6 months and no prelacteal feed. The percentage of children ever breastfed was high, and similar across time and maternal age groups. Adolescent mothers had a higher prevalence over the time period for continued breastfeeding at 1 and 2 years compared with young women. The finding that adolescents outperform other age groups on continued breastfeeding at 1 and 2 years should, however, be interpreted with caution as studies have shown that prolonged breastfeeding within the context of socioeconomic disadvantage may be associated with increased risk of malnutrition if not well supplemented with complementary foods.72–76 Our findings support evidence provided by other studies that breastfeeding rates and practices vary across maternal age-groups.52 53 69 70
Despite a general improvement in breastfeeding practices across time and in maternal age groups examined, our study also showed differential patterns in the changes reported over time across key breastfeeding indicators. We note a narrowing of gaps between maternal age groups in the percentage of children<6 months being exclusively breastfed due to more rapid increases among adolescent mothers (from 2.8% in 2008 to 24.8% in 2018) compared with young women (from 16.7% in 2003 to 28.6% in 2018). A similar narrowing was observed for no prelacteal feed indicator with steeper increases among young adolescents (from 21.5% in 2003 to 41.8% in 2018) compared with young women (from 34.3% in 2003 to 50.3% in 2018). These findings suggest the feasibility of improving optimal breastfeeding practices across the board and among specific maternal target groups.
We found that compared with young women and older adolescents, children of young adolescent mothers (<18 years) in the 2018 survey had 36% lower crude odds of early initiation of breastfeeding (p<0.001). This effect remained after sensitivity analysis using only children of first-birth order, meaning that infants of young adolescents remained less likely to be put to breast within 1 hour of birth compared with those of young women. However, this effect disappeared after adjusting for ethnicity, region and residence. Similarly, we did not find evidence of an association between maternal age group and exclusive breastfeeding of infants<6 months of age. Ethnicity and residence were the most important sociodemographic predictors of both breastfeeding practices examined in multivariable analyses. Adolescent mothers from the Hausa ethnic group, and those residing in the North West and South East regions, were particularly negatively affected, similarly to findings from other studies.77–79
We found that factors related to health service utilisation (mode and place of delivery and number of ANC visits received) were associated with both early breastfeeding initiation and exclusive breastfeeding <6 months, although with differing magnitude and direction of effects. Surprisingly, increased number of ANC visits was also associated with lower odds of early breastfeeding initiation. Previous studies also found negative association between number of ANC visits and early breastfeeding initiation.80 81 Although this finding seems counterintuitive, we believe that frequent ANC visits may signify increased care contact due to potentially complicated pregnancies where women are likely to experience antenatal and intrapartum challenges requiring medical intervention. When coupled with the finding that infants born by caesarean section were 87% less likely to be breastfed within an hour of birth compared with those born vaginally, the result corroborates findings from other studies.82–84 Caesarean section birth lowers the likelihood of early breastfeeding initiation due to factors including prolonged separation of mother and child, surgical issues like the effect of anaesthesia and the stress or fatigue from a difficult labour or other maternal complications.85–89 Overall, this highlights that intrapartum or childbirth experience is an important determinant of early initiation of breastfeeding. Nevertheless, increased engagement with health services outside of the childbirth period (higher number of ANC visits, delivery in health facility and postnatal breastfeeding counselling) was associated with higher likelihood of exclusive breastfeeding of infants<6 months. This is not surprising given that prenatal health services are expected to be sources of information which can help challenge cultural practices, myths and belief systems unfavourable to optimal breastfeeding practices.81 90–93
Birth order and pregnancy wantedness were found to be associated with early initiation of breastfeeding, with first birth order infants 25% less likely to be breastfed compared with second and higher birth orders (p=0.001). A possible explanation for this might be the increased social support that occasions birth of first children in Nigeria. Contrarily, such social support may not necessarily be supportive of optimal breastfeeding habits and may also interfere with the mother’s role as the primary carer.66 94 For example, grandmothers have been documented to play important roles in infant feeding decisions in many LMICs, potentially leading to suboptimal breastfeeding practices such as supplementation and early introduction of solids.94–96 These suggest that interventions to improve breastfeeding practices will be more effective if targeted both at mothers and their social or cultural networks. Infants from pregnancies which were reported as mistimed or unwanted were 30% less likely to have been breastfed early. This corroborates findings from other studies, one possible explanation being that unplanned pregnancies can compromise maternal use of healthcare where breastfeeding counselling is provided and thereby affect breastfeeding practice.80 97–99 Finally, the age group of infant was a strong predictor of exclusive breastfeeding; compared with infants 5–6 months of age, those 0–1 month old were more than three times more likely to be exclusively breastfed (aOR 3.16, p<0.001) and those 2–3 months more than twice as likely (aOR 2.63, p<0.001). These suggest overall shortened duration of exclusive breastfeeding.
Limitations
The DHS sampling methodology excludes adolescent mothers living in institutions. Furthermore, due to small sample sizes, we did not conduct multivariable analysis of continued breastfeeding at 1 or 2 years, the indicators where, in descriptive analyses, adolescent girls had higher prevalence of optimal breastfeeding compared with young women. Nevertheless, it would be important to examine why and under what individual and contextual conditions adolescent and young mothers breastfeed longer. Findings in this paper are also limited by the fact that women’s self-report on breastfeeding practices is not always reliable and is prone to socially desirable answers.100 In large surveys such as the DHS however, it is not feasible to prospectively collect data on feeding practices, but they nonetheless provide indicative information on a population level.
Conclusion
Conducting a contextualised disaggregated analysis on breastfeeding practices in adolescent and young women has shed light on key issues that need to be addressed. In most other studies, maternal age in relation to breastfeeding is explored as a confounder and rarely as the main exposure of interest. Environmental, professional and familial circumstances may explain higher rates of exclusive breastfeeding in younger maternal age groups (unemployment, school dropout, direct family support), making it an opportunistic practice. In addition to other health benefits, breastfeeding may play a crucial role via lactational amenorrhea—serving a protective effect against repeat unwanted pregnancies in adolescents and young women. Less than 20% of mothers in the 2018 DHS sample of adolescent and young women reported receiving postnatal breastfeeding counselling. There is an urgent need to explore initiatives to better support breastfeeding and nutritional practices in adolescents and young women. In Nigeria specifically, these should retain a strong focus on ethnic groups and geographic regions that are lagging behind. Our findings show that in Nigeria, beyond early initiation and continuation of breastfeeding practices, where these practices occur (geographic region and residence), in which groups (ethnicity, social support systems and maternal age) and how (continued breastfeeding at the risk of poor supplementation), hold significant bearing. Future observational and intervention studies can expect to find heterogeneous results across maternal age groups and contexts.
References
Footnotes
Handling editor Sanni Yaya
Twitter @lenkabenova, @lade_abeji, @badejokikiolu
Contributors LB conceptualised the study with input from MS, I-OOA and OB. LB conducted the data analysis. All authors contributed to interpretation of findings. LB and OB wrote the first draft, which was revised and approved by all authors.
Funding This study was funded by Fonds Wetenschappelijk Onderzoek (Senior Postdoctoral Fellow (to LB)), Belgian Development Cooperation (Doctoral Scholarship (to OB)).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available in a public, open access repository. Data are available for research purposes on www.dhsprogram.com after registration.